
Abstract
Purpose:
To evaluate clinical and fracture-related factors associated with failed closed reduction in high-risk pediatric supracondylar humerus fractures (SCHF), with emphasis on fracture morphology and intraoperative multidirectional instability.
Methods:
This retrospective cohort study included 318 consecutive children aged 2–12 years who underwent surgery for Gartland type III SCHF or intraoperatively confirmed Gartland type IV instability between 2015 and 2025. Fractures were classified as typical extension-type, medial oblique, lateral oblique, or flexion-type. Univariable and multivariable logistic regression analyses were performed.
Results:
Closed reduction was successful in 192 patients, whereas 126 required conversion to open reduction. Flexion-type fractures had the highest open reduction rate (80.0%; p < 0.001). In the full multivariable model, Gartland type IV instability was strongly associated with open reduction (odds ratio 5.21, 95% confidence interval 2.69 to 10.53; p < 0.001). Compared with flexion-type fractures, typical, medial oblique, and lateral oblique patterns had significantly lower adjusted odds. Older age and longer time from injury to surgery were also associated with open reduction.
Conclusions:
Flexion-type morphology and intraoperatively confirmed Gartland type IV instability were strongly associated with failed closed reduction. These findings may help surgeons anticipate reduction difficulty and plan operative resources in high-risk pediatric SCHF.
Significance of Study:
Recognizing fracture morphology and intraoperative multidirectional instability may help surgeons anticipate failed closed reduction in high-risk pediatric SCHF.
Level of evidence:
III
Keywords
Introduction
Supracondylar humerus fractures (SCHF) are the most common elbow fractures in children. In displaced injuries, operative treatment is frequently required, and closed reduction with percutaneous pinning remains the standard approach. However, the difficulty of closed reduction varies substantially according to fracture stability and morphology. Gartland type III fractures are completely displaced injuries, whereas Gartland type IV injuries represent a more unstable pattern characterized by multidirectional instability due to loss of both anterior and posterior periosteal support. Because type IV instability is usually confirmed intraoperatively under fluoroscopy rather than reliably identified on preoperative radiographs, it may only become evident during attempted closed reduction. When acceptable alignment or stability cannot be achieved or maintained by closed means, conversion to open reduction becomes necessary. This intraoperative failure of closed reduction represents an important clinical problem because it may reflect greater fracture complexity and may alter operative planning and surgical exposure.1 –4
Identifying predictors of failed closed reduction before surgery is clinically important because it may improve preoperative counseling and help surgeons anticipate procedural difficulty. Recent literature suggests that the likelihood of conversion to open reduction is influenced by multiple preoperative factors, including fracture morphology, neurological deficits, obesity, and selected radiographic characteristics.5 –9 Among these variables, flexion-type fractures have been reported as one of the strongest predictors of failed closed reduction and conversion to open reduction, with markedly higher odds than extension-type injuries in recent cohort studies.10 -12 This association is biologically plausible, as flexion-type injuries are thought to be associated with anterior soft-tissue interposition and loss of a stabilizing posterior periosteal hinge, thereby making closed reduction more difficult to achieve and maintain.8 –10
The effect of surgical delay on reduction success remains controversial. Although delayed fixation may theoretically increase swelling and make closed reduction more difficult, prior studies have not consistently shown a higher rate of open reduction or perioperative complications when treatment is deferred beyond the first 12–24 h. In particular, Gupta et al. 13 found no significant increase in open reduction or complications with treatment after 12 h, and Bales et al. 14 similarly reported no increase in open reduction or adverse outcomes with delayed pinning in most patients. This inconsistency likely reflects differences in case mix, fracture severity, and study design, and it also highlights a broader limitation in the existing literature: although multiple candidate predictors have been described, relatively few studies have evaluated them simultaneously within a multivariable predictive framework.5,7 –9,11
Therefore, the aim of this study was to evaluate clinical and fracture-related factors associated with failed closed reduction in a consecutive high-risk cohort of surgically treated Gartland type III SCHF and intraoperatively confirmed Gartland type IV instability. Particular emphasis was placed on fracture morphology and multidirectional instability, because these factors may influence the ability to achieve and maintain closed reduction. By evaluating these variables together with patient-related and treatment-related factors, this study sought to refine risk stratification for conversion to open reduction. We hypothesized that flexion-type morphology and intraoperative type IV instability would be associated with a higher likelihood of conversion to open reduction.
Methods
Study design and patient selection
This retrospective cohort study included consecutive pediatric patients who underwent surgical treatment for SCHF between January 2015 and December 2025 at a single tertiary referral center. Ethical approval was obtained from the institutional review board and all procedures were conducted in accordance with the Declaration of Helsinki.
Patients were eligible for inclusion if they met the following criteria: (1) age between 2 and 12 years, consistent with the commonly affected pediatric population reported in the literature; (2) diagnosis of displaced SCHF, including extension-type Gartland type III injuries, displaced flexion-type injuries, and fractures with type IV instability confirmed intraoperatively; (3) initial management with an attempt at closed reduction and percutaneous pinning under general anesthesia; and (4) availability of complete clinical and radiographic data, including preoperative imaging and intraoperative records.
Patients were excluded if they had open fractures, pathological fractures, previous surgery involving the affected elbow, associated ipsilateral upper extremity fractures that could affect reduction strategy, or incomplete data. In addition, patients in whom closed reduction was not attempted were excluded to ensure a homogeneous cohort for evaluating factors associated with conversion to open reduction.
The age range of 2–12 years was selected to capture the typical pediatric population in which SCHF most commonly occur, while excluding very young children with atypical injury mechanisms and older adolescents with fracture patterns approaching adult morphology.1,2 This approach was intended to improve cohort homogeneity and reduce age-related confounding.
Fracture classification
Fractures were initially evaluated using the best available preoperative anteroposterior and lateral elbow radiographs and classified according to the modified Gartland classification system. Because true orthogonal radiographs may be difficult to obtain in displaced pediatric SCHF due to pain, swelling, and fracture displacement, classification was based on the most diagnostic available views. All fractures were initially managed as displaced unstable SCHF, as type IV instability can only be confirmed intraoperatively.
Gartland type IV fractures were defined intraoperatively based on fluoroscopic assessment under general anesthesia. Fractures demonstrating multidirectional instability, including flexion-extension and rotational instability during fluoroscopic manipulation under anesthesia, were classified as Gartland type IV.
In addition to Gartland classification, fractures were categorized using predefined radiographic morphology categories—typical extension-type, medial oblique, lateral oblique, and flexion-type—based on preoperative radiographic fracture patterns. Representative preoperative radiographic examples of each morphology category are provided in Figure 1.
