
Abstract
Background:
Pediatric horizontal distal metaphyseal tibial fractures are relatively uncommon injuries. While nonoperative treatment remains the standard of care for most cases, certain fracture patterns may carry a higher risk of treatment failure, and optimal treatment strategies are still unclear. The aim of this study was to investigate the frequency, anatomical location of these fractures within the metaphysis, and risk factors associated with treatment failure in nonoperative management.
Methods:
A retrospective, registry-based cohort study was conducted to evaluate treatment success in 86 consecutive pediatric patients with distal metaphyseal horizontal tibial fractures between 2014 and 2023. Demographic, clinical, and radiographic data were analyzed. Logistic regression analysis was performed to identify independent predictors of nonoperative treatment failure. Nonoperative treatment failure was defined as the requirement for cast wedging, re-reduction, or surgical intervention due to loss of reduction or coronal angulation greater than 10° observed on final follow-up radiographs.
Results:
Of the 86 patients included, 70 (81%) were initially treated non-operatively, while 16 (19%) underwent primary surgical fixation. The overall failure rate in the nonoperative group was 35.3% (25/70). Multivariable logistic regression identified 3 independent predictors of treatment failure: age >11 years (adjusted odds ratio [OR], 10.1; 95% confidence interval [CI], 1.3–81.7; p = 0.030), the presence of a complete fibular fracture (adjusted OR, 6.1; 95% CI, 1.2–30.1; p = 0.027), and initial coronal angulation >10° (adjusted OR, 4.9; 95% CI, 1.1–23.0; p = 0.042). The complication rate was significantly higher in the operative group compared to the nonoperative group (18.3% vs. 4.3%; relative risk, 4.4; 95%CI 1.0–19.7, p = 0.042).
Conclusions:
Nonoperative treatment remains an effective approach for the majority of pediatric horizontal distal metaphyseal tibial fractures. However, patients with older age, concomitant complete fibular fractures, or marked initial angulation may benefit from early surgical intervention to mitigate the risk of treatment failure.
Level of Evidence:
Introduction
Tibial fractures account for approximately 15% of all pediatric fractures, with distal tibial fractures comprising nearly half of these cases.1,2 Distal horizontal metaphyseal tibial fractures with significantly lower incidence pose unique management challenges.3,4
Gillespie et al. described distal horizontal metaphyseal tibial fractures with posterior angulation as initially appearing benign yet frequently resulting in unacceptable progression of the angulation by the end of cast treatment. To address this, casting the limb in equinus was proposed in cases with posterior angulation. 5 Domzalski et al. 3 identified two primary displacement patterns in distal metaphyseal tibial fractures: valgus recurvatum and varus procurvatum. Recognition of these patterns may facilitate selection of appropriate treatment strategies and for predicting the risk of treatment failure. 1 Additionally, Megerian et al. 6 emphasized that the sagittal morphology of the distal tibia characterized by a consistent apex posterior bowing may affect the quality of fracture reduction and should inform treatment planning.
Management strategies depend on multiple factors, including patient age, fracture pattern, and the degree of displacement. Nonoperative treatment with closed reduction and casting remains the standard of care for nondisplaced or minimally displaced fractures. 3 However, significantly displaced fractures with high instability may necessitate surgical fixation using K-wires, plates, or external fixators. 4 Treatment decisions are often influenced by factors such as the presence of a concomitant fibular fracture, the initial displacement magnitude, and the degree of angular deformity. 3 Given the risk of malunion, regular clinical follow-up and radiographic monitoring are necessary for early detection of complications and assessment of fracture healing. Optimizing management strategies is important for achieving favorable functional outcomes in pediatric patients.1,3
This study aimed to assess the frequency, typical metaphyseal location, and risk factors for treatment failure in nonoperative management of horizontal distal tibial fractures in children. We hypothesized that older age and initial displacement would increase the risk of treatment failure.
Material and methods
This was a single-center, registry-based study using a prospective fracture registry system developed and maintained at a tertiary-level pediatric hospital. The registry includes all fractures in patients aged ≤16 years treated at the institution since 2014, and contains patient demographics, injury mechanism, fracture location, treatment method, and follow-up data. We retrospectively identified all children diagnosed with distal metaphyseal horizontal tibial fractures between 2014 and 2023. A horizontal transverse metaphyseal fracture is defined as follows: “a fracture line deviating ≤10° from a line perpendicular to the longitudinal axis of the tibia on anteroposterior (AP) radiographs.” Fractures with an angular deviation >10° from this reference were classified as oblique metaphyseal fractures and were not included in the present cohort. Clinical records and radiographs were reviewed to confirm diagnosis and determine eligibility. Additional data were collected on radiographic displacement, associated injuries, and treatment details. High-energy mechanisms and more severe associated injuries (including open fractures and nerve injuries) were more common in the surgically treated group. However, in our multivariable logistic regression model focused on nonoperative failure, associated injuries were entered into the multivariable logistic regression model but did not retain statistical significance after adjustment for age, complete fibular fracture, and initial coronal angulation, and were therefore not identified as independent predictors of nonoperative treatment failure.
During the study period, a total of 111 patients were initially identified with distal horizontal metaphyseal tibial fractures. Three patients were excluded due to incorrect initial diagnoses, and one due to osteogenesis imperfecta. Additionally, 21 patients had a torus fracture and were excluded from the final analysis. Pure compression-type buckle injuries with localized cortical bulging and an intact opposite cortex, without measurable angular deformity in either the coronal or sagittal plane. All 21 excluded torus fractures met this definition and were therefore excluded from the final analysis. Consequently, 86 patients met the inclusion criteria and comprised the final study cohort (Figure 1).
