
Abstract
Purpose:
To compare revision and complication rates between telescopic and non-telescopic intramedullary rods in children with osteogenesis imperfecta (OI).
Methods:
A systematic review was conducted according to Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines and registered in the PROSPERO database (CRD42021287054). Databases were searched up to December 2025. Studies reporting surgical outcomes of intramedullary fixation in OI were included. Meta-analysis was performed using random-effects models.
Results:
Thirty-six studies including 1711 patients and 2459 treated bones were analyzed. Telescopic rods were associated with significantly lower revision rates compared to non-telescopic rods. No significant difference in overall complication rates was observed.
Conclusion:
Telescopic rods provide improved implant survival and reduce the need for reoperation in growing children with osteogenesis imperfecta, supporting their preferential use in clinical practice.
Keywords
Introduction
Osteogenesis imperfecta (OI) is a congenital connective tissue disorder characterized by qualitative or quantitative alterations in type I collagen. The main clinical manifestations include skeletal deformities and bone fragility, resulting from lower mineral density. Extra-skeletal features commonly associated with OI include blue sclera, dentinogenesis imperfecta, vascular fragility, and hearing loss. 1
Among the pharmacological treatments available, the use of bisphosphonates has gained recognition in recent years due to studies demonstrating their efficacy, supporting and recommending their application. 2 The concentration of bisphosphonates in the mineralized bone matrix inhibits bone resorption by osteoclasts and favors an increase in bone mineral density. The treatment is associated with outcomes such as increased cortical thickness, height of the vertebral body, and a reduction in musculoskeletal pain and fatigue. 3
Orthopedic surgery remains a cornerstone in the management of deformities and fracture prevention in moderate to severe OI. 4 Several devices are available for stabilizing fractures or bones that have undergone osteotomy. However, the bones of patients with OI are fragile, and some of these devices–such as an isolated plate–can create points of weakness at their ends, predisposing the bone to fractures. Intramedullary fixation is widely considered the most effective strategy for stabilizing fractures and osteotomies in OI. Non-telescopic intramedullary devices provide initial stability but lose effectiveness over time as the bone grows longitudinally, when the nail becomes proportionally smaller in relation to the bone. 4 In a meta-analysis of non-telescopic intramedullary fixation in patients with OI, the reoperation rate was 39.4% across 7 studies (n = 229 patients) that met the inclusion criteria. 4
The telescopic rod was developed to provide stability and protection during bone growth. The rod occupies the medullary canal and telescopes as the bone grows longitudinally. Different types of telescopic rods are available, with the Fassier-Duval (FD) rod currently being the most widely used intramedullary growth device in the surgical treatment of OI.5–8 Unlike older telescopic rods, the FD rod can be inserted through a single incision at one end of the bone, preserving the other. This approach allows for a more biological procedure with reduced morbidity.8,9 However, the FD rod is more expensive and requires a longer learning curve compared to non-telescopic implants.10,11 Complications, including joint invasion, migration, limitations in telescoping, and structural deformity of the FD rod, have been documented.8,12
Several studies13–18 have demonstrated the advantages of telescopic fixation over non-telescopic fixation. The aim of this study was to compare the rates of complications and reoperations associated with the use of telescopic versus non-telescopic rods in patients with OI. Through a systematic review, we seek to assess the frequency of complications and surgical revisions associated with each approach, while also estimating the relative risks of these outcomes between the two treatment modalities.
Methods
Registration and protocol
This review was registered in the PROSPERO database—registration number: CRD42021287054. The systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses 19 guidelines and the methodological recommendations outlined in the Cochrane Handbook for Systematic Reviews of Interventions. 20
Eligibility criteria
The inclusion criteria for selecting studies were: publication in scientific journals between 01/01/2000 and 12/31/2025; evaluation of patients diagnosed with OI undergoing surgical treatment (osteotomies to correct deformities or fractures) with intramedullary bone fixation; reporting the number of procedures and their outcomes, including the number of complications and/or reoperations; and description of the type of rod used in the procedure.
Studies including populations with conditions other than OI, studies that did not specify the type of rod used, case reports, systematic reviews, meta-analyses, and studies published outside the specified date range were excluded.
Information sources and search strategies
The original literature search was conducted in January 2024 and was subsequently updated in April 2026 to identify newly published studies. Both searches were performed using the same predefined methodology and search strategy across three electronic databases: Medline/PubMed, Embase, and LILACS. The search strategy included the descriptors “osteogenesis imperfecta” and “surgery,” combined using the expression (“osteogenesis imperfecta” AND surgery). The updated search expanded the publication period to include studies published between 2000 and December 2025. No language or country restrictions were applied.
Study selection
The study selection process was conducted independently by two authors (M.O.C. and M.P.S.), with any divergence resolved by a senior researcher (R.Y.). The selection followed a three-stage process: (1) screening of titles, (2) screening of abstracts, and (3) retrieval and thorough reading of full texts to apply the eligibility criteria.
Data extraction process
Data from the included studies were independently extracted into a spreadsheet by three members of the research team. In cases of disagreement regarding the extracted data, the decision of the senior author was followed.
Data items
General study characteristics extracted included the year of publication, country, and study design. Population data included the number of patients assessed, gender distribution (when available), patient age, Sillence classification, and follow-up duration. Procedure- and outcome-related data included the total number of bone segments operated on, the number of operations by bone type, the number of procedures by rod type, the number and categories of complications, the number of revisions, and the interval between the initial surgery and the first revision.
In this study, a revision was defined as the need for reoperation of the rod after the initial procedure. The primary outcomes assessed were the occurrence of complications and the need for surgical revision.
Synthesis methods and effect measures
Data were described with frequency and confidence interval for qualitative variables, and measures of central tendency (mean and median) and measures of dispersion (standard deviation, interquartile range, minimum, and maximum) for quantitative variables. All the statistical tests used a two-tailed α (p-value) of 0.05 and a 95% confidence interval (CI).
The number of bone segments that underwent surgical procedures and the assessment of the need for correction and revision were considered as the analytical unit for the combined effect of the studies. Data were grouped according to the type of rod used in the surgical procedure to compare outcomes (1) occurrence of complications and (2) need for revision. Pooled effects were calculated using meta-analysis models with the inverse variance method. Heterogeneity was considered substantial when I² exceeded 70%. When heterogeneity was not significant, fixed effects models were used. Heterogeneity between studies was assessed visually using Forest Plots and tested statistically with the I² test.
The analyses were performed using R Studio software (R Foundation for Statistical Computing, Vienna, Austria) with the metafor package.
Study risk of bias and certainty assessment
The methodological quality of individual studies was assessed using the Joanna Briggs Institute Critical Appraisal Tools, 21 tailored to each study design. Studies were categorized as having low risk of bias (≥80% of “yes” responses), moderate risk of bias (60%–79% of “yes” responses), or high risk of bias (<60% of “yes” responses). To evaluate the overall confidence in the review findings, the GRADE approach was employed, considering factors such as risk of bias, inconsistency, and imprecision in the evidence synthesis.
Assessment of publication bias
To evaluate the presence of publication bias, a funnel plot was constructed to visually assess asymmetry in the distribution of study effect sizes. As recommended by Higgins et al. 20 this analysis was performed only when at least 10 studies were included in the meta-analysis, ensuring sufficient statistical power to detect asymmetry.
Additionally, Egger’s regression test was conducted to statistically quantify the presence of asymmetry and potential publication bias. A p-value < 0.05 from Egger’s test was considered indicative of significant publication bias.
Results
Study selection
The search strategy resulted in 970 records: 492 in the Medline/PubMed database, 439 in Embase and 39 in LILACS. After excluding duplicates and screening by title and abstract, 128 studies were carefully analyzed by the authors through full-text reading. Finally, 36 studies that met the eligibility criteria were selected for this systematic review. The flowchart representing the study selection is shown in Figure 1.
