
Abstract
Early detection of ovarian cancer, particularly high-grade serous ovarian cancer (HGSOC), remains challenging due to the lack of reliable biomarkers. This study investigated the potential of tRNA-derived small RNAs (tsRNAs) as non-invasive diagnostic biomarkers using liquid biopsy. Using qRT-PCR, we analyzed the relative Ct values of selected tsRNAs in plasma samples from healthy controls and patients with early- and late-stage HGSOC. A logistic regression model constructed using the relative Ct value of the selected tsRNA demonstrated high sensitivity and specificity for distinguishing ovarian cancer patients from healthy controls, including those with early-stage disease. The model was validated in a multi-center cohort, and analysis confirmed the dysregulation of this tsRNA in tumor tissue compared to normal tissue. These findings suggest that this single plasma tsRNA may serve as a promising biomarker for early HGSOC detection, supporting its potential clinical utility pending further mechanistic studies.
Introduction
Ovarian cancer (OC), with high-grade serous ovarian cancer (HGSOC) accounting for the majority of pathological subtypes, is one of the most lethal malignancies in gynecology due to its insidious symptoms and the difficulty of early diagnosis.1,2 Despite the availability of various screening methods for early detection of OC, including imaging techniques (ultrasound, CT, MRI), blood biomarker assessments (e.g., CA-125, HE4), and multifarious diagnostic models (e.g., the ROMA model), yet none of these methods has demonstrateed satisfactory efficacy and convenience, resulting in only a limited number of cases being detected at early stages.3,4 This delayed detection greatly complicates treatment, leading to poor cure rates and overall survival.5–7 Evidence showed that the 5-year survival rate for stage I disease of OC is more than 90%, while that for advanced disease is lower than 30%.1,8 Therefore, developing a more reliable and effective early diagnostic tool is essential for facilitating treatment and ultimately prolonging the survival time for OC patients.
Small RNAs are small non-coding RNA (sncRNA) molecules, which include microRNA (miRNA), Piwi-interacting RNA (piRNA), tRNA-derived small RNAs (tsRNAs), etc. 9 Interestingly, tRNA-derived small RNAs (tsRNAs) are a newly discovered class of small RNAs identified through advances in sequencing technologies. 10 Previous studies have shown that tsRNAs not only accumulate intracellularly to exert biological functions but are also secreted by various cells and delivered between extracellular matrix and into bodily fluids.11,12 Due to the unique nucleotide modifications, tsRNAs exhibit great stability in bodily fluids as compared to traditional markers, making them a promising candidate for non-invasive, highly sensitive biomarker development.11,13 However, the potential of tsRNAs being a biomarker for early detection of OC, especially HGSOC, has not been stated yet.
An increasing number of early diagnostic methods rely on the detection of biomarkers in bodily fluids, such as plasma and urine, significantly enhancing the early detection rates of various tumors.14–17 Given the stability of tsRNAs in bodily fluids, they hold great potential as biomarkers for early cancer detection.18,19 In this study, we subjected plasma samples of 5 normal controls (NC), 5 early-stage HGSOC (EOC), and 5 late-stage HGSOC (LOC) to small RNA sequencing and developed a diagnostic model with strong performance for HGSOC, based on real-time quantitative reverse transcription PCR (qRT-PCR), utilizing regression analysis.
Materials and methods
Sample collection
Plasma samples were prospectively collected from patients prior to any therapy at the First Affiliated Hospital of Sun Yat-sen University between May 2023 and July 2024. Detailed criteria for participant inclusion and exclusion are provided in Supplementary Materials. All participants provided written informed consent, and the study was conducted in accordance with the principles of the Declaration of Helsinki. The study protocol was approved by the Institutional Review Boards of all participating institutions.
