
Abstract
Background:
Growth-related complications are a concern in skeletally immature patients undergoing anterior cruciate ligament reconstruction (ACLR). Reported outcomes of growth disturbances following ACLR in this population are heterogeneous.
Purpose:
We hypothesized that transphyseal ACLR performed with a standardized technique results in mild radiological, but clinically non-significant growth disturbances.
Methods:
This single-center study prospectively enrolled 50 patients with open growth plates undergoing transphyseal ACLR. Magnetic resonance imaging of the operated knee was performed preoperatively and at 6, 12, 24, and 60 months postoperatively. Growth-related outcomes included tibial and femoral physeal-diaphyseal angles in coronal and sagittal planes, Harris growth arrest line deviation, focal physeal bone bridge formation, physeal violation by tunnels, skeletal maturity, and premature physeal closure. Growth disturbances were also evaluated clinically.
Results:
Sixteen patients completed the 60-month follow-up. Eighty-seven point five percent had reached skeletal maturity by then. Physeal–diaphyseal angles remained stable over time, with no significant differences between preoperative and 60-month measurements (medial tibial physeal angle, p-value = 0.20; lateral femoral physeal angle, p-value = 0.91; posterior tibial physeal angle, p-value = 0.16; posterior femoral physeal angle, p-value = 0.30). Angular deviations (≥ ±5°) were identified in 37.5% of cases, but were minimal (max −6° and + 5°) and clinically insignificant. Bone bridges were observed in three patients (18.8%) and resolved spontaneously. No premature physeal closure or Harris growth arrest line deviation was identified. Mean physeal violation was minimal.
Significance of Study:
This study supports the safety of transphyseal ACLR in skeletally immature patients.
Conclusions:
Transphyseal ACLR in skeletally immature patients appears to be associated with minimal physeal injury and a low risk of clinically relevant growth disturbances.
Level of Evidence:
IV, Retrospective case series of prospectively enrolled patients.
Introduction
Over the past decades, the incidence of anterior cruciate ligament (ACL) injuries and reconstructions (ACLR) among children and adolescents has risen notably,1,2 largely attributed to greater participation in high-level sports and early involvement in athletic activities.3–5 Early surgical intervention is commonly advocated to restore knee stability and prevent secondary injuries.6–9 Growth-related complications remain a major concern in pediatric ACLR, as iatrogenic damage to the growth plate may result in angular deformities (AD) or leg length discrepancy (LLD). Chotel identified three types of growth disturbances. 10 Type A (Arrest): growth stoppage that occurs when a specific area of the growth plate is damaged, leading to the formation of a bone bridge that spans across the physis. Type B (Boost): accelerated growth thought to stem from increased local blood supply, which stimulates the still-open growth plate. Type C (deCelerate): slowed growth pattern caused by a “tenoepiphysiodesis” mechanism or excessive graft tension, producing a deformity.
Pediatric-specific techniques were developed to address both anatomical and developmental characteristics of young patients, aiming to minimize damage to the growth plate. To date, no technique has shown clear superiority over the others.7,8,11–13 Previous studies assessing growth disturbances after ACLR reported heterogeneous outcomes.14–17 Most assessments of growth disturbances rely on radiographic measurements or clinical examination, which may lack the sensitivity to detect subtle physeal abnormalities. Magnetic resonance imaging (MRI) is considered the modality of choice, especially in adolescents approaching skeletal maturity, for precise evaluation of physeal integrity. 18 It is considered a reliable modality for assessing skeletal maturity19–21 and physeal closure, with consensus building and training.22,23 Angular deviations are already known to be reproducibly measured on radiographs, 24 and their reliability on MRI has been validated in the coronal plane. 25
The present study aims to evaluate the presence of growth abnormalities on MRI up to 5 years post-surgery in growing patients who underwent surgery using a transphyseal technique. We hypothesize that clinically relevant growth disturbances are rare in this population, thereby supporting the safety of this technique in pediatric ACL surgery. To our knowledge, this is the first study to investigate growth-related changes by MRI with such an extended follow-up.
Methods
A single-center study was carried out, enrolling prospectively 50 consecutive patients. Ethical approval was granted by the local ethics committee.
Inclusion criteria
Surgery was performed on patients aged 6–16 years.
Symptomatic ACL rupture confirmed by MRI
Radiographic evidence of open growth plates on anteroposterior knee X-rays
Exclusion criteria
Previous surgeries on knee ligaments, joint infections, and inflammatory conditions
ACL tears or re-tears occurring during the follow-up period
Surgical procedure and postoperative care
Skeletal maturity was assessed using knee radiographs, and Tanner staging was evaluated at the time of surgery. All patients underwent the same surgical procedure, performed by two fellowship-trained pediatric orthopedic surgeons specialized in knee ligament reconstruction.14,26,27 The semitendinosus tendon was harvested, quadrupled (ST4), and fixed with adjustable suspensory devices, tensioned at 250 N for 15 min. Standard diagnostic arthroscopy addressed any associated intra-articular lesions. Using a Howell guide, 28 the tibial tunnel was created first, with the knee positioned in full extension, initially forming a 4.5 mm transphyseal tunnel with a transphyseal straight guide wire. Then, a 10-mm-deep intra-epiphyseal socket, sized to the graft, was drilled manually with a retrograde reamer. This ensured a 3 mm safety margin, as the epiphyseal height in prepubescent patients is at least 13 mm. 29 The femoral guide was inserted via the anteromedial portal (positioned just medial to the patellar tendon to prevent injury to the medial condyle during femoral socket reaming), with the knee flexed at approximately 120°. A 10-mm-deep transphyseal socket was then slowly reamed to match the graft diameter, followed by a 4.5 mm transphyseal transfixing tunnel. The graft was introduced through the anteromedial portal, tensioned to fully occupy the transphyseal femoral socket, and secured with an adjustable suspensory fixation device. The tibial suspensory button was then retrieved retrogradely and fixed on the medial tibial cortex with the knee flexed at 20°. Correct graft positioning and tension were confirmed arthroscopically. Physical therapy was conducted on an outpatient basis, following a written protocol, and started immediately. Patient follow-up occurred at five time points: preoperatively and postoperatively at 6, 12, 24, and 60 months.
