
Abstract
Automated leukaemia detection has received considerable attention in medical image processing, thanks to advances in machine learning and deep learning. Yet, differences in data sets, testing techniques and benchmarking strategies still pose difficulties for understanding their effectiveness. This paper offers a comprehensive analysis and review of selected works related to automated leukaemia detection using a data-driven approach. Instead of focusing on accuracy values, this review emphasises multi-metric evaluation, including sensitivity, specificity, F1-score, AUC, and dataset characteristics. The evaluation explores trends in performance over time, variability across methods, patterns of dataset use, and the distribution patterns of reported performance metrics. Visualisations and descriptive analysis of performance trends suggest that the characteristics of datasets, such as size, diversity, and representativeness, have a greater effect on accuracy than the complexity of model architectures. While recent studies on CNNs, hybrid models, and Transformers show a tendency to cluster in higher-accuracy ranges, there are still challenges in areas such as dataset bias, inconsistent benchmarking, lack of cross-validation across datasets, interpretability, and clinical applicability. To overcome these challenges, this review recommends a research roadmap that focuses on data-centric development, clinical applicability, and interpretability. The results of the review suggest moving away from optimising performance toward robustness, clinical applicability, and interpretability, offering insights into the development of a clinically applicable AI-assisted system for leukaemia detection.
Keywords
Introduction
Leukaemia represents a diverse group of haematological malignancies characterised by abnormal proliferation and differentiation of white blood cells, leading to progressive impairment of normal haematopoiesis. So, according to global cancer statistics, leukaemia continues to contribute significantly to cancer-related morbidity and mortality across both paediatric and adult populations, with notable geographic and demographic variation (Day, 2024; Siegel et al., 2025; Huang et al., 2023). The
Diagnosis of leukaemia is based on manual microscopic analysis of peripheral blood and bone marrow smear samples, along with immunophenotyping, cytogenetics, and molecular techniques. Although the method can be labour-intensive and prone to human error, it remains an essential tool for diagnosis because it is a subjective procedure that is vulnerable to inter-examiner variability, fatigue-related human error, and limited scalability in large-volume medical environments (Dores et al., 2012; Saleem et al., 2022). This has led to ongoing research into automated and computer-aided detection systems to support hematopathologists.
As noted in (Mishra et al., 2019; American Cancer Society, n.d.; Jha & Dutta, 2019) the initial computational strategies for leukaemia detection largely focused on utilising handcrafted features extracted from segmented blood cells, including but not limited to image-based texture, shape, and statistics. The latter were usually applied in combination with conventional ML algorithms such as k-nearest neighbours, support vector machines, or random forests. Although such approaches proved capable of automating leukaemia classification, their effectiveness depended heavily on image quality and staining, as well as on the handcrafted features used (Anilkumar et al., 2023; Bin Aof et al., 2022; Shah et al., 2021).
The introduction of deep learning, mainly convolutional neural networks (CNNs), showed a significant shift toward data-driven feature learning in medical image analysis (Atteia et al., 2022). So, there is no need for manual feature engineering; they learn features automatically. Additionally, CNN models have been found to demonstrate better competence in learning hierarchical and discriminative features from the raw images compared to manually engineered features (Abhishek, Jha, et al., 2022; Claro et al., 2022). Various studies have reported high classification accuracy for leukaemia detection using pre-trained CNN architectures and transfer learning strategies (Abhishek et al., 2023; Ridoy & Islam, 2020; Bibi, 2020; DeSant et al., 2021; Bukhari et al., 2022; Loey et al., 2020). CNN-based and ensemble learning frameworks have also demonstrated strong performance in microscopic blood smear analysis and subtype classification tasks (Hosseini et al., 2023; Tran et al., 2018; Osman, 2021; Claro, 2020; Aziz et al., 2020). In addition to this, a number of recent works have considered hybrid CAD systems, lightweight approaches, and feature-based classifiers to increase robustness and computational efficiency (Kassani et al., 2019; Mathur, 2020; Fatonah et al., 2020; Liu & Hu, 2022). While improvements observed in these works can be attributed to favourable experimental settings, they might not necessarily translate to other data sets or healthcare settings. In particular, a number of recent studies have looked at combining hand-engineered and deep learning features to capture information from both low-level texture features and high-level learned features. In order to overcome the weaknesses of CNN-only models, (Attallah, 2024; Ahmed et al., 2023) examined Transformer architectures. At the same time, CNN-Transformer hybrids have also been proposed to capture long-term dependencies and global interactions within medical images. Additionally, other deep learning methods have been extended to incorporate more complex representations (Jiang et al., 2021; Zhang et al., 2023). These methods have yielded impressive results but are highly dependent on dataset size and quality.
