
Abstract
Background:
Hereditary multiple osteochondromas (HMO) affecting the proximal radius and ulna represent a rare condition with limited documentation in the clinical literature. This study aims to describe a rare presentation of HMO involving the proximal forearm and discusses potential implications for management.
Methods:
We retrospectively reviewed patients with HMO treated at our center between 2010 and 2021. Radiographic measurements included the presence or absence of osteochondromas in the entire forearm, radial head status, degree of ulnar bow, and ulnar length percentage. Radiographic measurements were compared using a Brown-Forsythe and Welch test with Tamhane’s T2 post hoc analysis.
Results:
A total of 12 patients with 14 forearms were included in the study. At the final follow-up, all patients with proximal ulnar tumors who did not undergo resection developed subluxation or dislocation. In contrast, all patients with proximal tumors limited in the radius remained free of subluxation or dislocation of the radial head throughout the follow-up period. The mean ulna length percentage in the Located group was 1.07 ± 0.05, while 1.09 ± 0.03 in the Subluxation group and 0.98 ± 0.09 in the Dislocated group. The mean ulna bow in Located group was 12° ± 7°, while 9° ± 6° in Subluxation group and 15° ± 8° in Dislocated group. No significant differences were observed.
Conclusions:
Proximal osteochondromas from the lateral side of the ulna may be a high-risk factor leading to radial head dislocation. Therefore, surgical excision of the proximal ulnar tumor could serve as a potential intervention to reduce the risk of radial head dislocation in affected patients.
Introduction
Hereditary multiple osteochondroma (HMO) is a rare autosomal dominant genetic disorder affecting endochondral ossification. 1 It most commonly arises from the growth plates of long bones, ribs, pelvis, and scapula, often resulting in cosmetic deformity, pain, and dysfunction.2–4 The forearm is the most common site in the upper extremity with evident growth disturbances. The prevalence has been reported to be as high as 60% in patients with HMO. 5
Forearm deformities typically occur initially due to ulnar shortening, followed by increased radial bowing and radial head dislocation. 6 Reports have showed that radial head subluxation or dislocation occurs in 20%–30% of patients. 7 A dislocated radial head is associated with reduced forearm rotation and functional impairment. 8 Once the radial head is dislocated, treatment becomes complex and requires a multidisciplinary approach to achieve favorable outcomes.9,10 Many scholars believe that the primary goal of early treatment is to prevent or mitigate the progression of deformity, particularly radial head dislocation. Therefore, it is imperative for clinicians to accurately classify HMO and thoroughly analyze the risk factors contributing to radial head dislocation.