MRI and clinical follow-up
Growth disturbances were evaluated by comparing preoperative and follow-up MRIs, including at least coronal and sagittal sequences, obtained at 6, 12, 24, and 60 months after ACLR. MRI was performed exclusively on the operated limb. Two pediatric radiologists independently assessed all MRI parameters.
Primary outcome
Tibial and femoral physeal-diaphyseal angles in coronal and sagittal planes were evaluated at all time points. These were defined as the angles between the growth plate and the longitudinal axis of each bone in each midsectional plane, respectively (Figure 1).
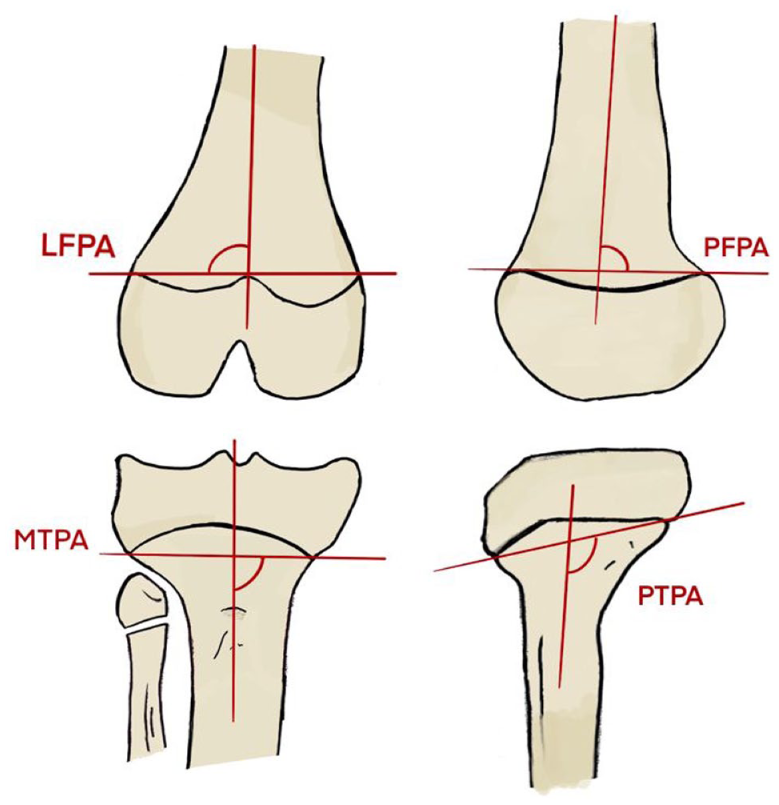
Coronal plane: LFPA: angle between the femoral growth plate and the longitudinal femoral axis. MTPA: angle between the tibial growth plate and the longitudinal tibial axis. Sagittal plane: PFPA: angle between the femoral growth plate and the longitudinal femoral axis. PTPA: angle between the tibial growth plate and the longitudinal tibial axis. LFPA: lateral femoral physeal angle; MTPA: medial tibial physeal angle; PTPA: posterior tibial physeal angle; PFPA: posterior femoral physeal angle.
A threshold value of 5° was applied to define a physiologically acceptable variation in physeal-diaphyseal angles between preoperative and follow-up examinations. In addition, growth disturbances were evaluated clinically in all patients, in a standing position, by assessing pelvic height and lower-limb alignment during physical examinations at all time points.
Secondary outcomes on MRI
Deviation of Harris growth arrest lines defined as loss of parallelism relative to the adjacent growth plate at all time points
Presence of focal physeal bone bridge (PBB) formation30,31 at all time points
Extent of physeal violation by bone tunnels calculated as the ratio of the tunnel cross-sectional area (calculated based on drill diameter from operative records) to the total growth plate cross-sectional area32,33 on preoperative MRI.
Premature closure of the tibial or femoral physis, evaluated relative to the proximal fibular physis 34 at all time points and skeletal maturity 35 at final follow-up.
Statistical analysis
Statistical analyses were performed using RStudio (version 4.5.1). For comparisons between two measurement times (preoperative and 60 months postoperatively), tests adapted to the paired nature of the data were used: a paired t-test when the differences followed a normal distribution, and a Wilcoxon signed-rank test when this was not the case. Normality of the data was assessed using the Shapiro–Wilk test. Confidence intervals for proportions were estimated using a binomial approach. The significance threshold was set at 5%. Regarding baseline characteristics and secondary outcomes, continuous variables were described as medians and interquartile ranges (IQRs), and categorical variables as frequencies and percentages.
Results
Fifty patients (33 boys, 17 girls) underwent transphyseal ACLR (mean age 13.2 years; range 9–16; mean Tanner stage 2.8) between September 2017 and April 2019. A total of 24 patients were lost to follow-up, 9 sustained a graft re-tear, and 1 experienced a rupture on the opposite side, resulting in 16 patients available for evaluation at 60 months.
