
Abstract
Purpose:
Rickets is a condition characterized by a defective mineralization on the epiphyseal plate, either in the form of nutritional or congenital hypophosphatemic rickets, which could lead to progressive bone deformity. One of said deformities is angular growth of the knee which can cause permanent disfigurement. Hemiepiphysiodesis is a surgical option to correct the deformity, yet the studies evaluating its results are rare. This review aimed to map the literature pertaining to this topic.
Methods:
A comprehensive search was performed across five databases: Pubmed, Cochrane, ProQuest, Embase, and Science Direct to identify studies involving children with rickets treated with hemiepiphysiodesis. Risk of bias was assessed using the Joanna Briggs Institute Critical Appraisal Tool, and the outcome data were compiled.
Results:
Six studies fulfilled the inclusion and exclusion criteria of this study with highly varied groupings and outcomes. However, the risk of bias of all studies was low to moderate. Hemiepiphysiodesis showed good outcome in function, radiological parameter, and correction rate with lower complication rate compared to osteotomy. The average time required to achieve full deformity correction was within 10.8–22.7 months. However, hemiepiphysiodesis has a risk of overshooting the correction or paradoxically rebounding to the prior condition, therefore, requiring routine follow-up.
Conclusion:
Hemiepiphysiodesis is beneficial for the correction of angular deformities in the knee due to rickets.
Significant of studies:
This review provides a crucial evidence base for clinicians by establishing hemiepiphysiodesis as a viable, less invasive alternative to osteotomy.
Introduction
Rickets is a condition characterized by a defective mineralization on the epiphyseal plate, either in the form of nutritional or congenital hypophosphatemic rickets, which could lead to progressive bone deformity. 1 Despite increased coverage in vitamin D, phosphate, and calcium supplementation, the prevalence of rickets has been increasing especially in developing African, Middle Eastern, or Asian countries. 2 Surgical treatment is usually reserved for the most severe form of rickets; especially in cases where skeletal deformity has already manifested. 1 One of the most devastating skeletal complication is angular deformity of the knee causing reduced function, mobility, and possible social seclusion.1,2
Treatment option to correct the angular limb deformity secondary to rickets includes bracing, acute osteotomy, and hemiepiphysiodesis or also commonly known as guided growth or growth modulation. 3 Hemiepiphysiodesis involves temporarily restraining growth on one side of a bone’s growth plate. 3 By doing so, the opposite, unrestrained side continues to grow, gradually straightening the limb over time. Various devices can be used for this “guided growth” technique, including staples, percutaneous transphyseal screws, and tension band plates (TBP) like the eight-plate. 4 This method is often preferred over more invasive options like osteotomies due to lower morbidity and fewer complications. 5
However, studies focusing on hemiepiphysiodesis in rickets are limited and there have been no consensus regarding when to use hemiepiphysiodesis, acute osteotomy, or conservative treatment. Data regarding correction rate, complication rate, functional outcomes, and possible complications are needed to guide the timing and the method of the intervention. 5 It should also be noted that hemiepiphysiodesis can also be used in conjunction with other treatment methods including osteotomies and conservative treatment such as pharmacological and physical rehabilitation. This study aims to evaluate hemiepiphysiodesis in rickets and its subsequent outcome to guide treatment in this rare condition.
Methods
This is a systematic review evaluating the outcomes of hemiephiphysiodesis in the treatment of rickets (PRISMA 2009 hemiephiphysiodesis rickets in supplemental material online). The protocol for this study has been registered in the International Prospective Register of Systematic Review under the submission CRD420261279447. This manuscript is reported based on the Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) Guidelines. 6
Eligibility criteria
Types of studies
We only included primary, full-text studies including trials and observational studies. Data from abstracts, proceeding, gray literatures, case reports, and review articles were excluded. Data from full text which were not written in English were also excluded from this review.
Types of participants
This review included patients with rickets either caused by nutritional or genetic etiologies (e.g. X-linked hypophosphatemic (XLH)), treated with hemiepiphysiodesis without regard on the form of deformity (genu varum, genu valgum, etc.) and the type of hemiepiphysiodesis (TBP, transepiphyseal screws, Blount staples, etc.). By nature of the treatment, the participants will be children with active growth plates. All nonhuman studies were excluded.
Information sources
We performed comprehensive search through several databases including PubMed, CENTRAL, Proquest, ScienceDirect, and SCOPUS. No limitation was applied regarding publication year. However, we excluded on-going trials, reviews, and case-reports. Reference lists from studies found were also hand-searched for related studies.
Search strategy
We used a combination of the keywords and their synonyms as the basis of our search strategy: “Hemiepiphysiodesis”; “Guided growth”; “Growth modulation”; “Rickets”; and “Rachitis.” Where possible, we used MeSH keyword and exploded all branches. If MeSH term for the keyword was unavailable, we included each synonym manually with special care for different spelling. The complete search strategy was included in the Appendix 1.