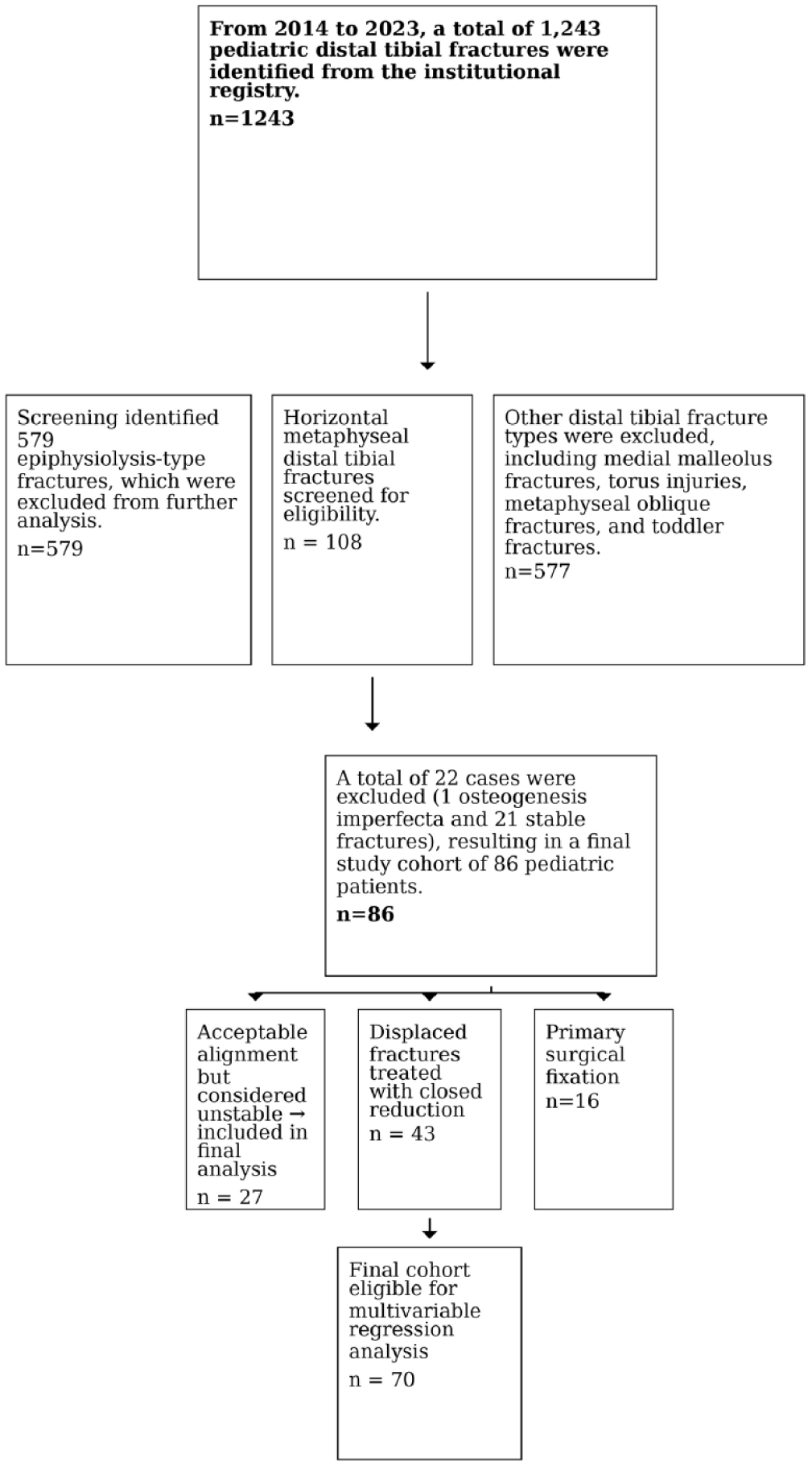
Flowchart illustration: Patient selection and grouping based on inclusion and exclusion criteria.
Fracture location was determined by measuring the distance (mm) from the distal tibial physis to the closest point of the horizontal fracture line on anteroposterior (AP) radiographs. To account for anatomical variation between patients, this distance was normalized by dividing it by the total height of the tibial metaphysis. The total metaphyseal height was defined according to the AO-PCCF as the distance between the distal tibial physis and the proximal metaphyseal–diaphyseal junction, identified radiographically at the point where the cortices become parallel and the metaphyseal flare transitions into the diaphysis. All fracture locations were re-evaluated using this standardized definition. The apparent proximal outlier in Figure 2 was carefully reviewed and confirmed to fall within the AO-defined metaphyseal region. The resulting distribution of these relative fracture locations is illustrated in Figure 2.
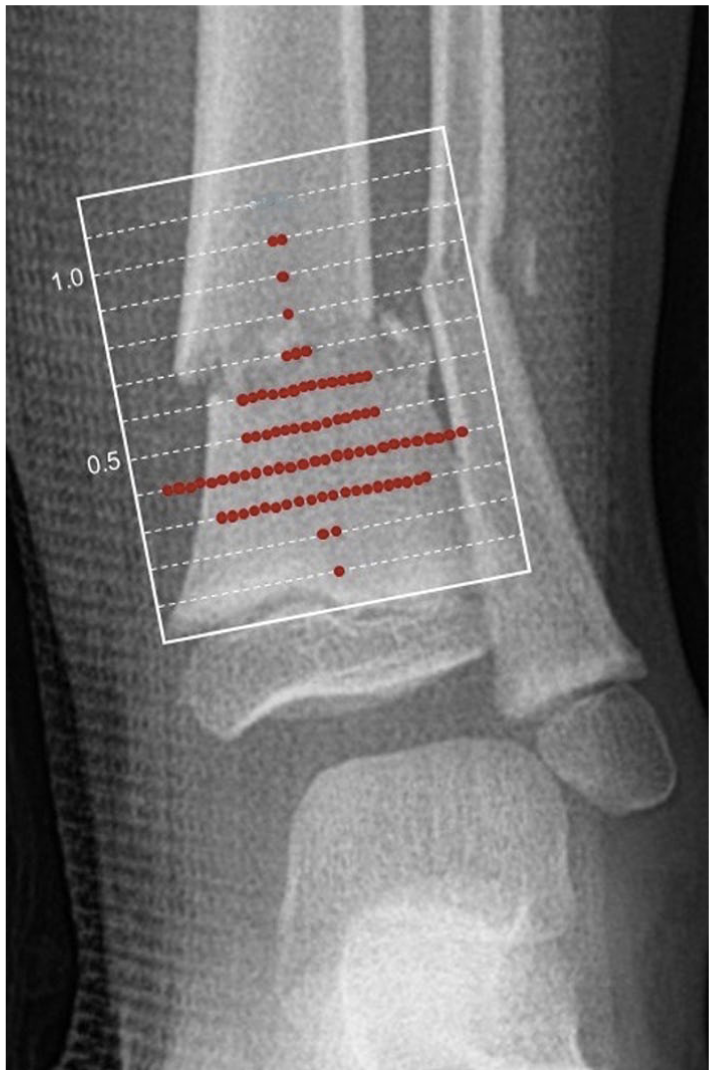
Anteroposterior radiographic overlay illustrating the anatomical distribution of distal metaphyseal tibial fractures.