A total of 158 samples were obtained from the First Affiliated Hospital of Sun Yat-sen University. These samples were randomly allocated into the following cohorts: a sequencing cohort (n = 15; including 5 normal controls [NC], 5 early-stage ovarian cancer [EOC], and 5 late-stage ovarian cancer [LOC]), a discovery cohort (n = 30; 10 NC, 10 EOC, 10 LOC), a model construction cohort (n = 93; 44 NC, 49 OC), and an external validation cohort (n = 20; 10 NC, 10 OC). Additionally, 60 independent samples were collected from two external medical centers: 30 from Xinhua Hospital Affiliated to Shanghai Jiaotong University School of Medicine (10 NC, 20 OC) and 30 from Hangzhou People’s Hospital (10 NC, 20 OC), to further validate the model for multi-center validation. There were no significant differences in key clinical parameters among the different cohorts, as confirmed by appropriate statistical tests (p > 0.05), ensuring the comparability of groups for subsequent analyses. The patient selection process is presented in Figure 1. Flowchart of patient selection.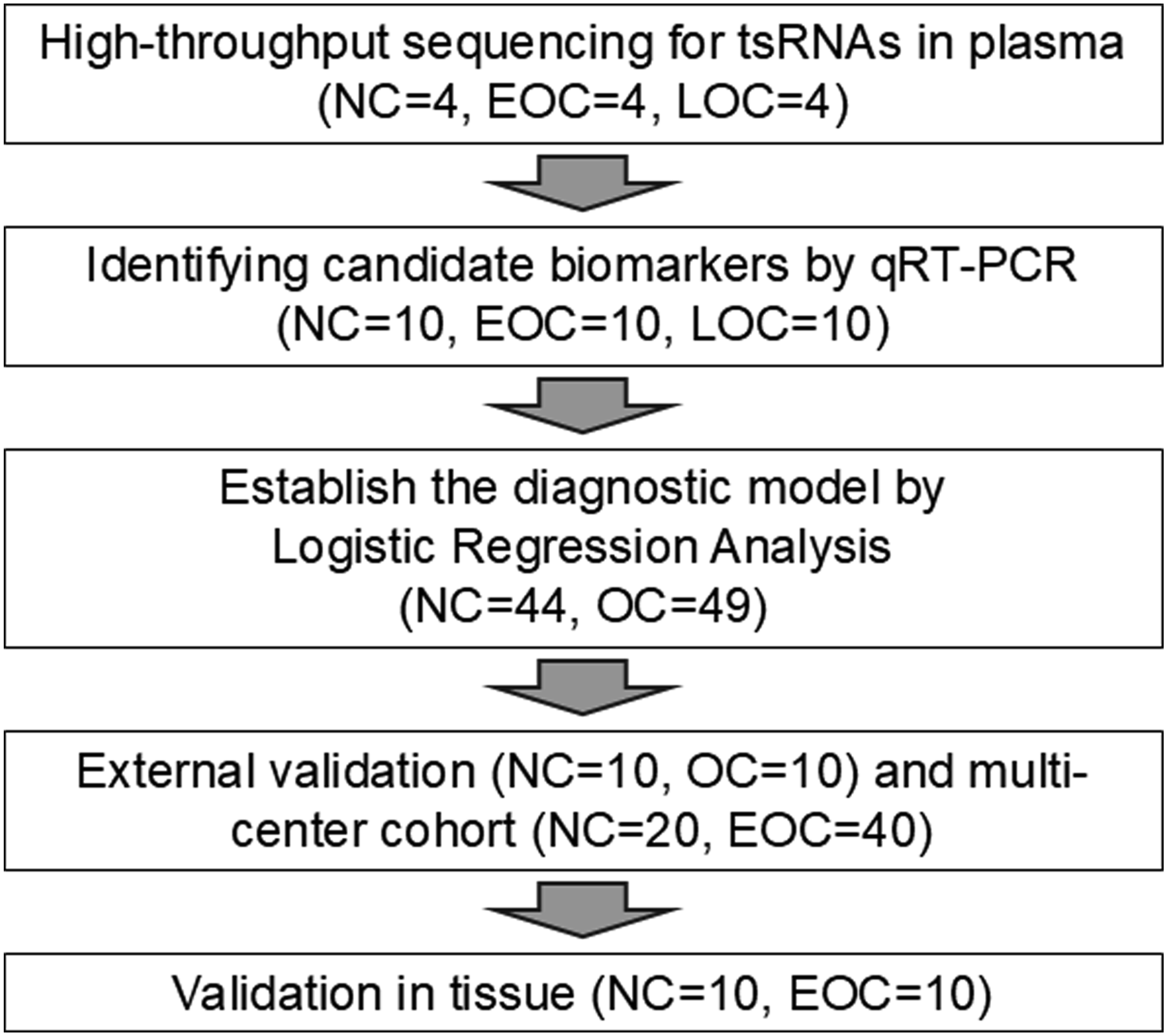
RNA sequencing data were obtained from The Cancer Genome Atlas (TCGA, https://portal.gdc.cancer.gov/) database for HGSOC patients (n=422) and the fallopian tube RNA sequencing of normal controls (n=180) was acquired from a professional website-The Genotype-Tissue Expression (GTEx, https://www.gtexportal.org/) portal. Every dataset from the TCGA and GTEx databases was available to the general public. And unnecessarily for ethics committee approval for those data.
Plasma RNA extraction
Peripheral venous blood samples (300 μL) were collected in EDTA anticoagulant tubes and immediately centrifuged at 1750 × g for 10 minutes at 4°C. The plasma was then aseptically aliquoted and stored at -80°C. RNA extraction was performed using the TRIzol method, specifically targeting small RNAs. Plasma was mixed with three times the volume of TRIzol, vortexed immediately, and after standing for a brief period, 1/5 volume of chloroform was added and vortexed again. The mixture was left at room temperature for 3-5 minutes, followed by centrifugation at 16000g for 20 minutes at 4°C. The supernatant was collected and mixed with two volumes of isopropanol, and RNA was precipitated at -20°C for 12 hours. After another round of centrifugation at 16000 × g for 20 minutes at 4°C, the supernatant was discarded, and 1 mL of 75% ethanol was added, followed by centrifugation at 16000 × g for 20 minutes at 4°C. The liquid was decanted, and the RNA was dissolved in an appropriate volume of DEPC-treated water. The RNA concentration was adjusted to 400 ng/μL using a Nanodrop One (Thermo Fisher Scientific, USA).