Selection process
Authors in pairs independently screened studies for inclusion in the review including all articles in which hemiepiphysiodesis is used as treatment for rickets. The screening was based on titles and abstracts, followed by a full-text evaluation. Disagreements are resolved by discussion or, if necessary, by a third author. The selection process was recorded in a PRISMA flow diagram (Figure 1).
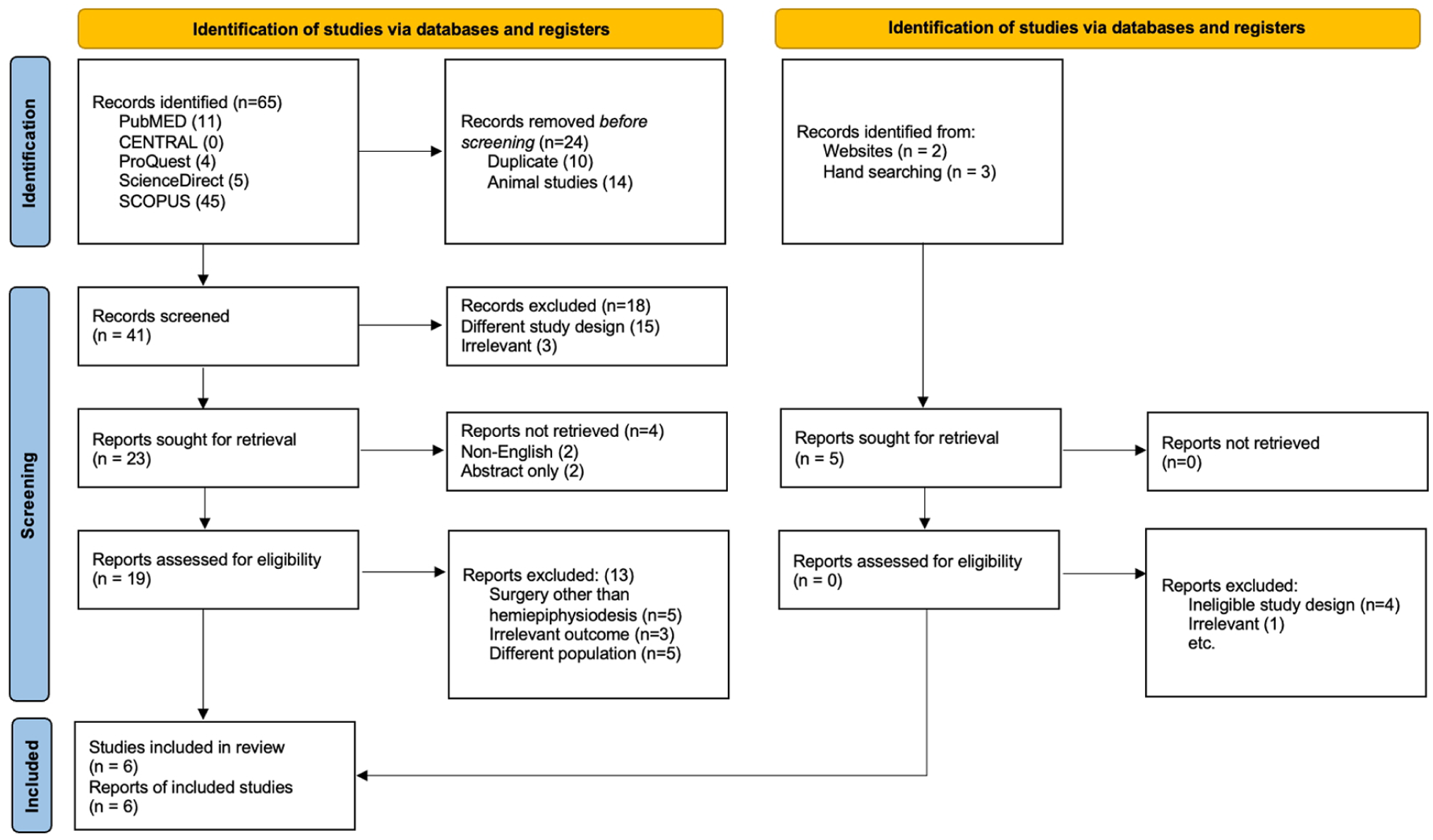
PRISMA flowchart. 6
Data collection process
Data were extracted independently by two different authors using the same form that denotes the characteristics and results of each studies. All disagreements were resolved by discussion or by a third author. Due to the limited pool of studies found in our preliminary search, we decided to include all types of outcomes and outcome measurements.
Assessment of risk of bias in included studies
The risk of bias was assessed by a pair of authors using Joanna Briggs Institute’s Critical Appraisal Tool (JBI-CAT). All disagreements are resolved through discussion or, if needed, by a third author.