Surgical fixation was defined as closed or open reduction in combination with internal fixation (K-wires, screws, plates). Treatment failure following cast treatment was defined as the requirement for cast wedging, re-reduction, or surgical intervention due to loss of reduction or angulation greater than 10° observed on final follow-up radiographs. Loss of reduction was defined as a fracture that initially met the acceptable alignment criteria after closed reduction and casting but subsequently progressed beyond the predefined threshold of >10° coronal angulation on follow-up radiographs. In 59 of 86 patients, primary closed reduction was performed in the emergency department under conscious sedation, whereas 27 patients underwent reduction under general anesthesia in the operating room. All reductions were performed by residents under the direct supervision of a pediatric orthopedic surgeon. Cast wedging and secondary closed re-reductions were performed in the fracture clinic or cast room, often under fluoroscopic guidance when needed, and under appropriate analgesia or light sedation for patient comfort. Primary surgery was considered in the presence of one or more of the following: Inability to achieve or maintain acceptable alignment with closed reduction and casting (including recurrent loss of reduction during the same admission), open fractures, segmental or markedly unstable patterns with substantial displacement, neurovascular compromise, or threatened soft-tissue envelope. Regarding changes over time: we have clarified that formal surgical indications remained stable over the study period (2014–2023). Minor changes occurred in anesthesia and analgesia protocols, but these did not affect the criteria for choosing surgery versus casting.
Statistics
Descriptive statistics, including means, ranges, and standard deviations, were calculated for continuous variables exhibiting a normal distribution. Normality was assessed using the Shapiro–Wilk test. Comparisons of mean values were performed using Student’s t-test.
Variables that did not follow a normal distribution were reported as medians with interquartile ranges. Frequencies and proportions were used to summarize categorical variables. Differences in proportions were assessed using the standardized normal deviate (Z) test, and the distribution of categorical variables was analyzed using the chi-square test or Fisher’s exact test when expected cell counts were less than five. The risk of nonoperative treatment failure was assessed using logistic regression analysis, with both crude and adjusted odds ratios (ORs) reported.
Prior to data collection, the study team predefined several factors potentially associated with an increased risk of failure following nonoperative management: older patient age, male sex, presence of a complete fibular fracture, varus angulation, recurvatum deformity (posterior apex), displacement >50%, and angulation >10° on either anteroposterior (AP) or lateral radiographic views. All predefined variables were included in the multivariate logistic regression model, regardless of their statistical significance in univariate analyses. A two-tailed p-value of less than 0.05 was considered statistically significant, and 95% confidence intervals (CIs) were reported where applicable. Statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) and Stats Direct version 3.0 (Stats Direct Ltd., Altrincham, UK).
Results
Of the 86 patients included, 70 (81%) were initially managed nonoperatively with casting, and 16 (19%) underwent primary surgical fixation. The mean age at the time of injury was 8.7 ± 4.0 years (median: 8.5 years), and 60 patients (70%) were male. Fracture lines were most commonly located between 30% and 60% of the total metaphyseal height, measured from the distal tibial physis (Figure 2). Eight patients had associated injuries: three sustained soft tissue injuries, two had nerve injuries, and two experienced combined soft tissue and nerve injuries. One patient had a contralateral distal tibial fracture, and another sustained an ipsilateral talar fracture.
Cast treatment (n = 70)
The most common injury mechanisms were playground and trampoline accidents (23%), followed by skiing (14.3%) and sledding (14.3%). One patient had an open fracture (Gustilo-Anderson type I). Most patients (96%) were treated with an above-knee cast (Table 1). Seventeen patients (24%) required re-reduction or cast wedging, and eight (11.4%) underwent delayed surgery due to loss of reduction. The mean duration of immobilization was 5.4 ± 2.0 weeks, and the mean time to full weight-bearing was 4.9 ± 2.1 weeks. Residual coronal angulation >10° on final radiographs was observed in 15 patients (21.4%). Three patients (4.3%) experienced complications, including pain, pressure ulcers, and one case of permanent tibial nerve injury.
Patient demographics and injury characteristics.
