
Abstract
Purpose:
Supracondylar fractures of the humerus are the most common elbow fractures in children. Surgical fixation is necessary in cases with complete displacement (Gartland type III), with closed reduction and pin fixation being preferred. It is sometimes impossible. This study examined radiological and clinical factors that influence the selection of open reduction methods for these fractures.
Methods:
A retrospective study was designed to investigate children aged 3–13 years with Gartland type III supracondylar humeral fractures (OTA/AO 13-M/3.1 III) treated with closed and open reduction techniques. We enrolled 140 patients in the closed reduction group (mean age 6.27) and 90 in the open reduction group (mean age 6.86). The main outcomes were achieving adequate closed reduction or switching to open reduction. We used univariate analysis and multivariate logistic regression to find independent risk factors and odds ratios for open reduction and internal fixation.
Results:
Older children were significantly more likely to have flexion-type fractures (P = 0.001). The final univariate analysis showed that older age (odds ratios (95% confidence interval): 1.1 (1, 1.3)), flexion-type fractures (odds ratios (95% confidence interval): 3.2 (1.4, 7.4)), low-level (below isthmus) fractures (odds ratios (95% confidence interval): 2.2 (1.3, 3.9)), and Pucker sign (odds ratios (95% confidence interval): 2 (1, 4)) were factors that significantly increased the chance of open reduction and internal fixation. The influence of older age and low-level fracture was also strongly demonstrated in multivariate analysis.
Conclusions:
As age increases, the chance of a flexion-type fracture rises, and thus the chance of needing open reduction. Low-level fractures reduce the possibility of achieving a stable closed reduction by creating a smaller, more cartilaginous distal fragment.
Type of study/level of evidence:
Introduction
Pediatric supracondylar humeral (SCH) fractures are the most common pediatric elbow fractures. According to preoperative radiography and the Gartland classification, these fractures are divided into two main types: extension and flexion. Each type has three subgroups based on the degree of displacement of the fractured fragment. The fourth type appears only during a reduction in the operating room. It is marked by multidirectional instability of the distal fragment. 1
The treatment for type I fractures is always non-surgical, as these fractures are stable and non-displaced. There is some debate about the treatment of type II fractures; however, the standard approach typically involves correcting the fracture alignment and using closed pin fixation. By contrast, type III fractures always necessitate surgical intervention and fixation. However, due to the robust periosteum in pediatric patients, these fractures can frequently be closely reduced with appropriate maneuvers.2,3
In some cases, closed reduction may not be possible. Close reduction failure may happen when the proximal fragment gets stuck in the brachialis muscle or when soft tissues like the brachialis artery, median or ulnar nerves, or periosteum are trapped in the fracture site. In these situations, open reduction is necessary. Predicting these conditions preoperatively is difficult, except in cases such as brachial artery entrapment, which often presents with loss of distal pulses and reduced limb blood flow. There is currently no consensus on this issue.4,5
Considering the complications and requirements of open reduction, predicting this situation can help the surgeon, in addition to informing the patient’s parents about the possible risks before surgery, prepare for surgery in a way that does not encounter any problems if needed, and thus, by reducing complications during surgery, expect better treatment results.
In this retrospective study, we investigated the effects of factors on treatment selection by comparing clinical and radiological findings from preoperative evaluations of children with Gartland type III fractures who underwent closed or open reduction.
Materials and methods
We conducted this study at an academic referral center after obtaining approval from the ethics committee. Using a computerized database, we reviewed all patients aged 3–13 who received treatment for a type III SCH fracture (including both extension and flexion types) at this center between 2021 and 2024. We then reviewed the patients’ files, including preoperative examinations and operative notes. We enrolled eligible patients by applying inclusion criteria, which included completeness of file information and acceptable anterior/posterior and lateral radiographs, and exclusion criteria, which included open fractures (except those with pinholes), fractures with vascular damage requiring exploration, revision surgeries, pathological fractures, patients with bone deformity in the elbow area, and type III cases that converted to type IV during surgery. Surgeons performed all cases of open reduction after closed reduction had failed. Ultimately, the study included 230 patients: 90 patients in the open reduction and internal fixation (ORIF) group and 140 patients in the closed reduction and percutaneous pinning group, all of whom underwent pin fixation. A total of 22 patients in the closed reduction group and 13 in the open reduction group were excluded, with mean ages of 5.9 and 6.8 years, respectively. Only two of these patients had flexion-type fractures, both of which had undergone ORIF. All patients in this study were operated on by orthopedic surgeons with orthopedic fellowship training, except for trauma and pediatric fellowships (unavailable at our center). We divided surgeons into two groups: one group included those with hand, shoulder, and elbow fellowships, while the other included other available fellowships, such as knee, hip, and spine. After the senior surgeon in the research group selected the appropriate radiographs, two fellowship-trained hand surgeons measured and recorded all radiological values using PACS (Picture Archiving and Communication System) software (Figure 1). The interclass reliability coefficients for the measurements made by the two surgeons were above 0.9, indicating a high level of reliability in the recorded values.