Reporting results of included studies
All outcomes are reported in a summary of studies table. If possible, data from at least two similar studies are compiled. If there are no similar studies, data will be presented as is with possible comparison to studies from different etiologies or treatments in the discussion. We contacted original study authors to account for the missing data from individual studies.
Certainty of evidence
All evidence found are evaluated by each author until a consensus was made regarding the certainty of evidence.
Results
Study selection
The systematic search was done on September 23, 2025 using predefined keywords. From the databases, we identified 65 studies and an additional 5 records were identified through other methods, including websites (n = 2) and hand searching (n = 3). Out of those, 10 duplicate records and 14 animal studies were removed automatically. We screened 41 studies manually and sought 23 reports for full-text assessment. Of the 23 articles sought, 19 were retrieved, while 2 were non-English and 2 abstract only articles were excluded. The successfully retrieved articles went through a rigorous full-text assessment, in which 13 studies were excluded for failing to meet the inclusion criteria. All five reports from other methods were retrieved but were subsequently excluded during eligibility assessment due to ineligible study design (n = 4) and irrelevance (n = 1). Finally, six articles were included in this review.
Study characteristics
This study included six studies (Table 1).7–12 Studies found are mostly from cohort study design except from one study 7 , which is a cross-sectional study. Most of the studies used tension band plate with two studies using staples transitioning from staples to tension band plate by the end of each study.8,12
Characteristics of included articles.
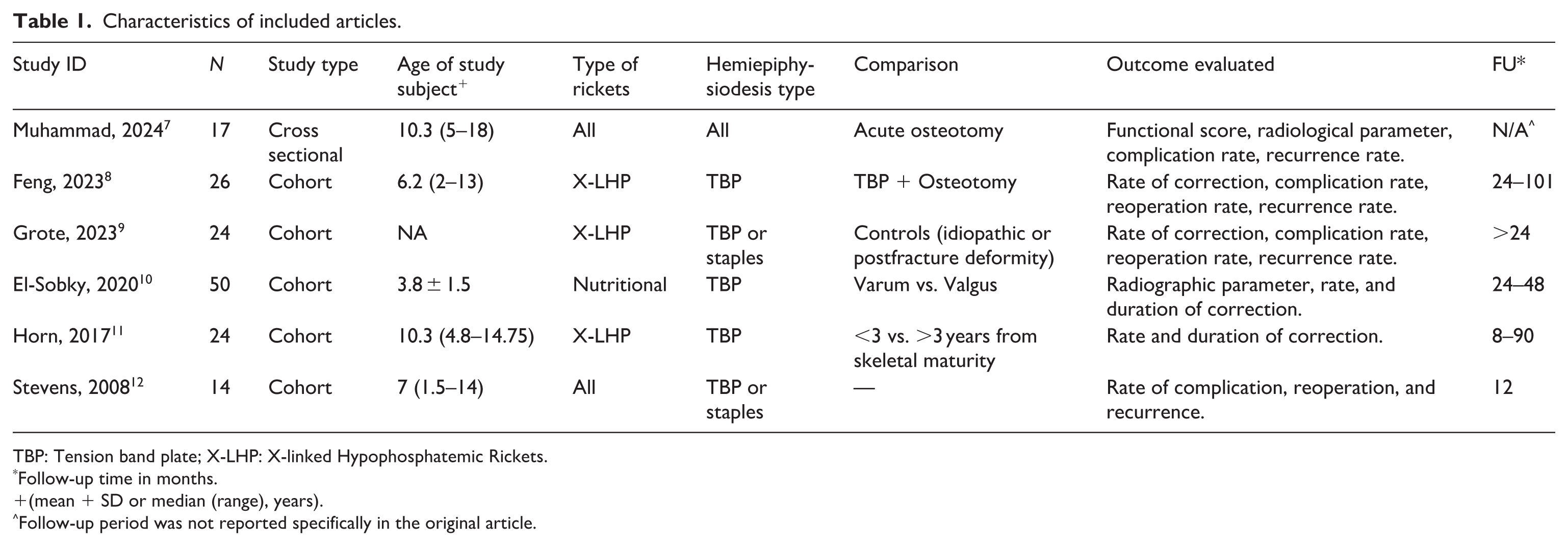
TBP: Tension band plate; X-LHP: X-linked Hypophosphatemic Rickets.
Follow-up time in months.
(mean + SD or median (range), years).
Follow-up period was not reported specifically in the original article.
Risk of bias in studies
Risk of bias assessment was done using the JBI CAT for cohort or case control. A summary of the risk of bias assessment is included in Figure 2. We can observe that the studies had low to moderate risk of bias.