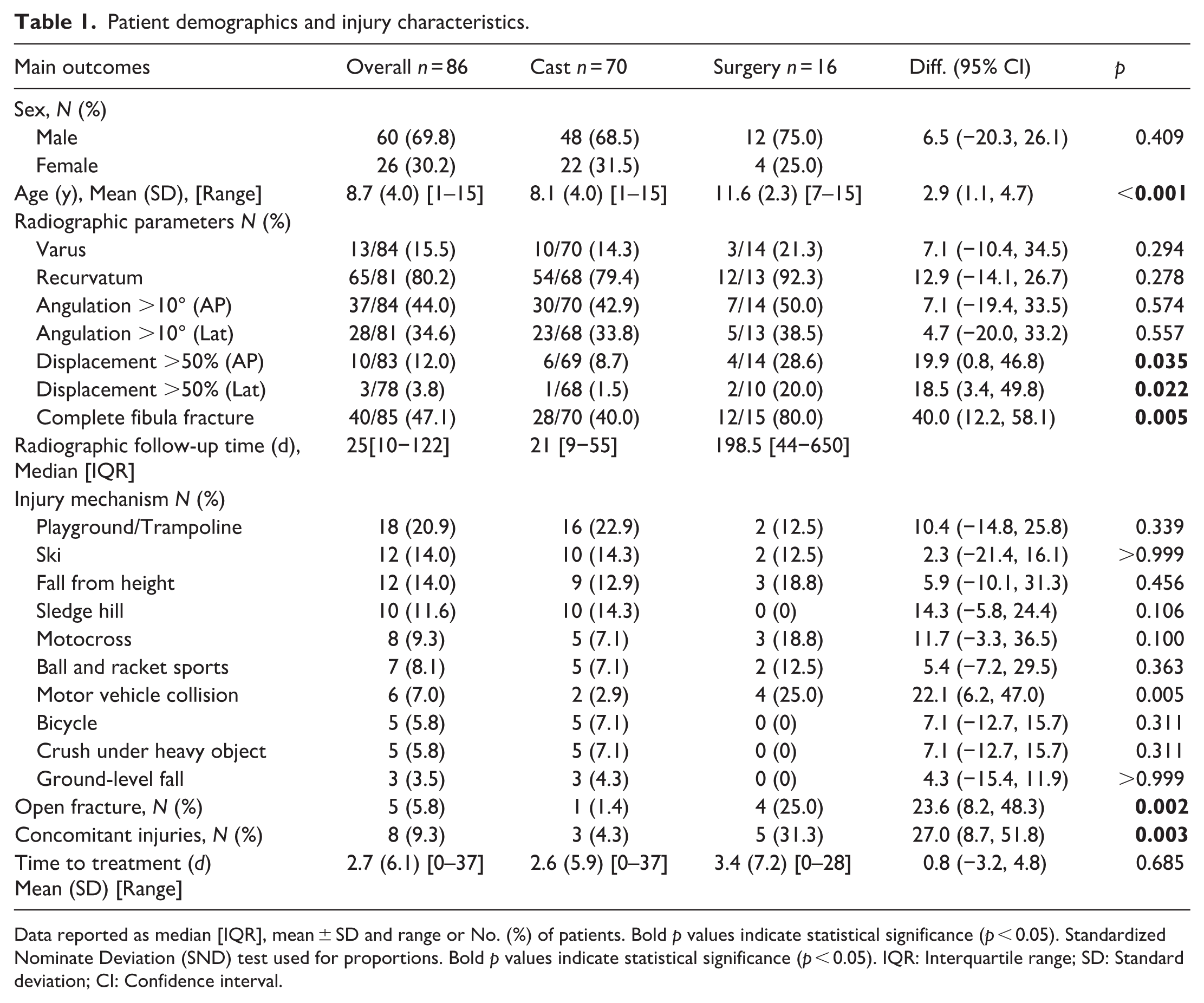
Data reported as median [IQR], mean ± SD and range or No. (%) of patients. Bold p values indicate statistical significance (p < 0.05). Standardized Nominate Deviation (SND) test used for proportions. Bold p values indicate statistical significance (p < 0.05). IQR: Interquartile range; SD: Standard deviation; CI: Confidence interval.
The overall treatment failure rate in the primarily cast treated was 35.3% (25/70) (Table 2). The choice of fixation method did not differ significantly between patients who underwent surgery following failed nonoperative treatment and those who were treated operatively from the outset (Table 3).
Treatment methods and complications.
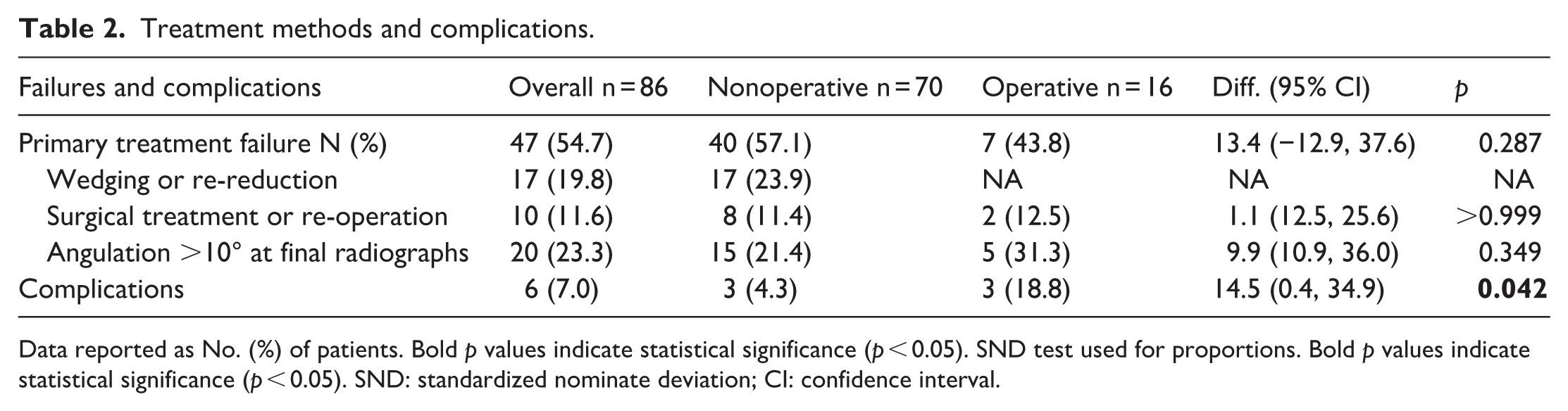
Data reported as No. (%) of patients. Bold p values indicate statistical significance (p < 0.05). SND test used for proportions. Bold p values indicate statistical significance (p < 0.05). SND: standardized nominate deviation; CI: confidence interval.
Fixation Methods.