Sequencing and primer design for tsRNAs
Sequencing was performed using PANDORA-seq, which employs a combinatorial enzymatic treatment to remove key RNA modifications that block adapter ligation and reverse transcription in sncRNA. The sequencing was conducted by Guangzhou Epigenetics Co., Ltd. 20 The comparison and identification of mature or precursor tRNA sequences were based on the small RNA annotation software SPORTS1.1 (available on GitHub at https://github.com/junchaoshi/sports1.1). Primer design and synthesis were carried out by Guangzhou RiboBio Co., Ltd., using the stem-loop method. This technique is covered by the company’s patent, and as per the company’s policy, the primer sequences are not disclosed.
Quantitative reverse transcription PCR experiment
Each RNA sample was reverse-transcribed into cDNA using the Bulge-loop™ qRT-PCR primer set (RiboBio Co., Ltd., Guangzhou, China), specifically designed for tsRNAs according to the manufacturer’s instructions. qRT-PCR was conducted on a real-time fluorescence quantitative PCR instrument (Bio-Rad CFX Connect Real-Time PCR System 1855201, Bio-Rad Laboratories, Inc., USA) following the manufacturer’s protocol with universal reagents. The relative expression levels were normalized using RNU6B (U6) (RiboBio, Guangzhou, China) as an internal control. The comparative expression level was evaluated by 2^-ΔΔCt method.
Statistical analysis
Sequencing data differential analysis, model construction, and plotting were performed using R software (version 4.3.2; https://www.Rproject.org) and its associated packages. For analysis of biomarkers and construction of diagnostic model, logistic regression algorithm was applied and calculated by the formula: Logit(P) = b0 + b1*ΔCt1 + b2*ΔCt2 … + bn*ΔCtn, where the bn meant the nth regression coefficients and the ΔCti meant the relative cycle threshold of each biomarker.21,22 Statistical analysis of ΔCt and graphing were conducted using SPSS 26.0 and Origin 2023. For normally distributed data, differences were analyzed using the Student's t-test, while for non-normally distributed data, the Mann–Whitney test was used. A fold change threshold of 2 was set, and P < 0.05 was considered statistically significant. This partitioning of training and validation subsets was performed using the “createDataPartition” function from the “caret” package in R.
Results
tsRNAs of different abundance in plasma were screened out between HGSOC and healthy controls