Previous studies have identified osteochondroma location, proportional ulnar shortening, and ulna bowing as predictors of radial head subluxation or dislocation.7,11 Reports have shown that patients with proportional ulnar length of less than 0.9 had a higher risk of radial head dislocation than those with proportional ulnar length of 0.9 or greater, whereas no radial head subluxation or dislocation occurred in patients with an ulnar bow of <17°. 7 However, we found that proximal forearm osteochondromas around the proximal radioulnar joint (PRUJ) was more likely to be associated with radial head subluxation or dislocation. Furthermore, these cases presented with radial head dislocation despite normal proportional ulnar length and ulnar bow. However, the characteristics of this type of HMO have been poorly reported. Documenting such cases will provide essential insights for clinical treatment.
In this study, we focused on the proximal radius or ulna osteochondroma around the PRUJ in patients with HMO and aimed to analyze the association between osteochondromas of the proximal radius or ulna and radial head dislocation.
Methods
Following approval from our institutional review board, we conducted a retrospective study of patients diagnosed with HMO involving the forearm at our institution between 2010 and 2021. A total of 135 patients had involvement of the ulna and radius. Patients with proximal forearm osteochondromas were included in the study. Patients who had undergone previous operations for symptomatic forearm osteochondromas were excluded. We documented the demographic characteristics of each patient, including age at the time of initial radiographic assessment, sex, osteochondroma location, radiocapitellar joint status, and follow-up duration.
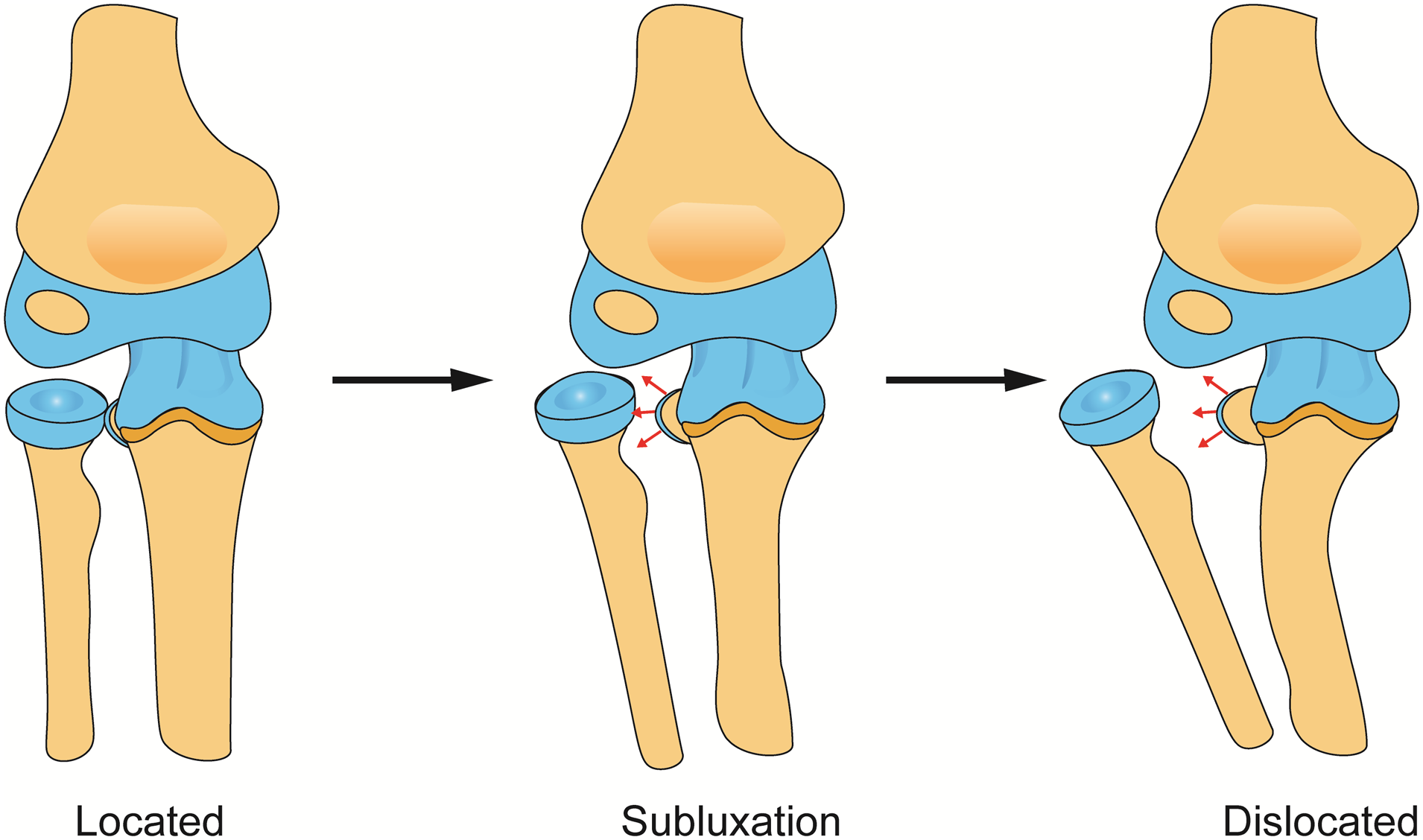
Patients were divided into three groups according to radial head status: located, subluxated, and dislocated. Subluxation and dislocation were determined either by intraoperative arthrography or radiographs using the methods described by Souder et al.
12
Forearm deformity was assessed based on previous reports, using ulnar length percentage and total ulnar bow (Figure 1).7,13 On anteroposterior radiographs, the ulnar/radial ratio was calculated as the length from the ulnar styloid tip to the olecranon edge divided by the radial length between the physeal centers, expressed as a percentage. The total ulnar bow was measured on orthogonal radiographs as the angle subtended by the proximal and distal mid-diaphyseal lines of the unla. The total ulnar bow was calculated as
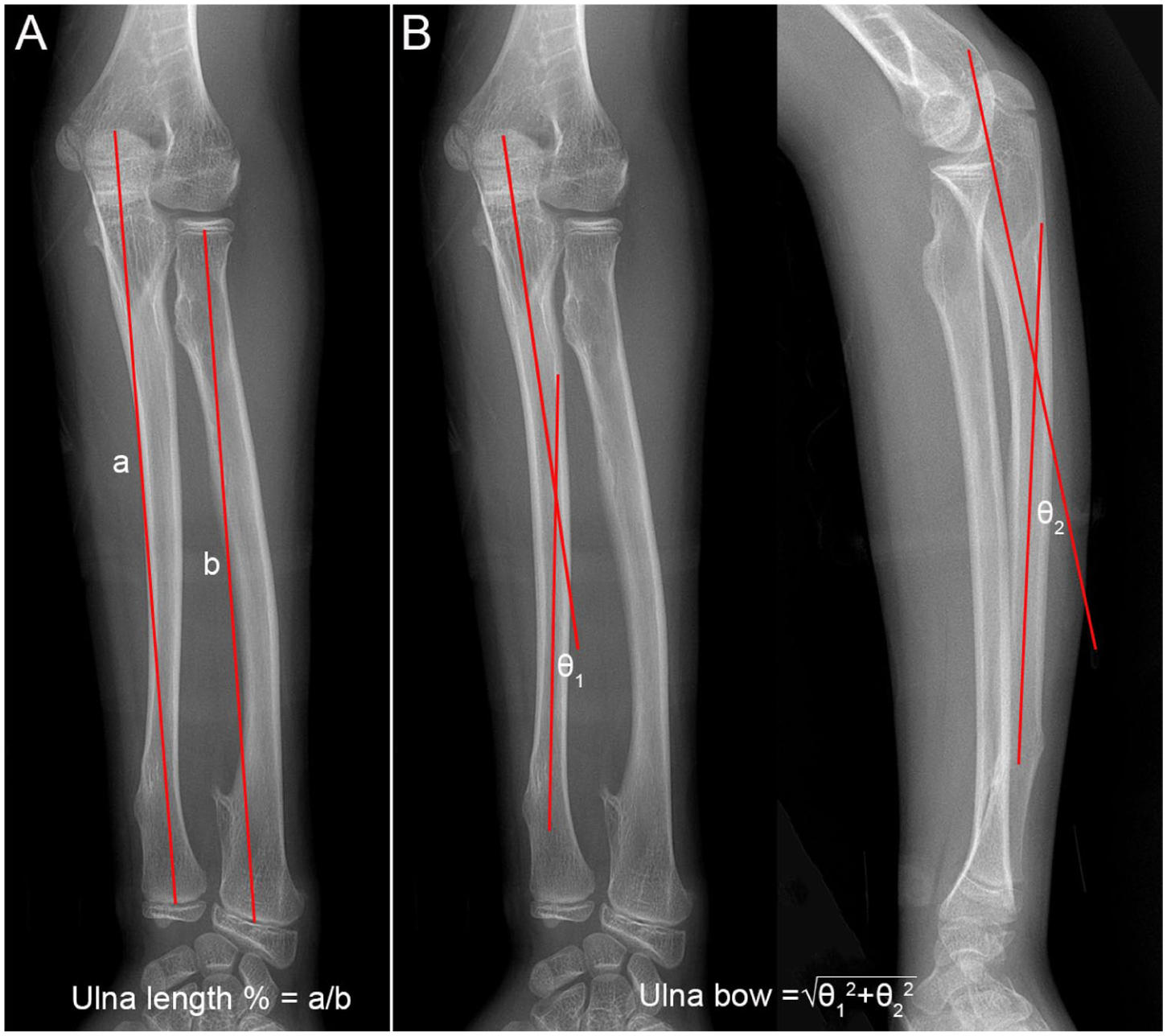
The radiographic measurements of ulna length percent (a) and ulna bow (b).