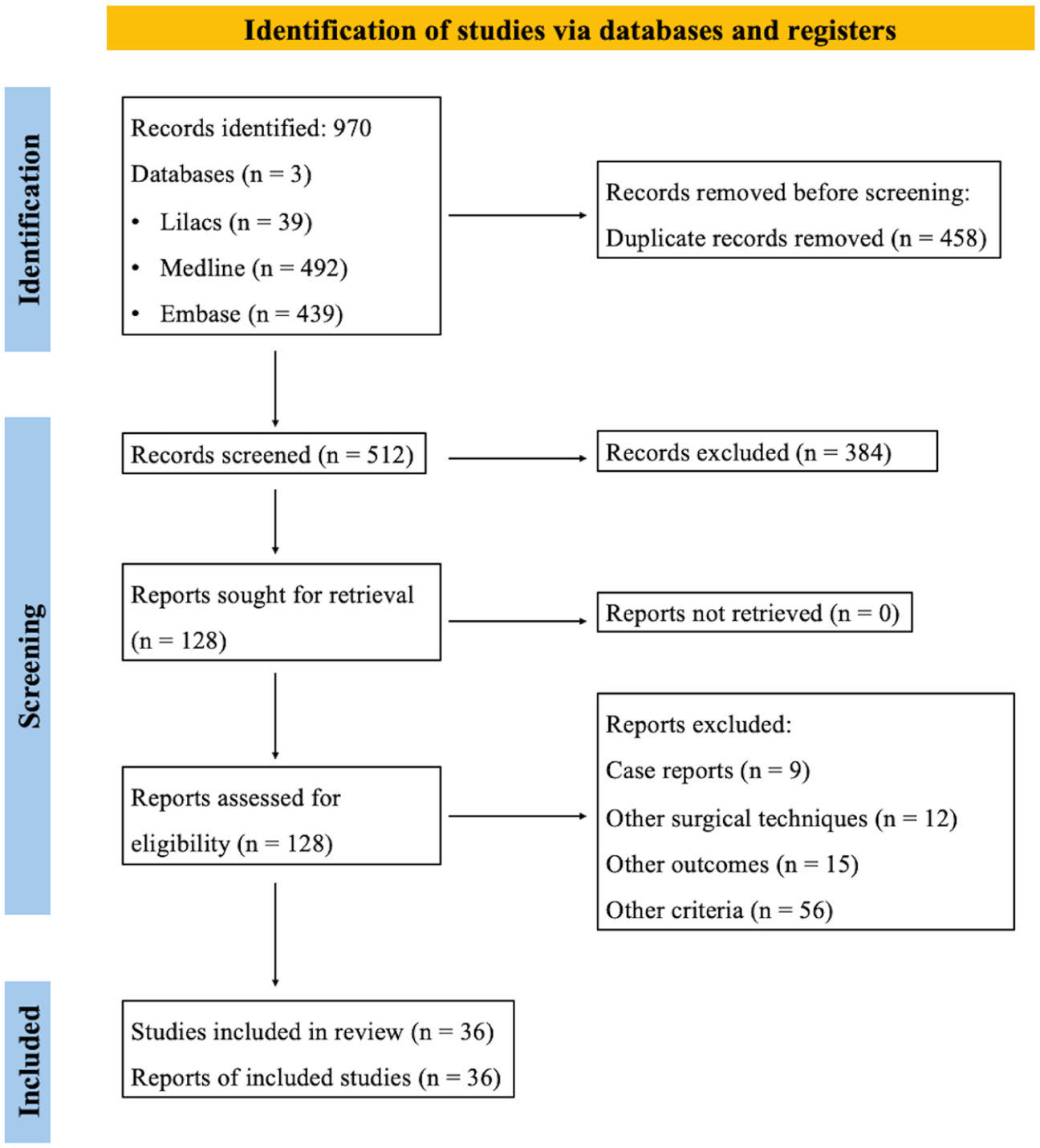
Flowchart for selecting studies on the treatment of patients with OI and the use of telescoped and non-telescoped rods.
Study characteristics
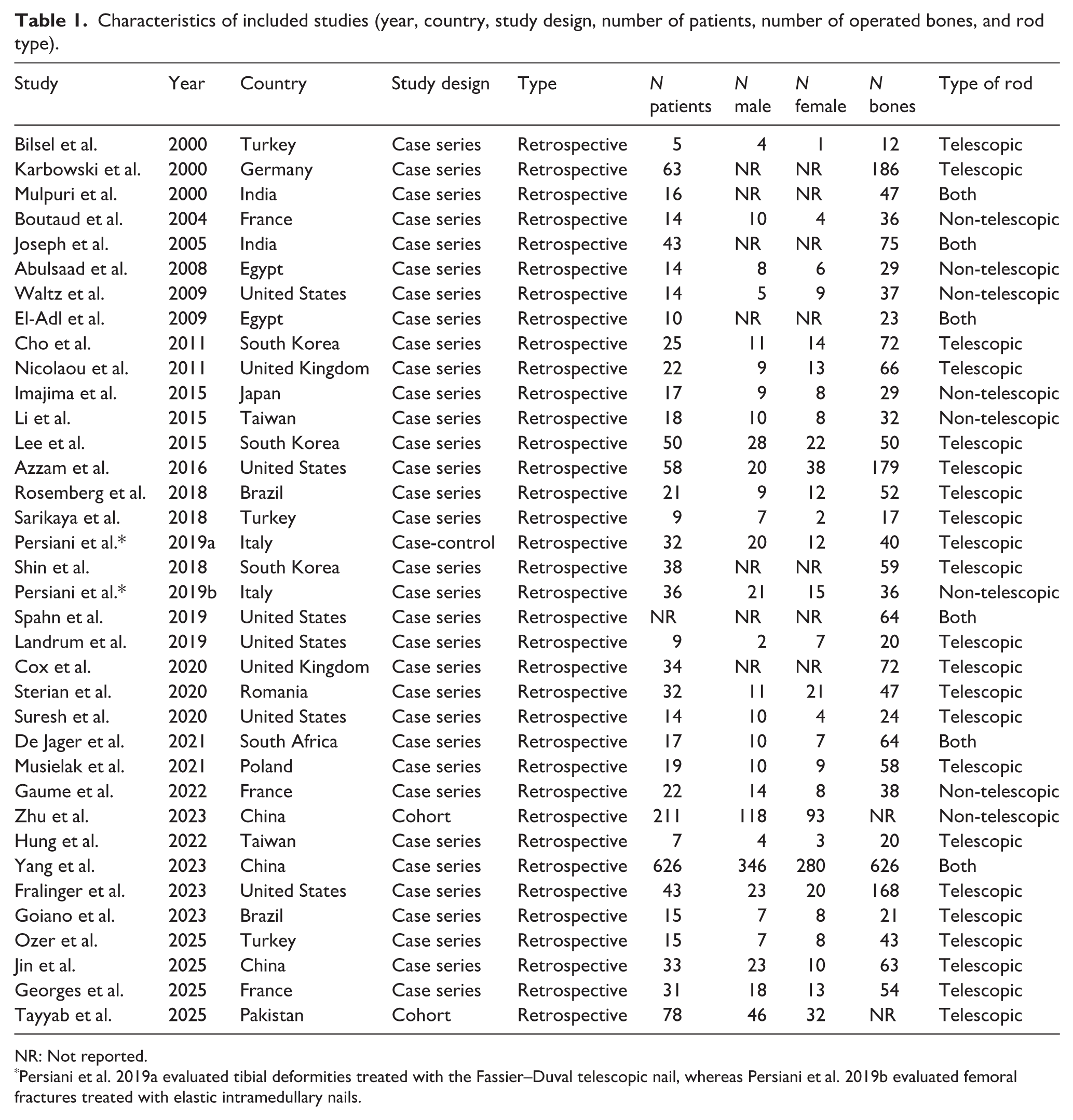
The general characteristics of the included studies are presented in Table 1. The studies were published between 2000 and 2025, and the majority followed a case series design (33 out of 36—91.7%; 95% CI 79.4%–97.6%), with 2 cohort studies (5.6%; 95% CI 1.2%–16.6%) and 1 case-control study (2.8%; 95% CI 0.3%–12.3%). Only one study was prospective (2.8%; 95% CI 0.3%–12.3%) and all the other studies were retrospective (97.2%; 95% CI 87.7%–99.7%). The studies were conducted in 17 different countries, with the United States having the highest frequency (6/36 studies, 16.7%), followed by China, South Korea, France, and Turkey (3/36 each, 8.3%), Brazil, Egypt, India, Italy, Taiwan, and the United Kingdom (2/36 each, 5.6%). South Africa, Germany, Japan, Pakistan, Poland, and Romania each had one study (1/36, 2.8%).
Characteristics of included studies (year, country, study design, number of patients, number of operated bones, and rod type).
NR: Not reported.
Persiani et al. 2019a evaluated tibial deformities treated with the Fassier–Duval telescopic nail, whereas Persiani et al. 2019b evaluated femoral fractures treated with elastic intramedullary nails.
Of the 36 studies included, 22 described the exclusive use of telescopic rods3,22–37 (61.1%; 95% CI 44.8%–75.7%), 8 described non-telescopic rods38–45 (22.2%; 95% CI 11.1%–37.6%), and 6 studies evaluated both types of rods13–17,46 (16.7%; 95% CI 7.3%–31.2%).
A total of 1711 patients underwent orthopedic surgery, with 1507 (88.6%) having their sex reported: 820 (54.4%) males and 687 (45.6%) females. The studies included an average of 49 patients, with sample sizes ranging from 5 to 626 patients.