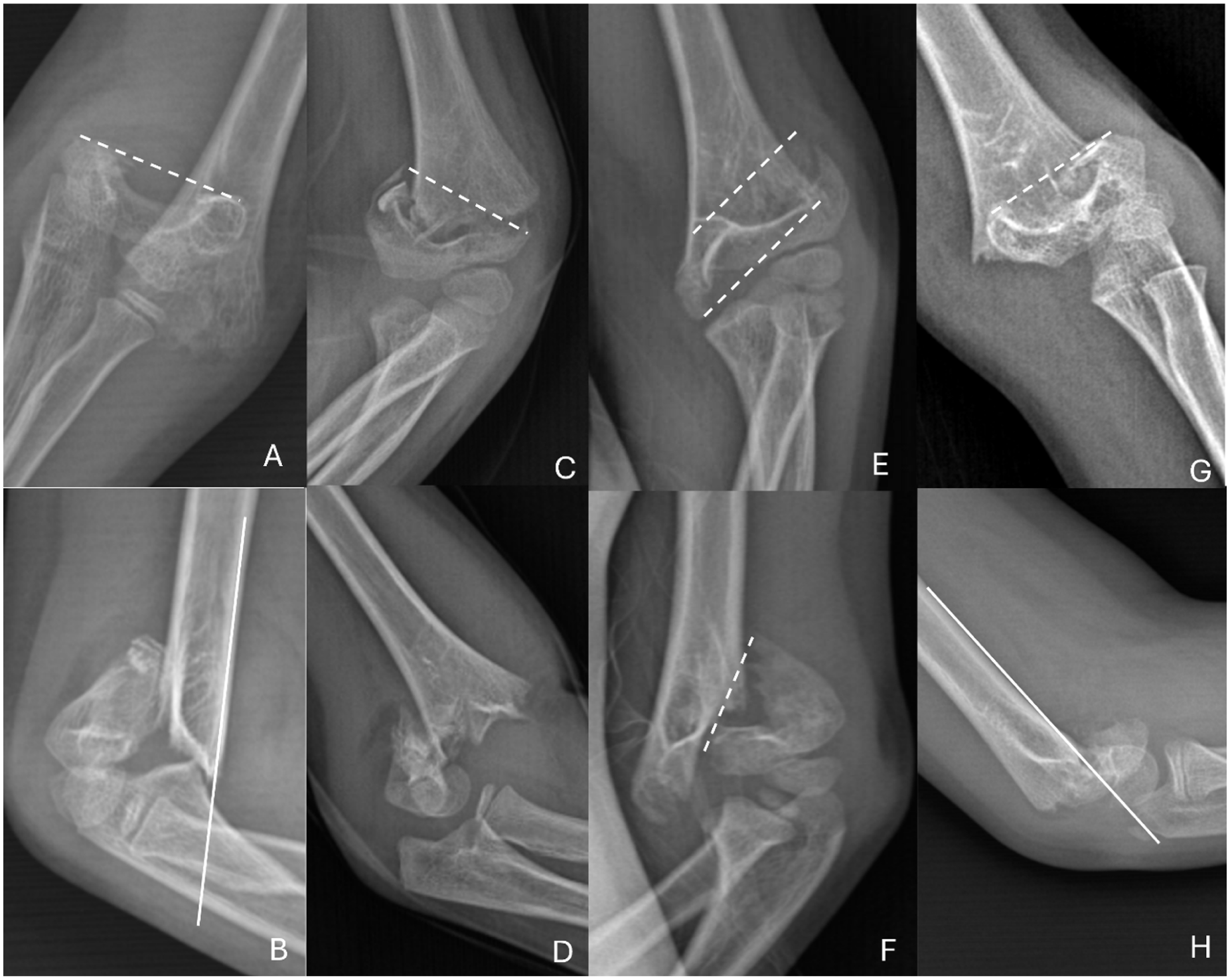
Representative preoperative radiographic examples of fracture morphology in pediatric supracondylar humerus fractures.
Surgical protocol
All patients were treated under general anesthesia with fluoroscopic guidance following a standardized surgical protocol. Surgical procedures were performed by 1 of 3 senior orthopedic trauma surgeons, each with a minimum of 15 years of independent trauma surgery experience, at a tertiary referral center where pediatric elbow trauma, including SCHF, is routinely managed by the same trauma team. An initial attempt at closed reduction was performed in all cases using gentle longitudinal traction, correction of medial/lateral displacement, and flexion-based reduction maneuvers appropriate for fracture alignment.
Following reduction, stability was assessed under fluoroscopy. During this assessment, fractures demonstrating persistent multidirectional instability, including flexion-extension and rotational instability, were identified as Gartland type IV injuries. Multidirectional instability alone was not considered an indication for open reduction if acceptable alignment could be obtained and maintained with percutaneous fixation. Conversion to open reduction was performed when acceptable closed reduction could not be achieved or maintained despite repeated closed maneuvers. This included persistent sagittal malalignment, unacceptable coronal alignment, failure of the anterior humeral line to appropriately intersect the capitellum on the lateral view, clinically relevant rotational malalignment, or inability to maintain reduction safely during pin insertion under fluoroscopy. Open reduction was therefore defined as failure of closed reduction requiring surgical exposure to achieve satisfactory alignment.
Outcome definition
The primary outcome of the study was conversion to open reduction, defined as the inability to achieve or maintain acceptable fracture alignment using closed reduction techniques, necessitating surgical exposure. The decision to convert was made intraoperatively by the treating surgeon when closed maneuvers failed to restore or maintain acceptable sagittal, coronal, or rotational alignment under fluoroscopy. Thus, conversion to open reduction reflected failed closed reduction rather than the presence of instability alone.
Variables assessed
Demographic, clinical, and fracture-related variables were evaluated for their association with conversion to open reduction. These included patient age, sex, dominance, side of injury, time from injury to surgery (hours), fracture morphology subtype, presence of preoperative nerve injury, and intraoperatively confirmed Gartland type IV instability. All variables were defined a priori based on their potential clinical relevance and previously reported associations in the literature.
Statistical analysis
All statistical analyses were performed using SPSS software (version 28.0; IBM Corp., Armonk, NY, USA). Continuous variables were assessed for normality using the Shapiro–Wilk test. Normally distributed variables were compared using the independent samples t-test, whereas nonnormally distributed variables were analyzed using the Mann–Whitney U test. Categorical variables were compared using the chi-square test or Fisher’s exact test as appropriate.
Univariable analyses were initially performed to evaluate the association between each variable and conversion to open reduction. The linearity assumption between continuous variables and the logit of the outcome was assessed prior to inclusion in the logistic regression models. Subsequently, a multivariable binary logistic regression model was constructed to identify independent factors associated with conversion to open reduction. Variable selection was based on clinical relevance and avoidance of multicollinearity rather than solely on univariable statistical significance. Multicollinearity was assessed using variance inflation factors (VIF). Potential collinearity between fracture classification variables was assessed and considered acceptable based on VIF values.
Because time from injury to surgery showed a right-skewed distribution, this variable was additionally evaluated in sensitivity analyses using clinically relevant categories (≤6 h, 6–12 h, and >12 h). Nonlinearity between time to surgery and the logit of the outcome was assessed using spline-based modeling. Categorical sensitivity models included the same core covariates as the primary regression analysis, with preoperative nerve injury coded as a binary variable.
Adjusted odds ratios (ORs) with 95% confidence intervals (CIs) were reported. Model performance was evaluated using the area under the receiver operating characteristic curve. A p-value less than 0.05 was considered statistically significant.
Results
A total of 318 pediatric patients met the inclusion criteria for this study. Closed reduction was successful in 192 cases, whereas 126 patients required conversion to open reduction. Baseline characteristics are summarized in Table 1. Patients who required open reduction were older than those managed with closed reduction (7.33 ± 2.71 vs. 6.09 ± 2.36 years) and had a longer interval from injury to surgery. Because this variable showed a right-skewed distribution, it is interpreted cautiously despite a higher mean value in the open reduction group (15.10 ± 25.56 vs. 5.41 ± 3.38 h). Gartland type IV instability was also more frequent in the open reduction group (52.4% vs. 34.4%), as was preoperative nerve injury (19.0% vs. 6.2%).