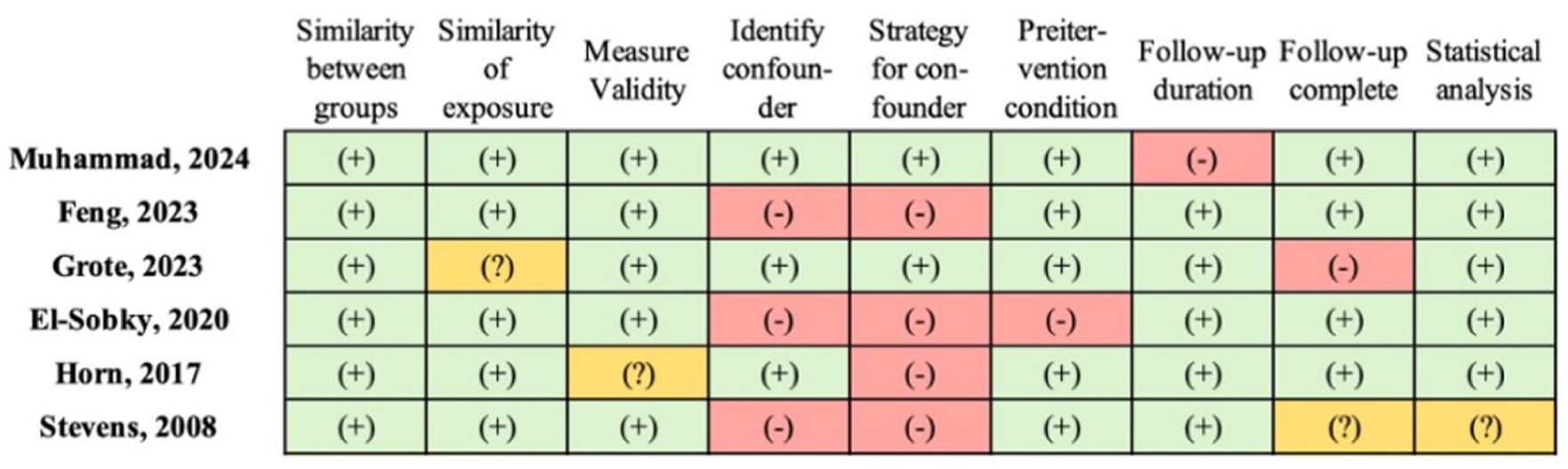
Risk of bias of included studies according to the JBI-CAT.
Synthesis of results
Functional score
Only one study evaluated the functional outcome after hemiepiphysiodesis. 7 Two instruments were used: the Active Scale for Kids and the Lower Extremity Functional Scale (LEFS). All patients reported satisfactory functional scores. However, an interesting observation is that Guided Growth showed better, albeit insignificant, functional outcomes than acute osteotomy (LEFS: 92.40 ± 6.77 vs. 85.79 ± 3.85; p-value: 0,056). 7
Radiological parameters
Tibiofemoral angle
Two studies included reported improvement on tibiofemoral angle (TFA) in patients who underwent guided growth surgery (GGS). Muhammad et al., 7 when comparing GGS with acute corrective osteotomy (ACO), reported greater changes of TFA in GGS group, albeit not statistically significant. When comparing between varus and valgum deformity on nutritional rickets patients who were subjected to temporary hemiepiphysiodesis using a two-hole eight-plate, El-Sobky et al. 10 reported notable improvements of TFA at the final follow-up on both groups.
Mechanical axis deviation
Across the three studies, the measurement and interpretation of mechanical axis deviation (MAD) were consistent in concept but differed in methodological detail and reporting style (Table 2). Grote et al., 9 studied patients with X-linked hypophosphatemic rickets (X-LHPR), adopted the knee zone classification previously described by Stevens et al. 13 to evaluate MAD. The study found that initial MAD did not significantly differ between XLH and control groups, but XLH patients were less likely to end treatment in zone 1 (55.0% vs. 77.8%). El-Sobky et al. 10 applied a more quantitative approach, defining MAD as the distance between the mechanical axis and the midpoint of the tibial epiphysis, expressed as a percentage of one-half of the tibial epiphyseal width. The study demonstrated significant postoperative improvement in MAD, with most limbs achieving alignment within the central one-third zone (no significant difference between varus and valgum deformities). In contrast, Stevens et al. 12 applied a more qualitative approach. In their study, MAD was defined as lateral or medial displacement of the mechanical axis relative to the center of the knee joint in standing anteroposterior radiographs. The authors reported qualitative improvements, with most patients achieving a neutral or near-neutral mechanical axis after guided growth, though specific numerical MAD values were not provided.
Summary findings on MAD.