For the remaining 16 patients, the median age at the time of surgery was 12.5 years (IQR 3.0). The sex distribution was balanced (56.3% male). Median body mass index (BMI) was 20.5 kg/m² (IQR 3.0). Injuries were sports-related and mostly occurred during soccer (18.8%) and skiing (18.8%) followed by rugby (12.5%) and motocross (12.5%). Median tibial tunnel was 8.0 mm (IQR 1.0) and femoral tunnel 7.0 mm (IQR 0.3). Preoperative MRI demonstrated no focal abnormalities of the growth plates. At final follow-up (median 60 months (IQR 1.3)), the median age was 17.3 years (IQR 1.4), and most patients (87.5%) had reached skeletal maturity on MRI. Patient characteristics are summarized in Table 1.
Patient characteristics.
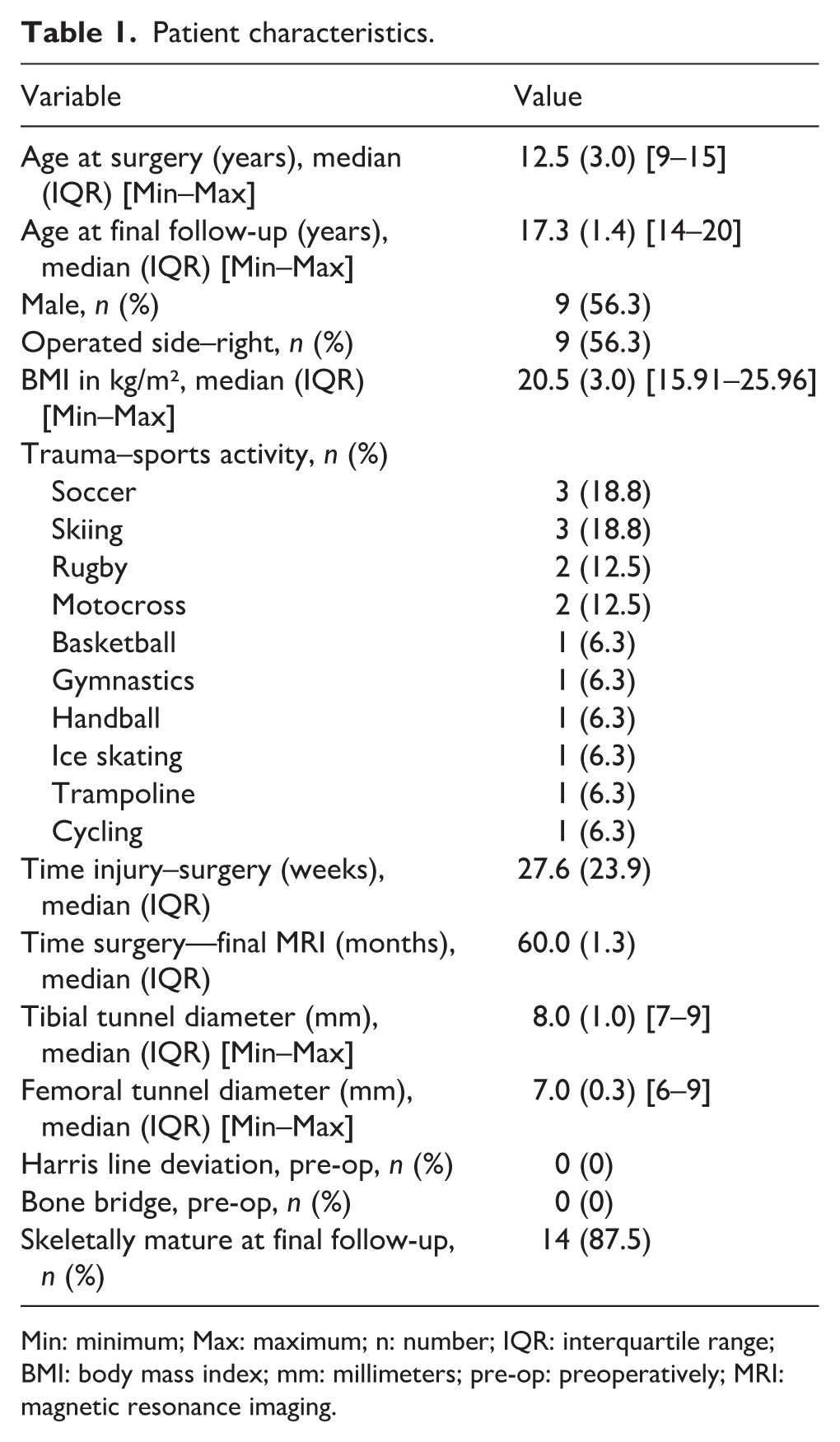
Min: minimum; Max: maximum; n: number; IQR: interquartile range; BMI: body mass index; mm: millimeters; pre-op: preoperatively; MRI: magnetic resonance imaging.