We used GraphPad Prism 8.02 (GraphPad Software, USA) in the descriptive and statistical analyses. Radiographic measurements were compared among groups using Brown-Forsythe and Welch test to assess differences in group distributions. Post hoc analysis was performed using Tamhane’s T2 test for multiple comparisons. All reported post hoc p-values were adjusted for multiple comparisons. A p-value of <0.05 was considered statistically significant.
Results
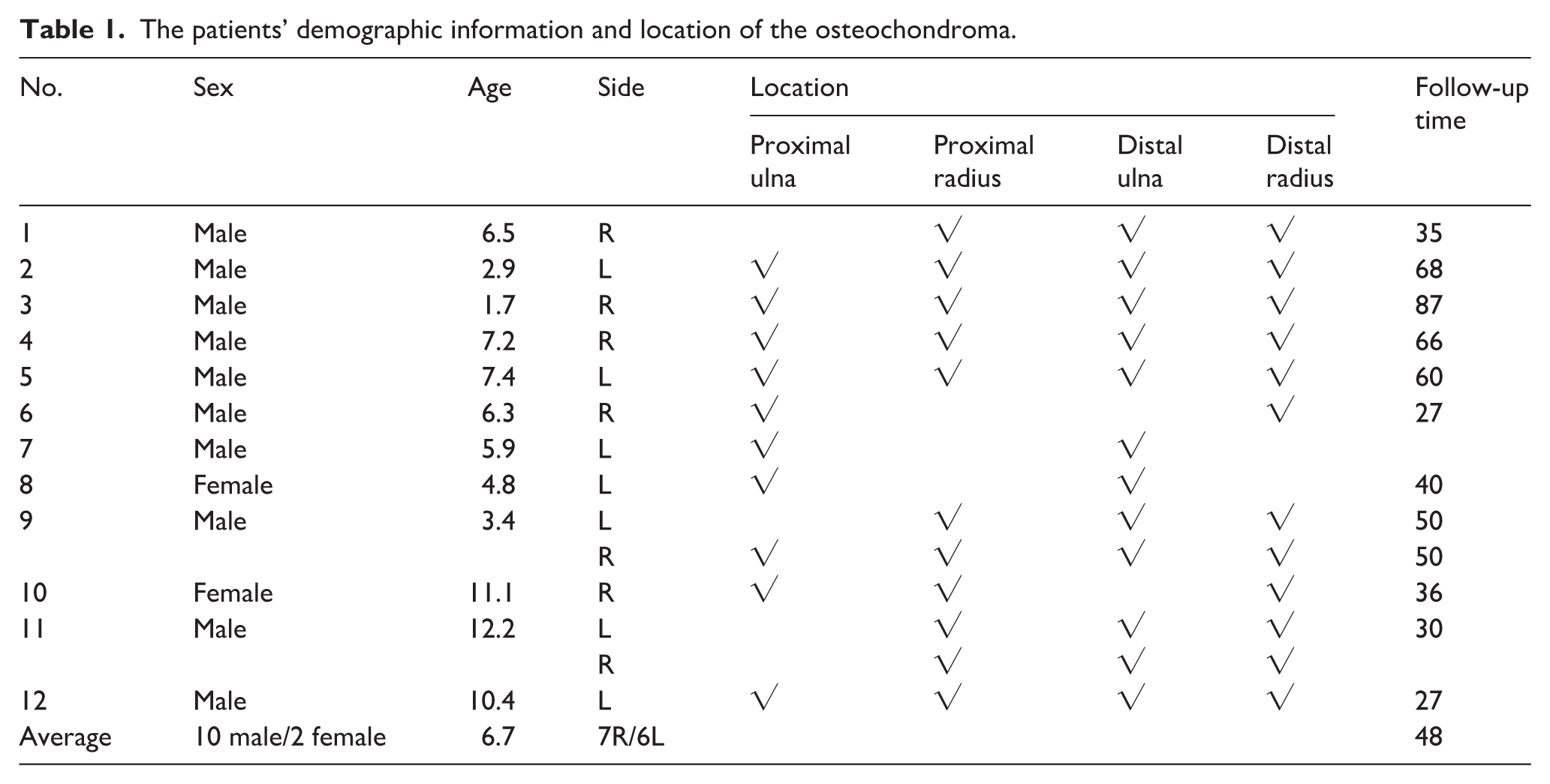
A total of 12 patients (14 forearms) were enrolled in this study, including 10 boys and 2 girls. The mean age at the initial radiographic examination was 6.7 years (ranging 1.7–12.2). Among them, seven patients had involvement of both the proximal ulna and proximal radius, three had isolated proximal ulnar involvement, and four had isolated proximal radial involvement. The minimum follow-up duration was 2 years. The demographic information is presented in Table 1.
The patients’ demographic information and location of the osteochondroma.