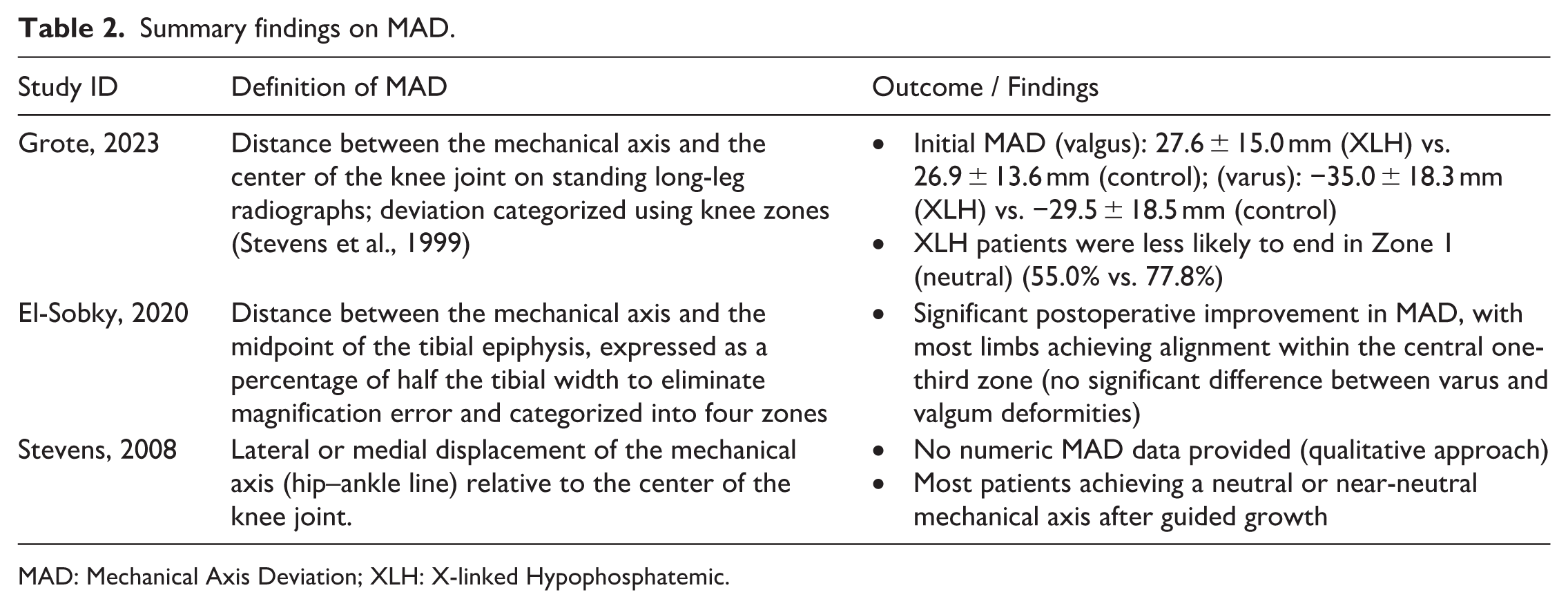
MAD: Mechanical Axis Deviation; XLH: X-linked Hypophosphatemic.
Mechanical lateral distal femoral angle
Four of six included studies used the mechanical lateral distal femoral angle (mLDFA) as a radiographic outcome measure to assess the correction of distal femoral deformity after guided growth (Table 3). The definition of mLDFA was consistent across studies, referring to the lateral angle between the mechanical axis of the femur and the distal femoral joint line. However, the means of reporting this outcome were varied between studies.
Summary findings on mLDFA.
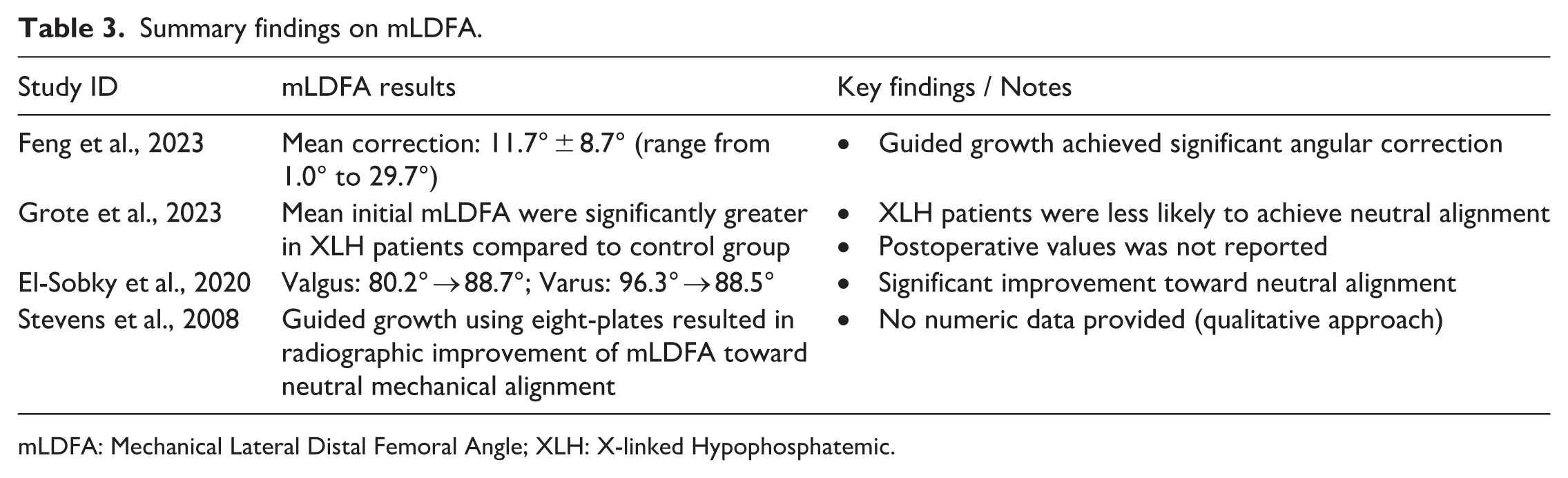
mLDFA: Mechanical Lateral Distal Femoral Angle; XLH: X-linked Hypophosphatemic.