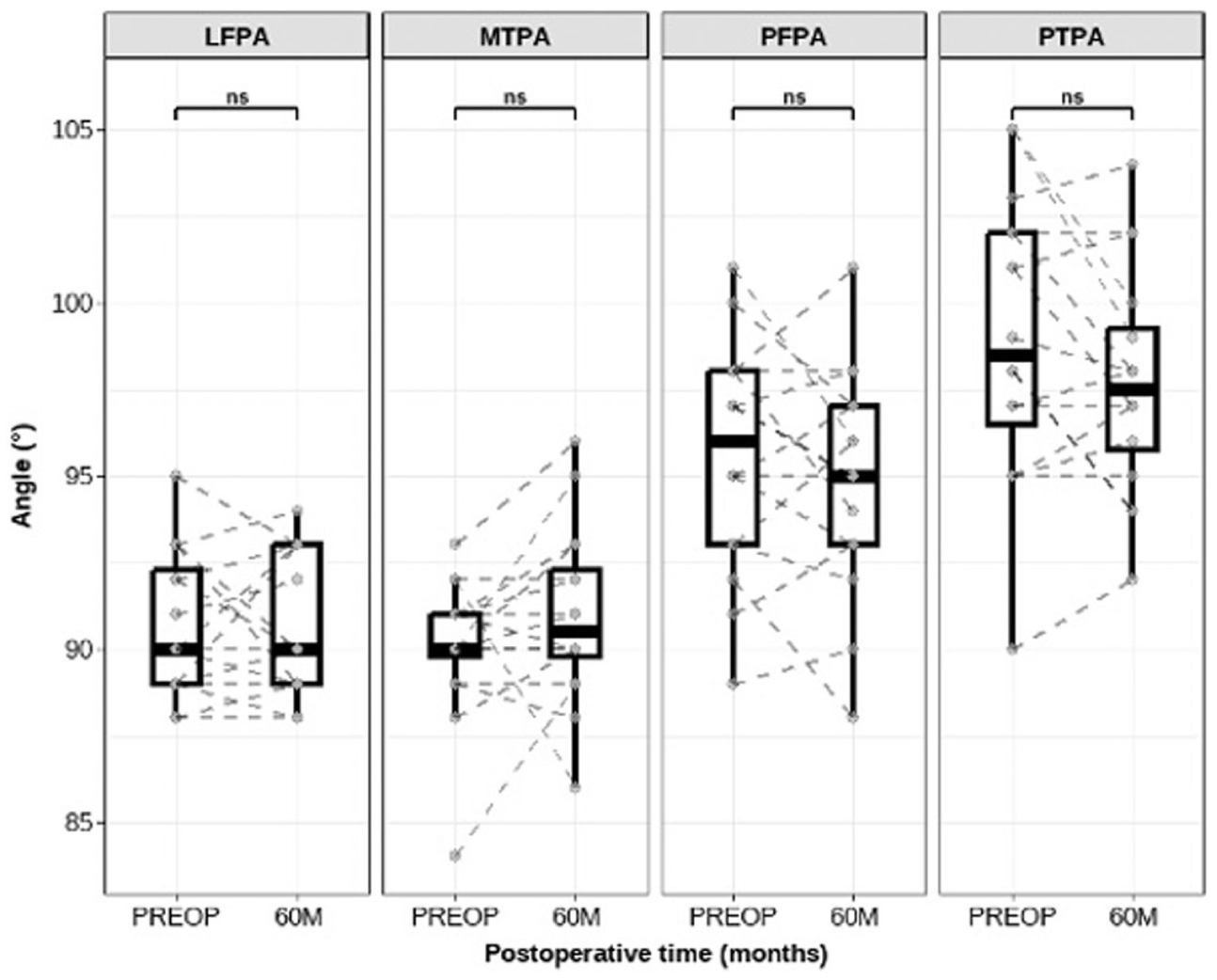
Median physeal-diaphyseal angles remained stable throughout the follow-up period. The median medial tibial physeal angle (MTPA) was 90.0° (IQR 1.3) preoperatively and remained 90.0° at 6 months (IQR 1.5), 12 months (IQR 2.0), and 24 months (IQR 3.3), with a slight increase to 90.5° (IQR 2.5) at 60 months. Similarly, lateral femoral physeal angle (LFPA) showed consistent values, with a median of 90.0° preoperatively (IQR 3.3), 90.0° at 6 months (IQR 2.0), 12 months (IQR 0.5), 24 months (IQR 3.0), and 60 months (IQR 4.0). For the posterior tibial physeal angle (PTPA), the median was 98.5° (IQR 5.5) preoperatively, slightly increasing to 99.5° at 6 months (IQR 6.0), 12 months (IQR 6.5), and 24 months (IQR 5.3), before decreasing to 97.5° (IQR 3.5) at 60 months. Finally, the posterior femoral physeal angle (PFPA) remained relatively stable, with median values of 96.0° preoperatively (IQR 5.0), 96.0° at 6 months (IQR 6.0), 95.0° at 12 months (IQR 5.0), 95.5° at 24 months (IQR 5.3), and 95.0° (IQR 4.0) at 60 months (Figure 2).
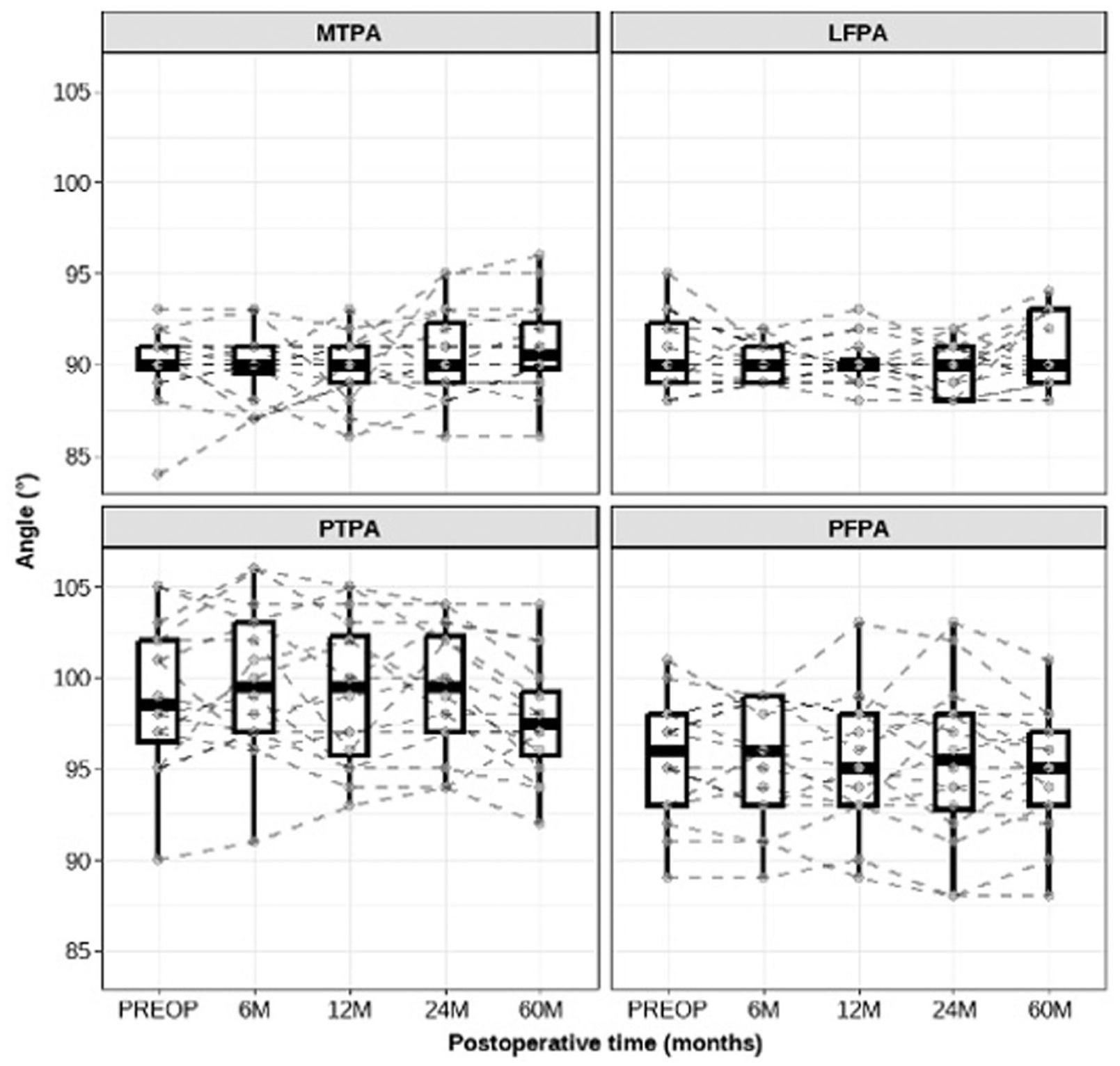
Evolution of angle measurements over time.