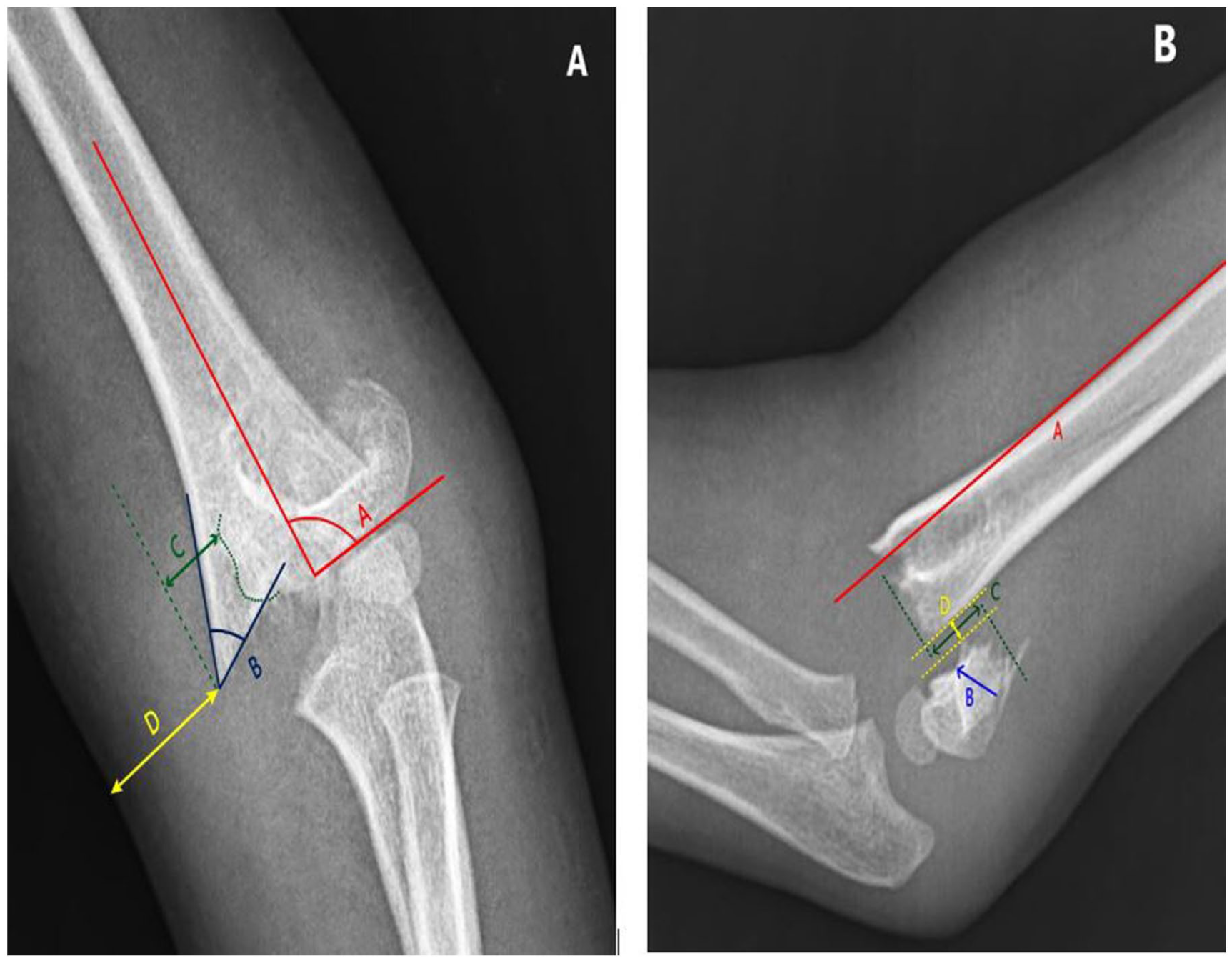
Example radiographic parameters measured on anterior–posterior (A) radiograph: (A) represents Baumann’s angle, (B) is the medial corner angle, (C) is the coronal displacement, and (D) is the tip-skin distance. Radiographic parameters measured on the lateral (B) radiograph: Anterior humeral line is labeled as (A), isthmus level marked by arrow (B), (C) is the axial shortening amount, and (D) shows sagittal displacement.
The results were analyzed by looking at the correlation of qualitative variables. This was done using two-way tables, chi-square statistics, and Fisher’s exact test. For quantitative variables, we used a t-test. We selected variables with a P-value of less than 0.2 for univariate and multivariate regression analyses (bold values in Tables 1, 2 and 3). The significance level was set at 0.05. The analyses were conducted using Stata software version 17 ( StataCorp LLC).
Comparison of the frequency distribution of clinical and demographic variables based on the ORIF and PCP groups.