Apart from advancements in methodologies, the availability of public databases has been vital to the development of leukaemia recognition research. There have been several benchmark databases like ALL-IDB, C-NMC, and blood cell databases on Kaggle that have facilitated replication and performance evaluation within the research (Ahmed et al., 2019; Labati et al., 2011; Gupta & Gupta, 2019). Many datasets suffer from limited sample sizes, class imbalance and a lack of multi-centre clinical diversity, which complicate fair comparisons and real-world deployment (Depto et al., 2023; Mustaqim et al., 2023). Despite a rapidly expanding body of literature, existing reviews often focus primarily on algorithmic taxonomy or performance comparisons, with limited attention to the primary datasets. Protocols related to the above-listed performance characteristics are outlined in references (Saleem et al., 2022; Shah et al., 2021; Das et al., 2022). Differentiating between methodological improvements and mere boosts to specific datasets is a difficult task.
Though computational leukaemia studies incorporate gene expression, flow cytometry, and hybrid techniques, the current paper mainly focuses on microscopy imaging techniques, as they constitute the largest body of work published to date.
Given the above findings, this review takes a data-driven approach to evaluate the methodologies used to diagnose and classify leukaemia from micrographs. This review aims to provide an objective, critical analysis of the methods used by researchers. In addition, highlighting areas of deficiency in the field that need to be addressed before successful translation to clinical practice.
Methodological Approaches for Literature Review
The current chapter explains the process used to search for and screen the literature on automated detection/classification of leukaemia in the existing body of research. To achieve this, a PRISMA 2020-compliant review protocol was used to maintain scientific rigour, replicability, and transparency throughout the process. In addition, a general application framework is provided for reference purposes.
Review Protocol and Study Design
The review of the literature meets the PRISMA criteria for systematic reviews and meta-analyses. The PRISMA standards are broadly recognised in scientific medicine and inter-disciplinary research fields to minimise selection bias and provide a framework for literature review. The PRISMA guidelines serve only as a means to report this review process; it does not form an independent review protocol. The primary objective of this review is to analyse the methodological evolution, dataset usage, and performance trends of deep learning and machine learning techniques for leukaemia detection and classification. This review discusses the automation of leukaemia detection and classification from blood smear microscopy images, providing uniformity in methodology and analysis. In this review, the term ‘detection’ refers to the differentiation between leukaemia and non-leukaemia, whereas ‘classification’ refers to the categorisation of leukaemia subtypes.
Literature Search Strategy
A thorough literature search was carried out in several scientific databases to make sure that all relevant researches have been taken into account such as ScienceDirect (Elsevier), IEEE Xplore, MDPI, SpringerLink, PubMed/MEDLINE, and Google Scholar (for extra studies). The search period was from January 2025 to March 2025.
The literature search was guided by different combinations of domain-specific and methodological keywords, including “medical image analysis”, “leukaemia detection”, “acute lymphoblastic leukaemia”, “blood cancer classification”, “machine learning”, “convolutional neural network”, “deep learning”, “transformer”, and “hybrid model”. A representative search string used in PubMed is as follows:
(“leukaemia detection” OR “blood cancer classification” OR “acute lymphoblastic leukaemia”) AND (“microscopic images” OR “blood smear”) AND (“machine learning” OR “deep learning” OR “CNN” OR “transformer”).
The search queries were designed for each database with consistent use of core keywords related to leukaemia detection, blood smear visualisation, machine learning, deep learning, CNNs, and transformers. The use of Boolean operators, ‘AND’ and ‘OR’, was utilized to make the search more accurate.
Only peer-reviewed journal articles and quality conference papers published between 2010 and 2025 were considered.
Inclusion and Exclusion Criteria
Before the process of article screening, it is essential to define appropriate inclusion and exclusion criteria for consistency and validity of results.
Inclusion Criteria
Research studies concerning the diagnosis or categorisation of leukaemia.
Use of machine learning, deep learning, or both methodologies.
The relevance of algorithms to publicly or clinically databases.
The availability of quantitative performance indicators.
The inclusion criteria involve studies devoted to the diagnosis/classification of leukaemia via microscopy.
Exclusion Criteria
Publications in languages other than English.
Review Articles, Editorials, and Opinion papers.
Research without experimental confirmation.
Studies directed towards non-haematological malignancies.
Study Quality Assessment and Risk of Bias
Improvements in the reliability of the methodology used included the qualitative analysis of studies in terms of data set transparency, methodology of the evaluation process, reporting adequacy, and quantified performance measures. In cases where methodological information was inadequate or the methodology was not replicable, studies were omitted from the full-text analysis. Various possible sources of biases, such as class imbalance and non-standardised train-test splits, were taken into account.