Transient axis deviations were noted over the course of follow-up (Figure 3). For the MTPA, no significant difference was found between preoperative and 60-month values (p-value = 0.20). At the final follow-up, 19% of patients ((95% confidence interval (CI)) 4%–46%; n = 3) showed a deviation ≥ ±5° (+5° in 2 patients, −6° in 1 patient), while 81% ((95% CI) 54%–96%; n = 13) remained within ±5°. For the LFPA, 60-month measurements were comparable to preoperative values (p-value = 0.91), with no patient exhibiting a deviation ≥ ±5° ((95% CI) 0%–21%; n = 0). PTPA values also showed no significant difference at 60 months (p-value = 0.16); 12% of patients ((95% CI) 2%–38%; n = 2) had deviations ≥ ±5° (−5° in one patient and −6° in the other), while 88% ((95% CI) 66%–98%; n = 14) were within ±5°. For the PFPA, no significant change was observed at final follow-up (p-value = 0.30). Only one patient (6%, (95% CI) 0.2%–30.2%) demonstrated a deviation ≥ ±5° (of −5°), whereas 94% ((95% CI) 70%–100%; n = 15) remained within ±5° (Figure 4). Clinically, standing pelvic height and lower-limb alignment measurements revealed no signs of growth disturbance. No patient reported symptoms such as pain, discomfort, or gait abnormalities.