To preliminarily assess the potential differences in tsRNA expression between HGSOC and normal fallopian tube epithelial tissues, we analyzed sequencing data from the GTEx (normal tissues) and TCGA (HGSOC tissues) databases. Analysis revealed differential expression of tsRNA-related genes, among which QTRT1 and SLFN13 showed significant differences in gene expression (Figure 2(A)). Based on this, we hypothesized that there may be differences in tsRNA levels between the plasma of HGSOC patients and that of healthy individuals. Consequently, we collected pre-treatment patients’ plasma from 5 normal controls (NC), 5 early-stage HGSOC (EOC), and 5 late-stage HGSOC (LOC) from our hospital. After RNA extraction and high-throughput sequencing, Uniform Manifold Approximation and Projection (UMAP) dimensionality reduction analysis was conducted to evaluate inter- and intra-group variability. Based on proximity in reduced-dimensional space, 4 NC, 4 EOC, and 4 LOC samples were selected for further analysis (Figure 2(B)). tsRNAs of different abundance between HGSOC and NC.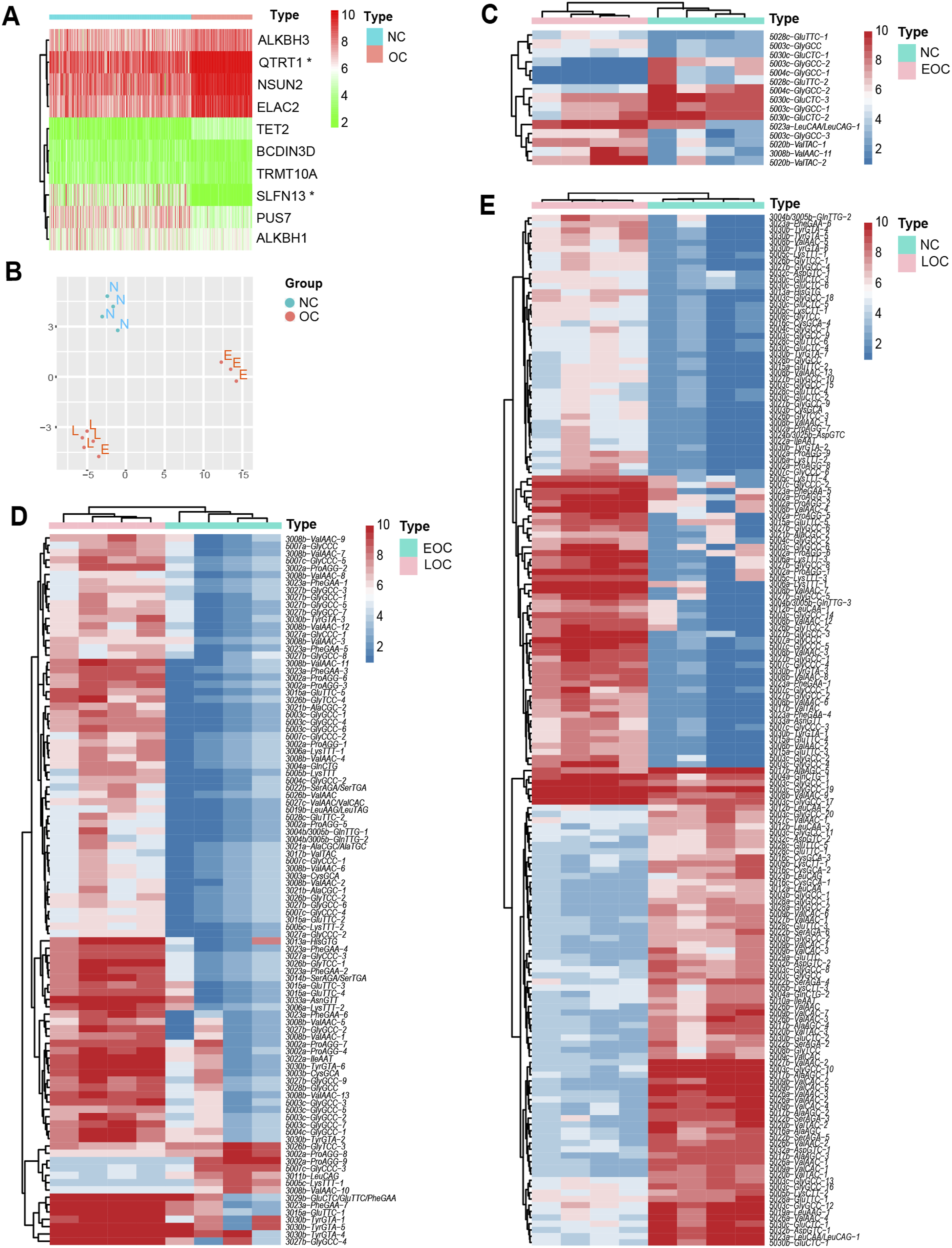
Based on the results of the differential analysis, we identified 15 fragments with statistically significant differences between NC and EOC (Figure 2(C)), 97 fragments between EOC and LOC (Figure 2(D)), and 166 fragments between NC and LOC (Figure 2(E)). To enhance diagnostic consistency across different clinical stages and compensate for the limited sample size of EOC specimens in subsequent large-scale modeling, for biomarker screening we selected fragments that exhibited statistically significant differences between the control group and early-stage patients, but no significant differences between early-stage and late-stage patients. A total of 8 fragments met these criteria.
Biomarkers were identified from the tsRNAs that met the specified criteria
Given the accessibility and widespread use of biomarker detection, further screening of biomarkers for model construction was performed using qRT-PCR technology. Due to the limitations of current techniques, only four fragments were suitable for specific primer design. These fragments are as follows: 1. tsRNA-5003c-GlyGCC; tsRNA-5004c-GlyGCC/GlyCCC (labeled as 3c1) 2. tsRNA-5003c-GlyGCC (labeled as 3c2) 3. tsRNA-5003c-GlyGCC; tsRNA-5004c-GlyGCC/GlyCCC (labeled as 3c3) 4. tsRNA-5020b-ValTAC; tsRNA-5020c-ValTAC (labeled as 20b)
The sequences of the fragments are provided in Supplementary Material.