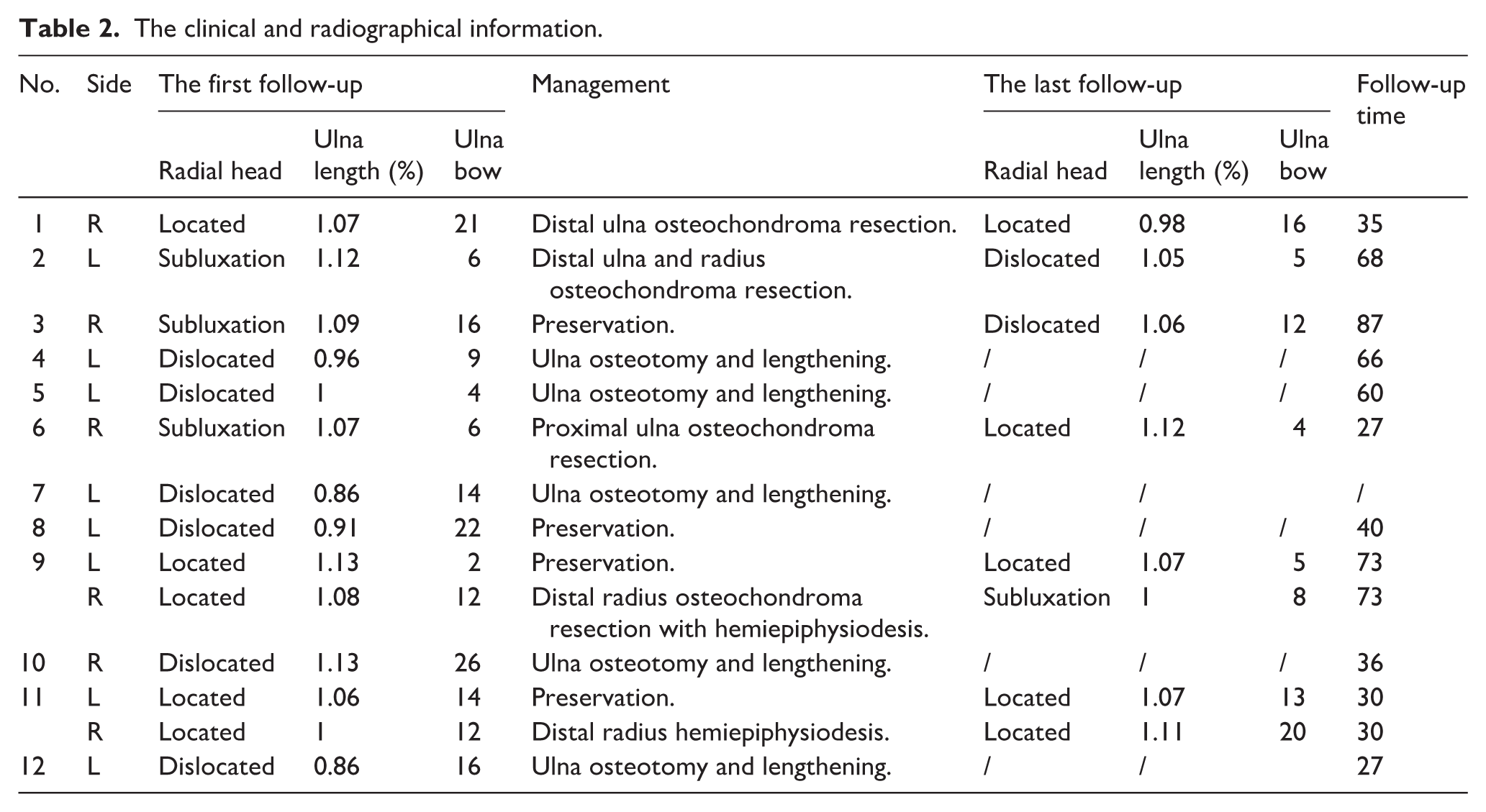
At the initial visit, six forearms presented with radial head dislocation, while three with radial head subluxation and five with located radial head. At the final follow-up, all patients (9 out of 10) with proximal ulnar tumors who did not undergo resection developed subluxation or dislocation. In contrast, all patients (four in four) with proximal tumors exclusively in the radius remained free of subluxation or dislocation of the radial head throughout the follow-up period. Detailed information is presented in Table 2.
The clinical and radiographical information.
The mean ulna length percentage in Located group was 1.07 ± 0.05, while 1.09 ± 0.03 in Subluxation group and 0.98 ± 0.09 in Dislocated group. There was no significant difference among them (Located versus Subluxation p = 0.73; Located versus Dislocated p = 0.19; Subluxation versus Dislocated p = 0.08). The mean ulna bow in Located group was 12° ± 7°, while 9° ± 6° in Subluxation group and 15° ± 8° in Dislocated group. There was no significant difference among them (Located versus Subluxation p = 0.91; Located versus Dislocated p = 0.89; Subluxation versus Dislocated p = 0.6). Only 33% of patients with radial head dislocation had ulnar length percentage below 0.9 at the initial visit, and 33% of patients with radial head dislocation had ulnar bow greater than 17° (Figure 2). All patients with radial head dislocation had a lateral prominence deformity of the elbow. Among the subluxation and dislocated groups, four patients presented with restricted elbow extension (95.0° ± 7.0°) and flexion (21.3° ± 6.3°).