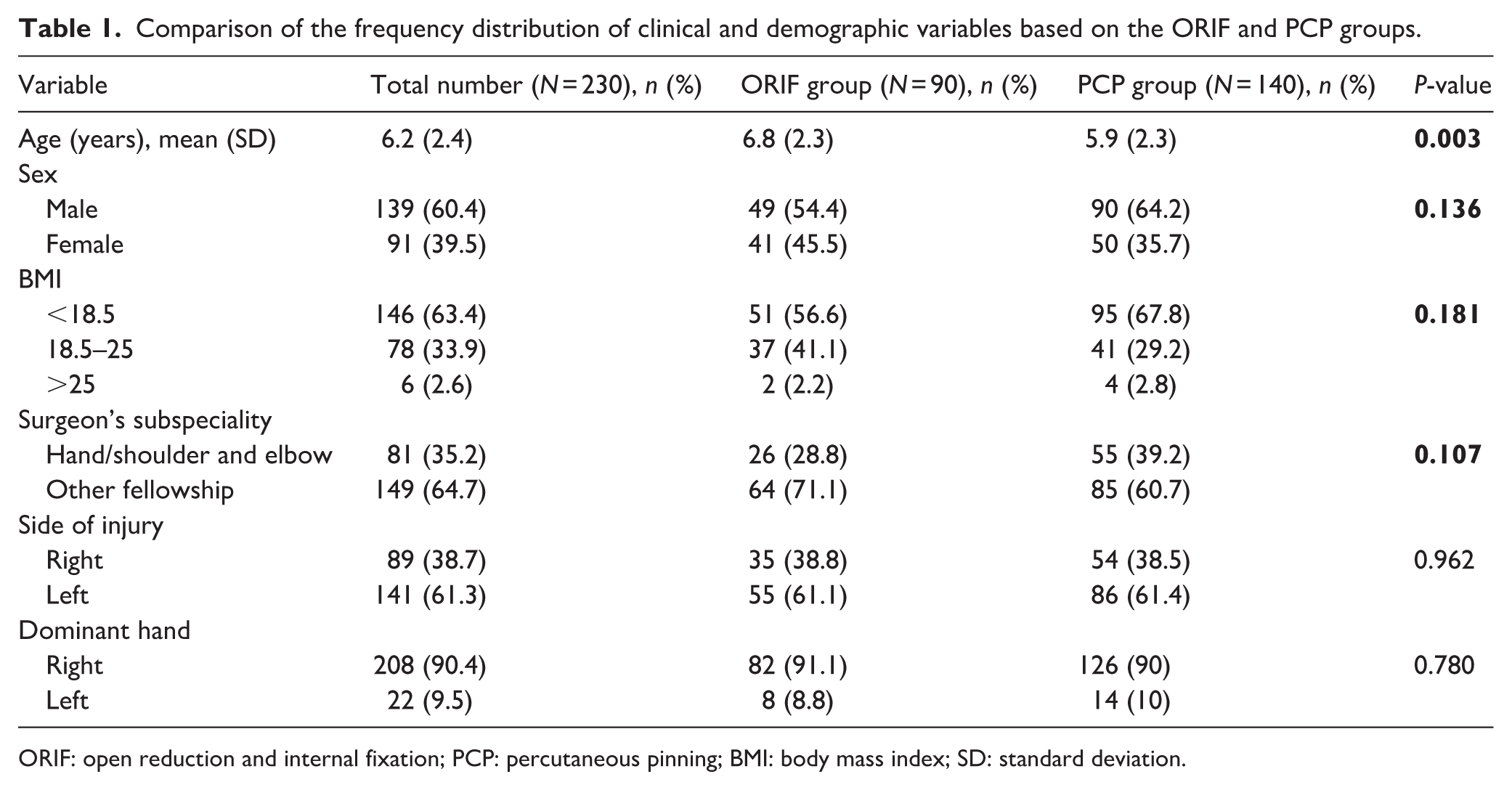
ORIF: open reduction and internal fixation; PCP: percutaneous pinning; BMI: body mass index; SD: standard deviation.
Comparison of the frequency distribution of clinical and radiological variables based on the ORIF and PCP groups.