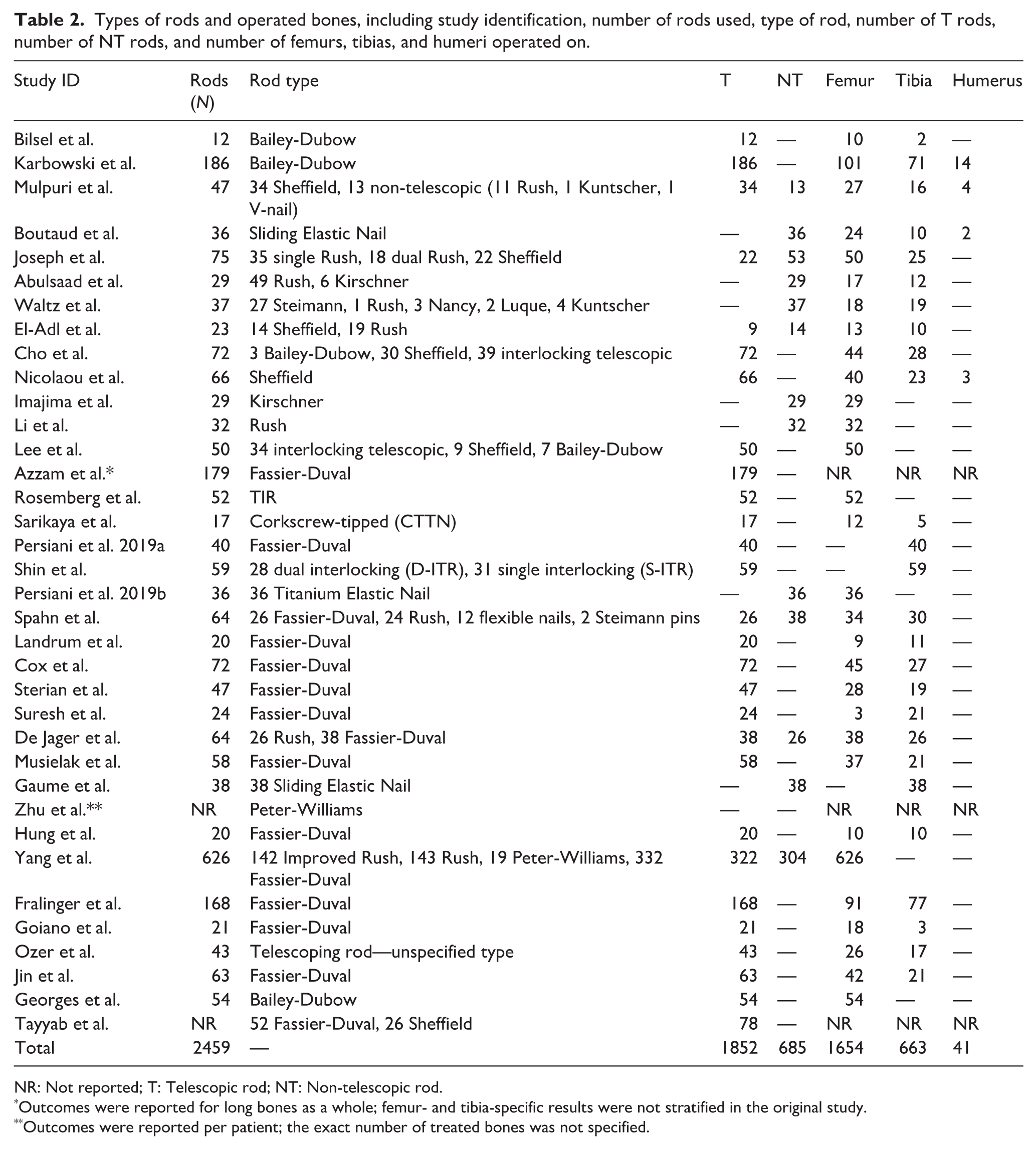
A total of 2459 bones underwent intramedullary fixation across the included studies (Table 2). Two studies did not specify which bone segments were operated on,27,45 accounting for 179 bones (femur, tibia, or humerus). However, it was possible to identify procedures on 2358 bone segments (95.9%), including 1654 femurs (70.1%), 663 tibias (28.1%), and 41 humeri (1.7%). Most telescopic rods used were of the Fassier-Duval type.
Types of rods and operated bones, including study identification, number of rods used, type of rod, number of T rods, number of NT rods, and number of femurs, tibias, and humeri operated on.
NR: Not reported; T: Telescopic rod; NT: Non-telescopic rod.
Outcomes were reported for long bones as a whole; femur- and tibia-specific results were not stratified in the original study.
Outcomes were reported per patient; the exact number of treated bones was not specified.
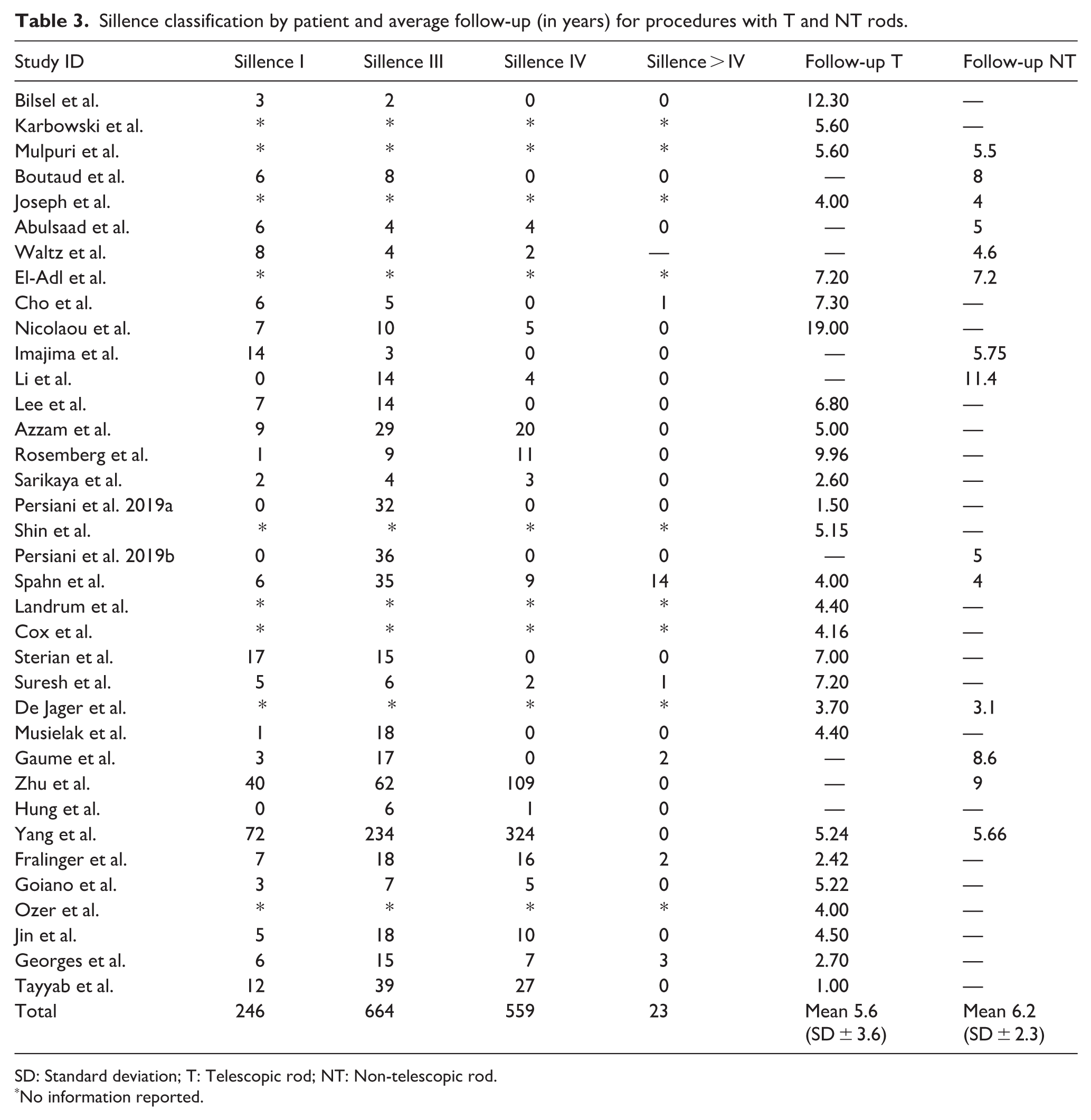
According to the classification by Sillence et al. 47 most studies differentiated the OI types between patients and operated bone segments. De Jager et al. 16 and Shin et al. 31 related the Sillence types only to the bones that underwent surgery, while Cho et al., 24 Azzam et al. 27 and others3,15,17,26,30,34,35,38,39,43,48–52 related the Sillence types only to patients (Table 3). Among the 1711 patients included, the Sillence classification was identified in 1492 (87.2%). Procedures were carried out on 246 patients classified as Sillence I or II (16.5%), 664 as Sillence III (44.5%), 559 as Sillence IV (37.5%), and 23 as Sillence V or higher (1.5%).
Sillence classification by patient and average follow-up (in years) for procedures with T and NT rods.
SD: Standard deviation; T: Telescopic rod; NT: Non-telescopic rod.
No information reported.
The average follow-up for patients with bones fixed using telescopic rods was 5.6 years (SD ± 3.6 years; range: 1–19 years), and for non-telescopic rods, it was 6.2 years (SD ± 2.3 years; range: 3.1–11.4 years).
The patients who underwent intramedullary fixation described in the included studies had an average age ranging from 4 to 10 years, with an overall average of 6 years (SD ± 1.4 years) for those with telescopic rods, and an average of 7 years (SD ± 1 year), ranging from 5 to 10 years for those with non-telescopic rods. All reported procedures were primary surgeries, performed for either deformity correction or fracture stabilization. The most frequent complications for both rod types are summarized in Table 4, with migration being the most frequent complication for patients with telescopic rods and fracture being the most frequent for those with non-telescopic rods.
Types of complications per patient described in the included studies.