For preliminary screening, we selected 10 NC and 10 EOC samples. The fragment labeled 3c1 did not follow the same trend observed in the sequencing data within the screening set. Although the fragment labeled 3c2 showed consistency with the sequencing results in plasma samples, the cycle threshold (Ct) values in qRT-PCR were greater than 33, indicating suboptimal reverse transcription feasibility. Fragments 3c3 and 20b demonstrated consistency with the sequencing data in plasma samples, along with good reverse transcription feasibility (Figure 3(A)). Following the designing logic for the target discovery process, we further included 10 LOC samples from the discovery cohort to evaluate the enrichment levels of the 3c3 and 20b fragments in the plasma of late-stage patients. The 3c3 fragment continued to exhibit the expected trend in LOC samples, whereas the 20b fragment did not meet the anticipated levels (Figure 3(B)). In a larger-scale validation (n = 93), 3c3 showed statistically significant abundance differences between NC and LOC samples, while 20b did not (Figure 3(C)). Consequently, we selected the 3c3 as the biomarker for model construction. Identification of candidate tsRNAs as biomarkers and construction of the diagnostic model.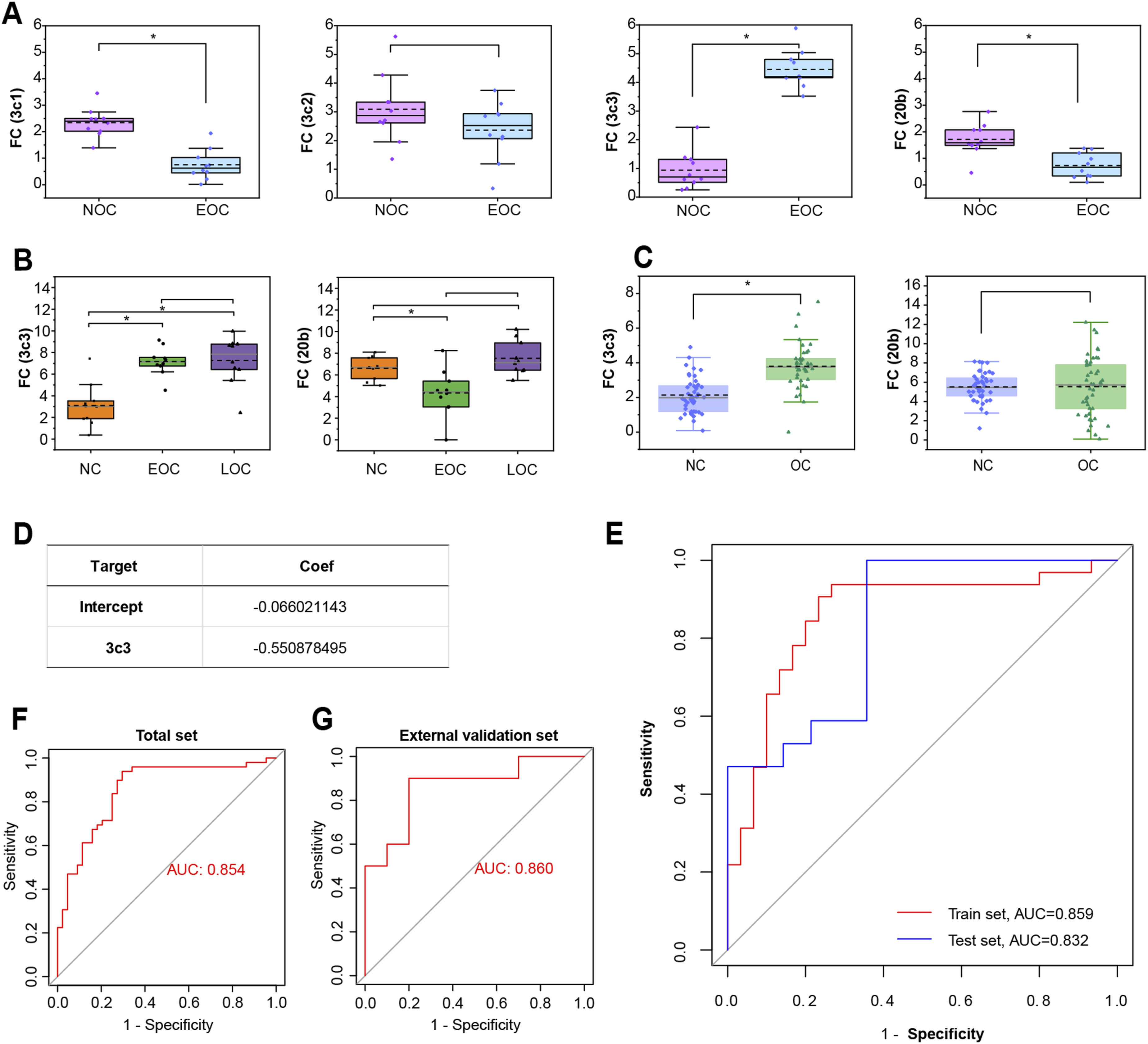
A diagnostic model was constructed based on a large sample size
We used the ΔCt values from qRT-PCR of plasma samples of NC and HGSOC patients for model construction. Given that the independent variable is a normally distributed continuous variable and the outcome is a binary variable, a logistic regression algorithm was applied. The modeling dataset was randomly divided, with 2/3 used as the training set and 1/3 as the internal validation set for model development. Ultimately, a model was successfully constructed based on the maximum area under the curve (AUC) of the receiver operating characteristic (ROC) curve from the training dataset (Figure 3(D)). The formula of derived model was as follows: Logit(P) = -0.066021143-0.550878495*ΔCt(3c3). According to the calculations, the AUC of the ROC curve was 0.859 for the training set and 0.832 for the internal validation set (Figure 3(E)), indicating that the model demonstrated good performance in both sets.
The model was further validated and exhibited excellent performance in early diagnosis of OC
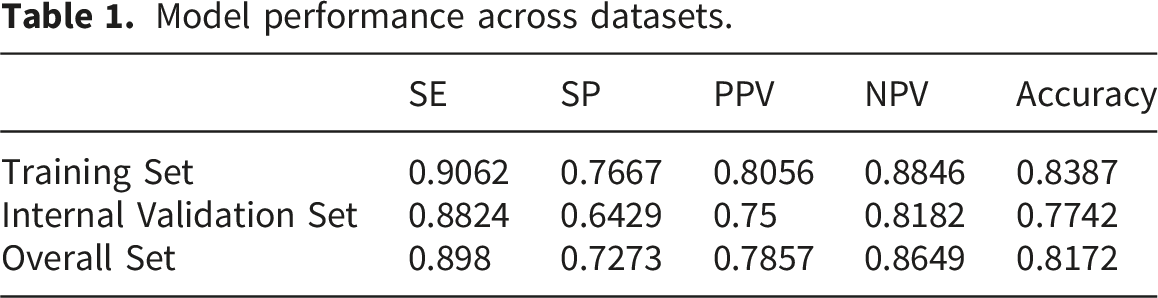
Model performance across datasets.
Performance evaluation and detection of tumor tissues.