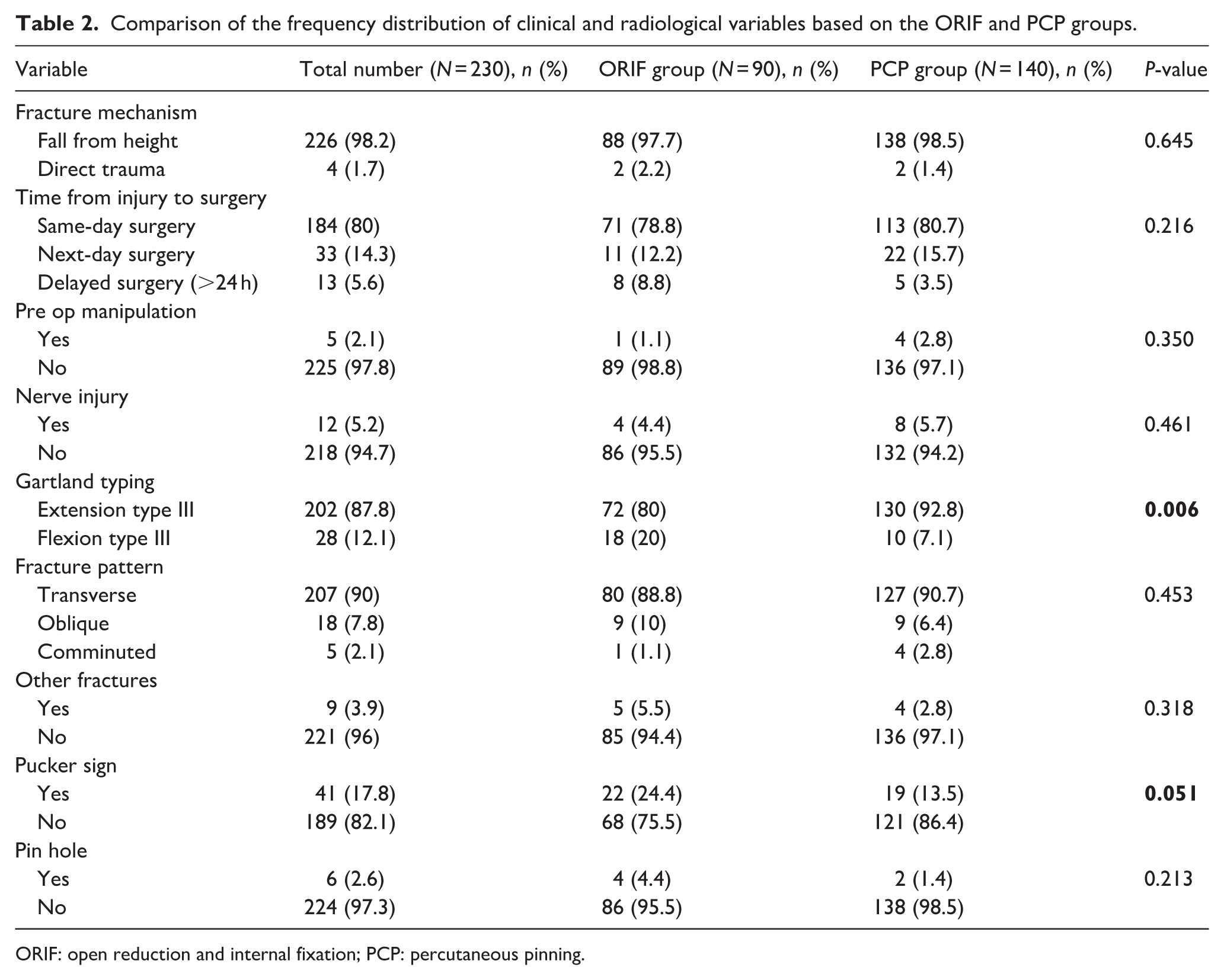
ORIF: open reduction and internal fixation; PCP: percutaneous pinning.
Comparison of mean (SD) and frequency (%) of radiological variables based on the ORIF and PCP groups.
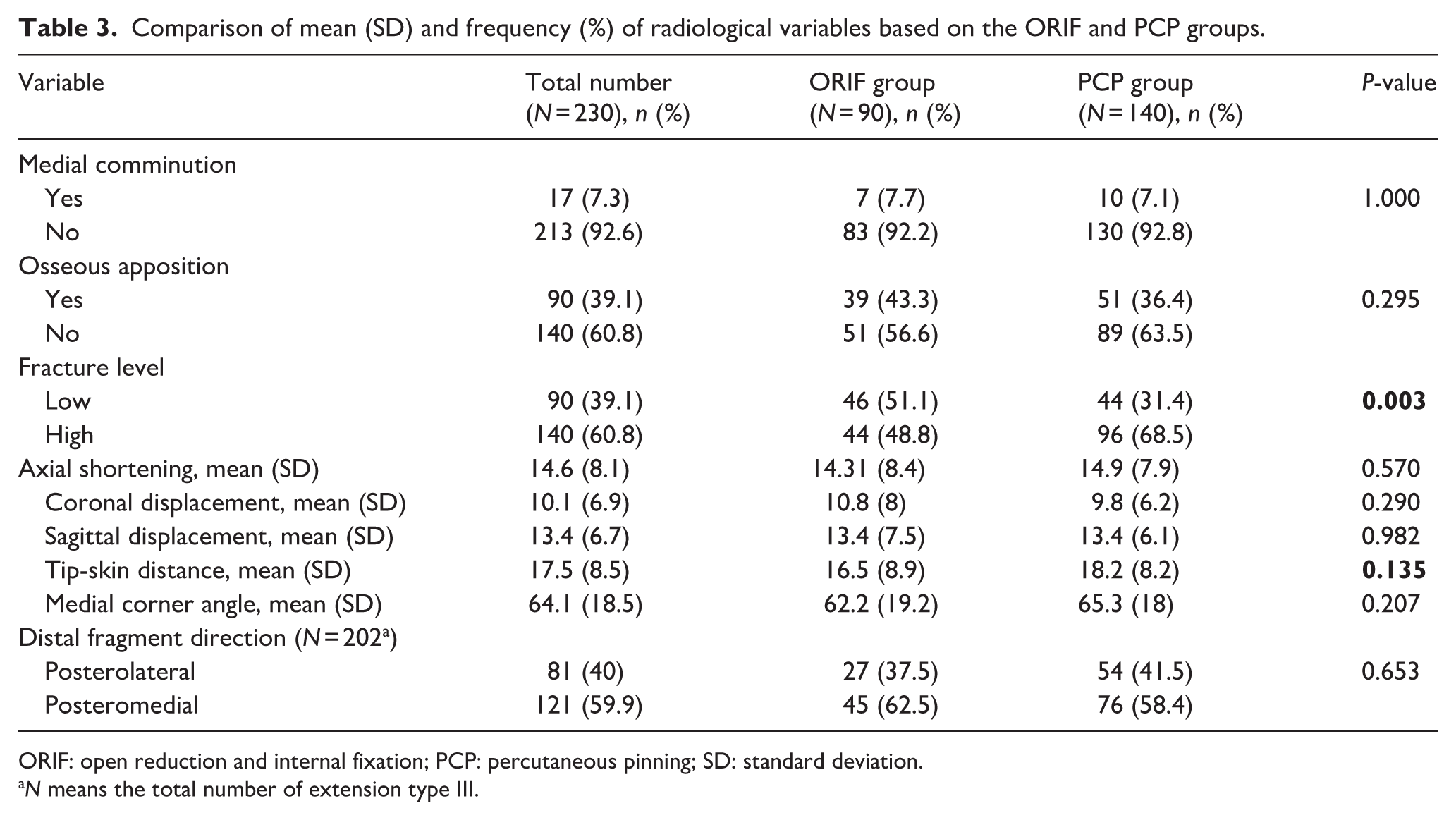
ORIF: open reduction and internal fixation; PCP: percutaneous pinning; SD: standard deviation.
N means the total number of extension type III.
Results
The mean age of patients in this study was 6.2 (SD = 2.4) years. The mean age for the ORIF group was 6.8 years, significantly higher than the 5.9 years for the close reduction and percutaneous pinning (CRPCP) group (P = 0.003). Regarding sex, 60.4% of the patients were male, and 39.5% were female. There was no significant link between the rate of ORIF and sex (P = 0.136). As the body mass index (BMI) category increased, the likelihood of receiving ORIF also rose. However, this relationship was not statistically significant (P = 0.181). Surgeons with fellowships other than upper extremity (hand/shoulder and elbow) performed 10% more ORIF, but this increase was not significant (P = 0.107; Table 1).
The most common fracture mechanism was a fall on the hand (98.2). Eighty percent of patients underwent surgery within the first 24 h. Patients whose surgery was delayed by more than 24 h were more likely to require open reduction; however, this difference was not statistically significant (P = 0.216). 5.2% of patients had preoperative nerve injury (only included patients whose nerve damage caused paralysis of the relevant muscles and who also had symptoms after surgery), with no significant difference observed between the two groups (P = 0.461). The fractures of five patients had been manipulated for reduction by non-orthopedics before referral, and only one required ORIF, suggesting no significant effect (P = 0.350). 