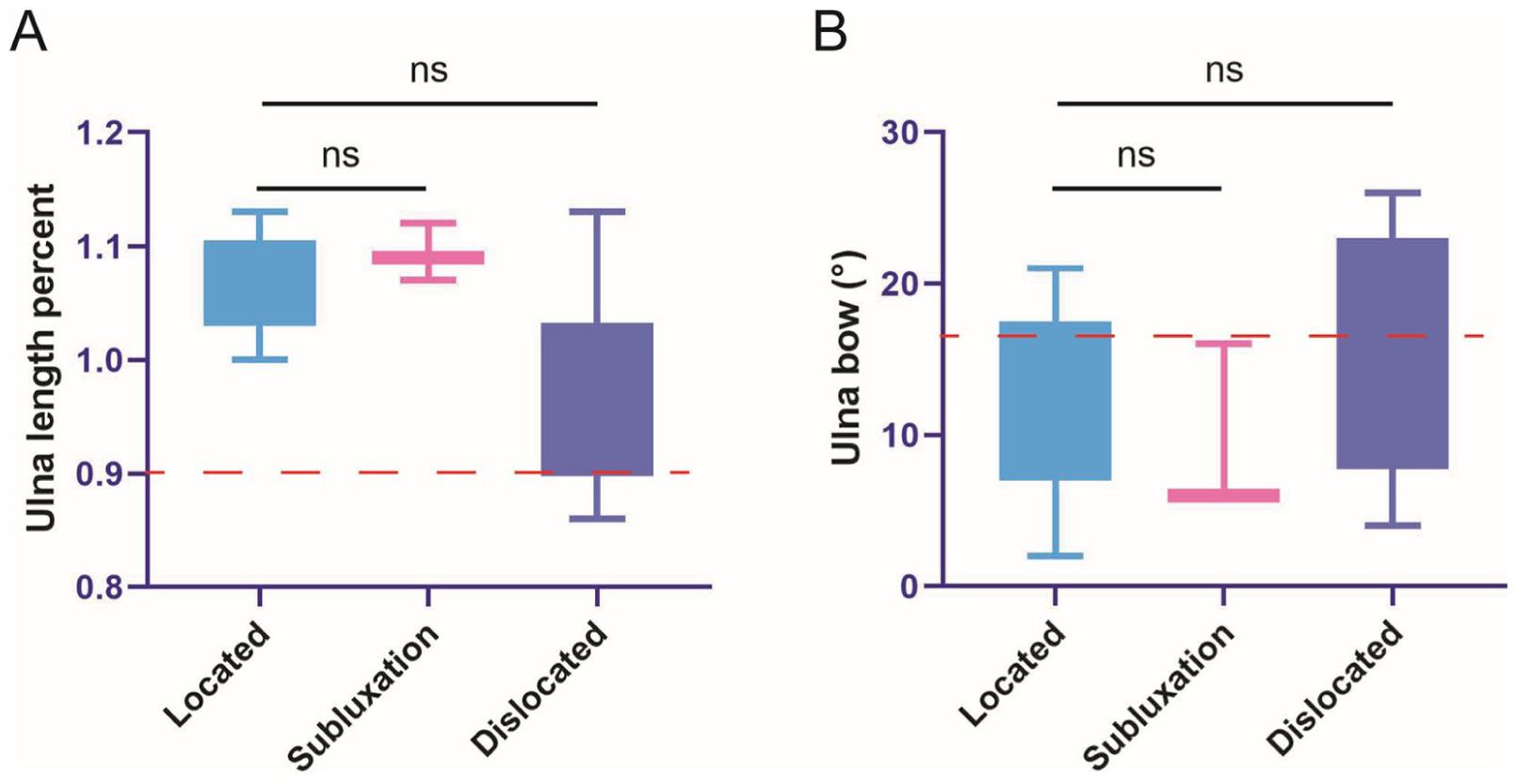
Box and whisker plots showing the range of ulna length percent (a) and ulna bow measurements (b). ns: p > 0.05. The red line indicate the risk factor number (0.9 in a; 17° in b).
Despite distal radius tumor resection and hemiepiphysiodesis performed on the right forearm in case 9, persistent radial head subluxation was observed during follow-up (Figure 3). In case 6, however, excision of the proximal ulnar tumor alone led to normalization of the radial head from subluxation (Figure 4). In case 1, enlargement of a solitary osteochondroma of the proximal radius did not lead to radial head dislocation during conservative follow-up (Figure 5).
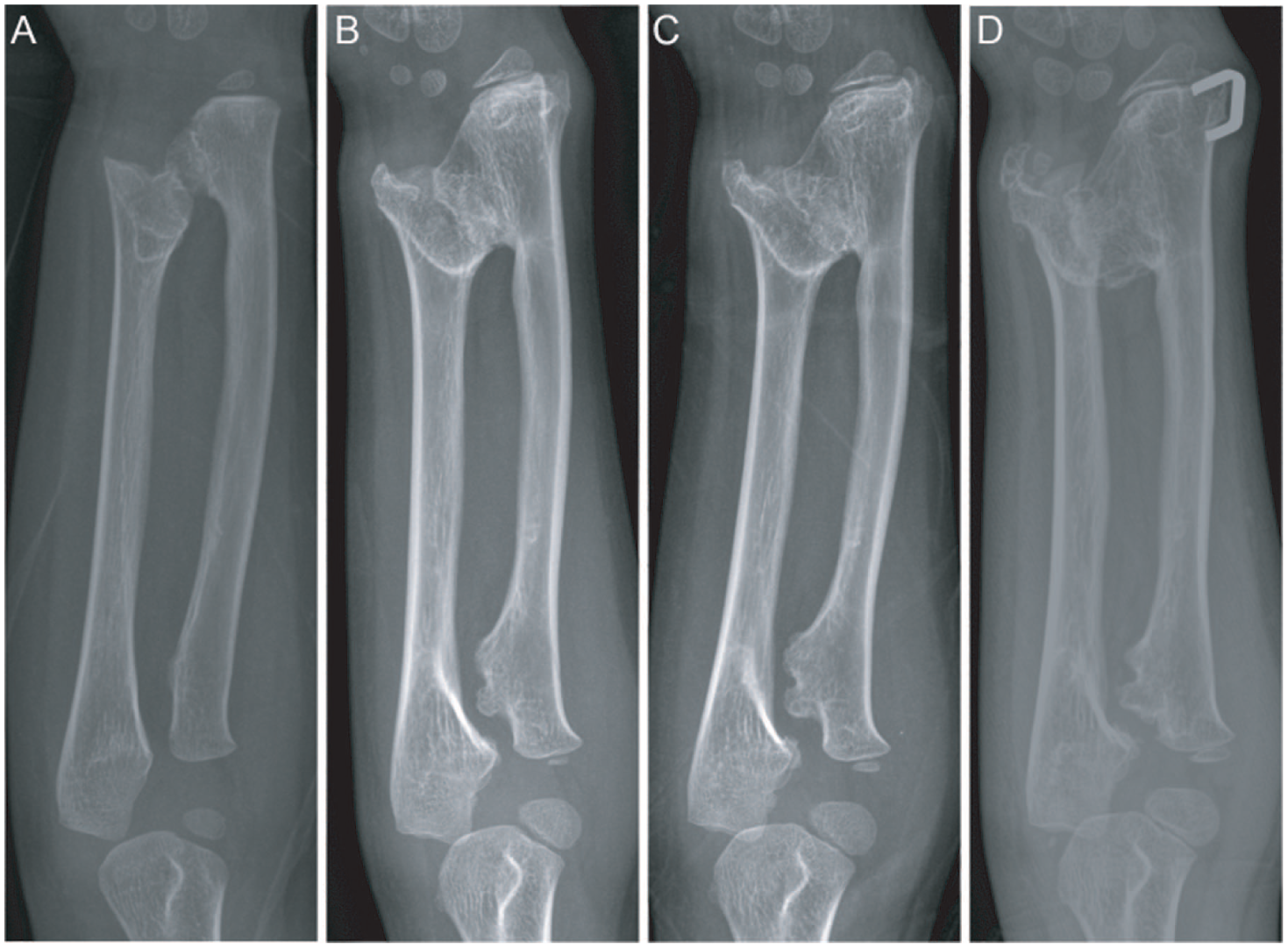