Study Selection Process (PRISMA Flow)
The selection of studies comprised of four steps
A total of 247 records were initially identified across all databases. After removing duplicates (n = 49), 198 records remained for screening.
During title and abstract screening, 132 studies were excluded for being outside the scope. The remaining 56 studies were assessed for full-text eligibility.
After full text screening, 13 articles were found not suitable for inclusion because of inadequate information on methodology or lack of evaluation metrics related to the study. A total of 43 articles was considered for qualitative and comparative analysis.
Articles with review papers, mutation prediction, flow cytometry, whole slide histopathology, and non-microscopy methods were excluded from the primary analysis of methodology.
The final analytical subset, therefore, consisted only of microscopy-based studies with clearly reported experimental methodologies and quantitative evaluation metrics.
The review and selection process was done independently by two reviewers, and any issues that arose were resolved through discussion and consensus. The overall study selection process is illustrated in Figure 1.
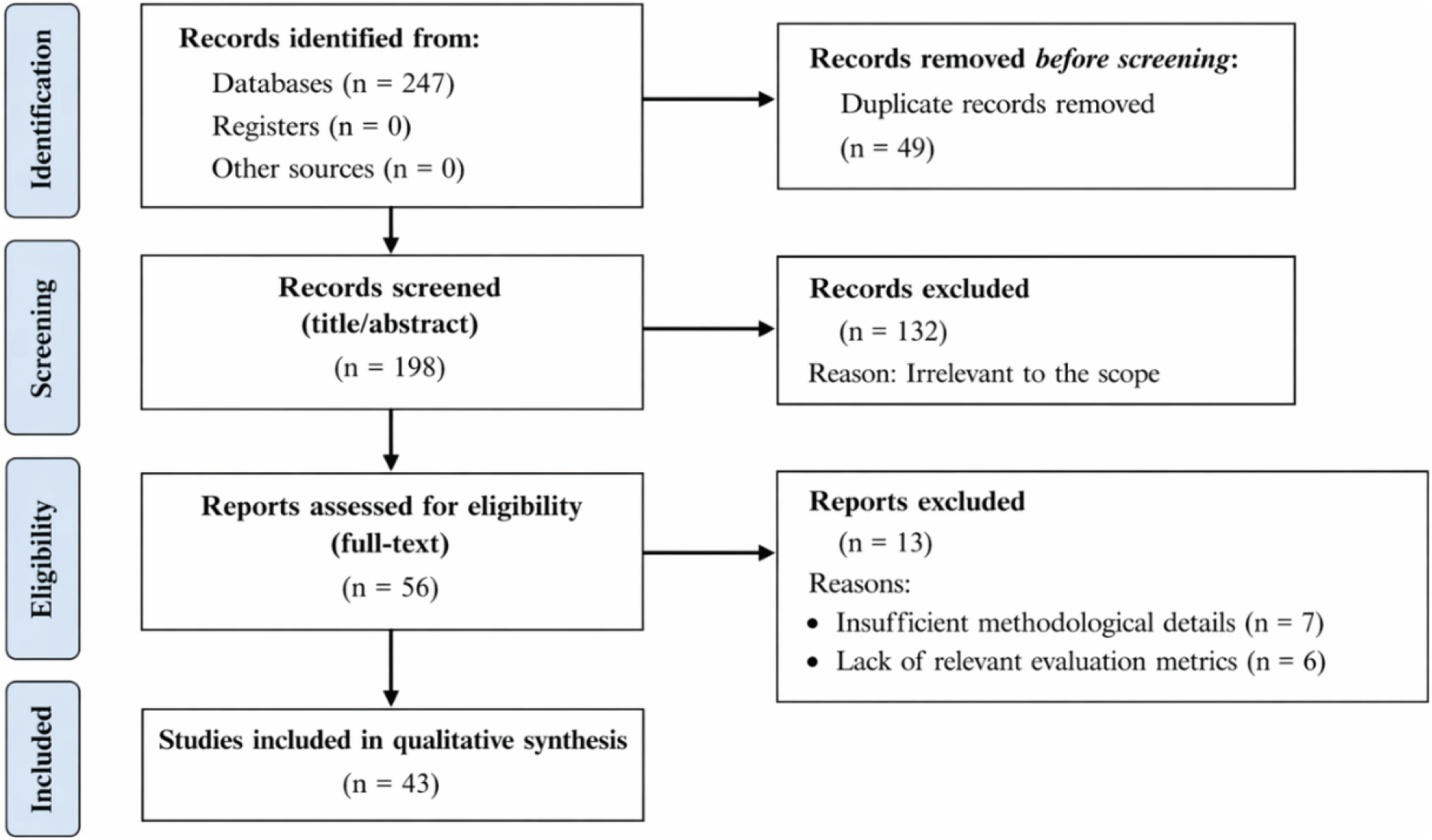
PRISMA 2020- compliant methodology flow diagram representing the study selection procedure for the literature review.