Baseline demographic, clinical, and fracture-related characteristics according to reduction method.
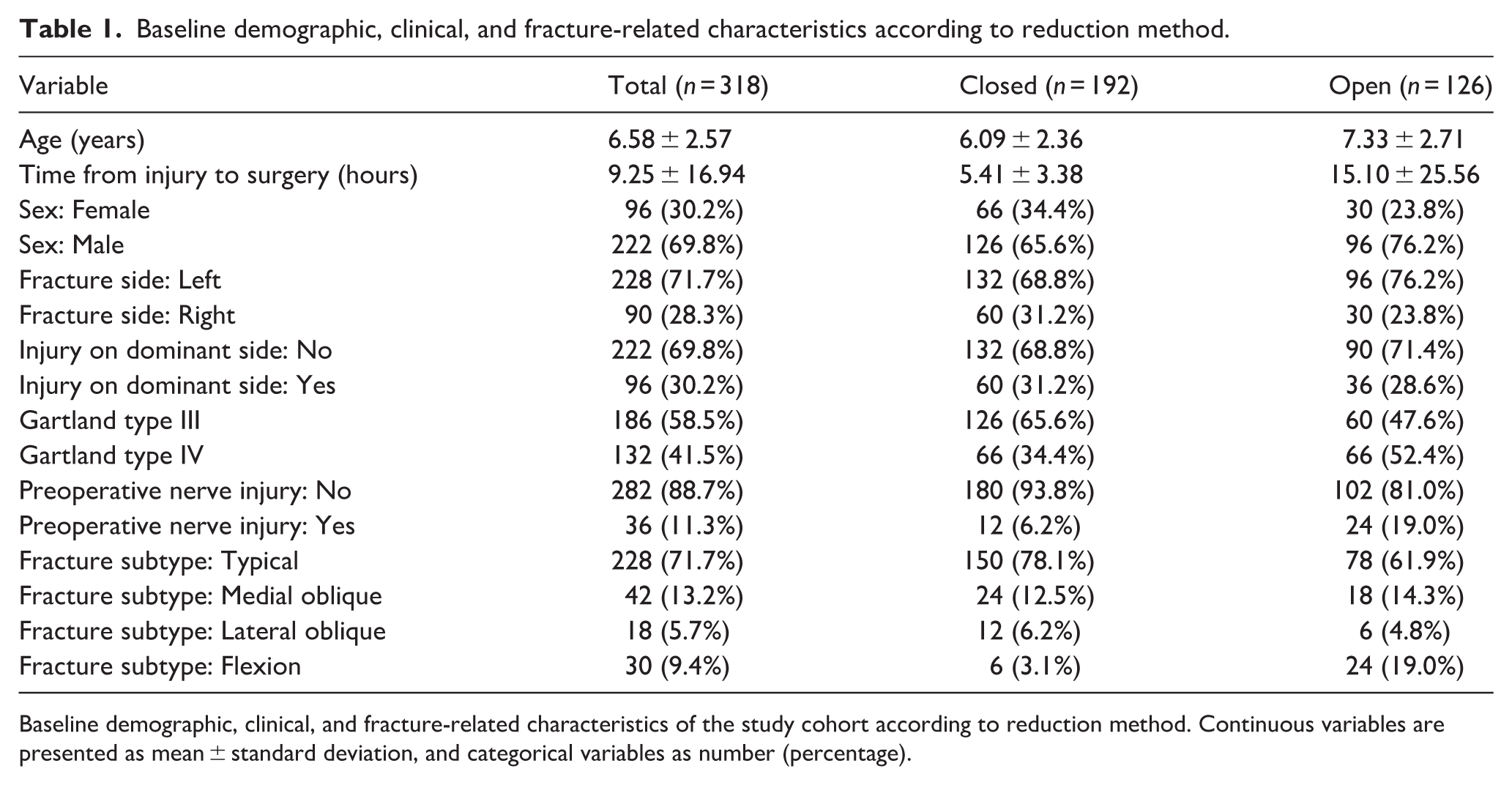
Baseline demographic, clinical, and fracture-related characteristics of the study cohort according to reduction method. Continuous variables are presented as mean ± standard deviation, and categorical variables as number (percentage).
Univariable analyses are presented in Table 2. Older age was associated with a higher likelihood of conversion to open reduction (mean difference 1.24 years, 95% CI 0.66 to 1.82; p < 0.001), as was longer time from injury to surgery (mean difference 9.69 h, 95% CI 5.16 to 14.22; p < 0.001). Gartland type IV instability was significantly associated with open reduction (OR 2.09, 95% CI 1.29 to 3.41; p = 0.002), and preoperative nerve injury showed an even stronger univariable association (OR 4.66, 95% CI 2.20 to 10.48; p < 0.001). Neither injury on the dominant side nor fracture laterality was significantly associated with conversion to open reduction. Male sex was not significantly associated with conversion to open reduction.
Univariable comparison of factors associated with conversion to open reduction.
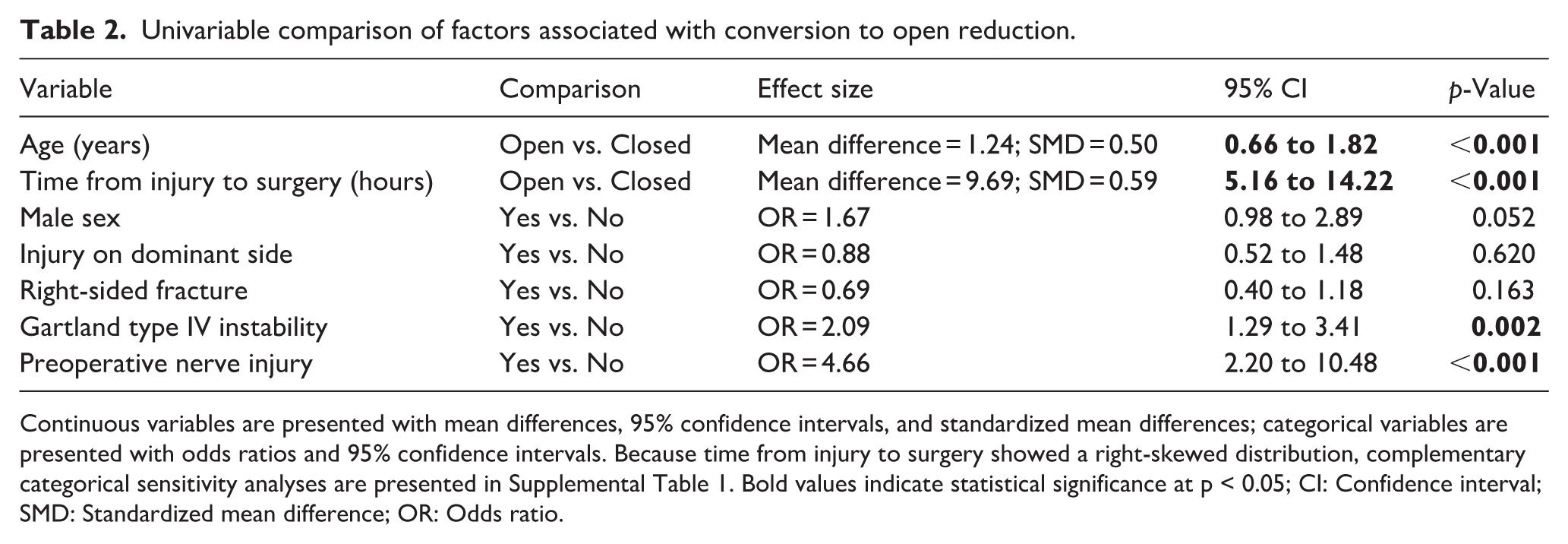
Continuous variables are presented with mean differences, 95% confidence intervals, and standardized mean differences; categorical variables are presented with odds ratios and 95% confidence intervals. Because time from injury to surgery showed a right-skewed distribution, complementary categorical sensitivity analyses are presented in Supplemental Table 1. Bold values indicate statistical significance at p < 0.05; CI: Confidence interval; SMD: Standardized mean difference; OR: Odds ratio.