Case 9 was a 3.4-year-old patient presenting with a proximal ulnar and radius osteochondromas. The proximal ulnar and radius tumors were managed conservatively without surgical intervention, but showed progressive subluxation during follow-up. (a) The initial visit; (b) after 44 months follow-up; (c) after 52 months follow-up; (d) after 73 months follow-up.
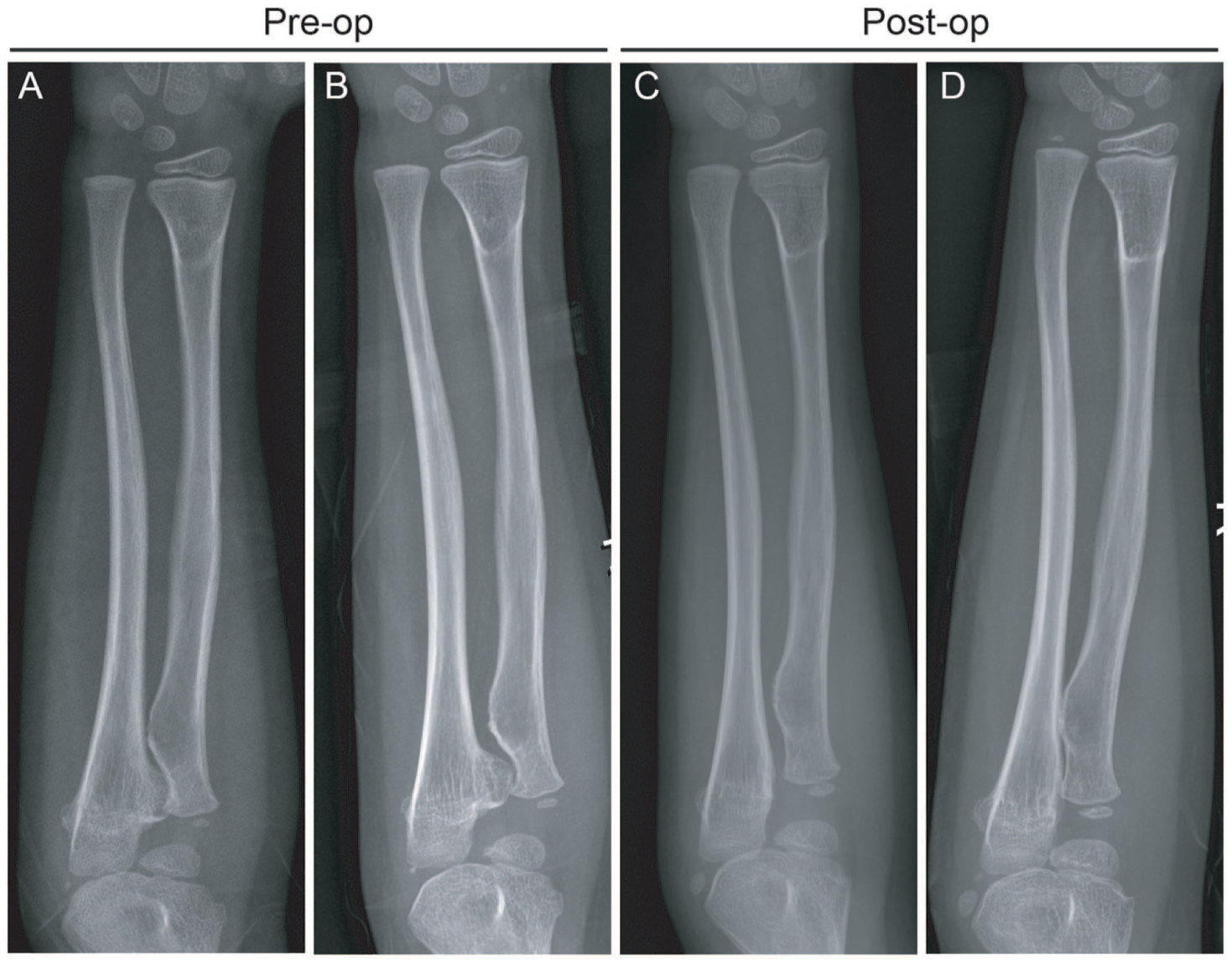
Case 6 involved a 6.3-year-old patient presenting with a proximal ulna osteochondroma and radial head subluxation. The osteochondroma was promptly excised, and subsequent follow-up revealed the resolution of the radial head subluxation. (a) The initial visit; (b) after 6 months follow-up before surgery; (c) postoperative 13 months; (d) postoperative 20 months.