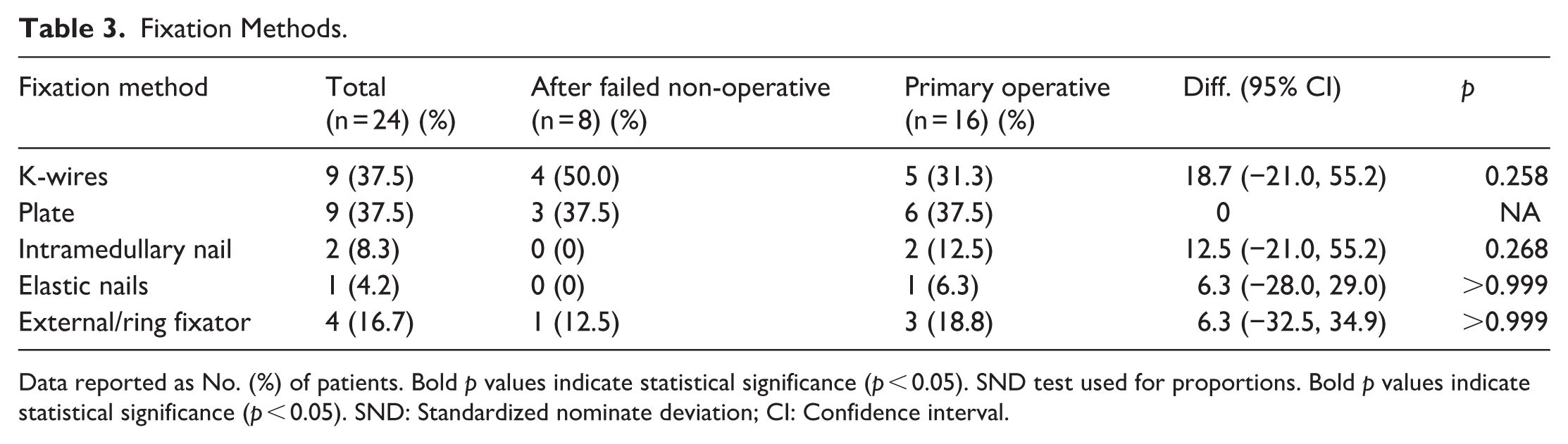
Data reported as No. (%) of patients. Bold p values indicate statistical significance (p < 0.05). SND test used for proportions. Bold p values indicate statistical significance (p < 0.05). SND: Standardized nominate deviation; CI: Confidence interval.
Surgical treatment (n = 16)
Primarily surgically treated experienced more often high-energy mechanisms, including motor vehicle collisions (25%), motocross (19%), and falls from height (19%) (Table 1). Four patients had open fractures, one Gustilo-Anderson type 1, one type 2 and two type 3. Fixation methods included K-wires (nine patients), plates (nine), intramedullary nails (two), an elastic nail (one), and external or ring fixators (four). Plates were used primarily for unstable metaphyseal fractures with significant displacement or comminution, particularly when a more rigid construct was desired near the physis. Elastic nails were used in a single case in which the fracture line extended more proximally and allowed stable intramedullary purchase while maintaining sufficient distance from the physis. Rigid intramedullary nails were reserved for older adolescents with nearly closed phyzes and more diaphyseal fracture extension, where intramedullary fixation could provide adequate stability without compromising growth. Patients received a mean of 7.1 ± 3.8 weeks of immobilization, and full weight-bearing was permitted at a mean of 5.7 ± 3.1 weeks. Residual angulation >10° was observed in five patients (31%). Three patients (18.8%) experienced complications: one required reoperation with a ring fixator, one developed skin necrosis requiring grafting, and one reported prolonged postoperative pain. For clarity, nonspecific pain has been removed as a complication. One patient in the surgical group developed prolonged neuropathic pain requiring extended medical management and follow-up, and this was classified as a complication. All patients with complications had initially been treated with K-wires. K-wires with diameters ranging from 1.6 mm to 2.0 mm were used, chosen according to the child’s bone size and cortical diameter. Following K-wire or plate fixation, all patients were initially immobilized in a long-leg cast for approximately 3–4 weeks. In the casting group in 55/70 patients were primarily treated with long leg cast and in surgical group 13/16 had long leg cast.