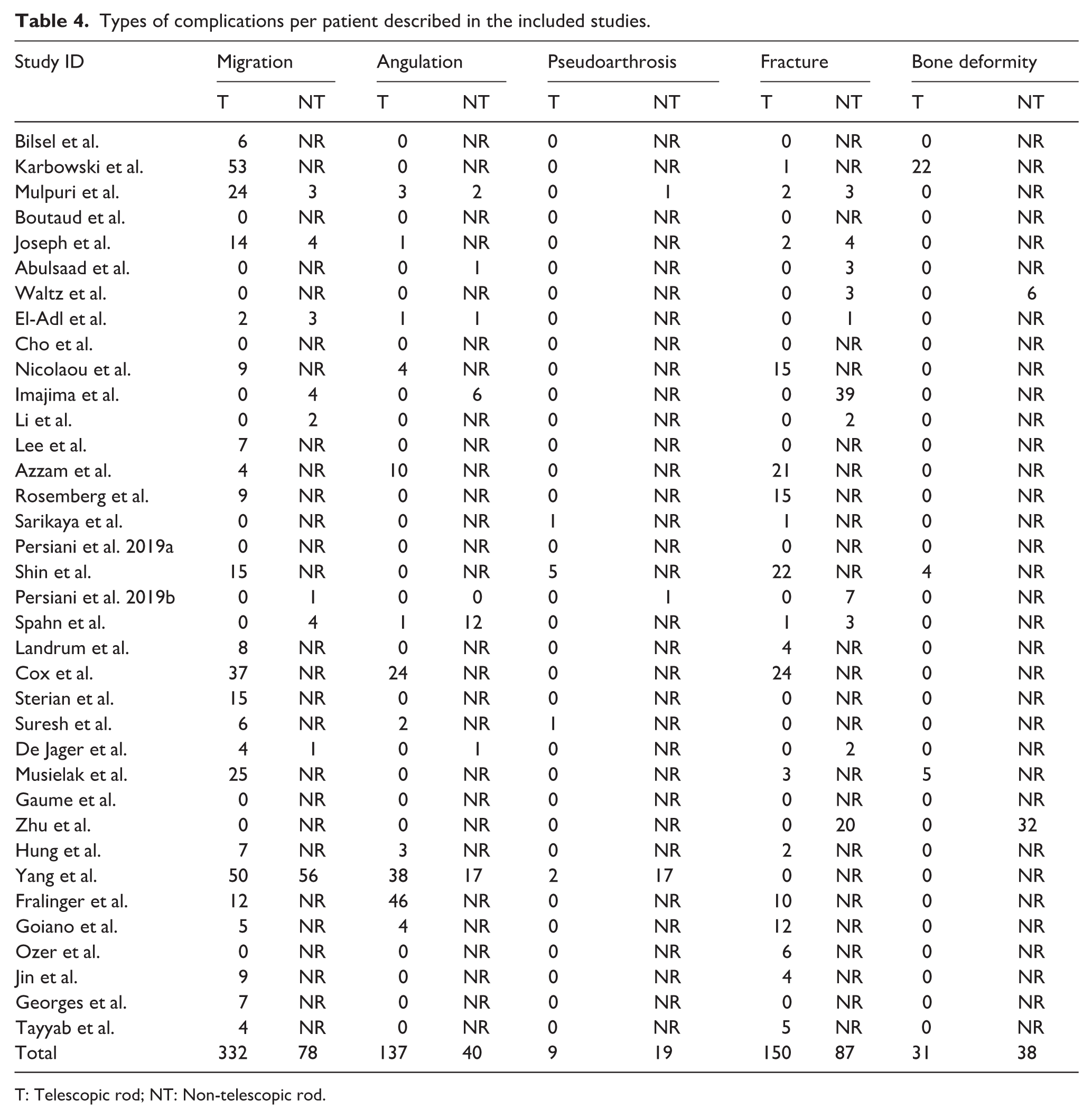
T: Telescopic rod; NT: Non-telescopic rod.
Among patients who required revision, the mean time to reoperation was 3.3 years in the telescopic group and 2.8 years in the non-telescopic group (Table 5).
Time elapsed (in years) between the first surgery and the first revision surgery, with the revision rate (per number of bones) per study, according to the type of rod (T or NT).
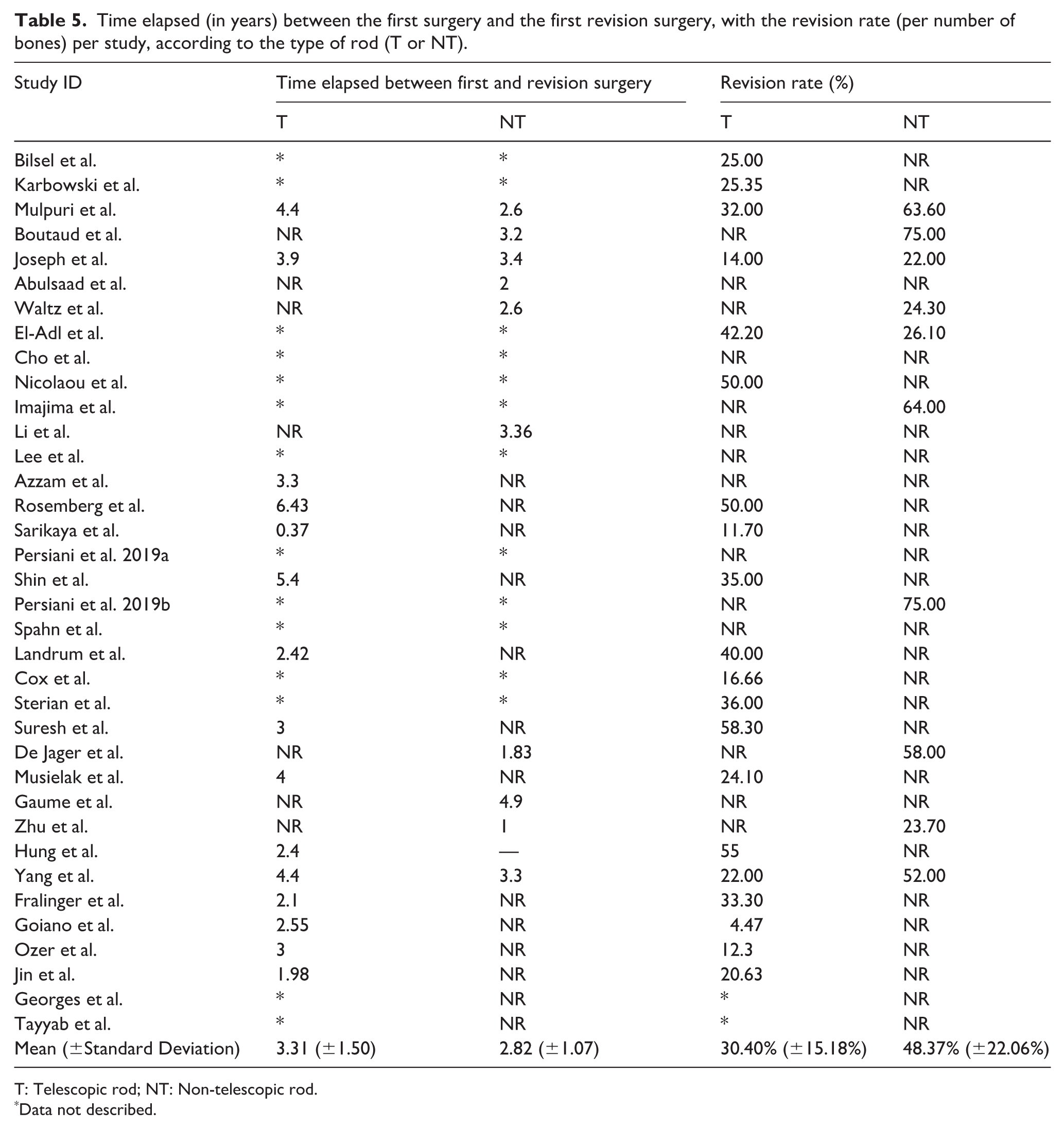
T: Telescopic rod; NT: Non-telescopic rod.
Data not described.
Pooled effects
The pooled effects were calculated using the number of bones operated on as the analytical unit. For the frequency of complications and revisions using telescopic rods, data from 28 of the 36 included studies were used (77.8%), and for non-telescopic rods, data from 13/36 studies (36.1%) were used. Six studies compared the outcomes of both rod types and were included for calculating the pooled Odds Ratio (OR). All meta-analysis models created for this study are shown in Table 6.
Meta-analysis models created to evaluate the frequency of complications and revisions, and the OR for operated bone segments with telescopic and non-telescopic rods, based on studies that assessed outcomes for both rod types.
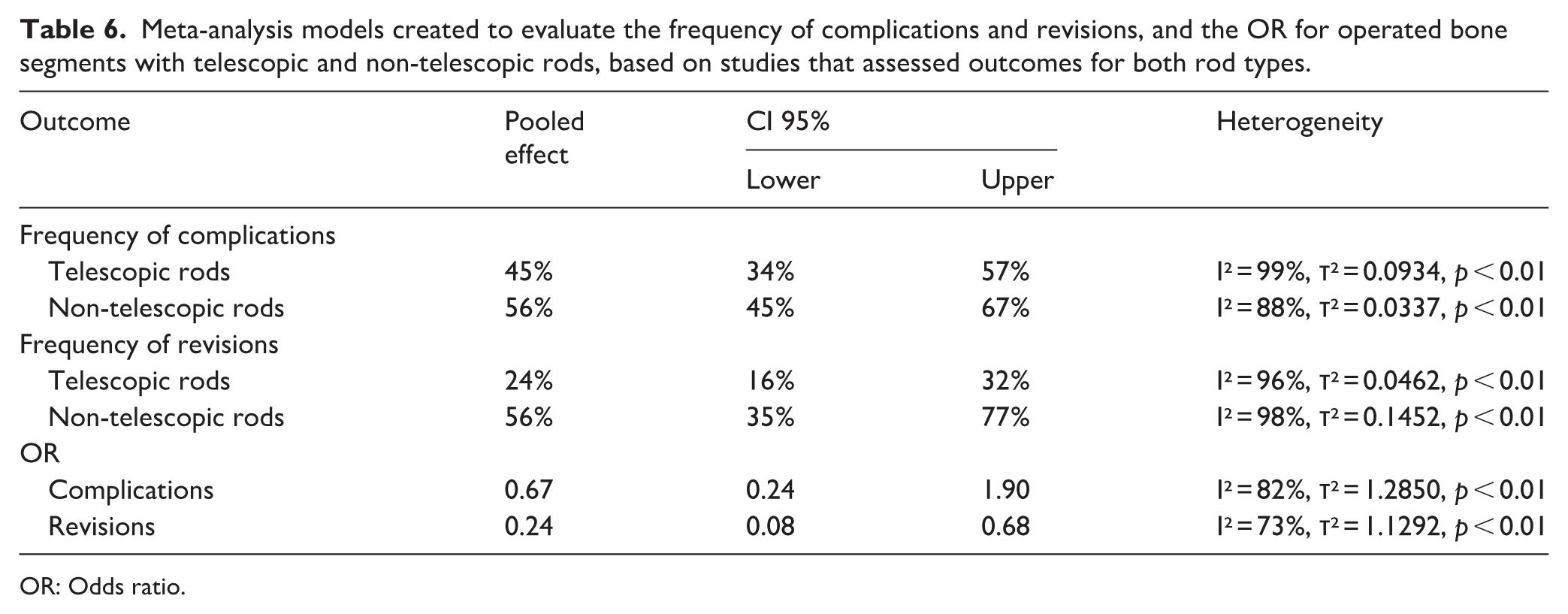
OR: Odds ratio.