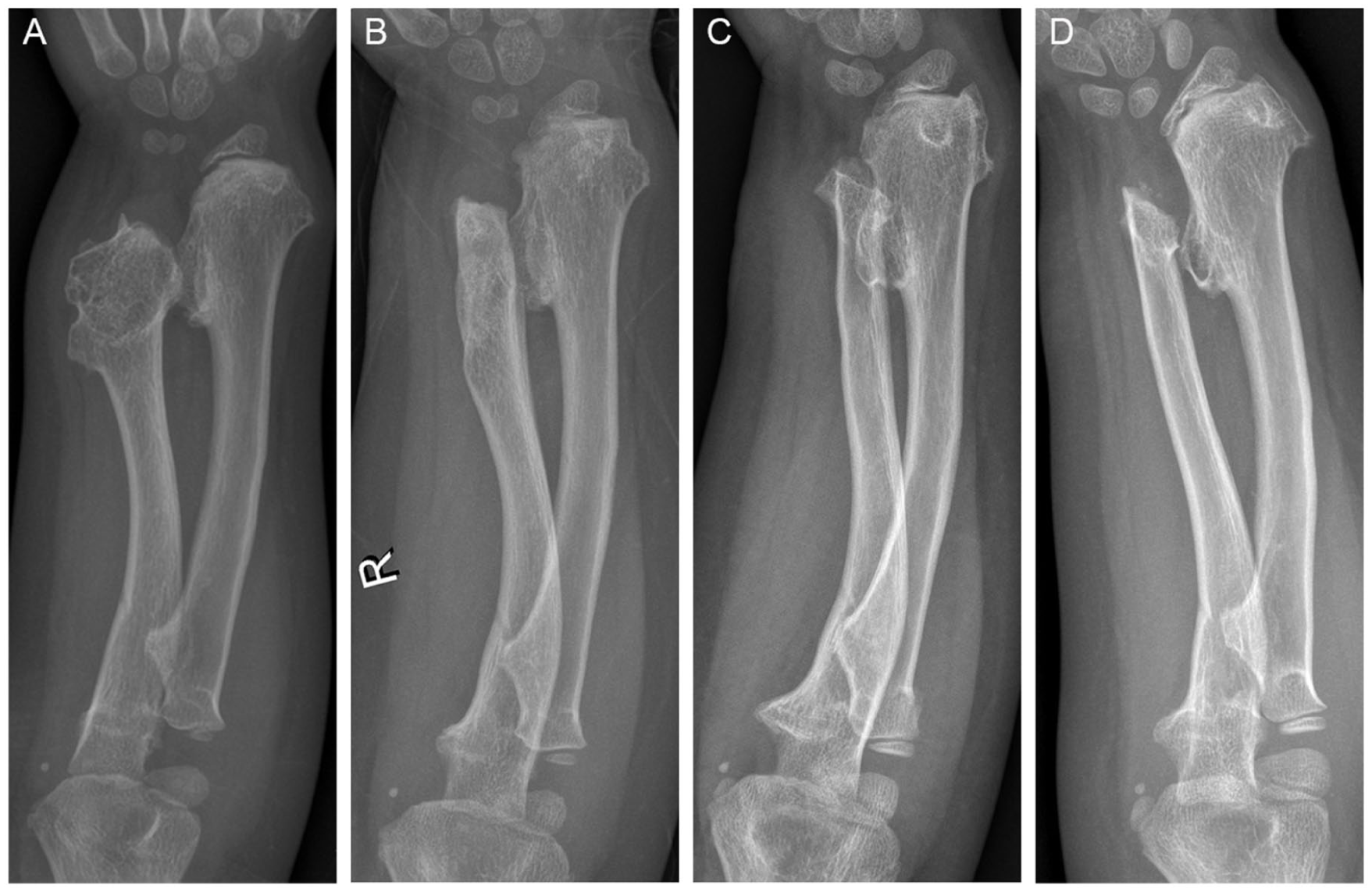
Case 1 involved a 6.5-year-old patient presenting with a proximal radius osteochondroma, without any evidence of osteochondroma in the proximal ulna. The patient undergone distal ulna osteochondroma resection without surgical intervention for the radial osteochondroma and showed no signs of radial head dislocation during follow-up. (a) The initial visit before surgery; (b) postoperative 2 months; (c) postoperative 24 months; (d) postoperative 35 months.
Discussion
HMO is a rare autosomal dominant disorder characterized by the formation of multiple benign osteochondromas, which can result in significant skeletal deformities and growth disturbances in pediatric populations. 14 Due to the extremely difficult treatment of radial head dislocation, there is currently no consensus on the most effective operative techniques for this condition. 15 Orthopedic surgeons currently seek to identify risk factors associated with radial head dislocation and favor more aggressive treatment to prevent radial head subluxation. 13 In our study, we focused on the proximal radius or ulna osteochondromas around the PRUJ and found that all patients with proximal ulnar osteochondromas who did not undergo proximal ulna resection presented with radial head subluxation or dislocation, whereas those with isolated proximal radial osteochondromas did not exhibit dislocation. Furthermore, there was no significant correlation between ulnar length ratio or ulnar bow and radial head dislocation in patients with proximal ulnar osteochondroma. These findings suggest that the proximal ulnar osteochondroma may represent an independent risk factor for radial head dislocation, indicating a potential need for further investigation into the underlying mechanisms and clinical implications.