87.8% cases were extension type III fractures, and the rest were flexion type. Patients with flexion-type fractures had a significantly higher rate of need for open reduction (P = 0.006). Ninety percent of the fractures were transverse, and the fracture form did not significantly affect the ORIF rate (P = 0.453). Approximately 4% of patients had fractures in other bones, with the distal radius being the most common. This associated fracture did not significantly increase the need for open reduction (P = 0.318). On examination, the Pucker’s sign was observed in nearly 18% of patients. More than half of these patients (53%) underwent ORIF (even with the milking maneuver). Although this finding was not statistically significant (P = 0.051), it was clinically important. A pinhole was observed in 2.6% of patients and did not significantly affect the choice of surgical procedure (P = 0.213; Table 2).
Medial comminution (any comminution in the medial column of the distal humerus on anterior-posterior (AP)radiographs) was observed in 7.3% of patients, with no significant effect on surgical procedure (P = 1). The radiographic analysis found that 60.8% of patients had separated proximal and distal fragments, which showed complete dissociation on lateral X-ray (Osseous apposition). However, ORIF odds were not affected significantly by this finding (P = 0.295). By contrast, 39.1% of patients had low-level fractures (based on the distal humeral isthmus on lateral radiographs as a baseline, fractures are divided into two groups: low level and high level). The values were 51% in the ORIF group and 31% in the PCP group, indicating a statistically significant difference (P = 0.003). The average axial shortening in all patients was 14.69 mm. The two groups had no significant difference (P = 0.570). The mean coronal and sagittal displacements of the distal segment were 10.19 and 13.48 mm, respectively, with no significant difference between the two groups. The mean medial corner angle was also 64.15 degrees, showing no significant difference between the groups (P = 0.207). In extension-type fractures, the distal fragment was displaced posteromedially in about 60% of cases. Direction of displacement did not significantly affect the need for open reduction in these fractures (P = 0.653; Table 3).