Fracture morphology differed significantly according to reduction method (Table 3). Flexion-type fractures had the highest open reduction rate at 80.0%, compared with 34.2% for typical fractures, 42.9% for medial oblique fractures, and 33.3% for lateral oblique fractures (overall p < 0.001; Figure 2).
Distribution of open and closed reduction according to fracture subtype.
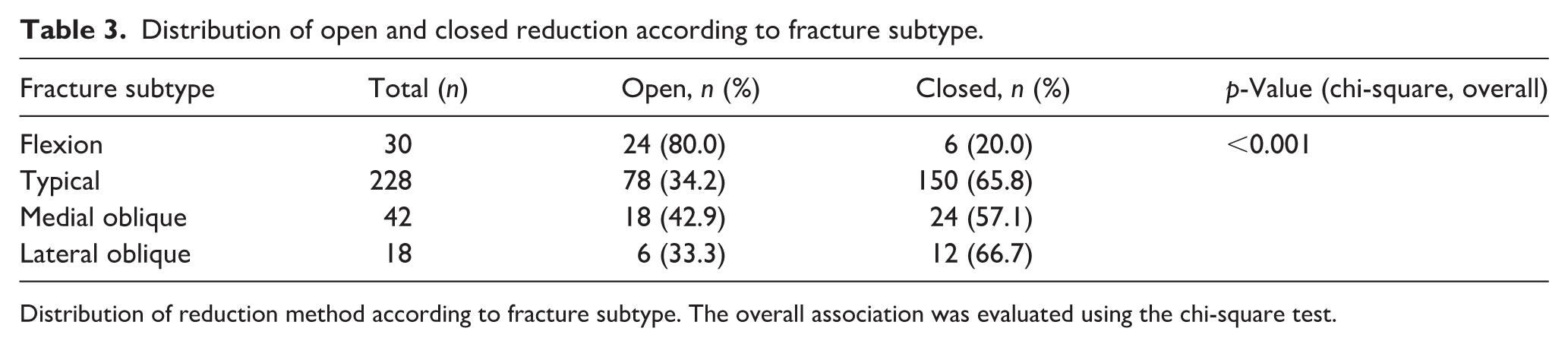
Distribution of reduction method according to fracture subtype. The overall association was evaluated using the chi-square test.
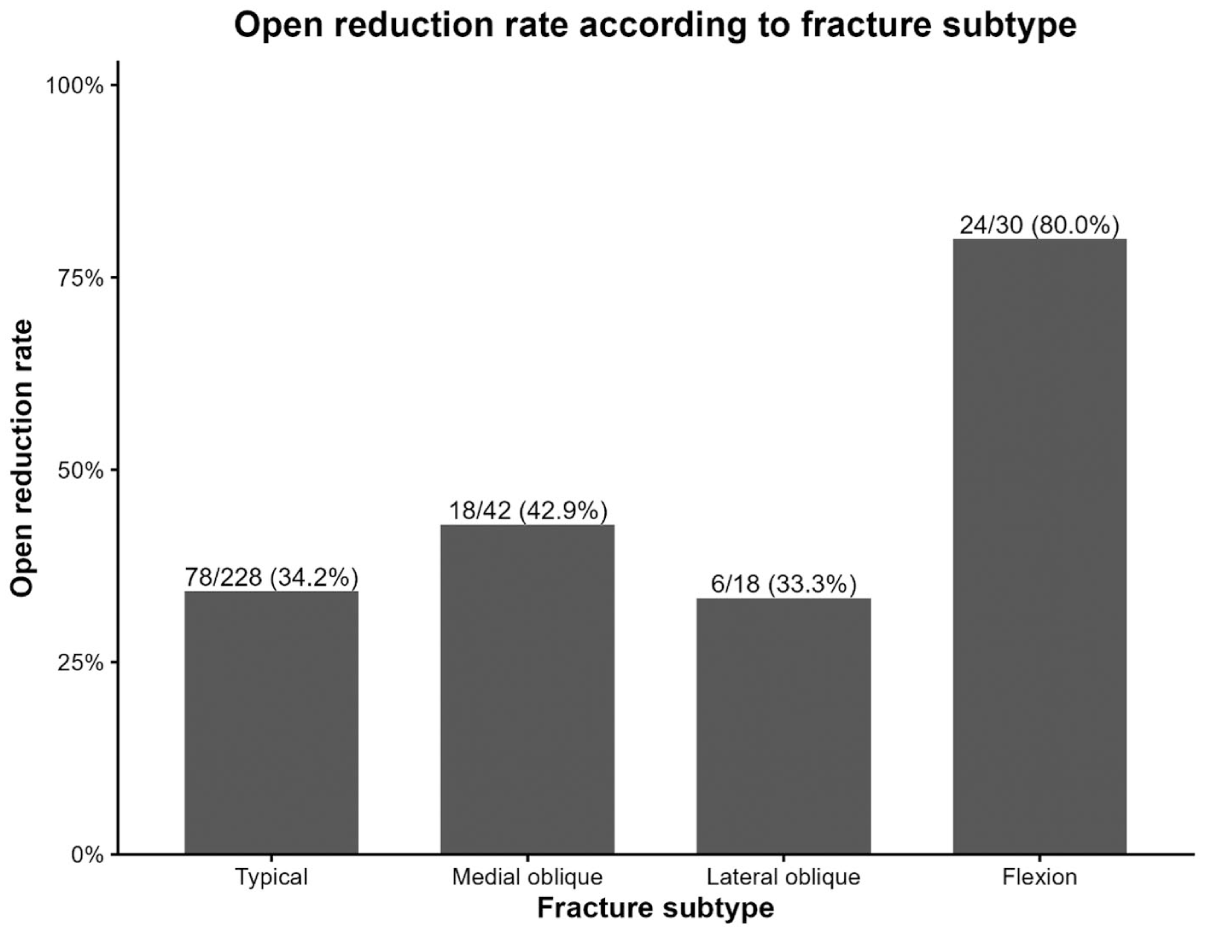
Open reduction rates according to fracture morphology subtype.