Feng et al 8 reported the average mLDFA correction was 11.7° ± 8.7° (range from 1.0° to 29.7°) in their study subjects, whereas Grote et al. 9 reported that the mean initial mLDFA were significantly greater in XLH patients compared to control group. In Stevens et al., 12 guided growth using eight-plates resulted in radiographic improvement of mLDFA toward neutral mechanical alignment, though exact numeric outcomes were not specified. El-Sobky et al. 10 quantified the change, reporting that mLDFA improved from 80.2° to 88.7° in valgus deformities and from 96.3° to 88.5° in varus deformities with most patients achieving near-normal alignment.
Mechanical medial proximal tibial angle
Four studies consistently reported the medial proximal tibial angle (MPTA) (or mechanical MPTA) as a radiographic measure to assess tibial alignment correction following guided growth procedures (Table 4). It was defined as the angle between the mechanical axis of the tibia and the tibial plateau.
Summary findings on MPTA.
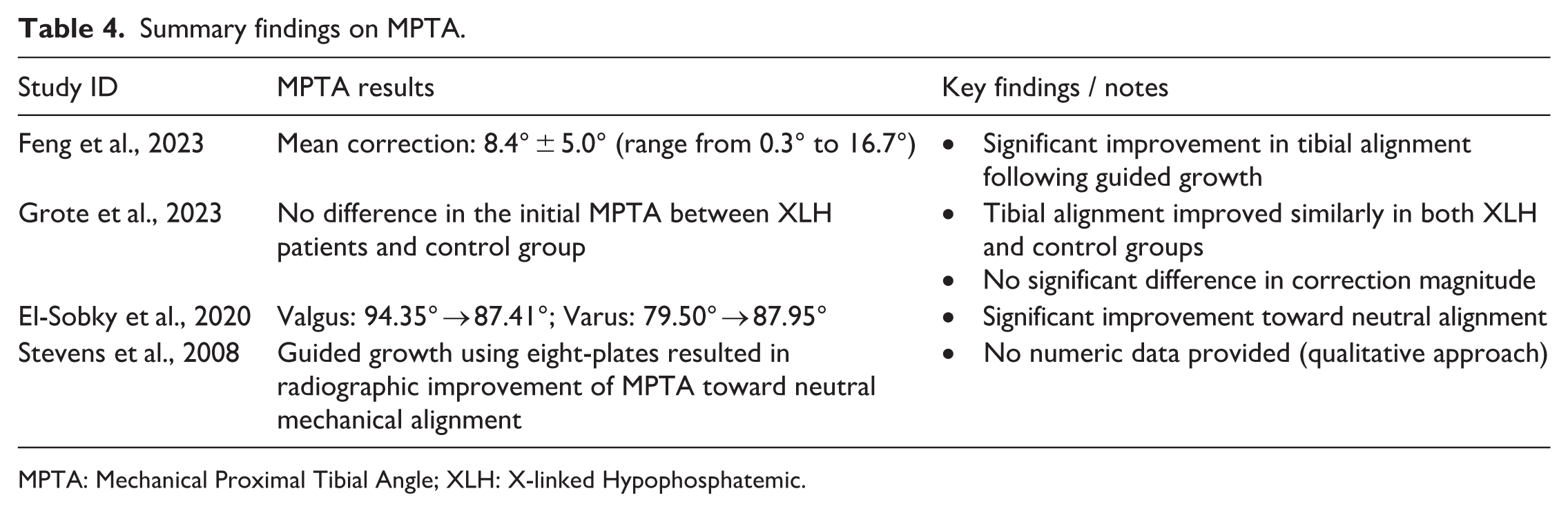
MPTA: Mechanical Proximal Tibial Angle; XLH: X-linked Hypophosphatemic.
Feng et al. 8 reported the mean MPTA correction was 8.4° ± 5.0° (range from 0.3° to 16.7°), whereas Grote et al. 9 reported no difference in the initial MPTA between XLH patients and control group. El-Sobky et al. 10 showed MPTA improvement from about 94.35° to 87.41° in valgus knees and 79.50°–87.95° in varus knees in nutritional rickets. Lastly, Stevens et al. 12 described radiographic improvement of MPTA toward normal in patients treated with guided growth procedure using staples or eight-plates, though numerical data were not detailed.