Based on the results in Tables 1–3, we selected the most influential variables with P-values less than 0.2. We analyzed them in Table 4 using univariate and multivariate regression to more accurately examine the net effect of these variables on the choice of surgery type. In univariate regression analysis, four factors, including age, flexion-type fracture, pucker sign, and low-level fractures, significantly increased the odds of ORIF. For example, each additional year of age in children increases the likelihood of ORIF by 1.1 times. In multivariate regression analysis, the effects of age and low-level fractures were again significant, indicating their strong influence.
Logistic regression analysis, both univariate and multivariate, was conducted to determine the probability of requiring ORIF surgery for variables identified as statistically or clinically significant.
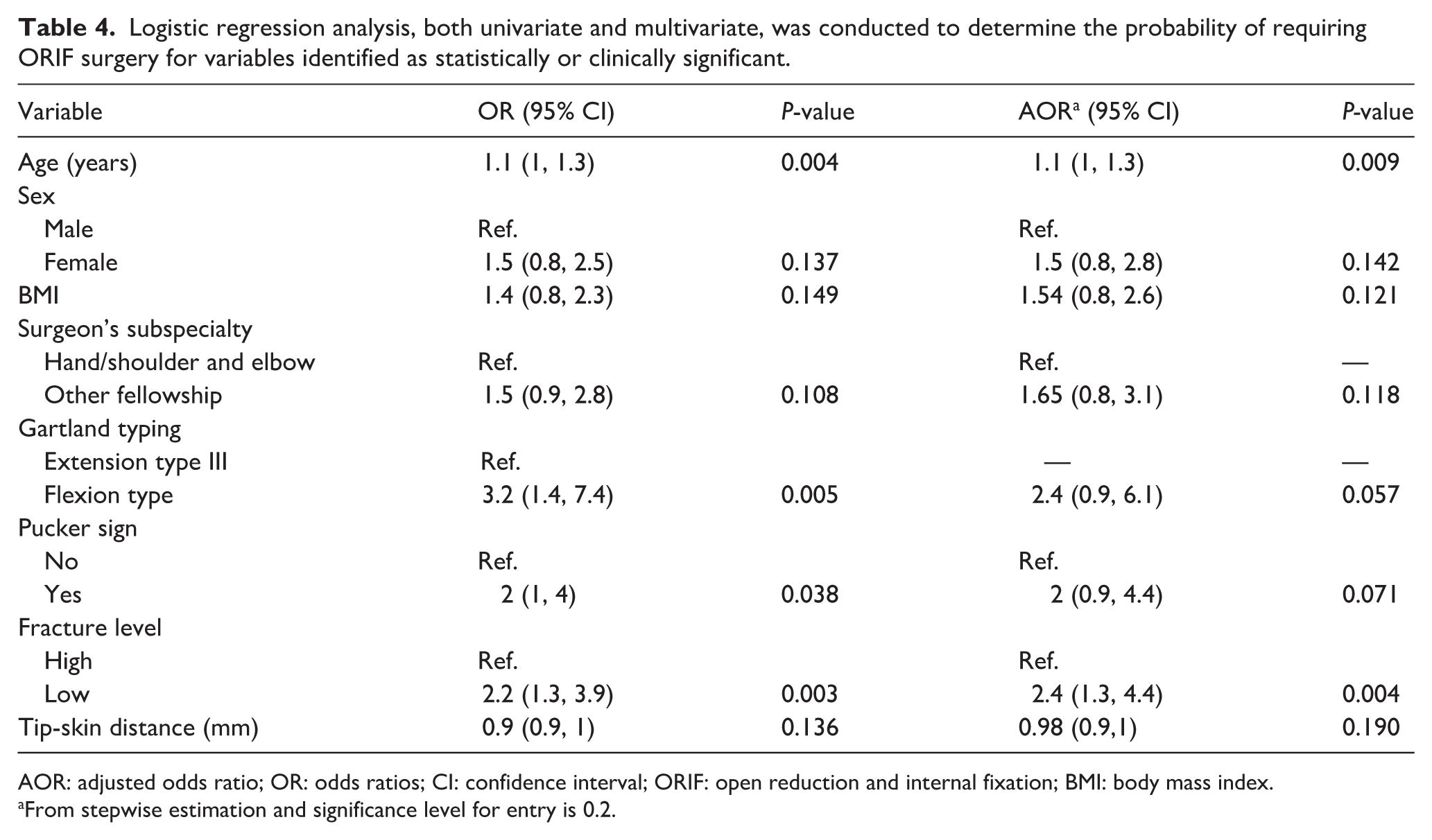
AOR: adjusted odds ratio; OR: odds ratios; CI: confidence interval; ORIF: open reduction and internal fixation; BMI: body mass index.
From stepwise estimation and significance level for entry is 0.2.
Being a girl, having a higher BMI class, and having surgeons with fellowships in areas other than upper extremity all increased the odds of ORIF by about 1.5 times when other factors were constant. Although this increase was not statistically significant, it was clinically significant.