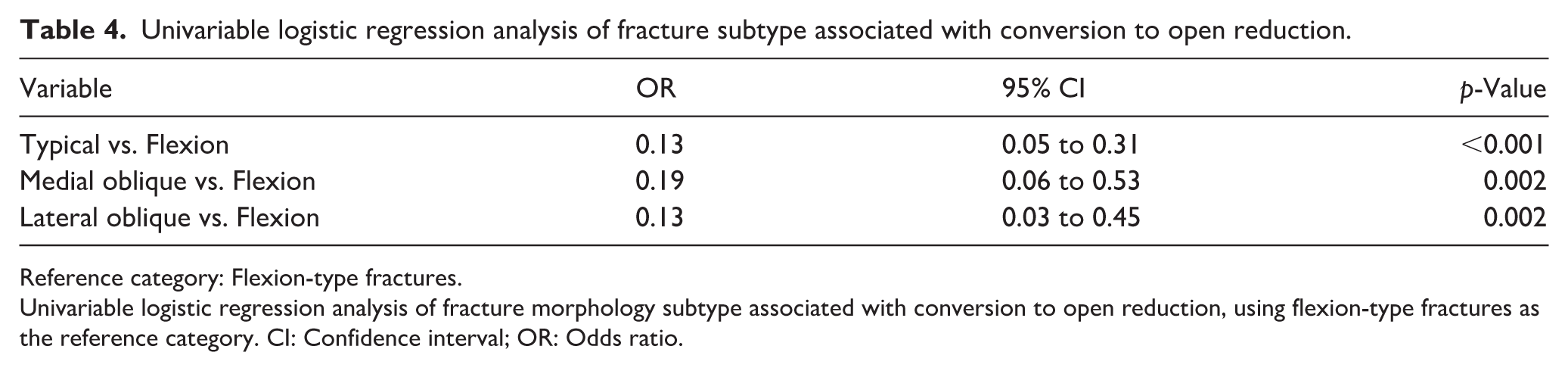
In univariable logistic regression using flexion-type fractures as the reference category (Table 4), all other fracture subtypes had significantly lower odds of open reduction. The odds ratios were 0.13 (95% CI 0.05 to 0.31; p < 0.001) for typical fractures, 0.19 (95% CI 0.06 to 0.53; p = 0.002) for medial oblique fractures, and 0.13 (95% CI 0.03 to 0.45; p = 0.002) for lateral oblique fractures.
Univariable logistic regression analysis of fracture subtype associated with conversion to open reduction.
Reference category: Flexion-type fractures.
Univariable logistic regression analysis of fracture morphology subtype associated with conversion to open reduction, using flexion-type fractures as the reference category. CI: Confidence interval; OR: Odds ratio.
The base multivariable logistic regression model is shown in Table 5. After adjustment, older age (OR 1.33, 95% CI 1.18 to 1.52; p < 0.001), longer time from injury to surgery (OR 1.26, 95% CI 1.17 to 1.36; p < 0.001), and Gartland type IV instability (OR 4.01, 95% CI 2.21 to 7.50; p < 0.001) remained independently associated with conversion to open reduction. Preoperative nerve injury was no longer independently significant (OR 1.87, 95% CI 0.84 to 4.32; p = 0.132). This model demonstrated good discrimination (Area under the curve (AUC) 0.799), low collinearity (maximum VIF 1.492), and a favorable events-per-variable ratio of 31.5.
Base multivariable binary logistic regression model evaluating independent factors associated with conversion to open reduction.
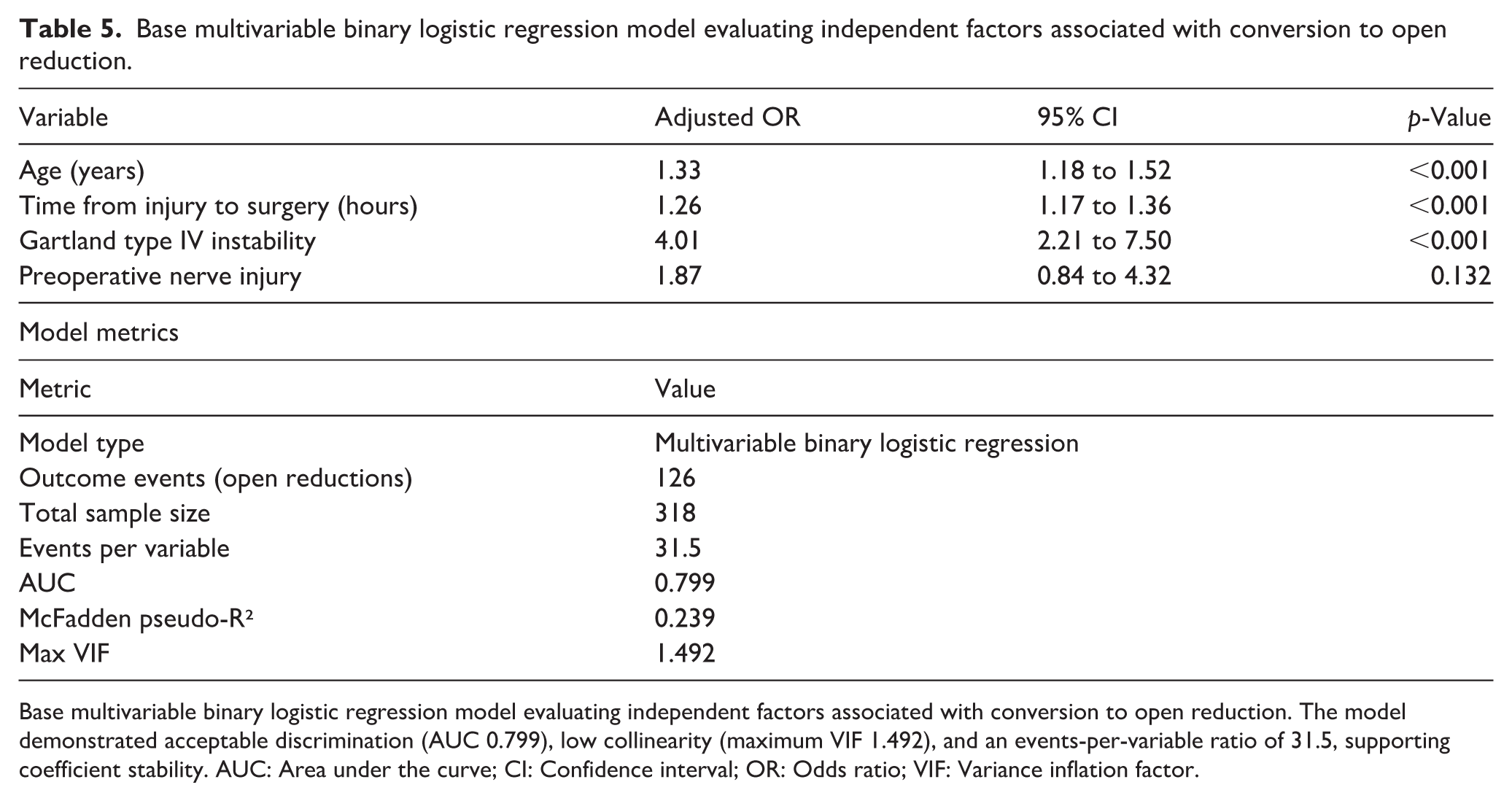
Base multivariable binary logistic regression model evaluating independent factors associated with conversion to open reduction. The model demonstrated acceptable discrimination (AUC 0.799), low collinearity (maximum VIF 1.492), and an events-per-variable ratio of 31.5, supporting coefficient stability. AUC: Area under the curve; CI: Confidence interval; OR: Odds ratio; VIF: Variance inflation factor.