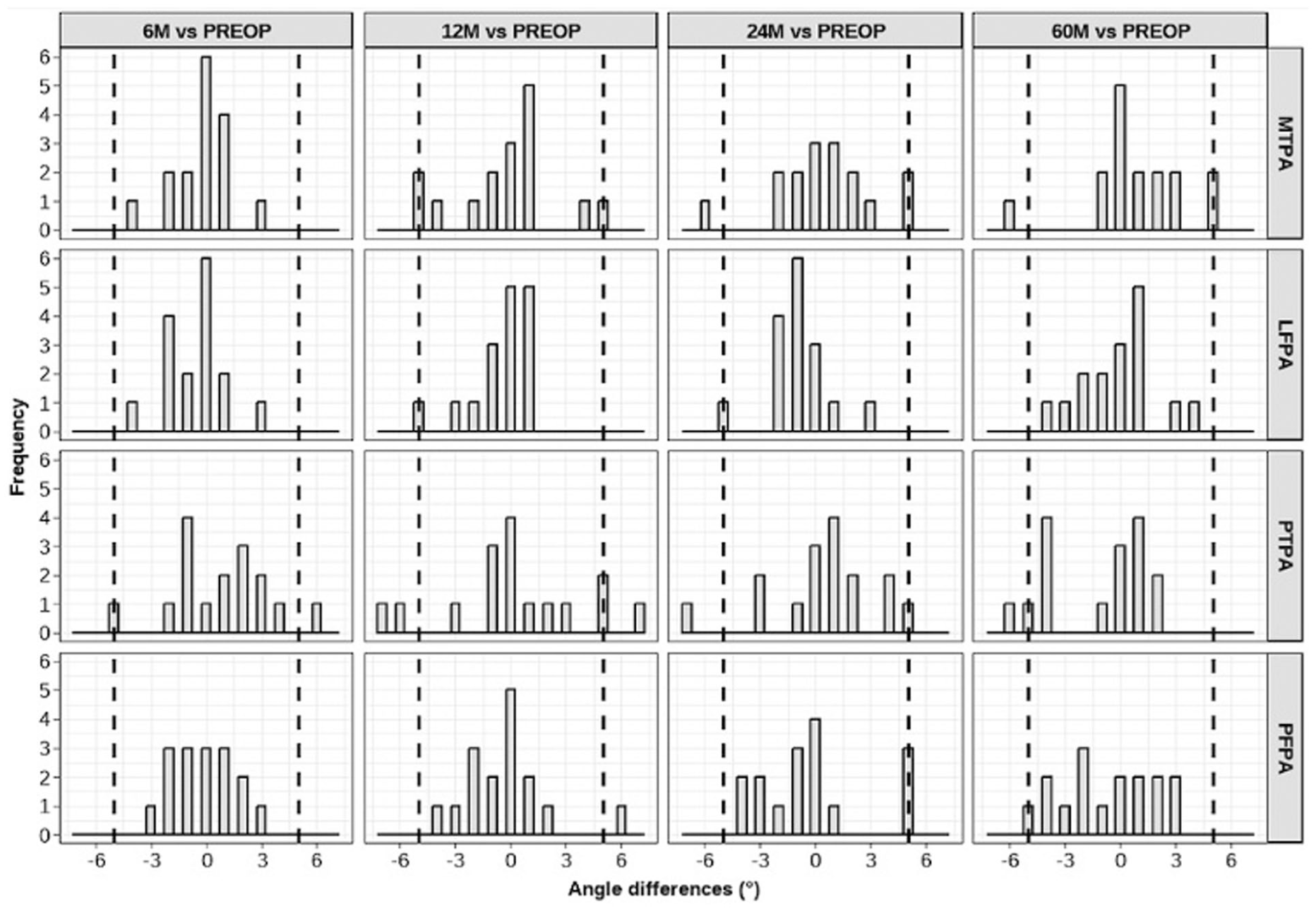
Angle differences between preoperative and postoperative times.
Changes in angle measurements pre-op versus 60 months post-op.
Harris growth arrest lines showed no deviation. No premature closure of tibial or femoral physis was observed compared to the proximal fibula. Throughout the follow-up, bone bridge formation was observed in three patients (18.75%) at least once, always transiently, and none persisted at 60 months. Physeal violation was minimal at 1.6% (IQR 0.2) and 1.1% (IQR 0.2) for the tibia and femur, respectively. More detailed individual information regarding the 16 patients is presented in Table 2A and B.
(A) Evolution of angular deviations ≥ ±5° and characteristics of physeal bone bridges and (B) additional information–9 remaining patients without significant angular deviation at final follow-up or physeal bone bridges.
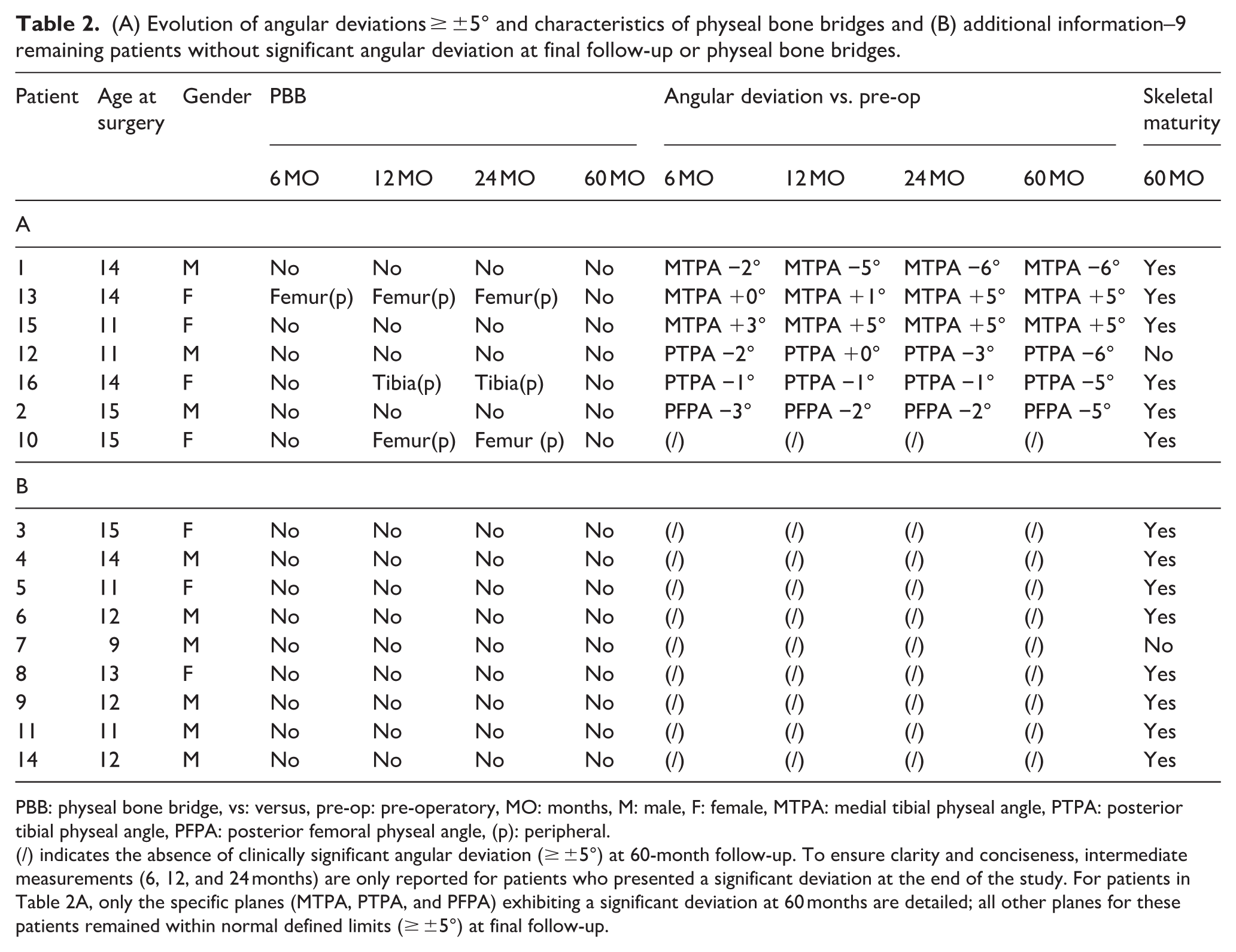
PBB: physeal bone bridge, vs: versus, pre-op: pre-operatory, MO: months, M: male, F: female, MTPA: medial tibial physeal angle, PTPA: posterior tibial physeal angle, PFPA: posterior femoral physeal angle, (p): peripheral.