When assessing the occurrence of complications (Figure 2), bones operated on using telescopic rods had a complication frequency of 45% (95% CI 34%–57%), while those operated on with non-telescopic rods had a complication frequency of 56% (95% CI 45%–67%) (Figure 3). Both models presented high heterogeneity, demonstrated by the behavior of the data from the included studies (99% and 88%, respectively). As the confidence intervals overlapped, no significant difference was found between the frequencies of complications for both rod types.
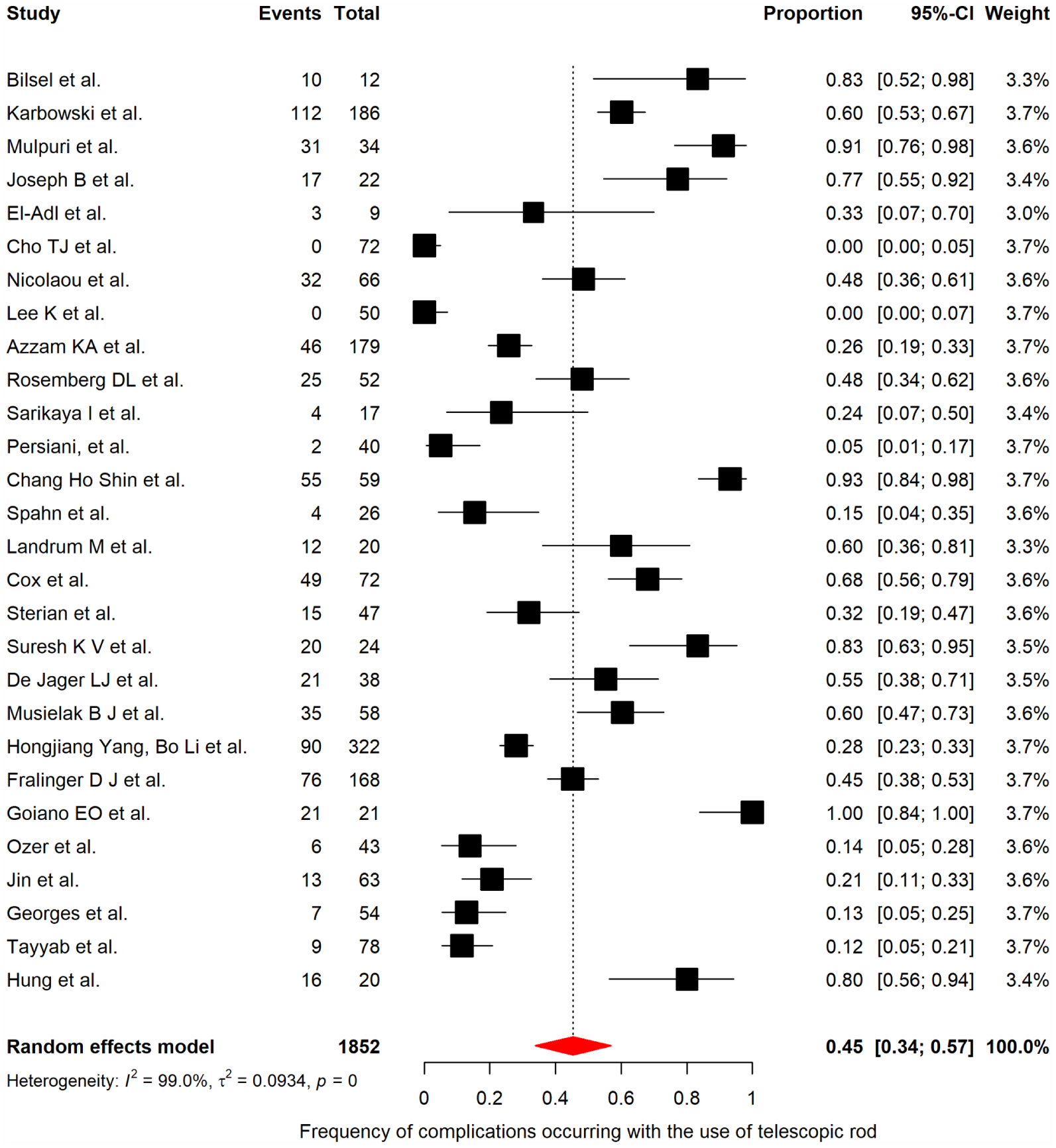
Forest plot showing the pooled effect of the frequency of complications in bones operated on using telescopic rods.
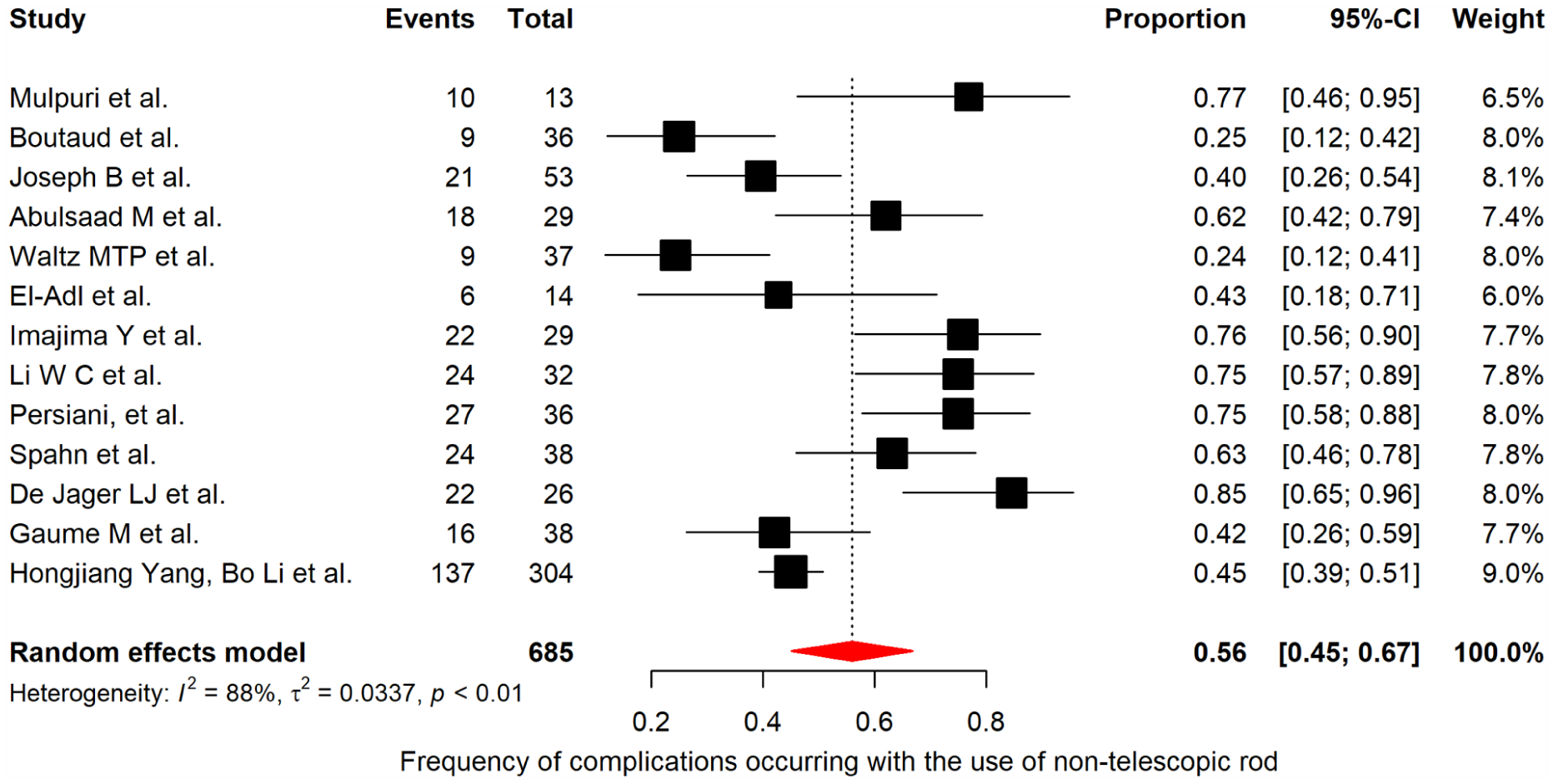
Forest plot showing the pooled effect of the frequency of complications in bones operated on using non-telescopic rods.