The location of osteochondromas has been linked to the progression of forearm deformity, for instance, larger lesions at the distal ulna have been associated with ulnar shortening, radial bowing, dislocation of the radial head, and decreased forearm rotation. 16 As osteochondromas most frequently affects the distal ulna and radius, previous research has primarily focused on addressing forearm malformation and preventing radial head dislocation at this anatomical site. 16 Masada et al. conducted a comprehensive analysis of forearm osteochondroma in 13 pediatric patients, stratifying them into 3 distinct types based primarily on the anatomical location within the distal radius, distal ulna, and the presence of concomitant radial head dislocation. Based on the Masada classification, Jo et al. proposed the addition of type 4, which includes osteochondromas in the distal ulna and radius.13,17 Gottschalk et al. categorized forearm osteochondromas into five types based on their specific locations along the entire forearm, and for the first time, focused on osteochondromas located at the proximal ulna and radius. 6 Due to the limited number of cases, the authors refrained from providing detailed information on the characteristics of this type. In our study, among 135 HMO patients with forearm involvement, only 12 patients were identified with proximal ulna or radius involvement, representing an incidence of approximately 9% among those with forearm involvement. To the best of our knowledge, this is the first study to investigate the association between proximal forearm osteochondromas and radial head dislocation.
In the past, the surgical indications for HMO included limb pain, cosmetic deformity, joint dysfunction, malignant transformation, and neurovascular compression by the tumor. Tumor-induced ulnar shortening and angulation are now recognized as the primary factors contributing to radial head subluxation. Various procedures have been used to correct forearm deformities and prevent radial head dislocation, including ulnar lengthening, hemiepiphysiodesis, and osteotomy.15,18–20 Lu et al. found that distraction osteogenesis at the proximal third of the ulna provides satisfactory clinical and radiological outcomes in patients with Masada type I and IIb deformities. 10 Belyea et al. found that surgical excision of forearm osteochondromas with ulnar tether release may help prevent subsequent surgical reconstruction and provides satisfactory clinical outcomes. 20 In this study, all patients with osteochondromas of the proximal ulna presented with radial head dislocation. Following resection of the proximal ulnar osteochondroma in one case, the radial head transitioned from subluxation to a normal state. These findings suggest that early resection of proximal ulnar tumors is a reliable method for preventing radial head dislocation, supporting the potential efficacy of timely surgical intervention in mitigating this complication.
The prolonged and continuous pressure exerted by the proximal ulnar osteochondroma on the radial neck may be the primary factor leading to radial head dislocation. The key to effectively treating this type of tumor lies in alleviating the chronic pressure exerted on the ulna, which is essential for successful management and long-term outcomes. In this study, four affected patients with proximal forearm involvement showed osteochondromas only in the radius, without ulnar involvement. No radial head dislocation was observed during follow-up. We postulate that the absence of dislocation in these cases is likely due to the radial tumor being located near the radial tuberosity, thus exerting minimal pressure on the ulna. We hypothesize that tumors at the proximal ulna that exert pressure on the radius may constitute a risk factor for radial head dislocation, although such occurrences have not been documented.
The study still has several limitations. First, the sample size in this study was small and the follow-up period did not extend to skeletal maturity. Second, as a retrospective study, it lacks sufficient cases to definitively conclude that resection of the proximal ulna tumor effectively prevents radial head dislocation. Subsequent large-scale, multi-center studies are necessary to corroborate these findings.
In conclusion, proximal osteochondromas arising from the lateral side of the ulna are highly suspected to be an independent risk factor for radial head dislocation. Therefore, surgical excision of the proximal ulna tumor may serve as a potential intervention to reduce the risk of radial head dislocation in affected individuals.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261461011 – Supplemental material for Proximal ulnar osteochondroma as a potential risk factor for radial head dislocation: A retrospective analysis
Supplemental material, sj-pdf-1-cho-10.1177_18632521261461011 for Proximal ulnar osteochondroma as a potential risk factor for radial head dislocation: A retrospective analysis by Han Xiao, Miao Li, Xiaoqian Tan, Qian Tan, Weihua Ye, Jiangyan Wu, Kun Liu, Haibo Mei, Guanghui Zhu and An Yan in Journal of Children's Orthopaedics
Footnotes
Acknowledgements
We thank the members of the Hunan Children’s Hospital for supporting this study. We acknowledge the program (the 14th Five-Year Plan Application Characteristic Discipline of Hunan Province (Clinical Medicine)) for its support of our project.
Author contributions
A.Y. and H.X. designed experiments. H.X., G.Z., X.T., Q.T., J.W., W.Y., H.M. and J.T. measured and collected the data. M.L., A.Y. and H.X. analyzed the data. H.X. and A.Y. wrote the manuscript. G.Z., A.Y., and H.X. assisted in the experiments and preparation of the manuscript.
Consent to publish
This work is approved by all authors for publication in the Journal of Children’s Orthopaedics.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by Hunan Provincial Medical Discipline Construction Project (xcsz [2025] No. 0084) Natural Science Foundation of Hunan Province, China (Grant No. 2026JJ60450).
Ethical approval
This is a retrospective observational study involving human participants and it was approved by Ethics Committee of Hunan Children’s Hospital (HCHLL-2026-177). All participants gave informed consent.
Availability of data and materials
The datasets generated and analyzed during the current study are available from the corresponding author upon reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.