In Table 5, comparing two types of fractures, flexion and extension, considering the same more influential variables, children with flexion fractures had a significantly higher average age (P = 0.001). Also, as previously mentioned, the need for open reduction was significantly higher in the flexion type (P = 0.004). However, variables such as sex, BMI, fracture level, and others did not show significant differences between the two fracture types.
Comparison of frequency distribution (%) and mean (Std. Dev.) of the multivariable logistic regression variables based on the extension and flexion type fractures.
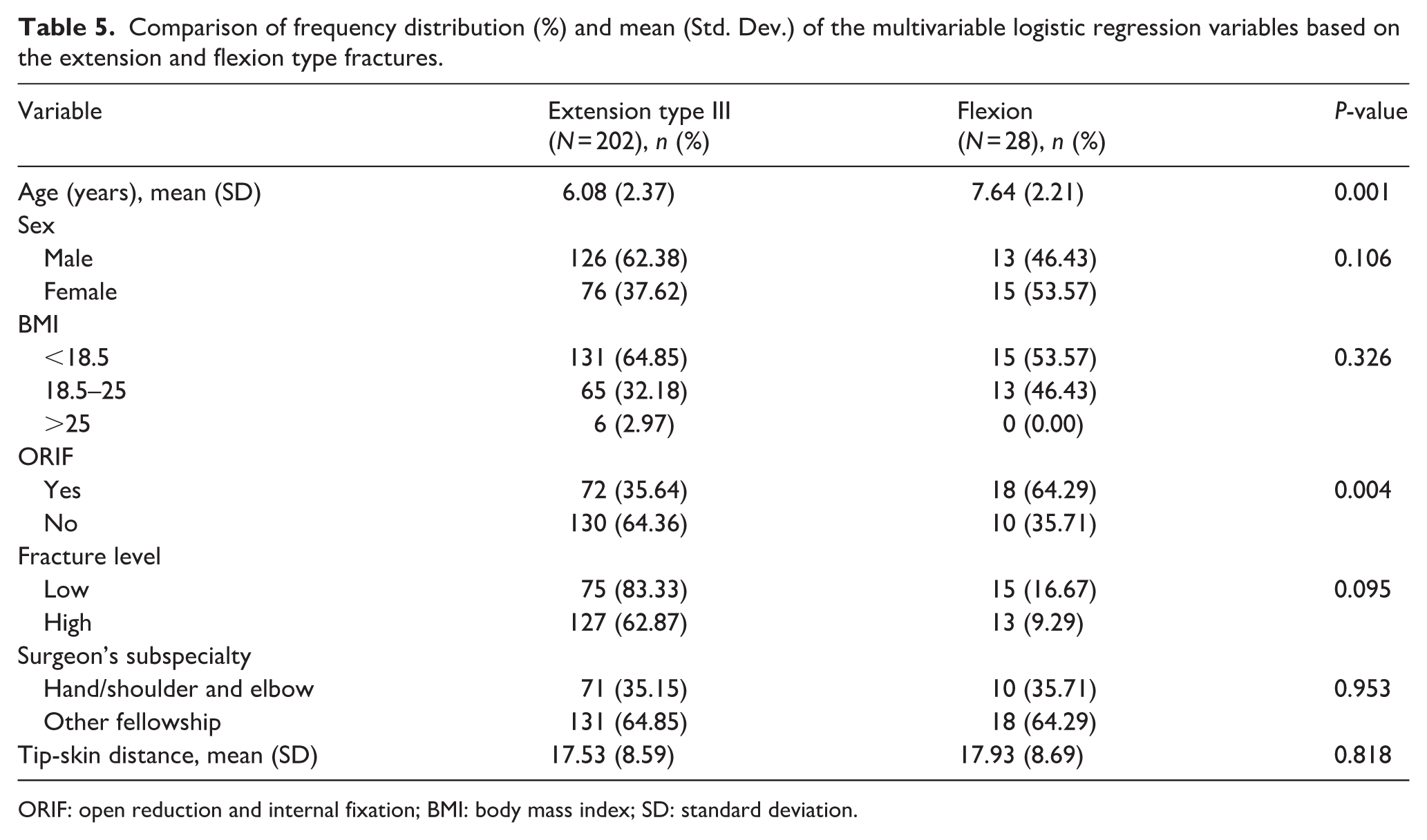
ORIF: open reduction and internal fixation; BMI: body mass index; SD: standard deviation.