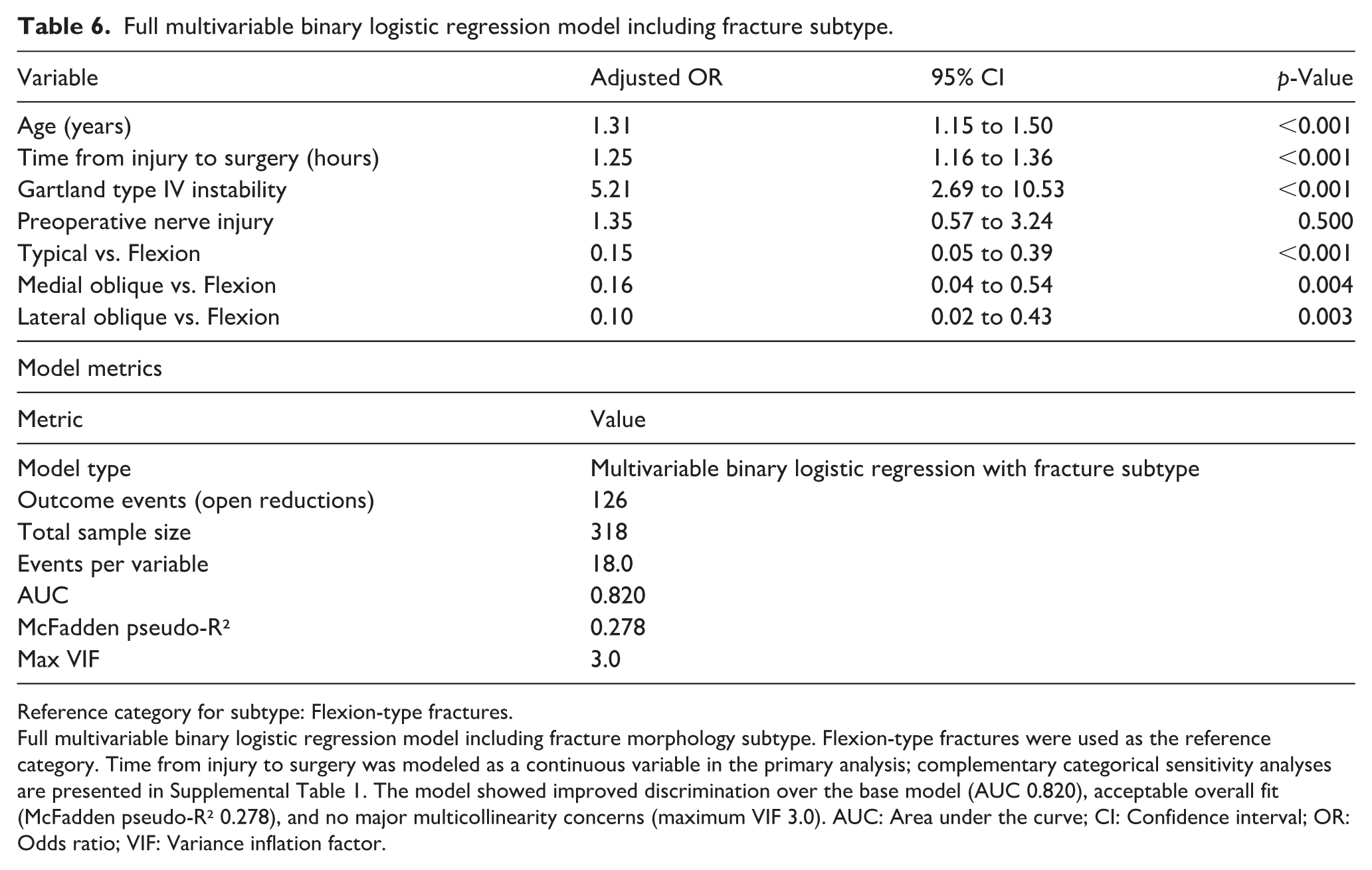
When fracture subtype was added to the model (Table 6), age, time from injury to surgery, and Gartland type IV instability remained associated with open reduction. Specifically, age was associated with a 31% increase in the odds of open reduction per year (OR 1.31, 95% CI 1.15 to 1.50; p < 0.001), and longer time from injury to surgery remained associated with conversion to open reduction in the primary continuous model (OR 1.25, 95% CI 1.16 to 1.36; p < 0.001). Adjusted odds ratios from the full multivariable model are summarized graphically in Figure 3. Because time to surgery showed a right-skewed distribution, additional sensitivity analyses were performed using categorical time intervals. Compared with surgery within 6 h, surgery at 6–12 h and after 12 h remained associated with higher odds of open reduction in both univariable and multivariable categorical analyses (Supplemental Table 1). Notably, although the adjusted odds ratio was higher in the >12-h category, the crude open reduction rates were similar between the 6–12-h and >12-h groups, suggesting possible instability of the estimate in the smallest delay category rather than a clear dose–response relationship. Gartland type IV instability remained strongly associated with open reduction, with more than fivefold higher adjusted odds (OR 5.21, 95% CI 2.69 to 10.53; p < 0.001). Preoperative nerve injury remained nonsignificant. Relative to flexion-type fractures, typical, medial oblique, and lateral oblique patterns were all associated with significantly lower adjusted odds of open reduction, with adjusted odds ratios of 0.15, 0.16, and 0.10, respectively. The full model demonstrated improved discriminative performance compared with the base model (AUC 0.820), with acceptable overall fit (McFadden pseudo-R² 0.278) and no major multicollinearity concerns (maximum VIF 3.0; Figure 4).
Full multivariable binary logistic regression model including fracture subtype.
Reference category for subtype: Flexion-type fractures.
Full multivariable binary logistic regression model including fracture morphology subtype. Flexion-type fractures were used as the reference category. Time from injury to surgery was modeled as a continuous variable in the primary analysis; complementary categorical sensitivity analyses are presented in Supplemental Table 1. The model showed improved discrimination over the base model (AUC 0.820), acceptable overall fit (McFadden pseudo-R² 0.278), and no major multicollinearity concerns (maximum VIF 3.0). AUC: Area under the curve; CI: Confidence interval; OR: Odds ratio; VIF: Variance inflation factor.