Risk factors for treatment failure
The complication rate was significantly higher in the primarily cast treated compared to the surgically treated (18.3% vs. 4.3%; relative risk, 4.4; 95% CI, 1.0–19.7; p = 0.042). Multivariable logistic regression identified three independent predictors of treatment failure: age >11 years (adjusted OR, 10.1; 95% CI, 1.3–81.7; p = 0.030), presence of a complete fibular fracture (adjusted OR, 6.1; 95% CI, 1.2–30.1; p = 0.027), and initial coronal angulation >10° (adjusted OR, 4.9; 95% CI, 1.1–23.0; p = 0.042). In contrast, gender, presence of varus (while the magnitude of coronal angulation (>10°) was predictive of failure, the direction did not independently affect failure risk), recurvatum deformities, and displacement >50% on initial imaging were not significantly associated with failure risk (Table 4).
Multivariate analysis of risk factors for nonoperative treatment failure.
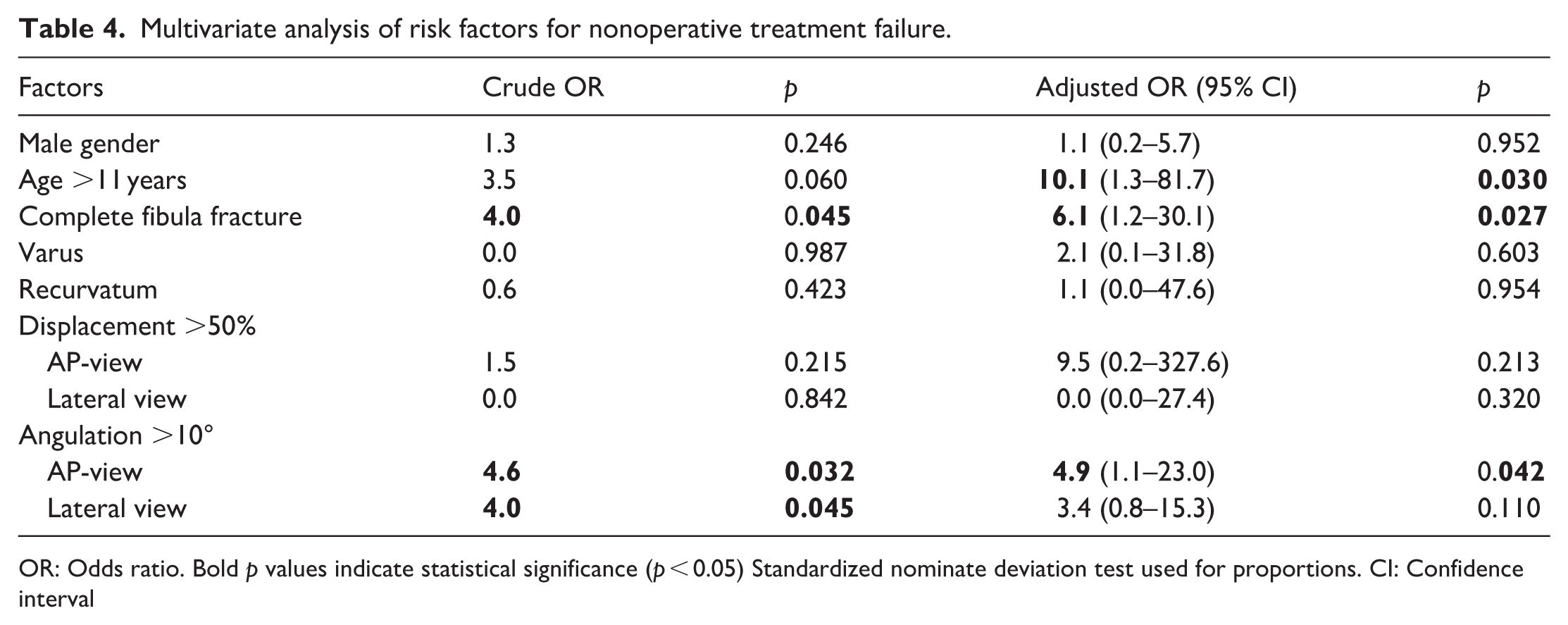
OR: Odds ratio. Bold p values indicate statistical significance (p < 0.05) Standardized nominate deviation test used for proportions. CI: Confidence interval
Discussion
This registry-based cohort study evaluated outcomes and complications following cast or surgical management of distal metaphyseal horizontal tibial fractures in children (Figure 3). A total of 86 patients were included, making this the largest study to date focused specifically on this uncommon fracture pattern in the pediatric population. The results indicate that while cast treatment is effective in most cases, certain factors such as older age, a concomitant fibular fracture, and initial coronal angulation greater than 10° significantly increase the risk of treatment failure. To the authors’ knowledge, the precise anatomical location of these fractures has not been previously described. In this cohort, most fractures were located at a relative distance of 0.3 to 0.6 from the widest dimension of the distal tibial metaphysis.
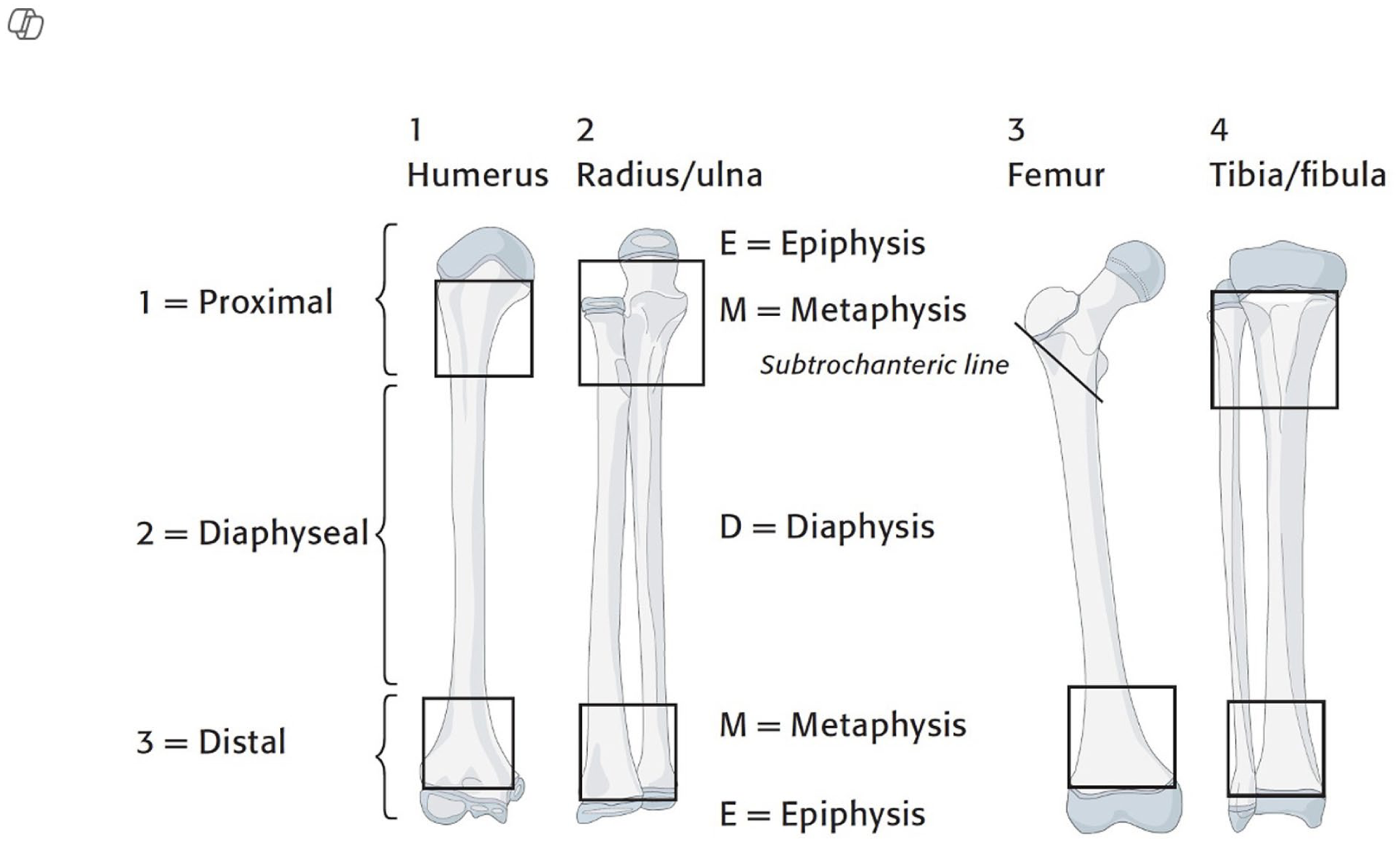
Anatomical definition of epiphysis (E), metaphysis (M), and diaphysis (D) for long bones based on AO classification principles.