Success rate and correction rate/velocity
Muhammad et al. 7 reported no significant difference in terms of correction success rate in hemiepiphysiodesis or GGS compared to ACO (87.5% vs. 71.4%, respectively). Similar result were also reported by Feng et al. 8 (76.9%), using an eight-plate for temporary hemiepiphysiodesis for X-LHPR children. Horn et al. 11 reported 65% of their study subjects achieved a neutral limb alignment with guided growth, with younger cohorts (>3 years from skeletal maturity) showed a higher rate of successful mechanical restoration than the older cohorts (90% vs. 30%, respectively). Also, those with varus deformity had significantly less satisfactory outcome than those with valgus deformity (53% vs. 100%, respectively).
The rate of angular correction is consistently shown to be dependent on the patient’s age, with younger children demonstrating a faster correction. 9 Feng et al. 8 reported the correction speed of the mLDFA and mMPTA of patients whose age 5 years old was faster than that whose age >5 years old, while Horn et al. 11 showed that significantly greater rates of correction at the operated physes were seen in the younger age group. After adjustment for age, Grote et al. 9 reported that XLH patients tend to correct at a 15%–36% slower rate than control patients for the distal femur mLDFA (whereas no significant difference on MPTA). The rate of correction have also been shown to differ between anatomical sites, with femoral indices improved at significantly faster rate than tibial indices.8,11
The average time required to achieve full deformity correction with guided growth varied between studies, with mean durations ranging from 10.8 months to 22.7 months.8–11 Grote et al. compared patients with XLH to a control group and found that XLH patients required significantly longer treatment times (19.5 months) than the control group (12.6 months) to achieve correction. 9
Rate of complication, reoperation, and recurrence
The overall complication rate for guided growth procedures in patients with rickets was reported to be low and tolerable.9,10 The most frequently cited hardware-related issue was screw loosening or staple migration. In Stevens et al.’s study, 10 of 14 patients underwent a total of 53 stapling procedures. Among the total procedures, staples migrations were found in 45% of them (24 of 53), but this problem was averted by switching to 8-plates, which had no instances of migration. 12 A direct comparison between GGS and ACO found no complications in the GGS group, while the ACO group had cases of neurovascular injury and implant failure. 7 Overcorrection was also identified as a complication, particularly when follow-up appointments were missed.9,10
The rate of deformity recurrence, or rebound, after implant removal showed considerable variability. Feng et al. 8 reported a rebound phenomenon in just one patient (3.8%), whereas Stevens et al. 12 using staples noted a rebound growth rate as high as 41%. A comparative study found recurrence rates of 37.5% in the GGS group and 28.6% in the ACO group. 7 Horn et al., reported only a single case of recurrent deformity in their cohorts of patients with X-linked hypophosphataemic rickets.9,10
The necessity for a more invasive osteotomy following a failed guided growth procedure was an important concern of the studies. The rate of subsequent osteotomy ranged from a single patient in one series to 37.5% in a cohort of patients with XLH.8,9,11 Patients with XLH also required a higher average number of secondary procedures compared to controls. 9 In another study, 30.8% of patients underwent a revision of their eight-plates, which in some cases was due to a long implant retention time rather than a failure of the device. 8
Discussion
Summary of main results
Our study found that hemiepiphysiodesis is a valid treatment in rickets with good functional and radiological outcome.7,9,10 However, patients with XLH were found to be more prone to MAD, recurrence, and slower correction in comparison to other types of rickets or other causes of angular deformity. 9 The rate of angular correction is consistently shown to be dependent on the patient’s age relating to the end of growth. 9 The average time for correction varied 10.8 months–22.7 months with overcorrection being a risk factor if follow-up appointments are missed.8–10
This high success rate, albeit with slower correction time, is also validated by the overall complication rates which are reported to be low and tolerable.9,10 Staples are found to have a larger rate of complication in comparison to the tension band plate. 12 However, both method are shown to still be better than ACO in terms of neurovascular injury and implant failure. 7 The rate of deformity recurrence, or rebound, after implant removal showed considerable variability. This high variability is coupled with the high variability of subsequent osteotomy.8,9,11 However, it has been shown that patients with XLH required a higher average number of secondary procedures compared to controls. 9
As shown in previous studies, hemiepiphysiodesis is an effective procedure for correcting angular deformities. However, other studies found that success of intervention is significantly higher in patients with idiopathic deformities (82.1%) compared to those with nonidiopathic conditions like rickets or Blount disease (44%). 14 Studies focusing on rickets report complete correction rates of only 76.9% in patients with X-LHPR and only half achieving a neutral mechanical axis.8,9 In contrast, studies on idiopathic genu valgum report that nearly all patients respond well to treatment, with all radiographic parameters showing significant correction.3,15 A direct comparison found that patients with X-LHPR correct femoral deformities at a 15%–36% slower rate than a control group with idiopathic or posttraumatic deformities. 9
The complication rate for hemiepiphysiodesis is generally low across different etiologies. For patients with rickets, reported complications include screw loosening (7.7%–16%) and, rarely, screw breakage (2%), with one study noting zero complications.8,10 In comparison, cohorts with idiopathic genu valgum have also reported no major complications or a low rate of complications requiring further surgery (2.8%). 3 As mentioned before, the rebound phenomenon is higher in non-idiopathic rickets such as Blount disease and Rickets. For idiopathic genu valgum, recurrence rates of 3.7%–3.8% have been documented. 16 In comparison, in a cohort including Blount disease, 52% of limbs experienced a rebound of more than 5°. Specifically for rickets, recurrence rates have been reported as high as 37.5% and as low as 2%–3.8%. 10 However, this finding must be taken in with a grain of salt due to the difference between studies.