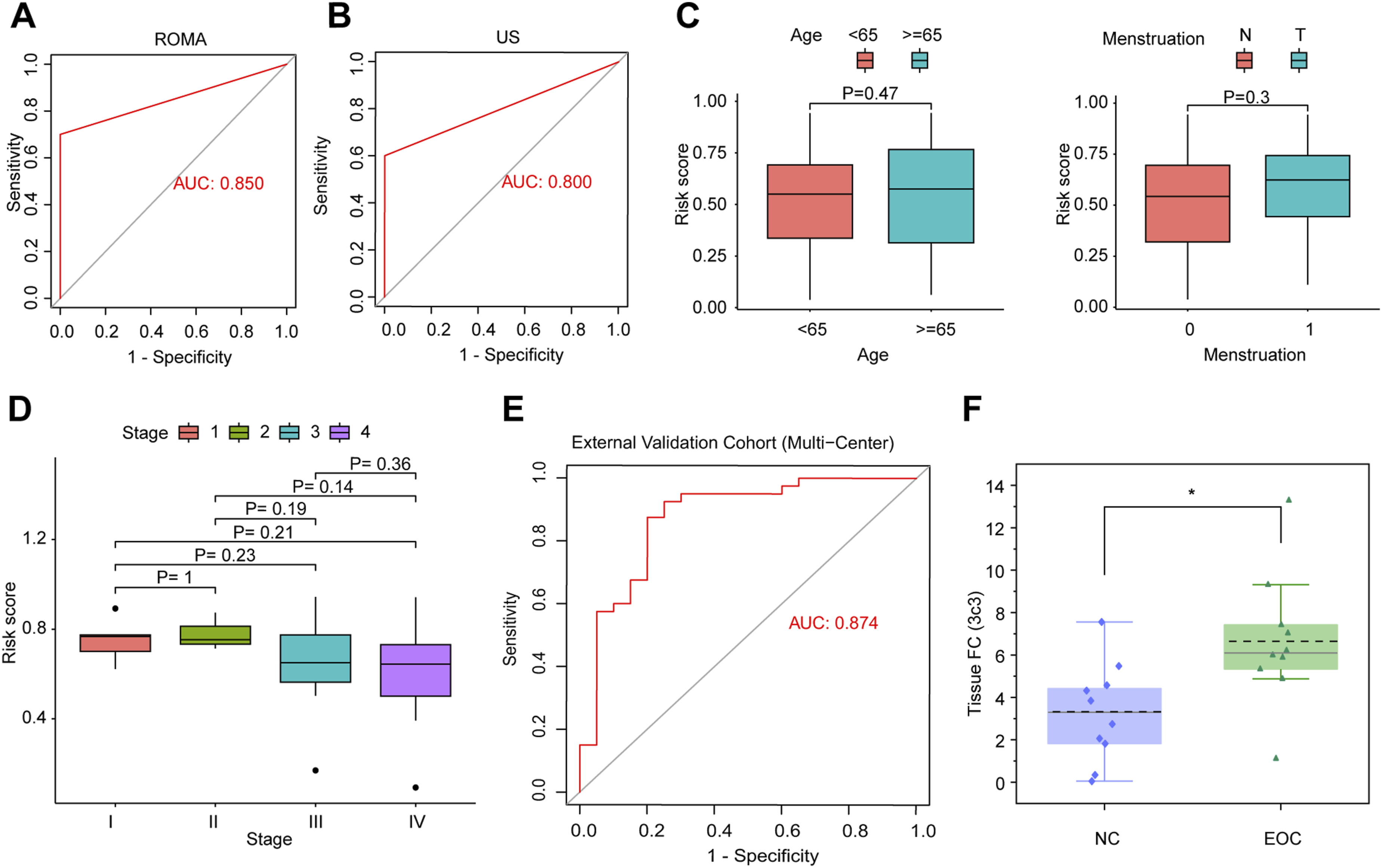
In addition, to evaluate the impacts of other clinical characteristics on the model’s score, we stratified the samples in the model construction set by different clinical parameters. The results indicated that there was no statistically significant difference in risk scores between these groups divided by age and menstrual status (Figure 4(C)). Furthermore, no significant difference was detected in risk scores across different clinical stages (Figure 4(D)). Taken together, these findings suggest that our model not only demonstrates strong performance in early diagnosis but is also independent of other clinical characteristics.
To evaluate the generalizability and diagnostic accuracy of our identified biomarker, we further validated the model using an independent multi-center cohort comprising 60 plasma samples collected from two additional hospitals (each providing 10 normal controls and 20 HGSOC patients). The validation results showed that the model achieved an AUC of 0.874 in the ROC analysis, demonstrating its robust generalizability and potential clinical utility for the early detection of ovarian cancer (Figure 4(E)).
The involved tsRNAs in the plasma are derived from cancerous tissue
To investigate whether the 3c3 fragment originates from cancerous tissue and to exclude the potential influence from high tumor burden, such as cachexia in advanced stages, we collected fallopian tube epithelial tissues from 10 NC patients and cancerous tissues from 10 EOC patients to perform qRT-PCR for tissue validation. The results showed that the abundance of the 3c3 fragment was significantly higher in EOC tissues compared to NC tissues (Figure 4(F)). This preliminary evidence suggests that the biomarker fragment in the diagnostic model is derived from tumor tissues.