When evaluating the complication outcomes in the studies that used both rod types the OR for bones with telescopic rod was found to be 0.67. However, the confidence interval (0.24–1.90) indicates a non-significant difference when compared to the group of non-telescopic rods, as shown in Figure 4.
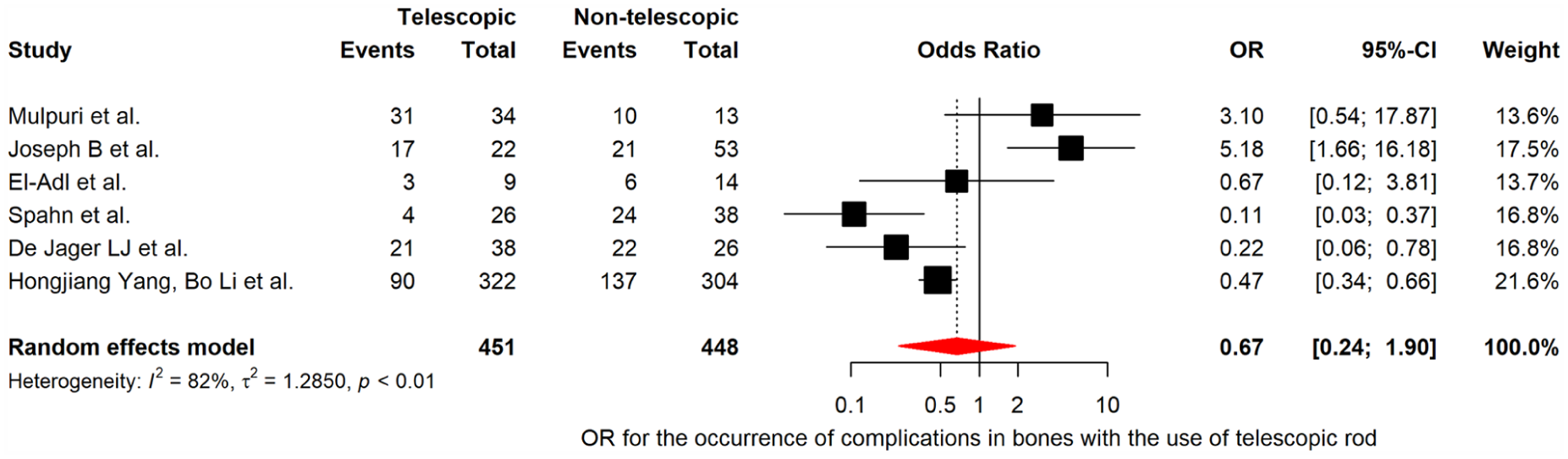
Forest plot showing the pooled OR effect of complications between bones operated on using telescopic and non-telescopic rods.
The frequency of revisions showed a significant difference when telescopic rods were used (24%; 95% CI 16%–32%) (Figure 5) and was significantly lower compared to non-telescopic rods (56%; 95% CI 35%–77%) (Figure 6). Both models showed high heterogeneity (96% and 98%, respectively).
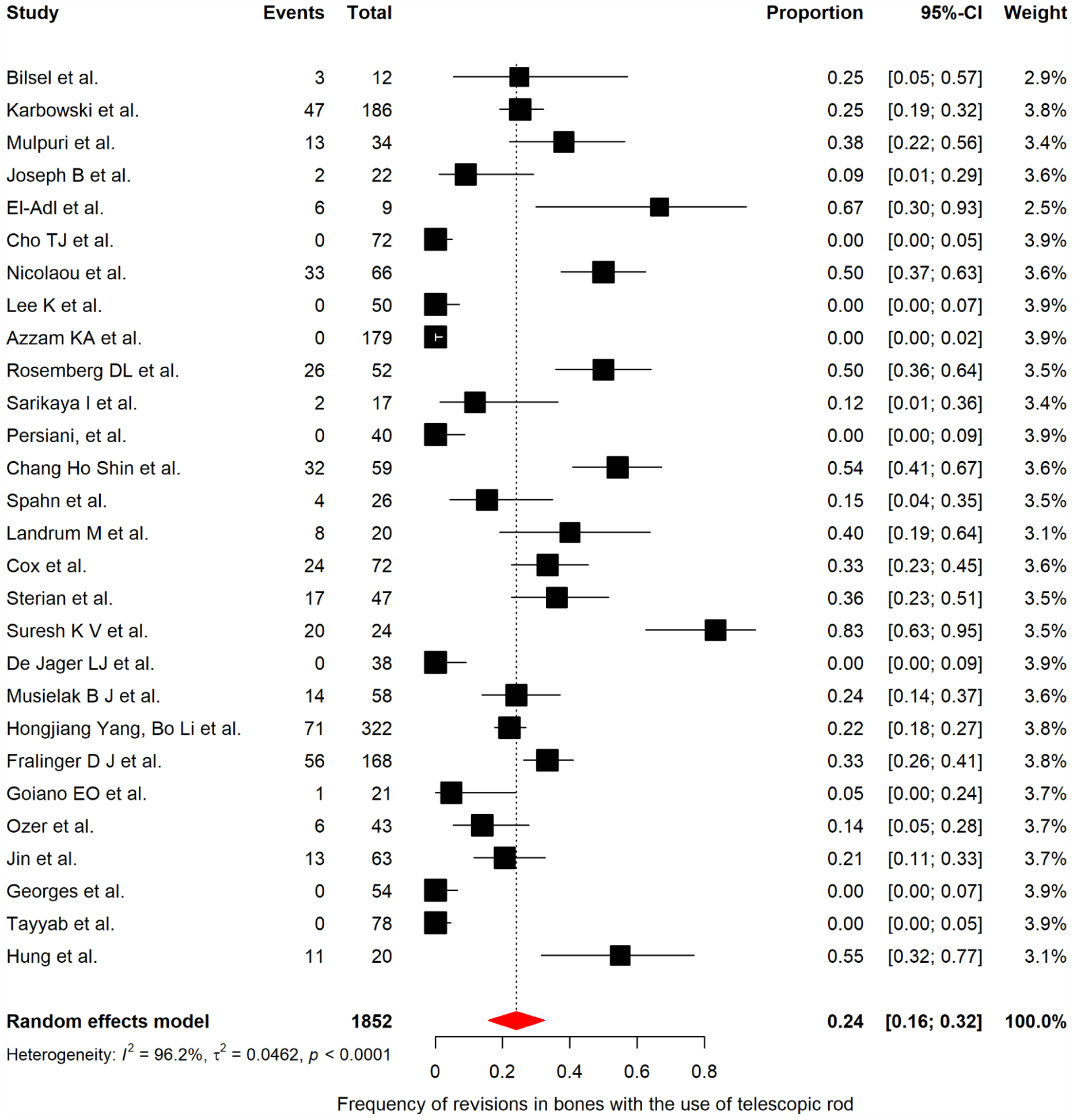
Forest plot showing the pooled effect of revision frequency in bones operated on using telescopic rods.
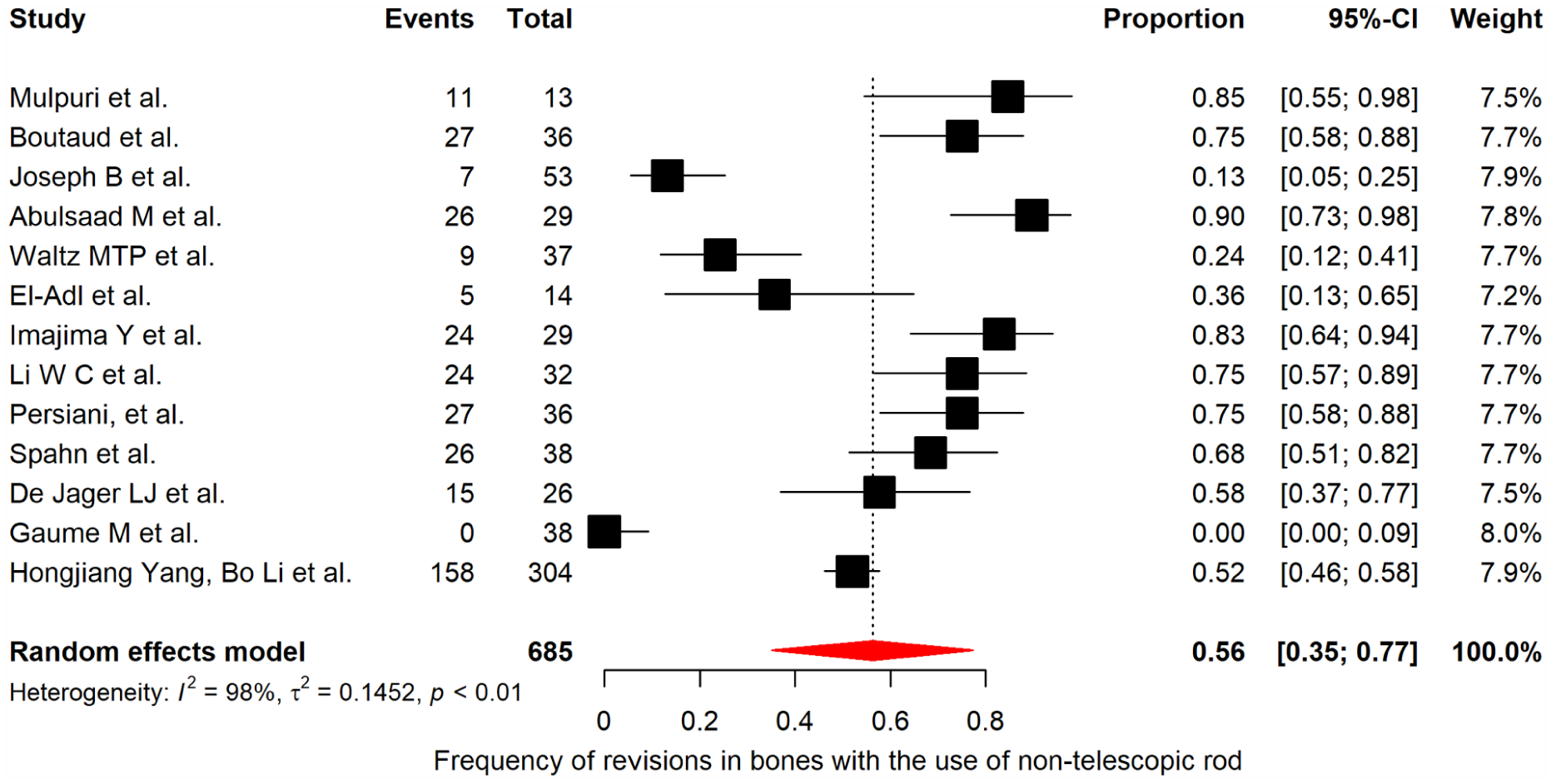
Forest plot showing the pooled effect of revision frequency in bones operated on using non-telescopic rods.