Limitations of the study
The studies included in this present review demonstrated considerable heterogeneity in terms of study populations, research design, reported outcomes, and the specific techniques of hemiepiphysiodesis employed. Therefore, the comparability of each studies is limited. As a result, the conclusions drawn from this review should be interpreted with caution, as differences in methodology and patient characteristics may have influenced the reported outcomes. We also excluded studies non-English studies which may be a source of bias.
Using a catch-all search strategy, we conducted a large-scale literature search in multiple databases. However, hemiepiphysiodesis is a complex treatment with multiple factors contributing to its success or failure. Therefore, this review might not completely encompass all the possible factors such as the etiology of rickets, nutrition and supplementation, or physical rehabilitation.
Furthermore, there has been no studies comparing the hemiepiphysiodesis technique with other techniques.
Implications for practice and future research
In this review, we highlighted the importance of the deformity correction in rickets since static and dynamic posture assessments may be negatively impacted by moderate-to-severe valgus and varus knee abnormalities.17,18 Hemiepiphysiodesis aims to improve lower limb biomechanical parameters in addition to correcting deformities and relieving discomfort.17,18 Joint instability, muscular weakness, range of motion restrictions, discomfort, meniscal injury, and ligament laxity are all consequences of lower limb abnormalities that can negatively impact balance and body weight distribution.17,18 Maintaining postural control requires a normal distribution of lower limb loads.17,18 Hemiepiphysiodesis is intended to improve body weight distribution and balance by partially or fully correcting valgus or varus knee deformity.17,18 Hemiepiphysiodesis aids in the restoration of the lower limb’s normal mechanical axis, which should enhances the biomechanical characteristics of the lower limb, especially static parameters.17,18
This is the first systematic review done to date focusing on rickets as a target for hemiepiphysiodesis. The systematic review was done rigorously. We included all articles pertaining to this topic. However, due to limited amount of studies, we are unable to make a proper recommendation from the result of this study. Patients undergoing hemiepiphysiodesis for rickets is still corrected, although the treatment might confer less benefit than for other causes of angular deformity of the knees.
This study highlights the limited number of primary studies focusing on hemiepiphysiodesis for rickets. Additional studies such as clinical trials or prospective cohort have an opportunity to contribute in this research area. Subsequent research are severely needed especially studies which compare hemiepiphysiodesis to other treatments or compare hemiepiphysiodesis techniques.
Conclusion
Our review found that hemiepiphysiodesis is an option for the correction of angular deformities in the knee due to rickets. Different etiologies of rickets responded differently to hemiepiphysiodesis with X-LHPR having the worst outcome; albeit still improved from the initial condition. The extent of the benefit of hemiepiphysiodesis and comparison to other mode of treatment still necessitates further research.
Supplemental Material
sj-doc-2-cho-10.1177_18632521261444934 – Supplemental material for Outcomes of hemiepiphysiodesis on lower limb deformities due to rickets: A systematic review
Supplemental material, sj-doc-2-cho-10.1177_18632521261444934 for Outcomes of hemiepiphysiodesis on lower limb deformities due to rickets: A systematic review by M Deryl Ivansyah, Aryadi Kurniawan and Ari Wibowo in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261444934 – Supplemental material for Outcomes of hemiepiphysiodesis on lower limb deformities due to rickets: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521261444934 for Outcomes of hemiepiphysiodesis on lower limb deformities due to rickets: A systematic review by M Deryl Ivansyah, Aryadi Kurniawan and Ari Wibowo in Journal of Children's Orthopaedics
Footnotes
Appendix 1
Author contributions
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research is funded by the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science, and Technology.
Ethical considerations
This study did not involve human participants or animals; therefore, ethical approval was not required.
Data availability
All data analyzed during this study are available from the corresponding author upon reasonable request.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.