Discussion
Despite advancements in surgical techniques and chemotherapy regimens, the prognosis for HGSOC remains poor, primarily due to its frequent diagnosis at advanced stages.1,23,24 This delay in detection contributes to suboptimal outcomes of surgery and the development of chemotherapeutic resistance after treatment.25–28 Therefore, early detection and intervention remain crucial for significantly improving HGSOC patient prognosis.5,29 Current biomarkers for OC, such as CA-125 and microRNAs, suffer from limited sensitivity and specificity, especially in early-stage disease.30,31 Thus, there is an urgent need to identify novel, non-invasive, and clinically applicable biomarkers that can improve early diagnostic accuracy and survival outcomes in ovarian cancer.
An increasing number of evidence suggest that small non-coding RNAs play a significant role in tumorigenesis and detection.11,12,32–35 Furthermore, their enrichment in tumor cells and secretion into plasma offer a promising pathway for early detection of cancer.36,37 Moreover, specific RNA modifications, such as methylation and acetylation, enhance the stability of tsRNAs in bodily fluids, making them ideal biomarkers for non-invasive testing. 13 Previous studies have focused on tsRNA-based biomarkers for cancers such as pancreatic, gastric cancer, breast cancer and so on.10,38–42 Although there are other existing biomarkers for ovarian cancer, such as CA125 and microRNAs, their efficacy and specificity remain suboptimal, and tsRNA-based biomarkers for ovarian cancer represent an underexplored area.4,43
We initially identified compositional differences in tsRNAs between the plasma of HGSOC patients and non-tumor patients through small RNA sequencing. Of eight tsRNA fragments differentially enriched in plasma of HGSOC patients, we found out one tsRNA fragment—tsRNA-5003c-GlyGCC/tsRNA-5004c-GlyGCC/GlyCCC—emerge as a particularly promising marker. By logistic regression algorithm, a model was successfully constructed using a large sample size and verified in two observational cohorts (one as a retrospective training cohort and the other as a prospective validation cohort). The analysis demonstrated that the model exhibited strong performance in predicting the presence of HGSOC with a promising AUC value regardless of other clinical parameters. Its efficacy in distinguishing early-stage patients from healthy controls surpasses that of other existing serum markers, highlighting its great potential as an early diagnostic biomarker (Figure 5). Flowchart of this study process.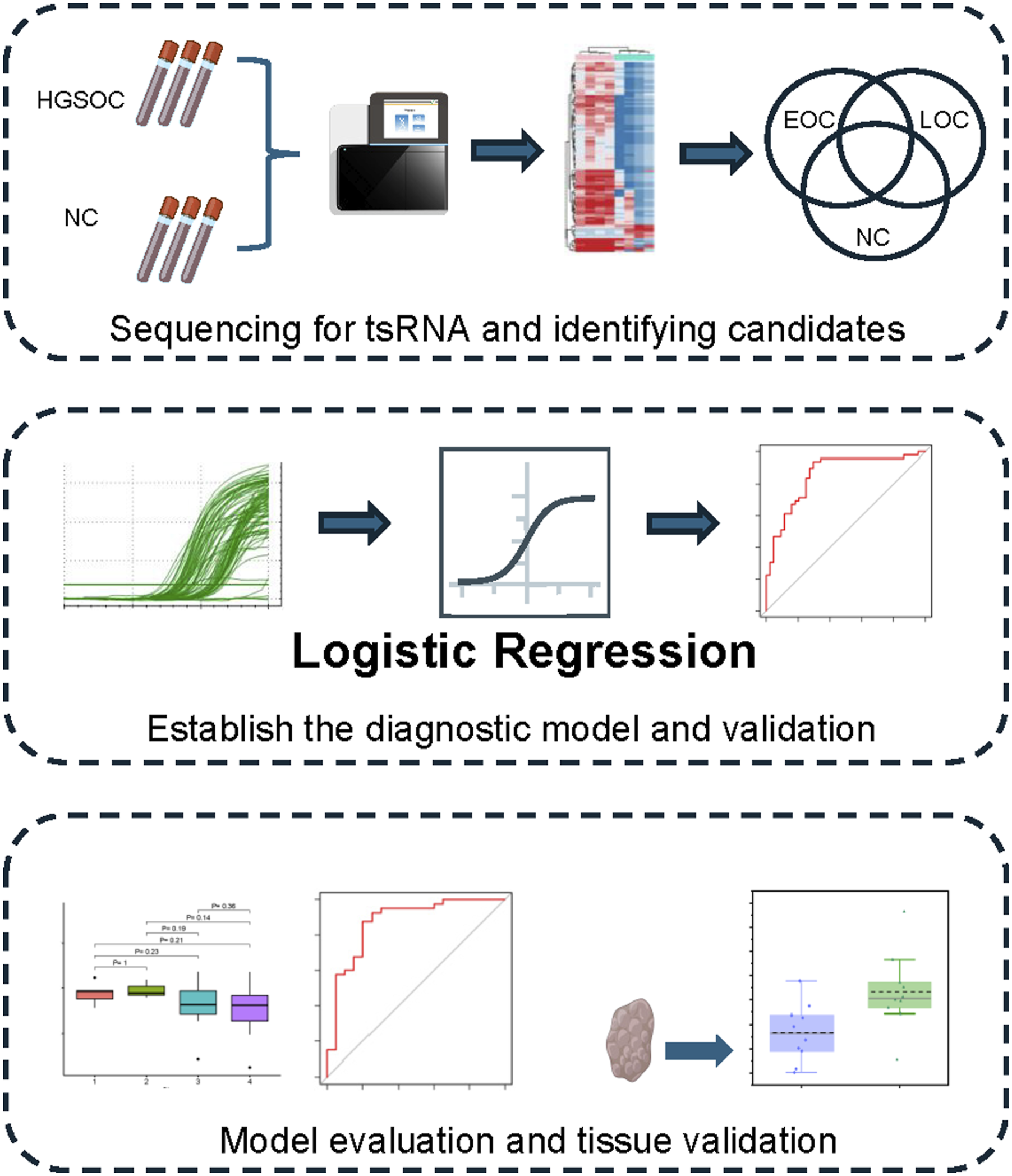
Prior to this study, although research had explored the biological roles of tsRNA in OC, no diagnostic models based on tsRNAs for early-stage HGSOC had been developed.44–47 This study is the first to demonstrate the potential of tsRNAs as diagnostic biomarkers for early-stage HGSOC. However, the limitations of this study include the lack of multicenter validation to assess its generalizability, and no investigation into the mechanisms underlying the generation of this tsRNA has been carried out. Additionally, while our model demonstrates promising diagnostic performance, further studies involving cost-effectiveness analyses are warranted to fully assess its practical advantage over existing screening methods in routine clinical practice.
Conclusion