When evaluating the OR for the need for revisions between bones with both types of rods, statistical significance was found, indicating a protective effect for bones treated with telescopic rods compared to those treated with non-telescopic rods (Figure 7). The pooled OR indicated that bones treated with telescopic rods had a 76% relative reduction in the odds of revision compared to non-telescopic rods.
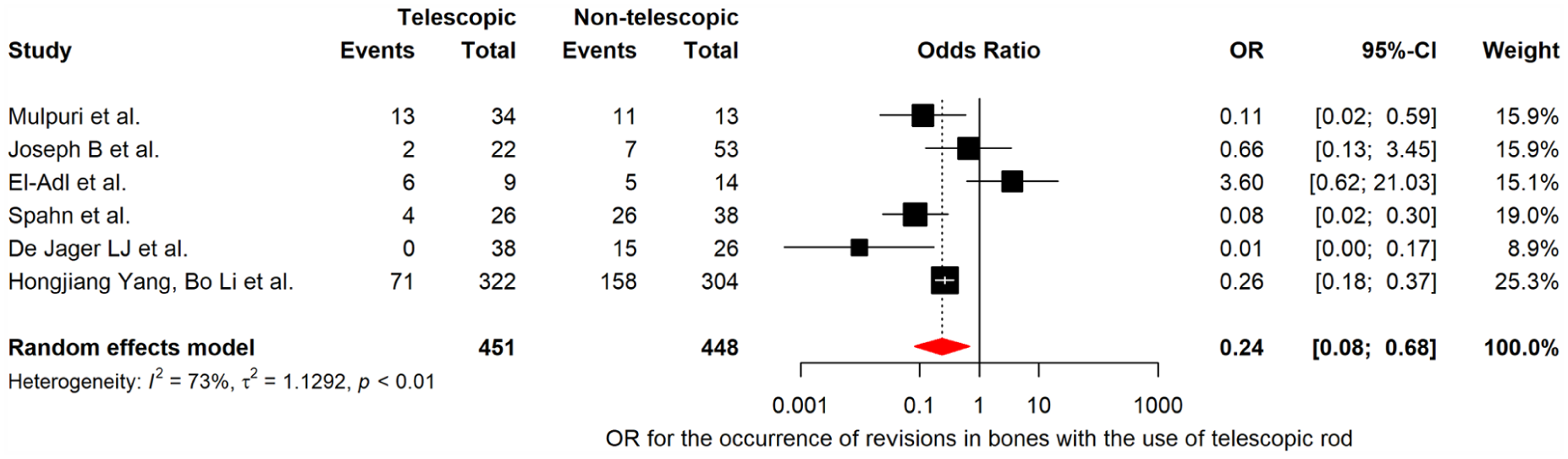
Combined effect of the OR for reoperation between bones operated on using telescopic and non-telescopic rods.
Risk of bias and certainty assessment
For the 33 case series studies evaluated, 16 (48.5%) presented low risk of bias, 14 moderate risk (42.4%) and 3 a high risk of bias (9.1%), as shown in Table 7. For the two case-control studies included, both were classified as low risk of bias, with 80% or more of the criteria achieving positive responses, and the cohort study presented a moderate risk of bias.
Individual assessment of risk of bias using the JBI critical appraisal checklist for case series or case-control studies.
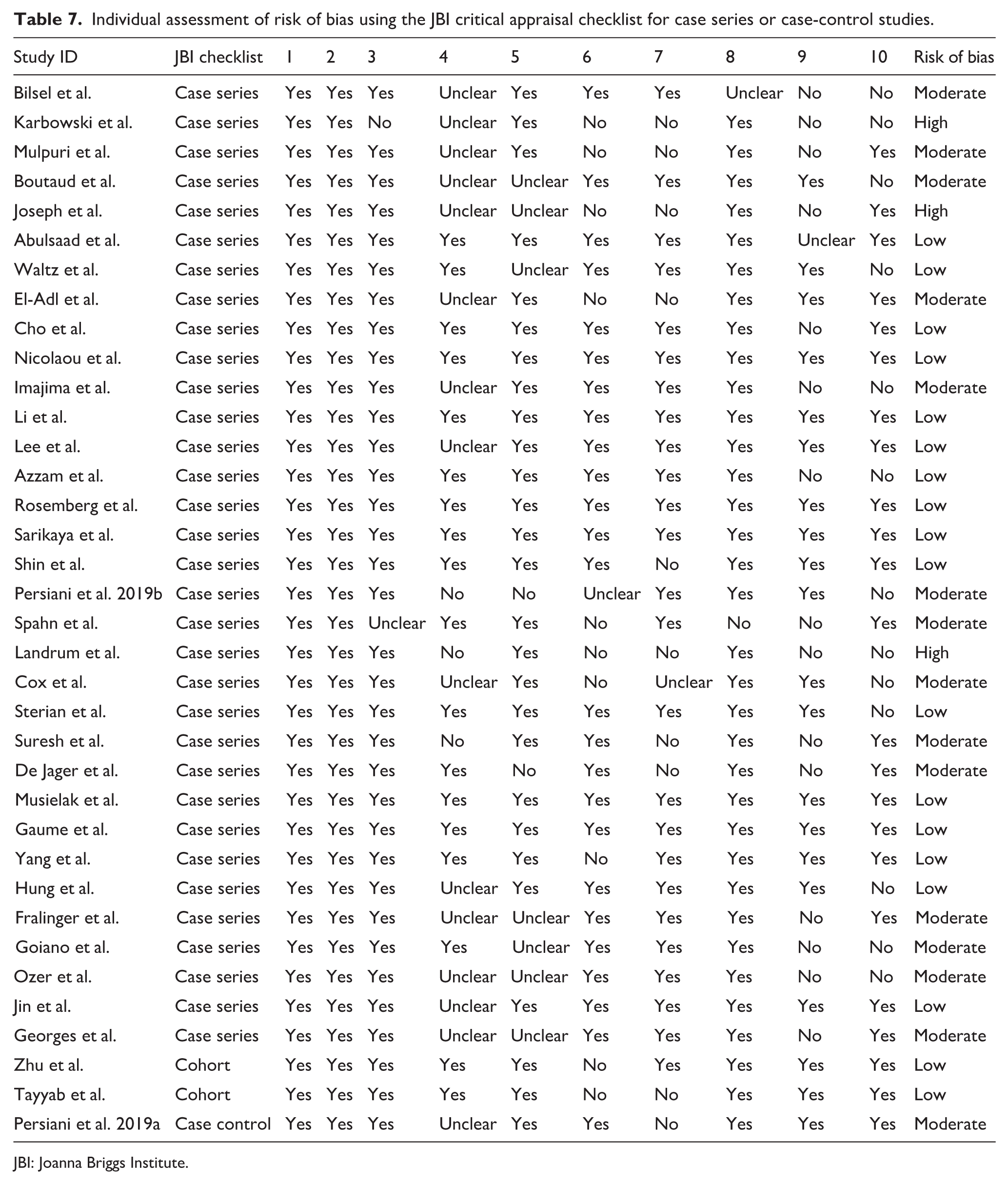
JBI: Joanna Briggs Institute.
A deeper analysis of the individual criteria revealed areas with higher proportions of “unclear” or “no” responses, particularly in item 4 (consecutive inclusion of participants), item 9 (demographics of presenting sites/clinics), and item 10 (statistical analysis). In item 4, nine studies were rated as “unclear,” indicating that many did not explicitly describe whether participants were included consecutively. This lack of clarity reduces the reliability of the sample by introducing potential selection bias. In item 9, 11 studies were rated “no” regarding the demographics of presenting sites or clinics, suggesting that many studies did not provide enough information about the geographic or demographic characteristics of the study settings, which is essential for determining generalizability. In item 10, ten studies were marked as “no,” suggesting that either inappropriate statistical methods were used or the analyses were poorly described, limiting the interpretability and reliability of the findings.