Distal metaphyseal tibial fractures are less common than diaphyseal injuries, and studies specifically addressing horizontal metaphyseal patterns remain limited. Domzalski et al. 3 identified two predominant displacement patterns valgus recurvatum and varus procurvatum which were also observed in our cohort, particularly among patients with initial coronal plane angulation exceeding 10°. Although previous reports have suggested that most of these fractures heal uneventfully with cast immobilization,1,3 our findings revealed a primary treatment failure rate of nearly 55%, which is substantially higher than previously reported rates. This discrepancy may be explained by the broader inclusion of unstable fracture patterns in our nonoperative cohort. Moreover, our multivariable analysis aligns with the findings of Civan et al., 4 who reported that metaphyseal fractures with concomitant complete fibular fractures and significant angular deformities are at increased risk for delayed union and may require closer clinical follow-up. Treatment failure was defined as the requirement for cast wedging, re-reduction, or surgical intervention due to loss of reduction or >10° coronal angulation at final follow-up in the cast-treated group, and re-operation or >10° coronal angulation at final follow-up in the surgically treated group. When considering only patients initially managed nonoperatively, the failure rate was 35.3% (25/70). However, when applying the composite definition of treatment failure across both treatment groups, failure was observed in 57.1% of the cast group and 43.9% of the surgical group, resulting in an overall treatment failure rate of 54.7% (Table 2).
Failure of cast treatment defined as the need for cast wedging, re-reduction, or surgical intervention was observed in 34.3% of patients initially managed conservatively. This finding is notable, as previous literature has often suggested that cast treatment is sufficient for the majority of pediatric metaphyseal tibial fractures.4,7 Ghannam et al. 2 reported that recurrence of deformity is more likely in cases with unstable initial reduction or inadequate cast molding. In our cohort, residual angulation greater than 10° was identified in more than 20% of the cast treated cases, emphasizing the necessity of careful radiographic assessment at each follow-up visit to minimize the risk of malunion.
Three significant predictors of nonoperative treatment failure were identified in our cohort: age greater than 11 years, the presence of a complete fibular fracture, and initial anteroposterior (AP) angulation exceeding 10°. Patients older than 11 years demonstrated a tenfold increased risk of failure, likely attributable to reduced remodeling potential, as younger children are more capable of compensating for angular deformities due to ongoing skeletal growth. 8 Complete fibular fractures, which may relate to higher-energy trauma, were also associated with increased odds of treatment failure. This finding is consistent with previous reports by Rohilla et al., 9 who linked complete fibular fractures to greater rotational instability in distal tibial fractures. Furthermore, initial AP angulation greater than 10° was independently predictive of failure, reinforcing the recommendations of the AO-PCCF, which emphasize that fractures exceeding acceptable alignment thresholds should be corrected or surgically stabilized (Figure 4). 10
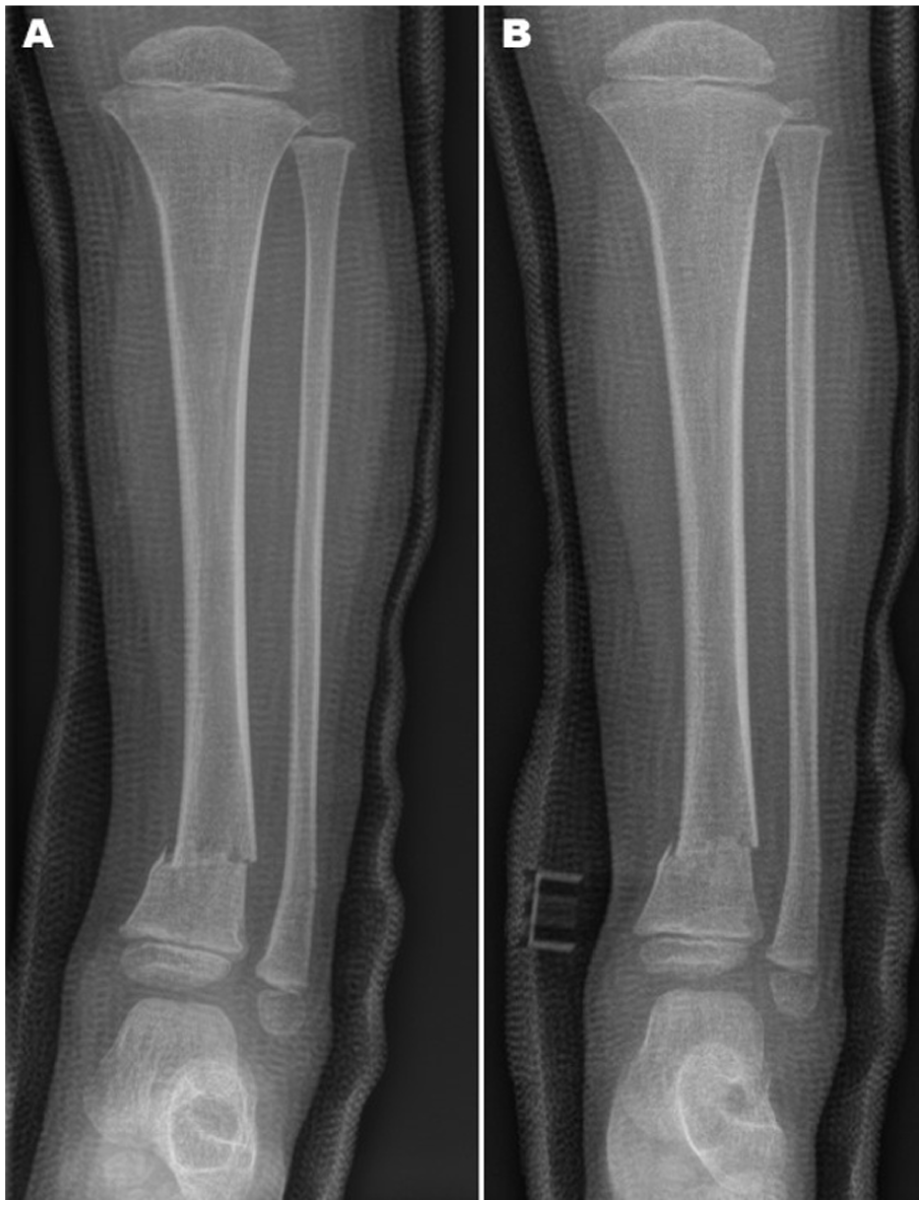
Three-year-old male with a distal metaphyseal horizontal tibial fracture initially treated with a long-leg cast.