(/) indicates the absence of clinically significant angular deviation (≥ ±5°) at 60-month follow-up. To ensure clarity and conciseness, intermediate measurements (6, 12, and 24 months) are only reported for patients who presented a significant deviation at the end of the study. For patients in Table 2A, only the specific planes (MTPA, PTPA, and PFPA) exhibiting a significant deviation at 60 months are detailed; all other planes for these patients remained within normal defined limits (≥ ±5°) at final follow-up.
Discussion
Transphyseal ACLR performed with a standardized technique was associated with mild radiological but no clinically relevant growth disturbances at mid-term follow-up. This is consistent with previous reports stating that minor, subclinical growth alterations may occur after transphyseal ACLR, whereas clinically significant disturbances requiring corrective surgery remain uncommon. 16 Bolzinger et al. 14 reported LLD in 13% of cases and mechanical axis deviation (MAD) in 34% at the femoral level and 53% at the tibial level, yet no clinically relevant growth disturbances were observed at 2-year follow-up. Calvo et al. 15 found no radiographic evidence of LLD or malalignment in their 10-year follow-up study. Seeto et al. 36 demonstrated stable postoperative limb alignment and growth, with only minor overgrowth in the operated limb and a few cases of LLD or MAD variations. McCarthy et al. 37 similarly reported no radiographic evidence of growth disturbances at a mean follow-up of 3 years. Carrozzo et al. 38 found an overall incidence of growth disturbances in 15.8% of patients who underwent radiologic evaluation after partial transphyseal All-Inside ACLR, yet all changes were minor and clinically insignificant.
Throughout follow-up, mean tibial and femoral physeal–diaphyseal angles showed no relevant variation, and minimal axis deviations were observed in a limited number of cases. Six patients (37.5%) exhibited persistent but minor angular changes at final follow-up, none of which translated into clinically relevant deformity.
In our cohort, most growth disturbances involved the tibia. A decrease in MTPA, with no clinical valgus, was observed in one case, possibly related to an overgrowth phenomenon (Chotel type B) associated with the 4.5 mm tunnel or with graft harvesting at the pes anserinus due to periosteal stripping. While two others exhibited an increased MTPA, potentially due to growth arrest (Chotel type A) or a tethering effect (Chotel type C), no clinical varus was noticed.
Two patients showed a decrease in PTPA, and a single decrease was noticed in PFPA, with no clinical recurvatum. Only one patient with an isolated decrease in PTPA of −6° still had open physis at final follow-up, thereby preventing the complete exclusion of clinically significant growth disturbances in the future.
It is important to emphasize that mild side-to-side differences in alignment are common in the general population and do not necessarily indicate a pathological process.39,40 Subtle deviations at final follow-up might simply reflect normal variability. The lack of a comparative, contralateral analysis in our study limits definitive interpretation.
Growth-related changes after ACLR may be transitory. We observed transient PBB formation in 18.8% of patients, a rate within the previously reported range of 4.2% to 20%.17,41,42 None led to clinically significant deformities, and all had resolved by final follow-up. Jeon et al. 43 reported transient growth alterations at 6-12 months postoperatively in patients with substantial growth remaining, particularly affecting the tibia. These changes were mainly observed in those with ≥4 cm of residual growth and tended to plateau after 6 cm of longitudinal growth remained, suggesting the possibility of temporary growth modulation following physeal injury or surgical intervention. These findings echo Chotel’s comment 44 on Yoo et al.’s 42 conclusions, highlighting that small epiphyseal bridges in younger children may lack clinical significance, as residual growth and expansive forces often allow spontaneous “de-epiphysiodesis.” By contrast, adolescents may have less remodeling potential, theoretically increasing their risk of persistent disturbances, although limited remaining growth reduces the likelihood of clinically meaningful deformities.
We were unable to demonstrate any association between PBB formation and growth disturbances due to the small sample size. Out of the three patients with PBBs, only one with a tibial PBB exhibited a borderline decrease in PTPA (−5°) and had closed physis by final follow-up, making causality difficult to establish.
Surgical techniques for pediatric ACLR vary widely, primarily influenced by skeletal maturity. In North America, epiphyseal techniques are commonly used in children with open growth plates, with a shift toward transphyseal reconstruction after puberty. 45 French surgeons often favor a transphyseal tibial tunnel combined with an epiphyseal femoral tunnel in prepubescent patients, moving to fully transphyseal techniques in adolescents. 46 Available evidence does not support the superiority of any single ACLR technique in preventing growth disturbances.
Notably, although it is commonly presumed to minimize the risk of growth disturbance, reported rates of growth abnormalities after all-epiphyseal reconstruction appear comparable to those observed after transphyseal techniques.7,47–49 A possible explanation lies in the trajectory of the epiphyseal tunnel, which must be placed as proximally and posteriorly as possible to approximate the native ACL footprint. Any inaccuracy in drilling may result in unintended physeal involvement and affect a relatively large surface area as the tunnel is tangential to the growth plate. Moreover, this trajectory crosses the epiphyseal side of the physis, its most vulnerable region. Cordasco et al. 50 found that all patients with a leg-length discrepancy of more than 5 mm after all-epiphyseal ACLR were patients whose tibial physis was violated by the graft tunnel.