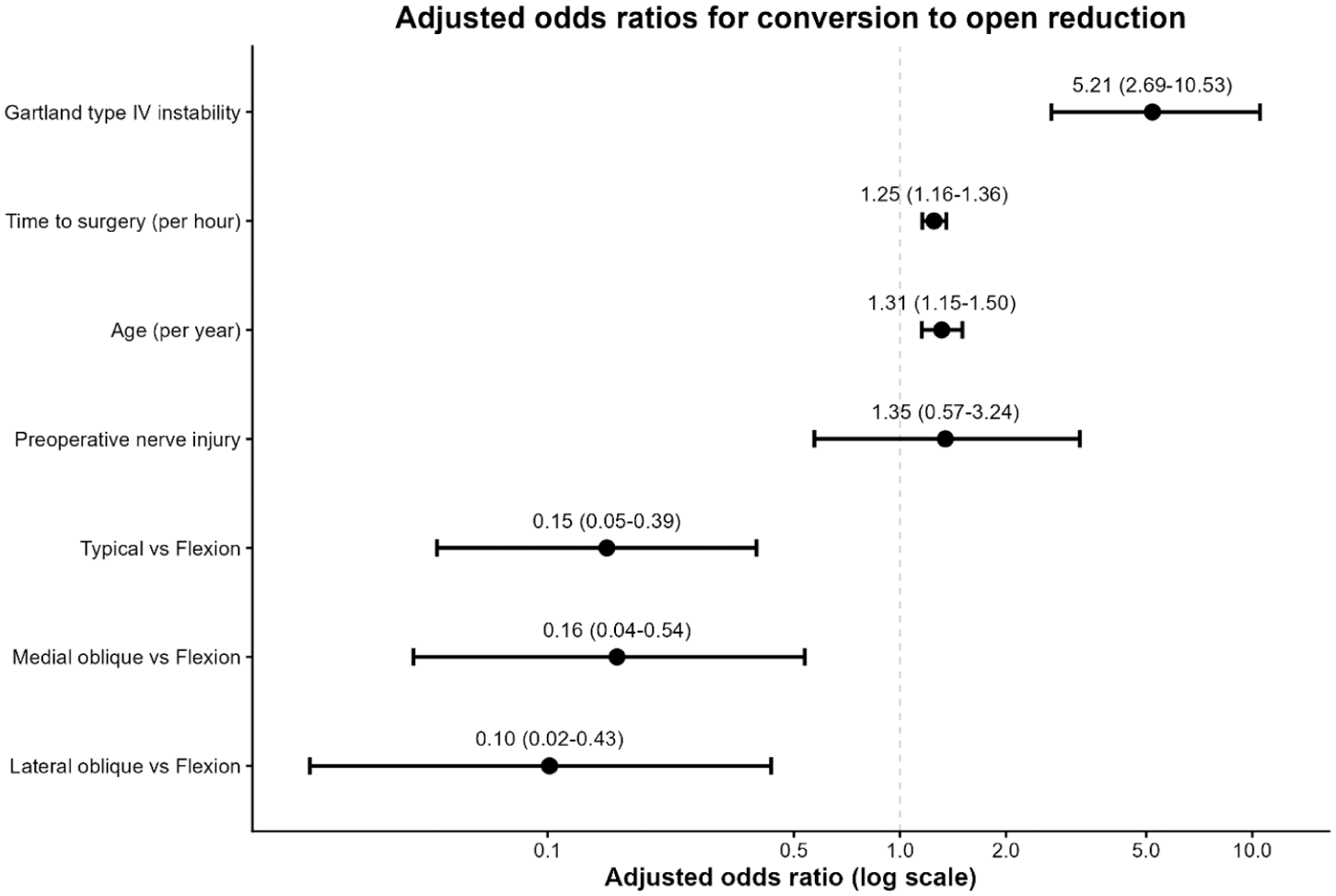
Forest plot of adjusted odds ratios from the full multivariable logistic regression model.
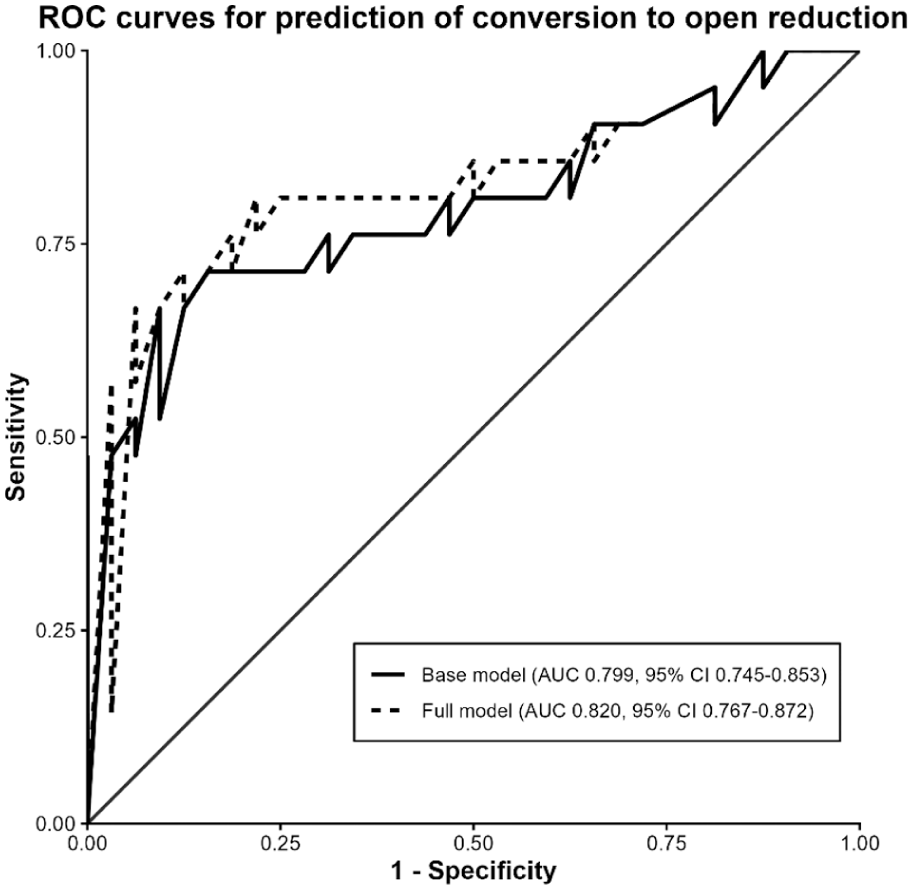
ROC curves of the base and full multivariable logistic regression models predicting conversion to open reduction.
Discussion
The main finding of this study was that failed closed reduction in high-risk pediatric SCHF was associated with a combination of fracture morphology, intraoperative multidirectional instability, age, and time from injury to surgery. Among these factors, flexion-type morphology and intraoperatively confirmed Gartland type IV instability were the most clinically relevant fracture-related features. These findings are consistent with recent literature showing that fracture pattern, neurological status, obesity, selected radiographic features, and instability-related factors may influence the likelihood of open reduction in displaced pediatric SCHF.5,7 –12 By evaluating these variables within a single multivariable model, the present study supports a practical risk-stratification approach for anticipating reduction difficulty in high-risk cases.
The conversion rate observed in this study was relatively high and should be interpreted in the context of the study population. This cohort was limited to displaced high-risk fractures in which an initial closed reduction was attempted and included a substantial proportion of flexion-type and intraoperatively unstable injuries. Therefore, the observed conversion rate should not be interpreted as the open reduction rate for all pediatric SCHF. Importantly, the aim of the study was not to establish a universal open reduction rate, but to identify factors associated with failed closed reduction within a high-risk cohort treated using a consistent institutional protocol. Nevertheless, because conversion may still be influenced by surgeon judgment, this issue has been acknowledged as a limitation.
Fracture morphology was strongly associated with reduction success in our cohort. In particular, flexion-type fractures demonstrated a markedly higher rate of open reduction (80%), which is consistent with prior studies reporting substantially increased odds of failed closed reduction and conversion to open reduction in this subgroup. Prior studies have consistently identified flexion-type configuration as a high-risk pattern for failed closed reduction and conversion to open reduction.9 –12 In our analysis, this association persisted in both univariable and multivariable models, with nonflexion fracture patterns showing significantly lower adjusted odds of open reduction. Although the underlying mechanism cannot be directly assessed in this study, flexion-type injuries are thought to be associated with anterior soft-tissue interposition and disruption of stabilizing periosteal structures, which may hinder the achievement and maintenance of closed reduction. These findings underscore the importance of careful preoperative assessment of fracture morphology and suggest that flexion-type configuration should be considered a high-risk pattern for conversion to open reduction.