Publication bias was not assessed for the Odds Ratios calculation due to the limited number of studies included (n = 6). Evidence of small-study effects was identified in some pooled analyses, suggesting potential publication bias; therefore, pooled estimates should be interpreted with caution. In contrast, no evidence of publication bias was found for complications with non-telescopic rods (p = 0.261), with a bias estimate of 2.25. The pooled effect models for complications were rated as having low-quality evidence according to GRADE, reflecting the limitations of the included studies.
For the outcome of revisions with telescopic rods, significant evidence of publication bias was identified (p < 0.0001), with a bias estimate of 5.09. Similarly, revisions with non-telescopic rods also showed significant publication bias (p = 0.005), with a bias estimate of 9.44. The pooled effect models for revisions were rated as having low to moderate quality of evidence according to GRADE, reflecting the inherent limitations in study design and reporting.
Discussion
Osteogenesis imperfecta is characterized by bone fragility and progressive deformities that frequently require surgical intervention. Intramedullary fixation remains the cornerstone of orthopedic management; however, the optimal implant strategy continues to be debated. Although intramedullary devices provide additional structural support, high rates of complications and reoperations have been reported in small series.4–9,28 The aim of this study was to compare telescopic and non-telescopic intramedullary devices used in lower limb orthopedic surgeries in patients with OI.
Scollan et al. 4 conducted a meta-analysis of seven studies published between 1986 and 2016, to evaluate surgical complications in pediatric patients with OI who underwent non-telescopic intramedullary fixation. They found rod migration to be the main complication, followed by fractures and bone deformities. Over a mean follow-up of 5.25 years, the average reoperation rate was 40%. Yong et al. 53 reviewed 24 studies published between 1970 and 2020, including 594 patients. Six studies compared telescopic rods with non-telescopic rods, while 18 studies pooled data on telescopic rods only. Despite these previous findings, most available evidence remains limited by small sample sizes and heterogeneity, highlighting the need for updated and more comprehensive analyses. Their findings showed that the rates of complications and reoperations were lower with the use of telescopic rods compared to non-telescopic rods. In addition, the evolution of telescopic rods contributed to reducing these rates. The inclusion of more recent studies further reinforces these findings. Jin et al., 50 analyzing 63 long bones treated with Fassier–Duval rods, reported a revision rate of approximately 20%, with complications mainly related to refracture and implant failure. Similarly, Ozer et al., 49 evaluating 43 lower limb bones treated with telescopic rods, described a lower overall complication rate, with revision events primarily associated with refracture, pseudoarthrosis, and rod migration. Georges et al. 51 reported hardware migration in a subset of femoral procedures using telescopic rods, highlighting that mechanical complications remain relevant even with modern implants. These contemporary data are consistent with the overall trend observed in the present meta-analysis, further supporting the durability and improved survival of telescopic rods compared to non-telescopic devices.
Our study, which now includes 36 studies published between 2000 and 2025, represents 1 of the most comprehensive syntheses to date on intramedullary fixation in osteogenesis imperfecta. The inclusion of more recent studies strengthens the external validity of our findings while maintaining methodological consistency with previous analyses. However, the reporting of variables across studies was heterogeneous and often incomplete.
The evolution of telescopic rod design over the past decades likely contributed to the improved outcomes observed. Earlier systems such as Bailey–Dubow 54 and Sheffield 55 rods were associated with higher rates of mechanical complications, whereas newer designs, particularly the Fassier–Duval rod 56 allow less invasive implantation and improved telescoping mechanics. The predominance of modern telescopic systems in recent studies may partially explain the lower revision rates observed in the current analysis. This technological progression likely explains part of the improved outcomes observed in more recent studies included in this review.
In the selected studies, some reported the number of bones operated on, while others reported the number of patients. Some studies included both. Similar inconsistencies were also reported for gender, Sillence classification and complications. Nonetheless, the data provided valuable insights into the rates of complications and reoperations relative to follow-up duration. The most robust finding of this study is the significantly lower revision rate associated with telescopic rods. The pooled analysis demonstrated a substantial reduction in the need for reoperation, with an estimated 76% relative reduction in odds compared to non-telescopic implants. This finding is clinically meaningful, as revision surgery in patients with OI is associated with increased morbidity, prolonged rehabilitation, and higher healthcare costs. This reinforces the role of telescopic rods as the preferred strategy for long-term skeletal management in growing patients.
Complications represent adverse events occurring during the postoperative recovery period. These include rod-related events such as migration, structural deformity or telescoping failure (in the case of telescoping or sliding stems), as well as patient-related occurrences such as fractures, pseudarthroses and pain. Infection is an event related to surgical procedures.
Rod migration and post-surgical fractures were the most frequently reported complications across studies for both rod types. However, the reporting of complication subtypes was inconsistent, precluding reliable quantitative comparison between groups. Azzam et al., 27 who used 179 FD rods, described structural deformity and pain after initial surgery as complications, with 100% reoperation rates. De Jager et al., 16 using 26 smooth rods and 38 FD rods, and Persiani et al., 30 using 40 FD rods, did not report revisions in their studies. Interestingly, despite the lower revision rates observed with telescopic rods, no significant difference was found in overall complication rates between the two groups. This apparent discrepancy may be explained by the nature of the complications. While telescopic rods are still susceptible to mechanical issues such as migration or failure of telescoping, these events may not always require surgical revision. In contrast, complications associated with non-telescopic rods, particularly progressive deformity or loss of fixation due to growth, more frequently necessitate reoperation. Therefore, the clinical relevance of complications should be interpreted in the context of their impact on reoperation rather than their mere occurrence.
Revisions generally occurred several years after the index procedure, with mean times to revision of 3.3 years for telescopic rods and 2.8 years for non-telescopic rods. Although some studies did not describe the time between initial surgery and revision, others reported follow-up times averaging over 5 years. For example, Azzam et al. 27 reported 3.3 years for tibial surgeries and 4.3 years for femurs surgeries. Rosemberg et al. 28 reported 6.43 years, and Cho et al. 24 described revisions after a mean follow-up of 6.2 years. They showed that most revisions occurred after fractures and bowing of the rod at the internal or external intersection point of the components (male and female). These complications usually occur after growth of the telescopic mechanism, suggesting many fractures could be predicted. This would allow the surgeon to define more accurately time for component replacement, potentially avoiding fracture and rod breakage. Most studies did not specify the exact timing of these fractures or their relationship to rod telescoping. If these fractures could be prevented, migration might become the predominant complication. Careful attention to technical factors, such as rod insertion and fixation, can reduce migration rates. 26
Exploratory observations across studies suggested that younger age and greater surgical burden may be associated with higher complication and revision rates; however, these associations should be interpreted cautiously due to heterogeneity and study design limitations.
The high heterogeneity observed across studies is an important limitation and likely reflects variability in implant design, surgical technique, patient age, severity of disease, and duration of follow-up. Additionally, differences in reporting outcomes, particularly regarding bone-level versus patient-level data, contributed to variability in pooled estimates. Despite this heterogeneity, the direction of effect remained consistent across studies. However, no significant differences were found based on gender or Sillence classification.
Six studies compared both fixation mechanisms, showing that the need for surgical revision was statistically higher for non-telescopic rods compared to telescopic rods. Yang et al. 17 reported revision rates of 22% for telescopic rods and 52% for non-telescopic rods, with a follow-up of over 5 years.
This study has several important limitations. Most included studies were retrospective case series, with inherent risk of bias and limited control for confounding factors. Reporting heterogeneity was substantial, particularly regarding anatomical distribution, complication definitions, and Sillence classification. Additionally, some studies reported outcomes per patient rather than per treated bone, precluding their inclusion in the quantitative synthesis. The predominance of bone-level analysis may also limit direct comparison with studies reporting patient-level outcomes. Evidence of publication bias was also identified in revision outcomes, suggesting that pooled estimates should be interpreted with caution.
Conclusion
Telescopic rods are associated with significantly lower revision rates and improved implant survival compared with non-telescopic rods in children with osteogenesis imperfecta. Although overall complication rates remain similar between groups, telescopic devices appear to reduce the need for reoperation, representing a clinically relevant advantage in the long-term management of these patients.
These findings support the preferential use of telescopic rods in growing children with OI. However, given the heterogeneity and predominantly retrospective nature of the available evidence, further prospective and comparative studies are needed to better define optimal surgical strategies and long-term outcomes.
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261461890 – Supplemental material for Telescopic rods vs. non-telescopic rods in the treatment of osteogenesis imperfecta: A systematic review
Supplemental material, sj-pdf-1-cho-10.1177_18632521261461890 for Telescopic rods vs. non-telescopic rods in the treatment of osteogenesis imperfecta: A systematic review by Rafael Yoshida, Matheus Pimentel Sombra, Michelle de Oliveira Cardoso and Mônica Paschoal Nogueira in Journal of Children's Orthopaedics
Footnotes
Author contributions
R.Y.: Conceptualization, Data collection, Manuscript drafting, Methodology.
M.P.S.: Data collection, Literature review, Manuscript revision.
M.O.C.: Data analysis, Manuscript revision.
M.P.N.: Critical revision, Final approval, Supervision.
All authors approved the final version of the manuscript.
Data availability
All data supporting the findings of this study are available within the article and its supplementary materials.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Not applicable. This study is a systematic review of previously published studies.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.