Discussion
According to previous studies, Gartland type III supracondylar humeral fractures in children always require surgical intervention and are treated in most cases with closed reduction and pin fixation. Still, if this method fails, open reduction is necessary.1,2 This study has identified possible factors contributing to the failure of this method by examining a large number of these patients. It does this by closely examining factors from earlier studies and other potential causes. Our study, consistent with previous research, indicated that flexion-type fractures and fractures in older children need more open reduction.4,6,7 In addition, fractures located below the isthmus necessitate significantly more open reduction. 8
In our study, older patients had a higher likelihood of requiring ORIF, which was also confirmed in some previous studies.4,6,7,9 With increasing age, the thickness and strength of the periosteum, one of the most critical factors in pediatric fractures that prevents excessive displacement of fracture fragments and helps in better fracture reduction, decrease, which could be one of the reasons for this finding.2,3 Older children may experience more severe trauma due to engaging in riskier physical activities, and their stronger muscles can complicate fracture reduction.7,10 However, this relationship has not been proven in some other studies.10,11 The latest meta-analysis also did not show this relationship, which may be one reason for including patients with different types of this fracture in the analyses. 12
Closed reduction of flexion-type SCH fractures usually has a higher failure rate. 13 In our study, the chance of ORIF for these types of fractures was significantly higher, which was in line with previous studies’ findings.6,7,10 However, a recent meta-analysis did not prove this relationship. 12 These fractures are much less common than the extension type, and one reason surgeons fail to reduce them successfully may be their limited exposure and, as a result, their lack of experience and familiarity with closed reduction techniques of this type. Conditions such as distal fragment rotation and ulnar nerve injury have been reported as risk factors for failure to reduce these fractures. 13 Also, in our study, patients with flexion-type fractures were older on average. This could explain their higher need for ORIF.
Standard radiographs are needed to comment on radiological parameters. However, these can be hard to get in patients with unstable fractures. In our study, only a low-level fracture was significantly linked to a higher chance of ORIF. We verified the accuracy of fracture-level determination on postoperative radiographs and performed this adjustment, which was entirely consistent with our initial findings; thus, it is a convenient parameter even in radiographs that meet the minimum required standards. In the study by Tokyay et al., low-level fractures were significantly more likely to undergo ORIF. 8 Kang et al. also found that in patients treated with CRPCP, low-level fractures had significantly more difficult reductions and worse outcomes, probably due to instability and loss of reduction of these fractures. 14 The instability of these fractures may be due to the small size and cartilaginous nature of the distal fragment. These features make it harder to place and keep the pins in position. These fractures are intracapsular, likely harming the periosteum, capsule, and ligaments.8,14
Our study showed that the risk of ORIF increases with higher BMI. However, this finding was insignificant, unlike the meta-analysis by Transtrum et al. More severe injuries, greater fracture displacement, and a large amount of damaged soft tissue make close reduction more challenging for these patients. 12
Delays of more than 24 h in treatment were associated with an increased likelihood of ORIF among our patients. Although contrary to the meta-analysis of Loizou et al., this was not statistically significant, it was clinically important. 15 Over time, particularly if an adequate initial reduction has not been performed, soft-tissue damage increases, and reduction becomes more difficult. 16 Therefore, these fractures should be treated urgently.
Pucker’s sign indicates greater fracture displacement and soft tissue damage, which can make fracture reduction more difficult.2,17 Our study also confirmed the role of this important clinical finding in increasing the chance of ORIF. Although this effect was not observed in the study by Smuin et al., the number of these patients studied was much smaller in that study than in ours. 17
The radiological criteria in this study were those measured on AP and lateral elbow X-rays with basic acceptable standards. As noted previously, obtaining standard preoperative radiographs in children with SCH fractures is challenging. Many young patients with this fracture cannot have accurate radiographs due to their age and the fracture’s unstable nature. Some criteria from earlier studies were not reviewed. We could not examine them in many radiographs. We identified several cases in which repeated radiographs significantly altered these criteria.
Many radiological parameters are not measured using standard methods, so the criteria still lack the accuracy for reliable assessments. Future studies can enhance the efficiency of this tool by standardizing methods.
Finally, analysis of our findings from a significant number of patients at a tertiary referral center showed that older children with flexion-type fractures and a Pucker sign are more likely to require ORIF, and radiological findings, such as sub-isthmus fractures, can help predict the need for ORIF, despite significant limitations in radiological assessment.
A key aspect of our study is that we only examined Gartland type III fractures, the most challenging type. This approach provides more detailed information than studies that include a variety of fracture types.
A key limitation of our study was its retrospective design. We also had to exclude several patients due to the absence of standard radiographs.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261456089 – Supplemental material for Factors associated with open reduction of pediatric type III supracondylar humerus fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521261456089 for Factors associated with open reduction of pediatric type III supracondylar humerus fractures by Farid Najd Mazhar, Bushra Zareie, Hooman Shariatzadeh, Ahmad Hasan, Meisam Jafari Kafiabadi, Narges Akhlaghi and Omid Mahmoudi Nasab in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
The authors gratefully acknowledge Dr. Mohammad Amin Hagh Bin for his valuable assistance in designing figures.
Author contributions
Farid Najd Mazhar and Hooman Shariatzade: conceptualization, supervision, manuscript writing (review & editing); Bushra Zareie: statistical analysis; Omid Mahmoudi Nasab, Ahmad Hasan, Narges Akhlaghi, Meisam Jafari Kafiabadi: data acquisition, literature review, manuscript writing (review & editing), final approval.
Data availability statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval declaration
Ethics approval with a waiver of consent was obtained from the Iran University of Medical Sciences Ethics Committee (IR.IUMS.REC.1403.1058).
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.