In our study, physeal violation was lower than previously reported values42,51 and far below the 7%–12% critical threshold associated with growth complications.52,53 No premature physeal closure was observed in the femur or tibia compared with the proximal fibular growth plate, although this result should be interpreted cautiously, as the physis may not close simultaneously. 34 Meticulous surgical technique is a key determinant in minimizing growth-related complications. Most reported cases of growth disturbances requiring surgical correction were associated with technical errors, regardless of the reconstruction method.47,54 Regarding transphyseal ACLR, careful tunnel placement and sizing remain fundamental, and the procedure should be performed exclusively by appropriately trained surgeons. Preservation of the perichondral ring is essential and requires careful technique when preparing the femoral footprint. Tibial tunnels larger than 9 mm should be avoided, as they result in greater physeal violation. 33 No bone grafts or fixation devices should cross the physis. 54 Placing soft-tissue grafts across open physis appears to prevent the formation of PBBs. 55
Another important concern in pediatric ACLR is the relatively high rate of graft re-rupture reported in this population. Although graft failure was not the primary outcome of the present study, the re-tear rate observed in our cohort (18%) is consistent with high rates reported in the current literature.7,56 This highlights the importance of ongoing efforts to optimize surgical strategies that are not only safe with respect to physeal preservation and growth but also mechanically reliable for graft maturation and long-term graft integrity.
This study has multiple limitations. The substantial loss to follow-up introduces a risk of attrition bias. Although most patients reached skeletal maturity, late-onset disturbances cannot be fully excluded. However, the 5-year follow-up allows meaningful assessment of mid-term growth behavior. Future studies with larger patient populations should be planned to confirm these mid-term observations and further evaluate long-term growth-related outcomes after transphyseal ACLR in skeletally immature patients. Although we prioritized MRI to provide a comprehensive evaluation of growth-related outcomes, we acknowledge that the absence of long-leg radiographs limits the precision of angular alignment interpretation, which remains the gold standard for this specific parameter. Further validation of angular measurements using MRI would strengthen the assessment of growth-related changes in future studies. While some patients were in late adolescence at the time of surgery, their inclusion was justified by the visualization of open physis on initial MRIs. The detection of focal PBB in these patients up to 24 months postoperatively confirms that the growth plates remained biologically active and susceptible to morphological changes. Furthermore, MRI provides the unique advantage of visualizing the physis even as it approaches closure and after skeletal maturity. This allowed for consistent longitudinal measurement of physeal–diaphyseal angles across all time points, ensuring that measurements taken at final follow-up remained directly comparable to those obtained while the physis were still open. Precise preoperative skeletal age was not measured in this series, and initial skeletal maturity was assessed using knee radiographs and Tanner staging at the time of surgery. The aforementioned evaluation was considered sufficient for surgical decision-making, reflecting the practice settings within our institution, as patients identified as skeletally immature are all treated using the same pediatric technique, whereas skeletally mature patients are managed by adult orthopedic surgeons. Consequently, the results should be interpreted with caution and regarded as preliminary. Nevertheless, this study provides the longest MRI-based follow-up of growth disturbances in this population.
Conclusion
Transphyseal ACLR in skeletally immature patients appears to be associated with minimal physeal violation, low rates of bone bridge formation, and clinically non-significant growth disturbances at mid-term to long-term follow-up.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261456086 – Supplemental material for Five-year MRI follow-up of growth-related complications after ACL reconstruction in children and adolescents
Supplemental material, sj-pdf-1-cho-10.1177_18632521261456086 for Five-year MRI follow-up of growth-related complications after ACL reconstruction in children and adolescents by Caroline de Pesters, Antoine Laval, Linda Staali, Clara Flumian, Marie Faruch and Franck Accadbled in Journal of Children's Orthopaedics
Footnotes
Author contributions
All authors contributed substantially to this study, in both the writing of the manuscript and the acquisition of the study data:
Data
Data from this study are not publicly available due to ethical and privacy restrictions, but are available from the corresponding author upon reasonable request*
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: C.d.P., A.L., L.S., C.F., and M.F.: declare that they have no conflict of interest. F.A.: none for this study. Consultant with Orthofix and Zimmer Biomet.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval for this study was obtained from the local ethics committee (RnIPH 2019-56). A prospective analysis of the data of patients with Anterior Cruciate Ligament. Reconstruction over the years 2017–2019 was performed at Toulouse University Hospital. Fifty evaluations and or data were gathered. According to French law on ethics, patients were informed that their codified data would be used for the study. According to French ethics and regulatory law (public health code), prospective studies based on the use of usual care data should not be submitted to an ethics committee, but they must be declared or covered by a reference methodology of the French National Commission for Informatics and Liberties (CNIL). Collection and computer processing of personal and medical data were implemented to analyze the research results. Toulouse University Hospital signed a commitment to compliance with the reference methodology MR-004 of the French. National Commission for Informatics and Liberties (CNIL). After evaluation and validation by the data protection officer and according to the General Data Protection. Regulation*, this study completes all the criteria, it is registered in the register of data study of the Toulouse University Hospital (number’s register: RnIPH 2019-56) and covered by the MR-004 (CNIL number: 2206723 v 0). This study was approved by Toulouse University Hospital and confirms that ethical requirements were totally respected in the above report. *Regulation (EU) 2016/679 of the European Parliament and of the Council of 27 April 2016.
Informed consent
Informed consent was obtained from all patients (legal guardians) included in the study.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.