In this study, we identified a specific tsRNA sequence in plasma that can serve as a non-invasive, convenient, and reliable biomarker for the diagnosis of human HGSOC, particularly demonstrating superior performance in early-stage detection compared to other existing screening methods. However, further research is necessary to elucidate the mechanisms underlying the production of this tsRNA and to assess its potential for clinical application.
Supplemental material
Supplemental material - A novel diagnostic model for early-stage high-grade serous ovarian cancer based on serum tRNA-derived fragments
Supplemental material for A novel diagnostic model for early-stage high-grade serous ovarian cancer based on serum tRNA-derived fragments by Xueyuan Zhao, Weijia Wen, Jia Yan, Li Yuan, Linna Chen, Songlin Liu, Haolin Fan, Hongye Jiang, Chaoyun Pan, Chunyu Zhang, Shuzhong Yao in Cancer Biomarkers
Supplemental material
Supplemental material - A novel diagnostic model for early-stage high-grade serous ovarian cancer based on serum tRNA-derived fragments
Supplemental material for A novel diagnostic model for early-stage high-grade serous ovarian cancer based on serum tRNA-derived fragments by Xueyuan Zhao, Weijia Wen, Jia Yan, Li Yuan, Linna Chen, Songlin Liu, Haolin Fan, Hongye Jiang, Chaoyun Pan, Chunyu Zhang, Shuzhong Yao in Cancer Biomarkers
Footnotes
Ethical considerations
The studies involving humans were approved by Committee on the Use of Clinical Research of the First Affiliated Hospital of Sun Yat-sen University. The studies were conducted in accordance with the local legislation and institutional requirements. The design of this study follows the tenets of the Declaration of Helsinki. The research methods and specimen collection procedures involved in this study were submitted to and approved by the Ethics Committee of The First Affiliated Hospital of Sun Yat-sen University (No. [2022]510).
Consent to participate
All participants provided written informed consent, and the study was conducted in accordance with the principles of the Declaration of Helsinki.
Author Contributions
Xueyuan Zhao and Yan Jia performed the experiments and analyzed the data. Xueyuan Zhao and Weijia Wen wrote the manuscript. Li Yuan, Songlin Liu, and Haolin Fan participated in the experiments and assisted with the collection of clinical data. Chaoyun Pan provided guidance on experimental design. Chunyu Zhang conceived the project and secured funding. Shuzhong Yao and Hongye Jiang provided resources, obtained funding, and supervised the project. All authors contributed to the article, reviewed and approved the submitted version, and agreed to be accountable for all aspects of the work.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the National Key R&D Program of China (2022YFC2704201 to Shuzhong Yao), National Natural Science Foundation of China (82273365 to Shuzhong Yao, 82403524 to Chunyu Zhang), China Postdoctoral Science Foundation (2023M744070 and 2024T171074 to Chunyu Zhang), Postdoctoral Fellowship Program of CPSF (GZC20233282 to Chunyu Zhang), Guangdong Medical Science and Technology Research Foundation (A2024280 to Chunyu Zhang), Science and Technology Plan of Guangdong Province (2023A0505050102 to Shuzhong Yao), Guangzhou Science and Technology Program (2024B03J1336 to Shuzhong Yao), Sun Yat-sen University Clinical Research Foundation of 5010 Project (2017006 to Shuzhong Yao), and Guangdong Basic and Applied Basic Research Foundation (2023A1515110333 to Chunyu Zhang, 2024A1515013045 to Hongye Jiang).
Declaration of conflicting interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
Data Availability Statement
The data used and/or analyzed during the current study are available upon reasonable requests.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.