Gartland type IV instability was associated with higher odds of conversion to open reduction in our study. However, this finding should not be interpreted to mean that instability alone is an indication for open reduction. Unstable fractures may still be successfully reduced and stabilized percutaneously when acceptable alignment can be obtained and maintained. In the present study, conversion to open reduction reflected failure to achieve or maintain acceptable reduction despite closed maneuvers. Therefore, intraoperatively confirmed multidirectional instability should be interpreted as a risk marker for reduction difficulty rather than as a standalone indication for open reduction. This interpretation is consistent with previous reports describing type IV fractures as multidirectionally unstable injuries with loss of periosteal support, which may increase the difficulty of achieving and maintaining closed reduction.15,16
The association between increased time from injury to surgery and higher odds of open reduction warrants careful interpretation. Although a statistically significant relationship was observed in our analysis, current evidence does not consistently support a direct causal effect of surgical delay on reduction failure. Previous studies have reported no significant increase in open reduction rates or perioperative complications with delayed treatment beyond the first 12 to 24 h,13,14 and recent meta-analytic data suggest that the effect of delay is highly heterogeneous and likely confounded by fracture severity and associated injury characteristics. 5 In our cohort, the distribution of time to surgery was markedly right-skewed, with a small number of extreme delays. Sensitivity analyses using categorical time intervals showed that, compared with surgery within 6 h, both 6–12-h and >12-h delays remained associated with higher odds of open reduction. However, the crude open reduction rates were very similar between the 6–12-h and >12-h groups, despite a larger adjusted odds ratio in the >12-h category, suggesting that the latter estimate may have been influenced by small sample size and model instability rather than a true dose–response pattern. Accordingly, this finding should not be interpreted as a simple hour-by-hour causal relationship. More plausibly, surgical timing in this setting reflects case complexity, soft-tissue status, and treatment prioritization. Therefore, time to surgery should be interpreted as a context-dependent factor rather than a standalone predictor.
Older age was independently associated with an increased likelihood of open reduction in our cohort. This finding is consistent with previous studies identifying age as a contributing factor in reduction difficulty.5,8,11 Several mechanisms may explain this association. Older children are more likely to sustain higher-energy injuries, which may result in greater fracture displacement and soft-tissue disruption. In addition, increased muscle mass and soft-tissue resistance may limit the effectiveness of closed reduction maneuvers. Furthermore, age-related differences in fracture characteristics and periosteal integrity may reduce the likelihood of achieving and maintaining stable closed reduction.
Preoperative nerve injury showed a strong association with open reduction in univariable analysis but did not remain significant after multivariable adjustment. This finding suggests that nerve injury may function as a surrogate marker of fracture severity rather than an independent predictor. Previous studies have demonstrated that nerve injuries, particularly in flexion-type fractures, are closely associated with more complex fracture patterns and increased likelihood of open reduction. 10 Moreover, larger reviews have emphasized that neurological deficits often reflect higher-energy trauma and greater soft-tissue disruption rather than acting as independent determinants of treatment strategy.2,5 When key factors such as fracture morphology and instability were accounted for in our model, the independent contribution of nerve injury diminished. This finding underscores the importance of multivariable modeling in distinguishing true independent predictors from correlated clinical features.
The multivariable models showed acceptable to good discrimination, with an AUC of 0.799 for the base model and 0.820 for the full model including fracture subtype. 17 The improvement after adding fracture morphology supports its clinical relevance for risk stratification. The events-per-variable ratio and VIF were also acceptable, supporting the stability of the regression estimates.18,19
Clinically, these findings may help surgeons anticipate reduction difficulty and plan operative resources in high-risk cases. Recognition of flexion-type morphology and intraoperatively identified multidirectional instability may support preoperative counseling, operating room preparation, and intraoperative decision-making.
This study has several limitations. First, its retrospective design introduces potential selection bias and limits causal inference. In particular, treatment decisions and timing of surgery may have been influenced by clinical factors not fully captured in the dataset. Second, this was a single-center study, which may limit the generalizability of the findings to other institutions with different patient populations or surgical practices. Third, although the overall cohort size was substantial, certain subgroups—particularly flexion-type fractures—were relatively small, which may affect the precision of subgroup estimates. Fourth, intraoperative decision-making regarding conversion to open reduction, although guided by predefined criteria, may still be subject to surgeon-dependent variability. Surgeon-level variation was not analyzed separately, which should be considered when interpreting the relatively high conversion rate and the generalizability of the findings. Fifth, specific mechanical obstacles to closed reduction, such as soft-tissue interposition, brachialis entrapment, or the exact intraoperative reason for irreducibility, were not uniformly documented in the operative records and therefore could not be analyzed as separate variables. Finally, although multiple clinically relevant variables were included in the multivariable models, residual confounding from unmeasured factors cannot be entirely excluded.
Conclusion
In this single-center high-risk cohort, flexion-type fracture morphology and intraoperatively confirmed Gartland type IV instability were strongly associated with failed closed reduction in pediatric SCHF. Older age and longer time from injury to surgery were also associated with conversion to open reduction, although the timing association should be interpreted cautiously as a possible marker of case complexity rather than a direct causal effect. These findings may help surgeons anticipate reduction difficulty and plan operative resources, but external validation is needed before broader generalization.
Supplemental Material
sj-docx-1-cho-10.1177_18632521261466892 – Supplemental material for Fracture morphology and multidirectional instability in failed closed reduction of pediatric supracondylar humerus fractures
Supplemental material, sj-docx-1-cho-10.1177_18632521261466892 for Fracture morphology and multidirectional instability in failed closed reduction of pediatric supracondylar humerus fractures by Muhammed Furkan Darilmaz and Mustafa Bulut in Journal of Children's Orthopaedics
Supplemental Material
sj-pdf-1-cho-10.1177_18632521261466892 – Supplemental material for Fracture morphology and multidirectional instability in failed closed reduction of pediatric supracondylar humerus fractures
Supplemental material, sj-pdf-1-cho-10.1177_18632521261466892 for Fracture morphology and multidirectional instability in failed closed reduction of pediatric supracondylar humerus fractures by Muhammed Furkan Darilmaz and Mustafa Bulut in Journal of Children's Orthopaedics
Footnotes
Author contributions
MFD contributed to study conception, methodology, statistical analysis, manuscript drafting, and critical revision. MB contributed to data curation, data interpretation, supervision, and critical revision. All authors read and approved the final manuscript.
Availability of data and materials
The datasets analyzed during the current study are available from the corresponding author upon reasonable request. All data are anonymized and stored securely in accordance with institutional and ethical regulations.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethics approval and consent to participate
This retrospective cohort study was conducted at the Department of Orthopaedics and Traumatology, Aksaray University Training and Research Hospital. The study protocol was approved by the Institutional Ethics Committee of Aksaray University (Approval number: 2026/112, SAGETIK 2026-83). Due to the retrospective design of the study and the use of anonymized data, the requirement for informed consent was waived by the Institutional Ethics Committee of Aksaray University. All procedures were performed in accordance with the ethical standards of the institutional and national research committee and with the 1964 Helsinki Declaration and its later amendments.
Permission to reproduce material from other sources
No previously published figures, tables, or copyrighted materials were reproduced in this study. Therefore, no permissions were required.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.