The surgically treated subgroup primarily underwent fixation with plates and K-wires and experienced a complication rate of 18.8%, which was significantly higher than that observed in the cast treated patients (4.3%). Although the difference in complication types did not reach statistical significance, complications such as skin necrosis, nerve injuries, and loss of reduction underscore the potential morbidity associated with surgical intervention but may also indicate higher energy of surgically treated fractures (Figure 5).
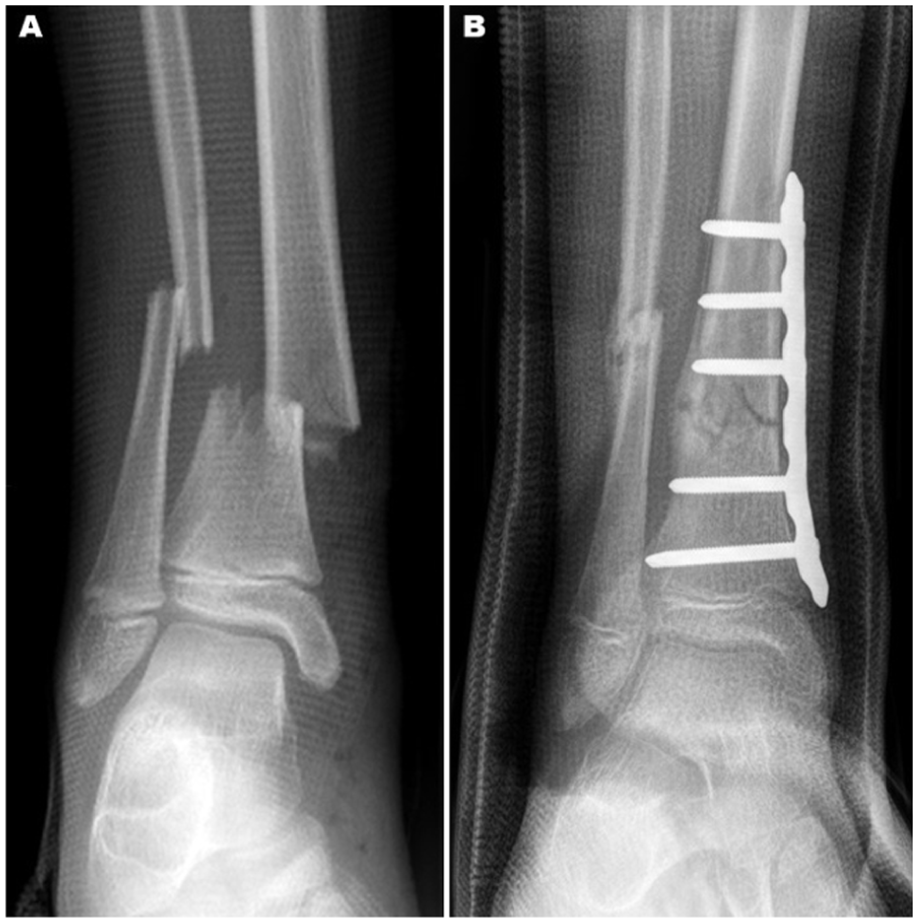
Nine-year-old female patient presenting with a comminuted distal metaphyseal horizontal tibial fracture.
The strengths of this study include relatively large sample size, and the application of robust multivariate analysis. However, several limitations must be acknowledged. The retrospective design inherently introduces risks of selection and information bias. Additionally, the absence of standardized functional outcome measures limits the ability to assess long-term results comprehensively. Lastly, variability in casting techniques and surgical expertise among treating physicians may have influenced patient outcomes.
Future prospective studies with longer follow-up durations and incorporation of patient-reported outcome measures are warranted to better elucidate the long-term consequences of malalignment and the need for reoperation. Cast treatment remains the standard initial approach for many distal metaphyseal tibial fractures in children. Our findings do not suggest that all patients with risk factors (older age, fibular fracture, >10° angulation) should automatically undergo primary surgery. Instead, our intention is to highlight that these three factors identify a subgroup at higher risk of failure with cast treatment: We have revised the conclusion to state that such patients “may benefit from early surgical consideration” rather than implying mandatory primary surgery. Additionally, the development and implementation of standardized treatment protocols, such as clearly defined surgical indications and thresholds for cast wedging, may improve the consistency and quality of clinical outcomes.
Conclusion
This study confirms that while cast management remains the standard of care for pediatric distal metaphyseal tibial fractures, older age, concomitant fibular fracture, and initial coronal angulation greater than 10° substantially increase the risk of treatment failure. Early identification of these risk factors and appropriately tailored management may help prevent complications, malunion, and reoperation, ultimately improving clinical outcomes in this patient population.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261436703 – Supplemental material for Distal metaphyseal horizontal tibial fractures in children
Supplemental material, sj-pdf-1-cho-10.1177_18632521261436703 for Distal metaphyseal horizontal tibial fractures in children by Halil Kara, Maija Jääskelä, Topi Laaksonen, Petra Grahn, Ilkka Helenius and Matti Mikael Ahonen in Journal of Children's Orthopaedics
Footnotes
Author contributions
Halil Kara: Data analysis or interpretation, Data collection, Drafting the manuscript, Literature review
Maija Jääskelä: Data analysis or interpretation, Data collection, Drafting the manuscript, Literature review
Topi Laaksonen: Critical revision, Study conception and design, Supervision or final approval
Petra Grahn: Critical revision, Study conception and design, Supervision or final approval
Ilkka Helenius: Critical revision, Study conception and design, Supervision or final approval
Matti Mikael Ahonen: Critical revision, Study conception and design, Supervision or final approval
Data availability statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.*
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical statement
The institutional review board approved the study protocol and waived the requirement for individual informed consent because the study used de-identified retrospective data.
(HUS/564/2024).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.