For each selected study, the following information was systematically extracted: the type of leukaemia addressed (ALL, AML, CML, CLL, or mixed), dataset used and its characteristics, methodological approach (handcrafted, CNN, hybrid, Transformer-based), feature extraction and selection techniques, classifier architecture and then reported performance metrics.
The research in this review is descriptive and comparative, but not inferential, due to differences in datasets, preprocessing steps, assessment procedures, and class imbalance.
The selected data are used to create the tables in Chapter 3 (Table 1 – Dataset Summary; Table 2 – Methodology-Accuracy Comparison).
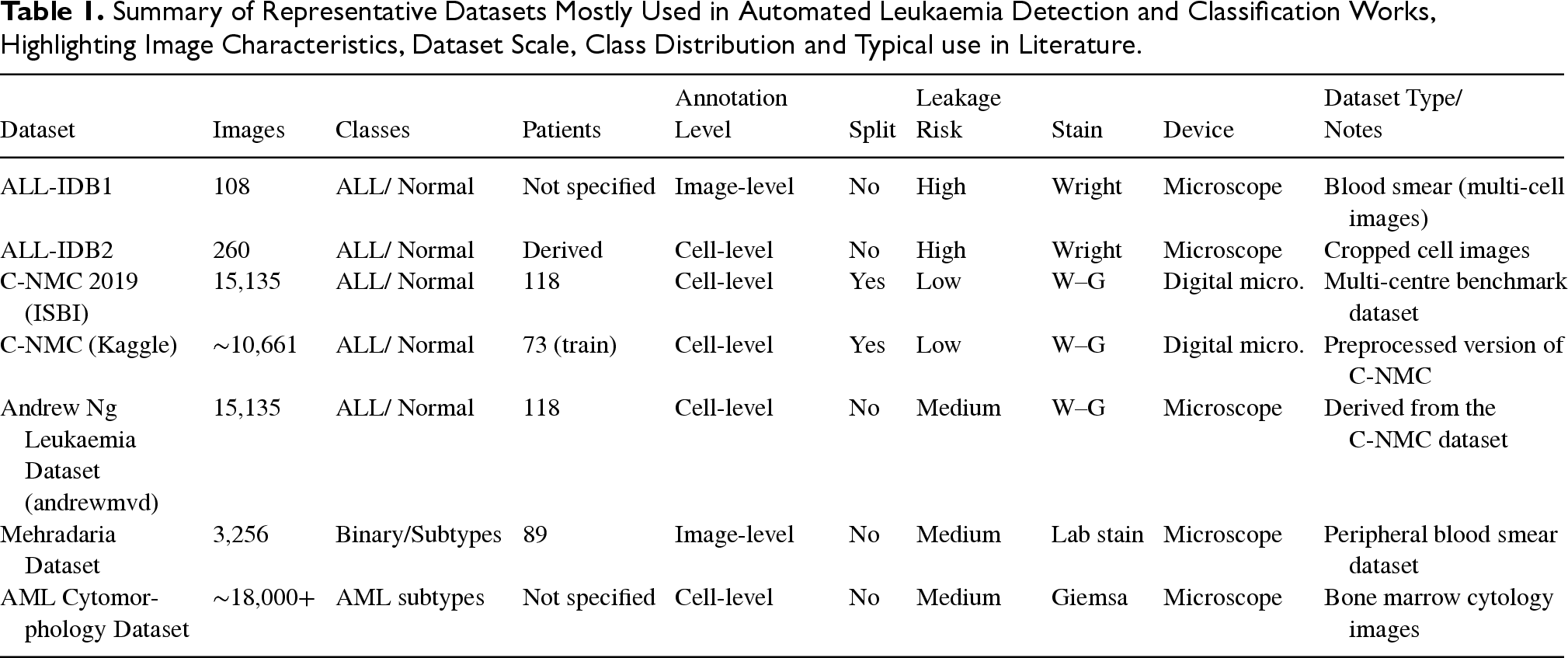
Summary of Representative Datasets Mostly Used in Automated Leukaemia Detection and Classification Works, Highlighting Image Characteristics, Dataset Scale, Class Distribution and Typical use in Literature.
Summary of Representative Datasets Mostly Used in Automated Leukaemia Detection and Classification Works, Highlighting Image Characteristics, Dataset Scale, Class Distribution and Typical use in Literature.
Comparison of Research Articles on Leukaemia Detection and Classification Using Microscopes, Including Methodology Types and Performance Metrics Used.
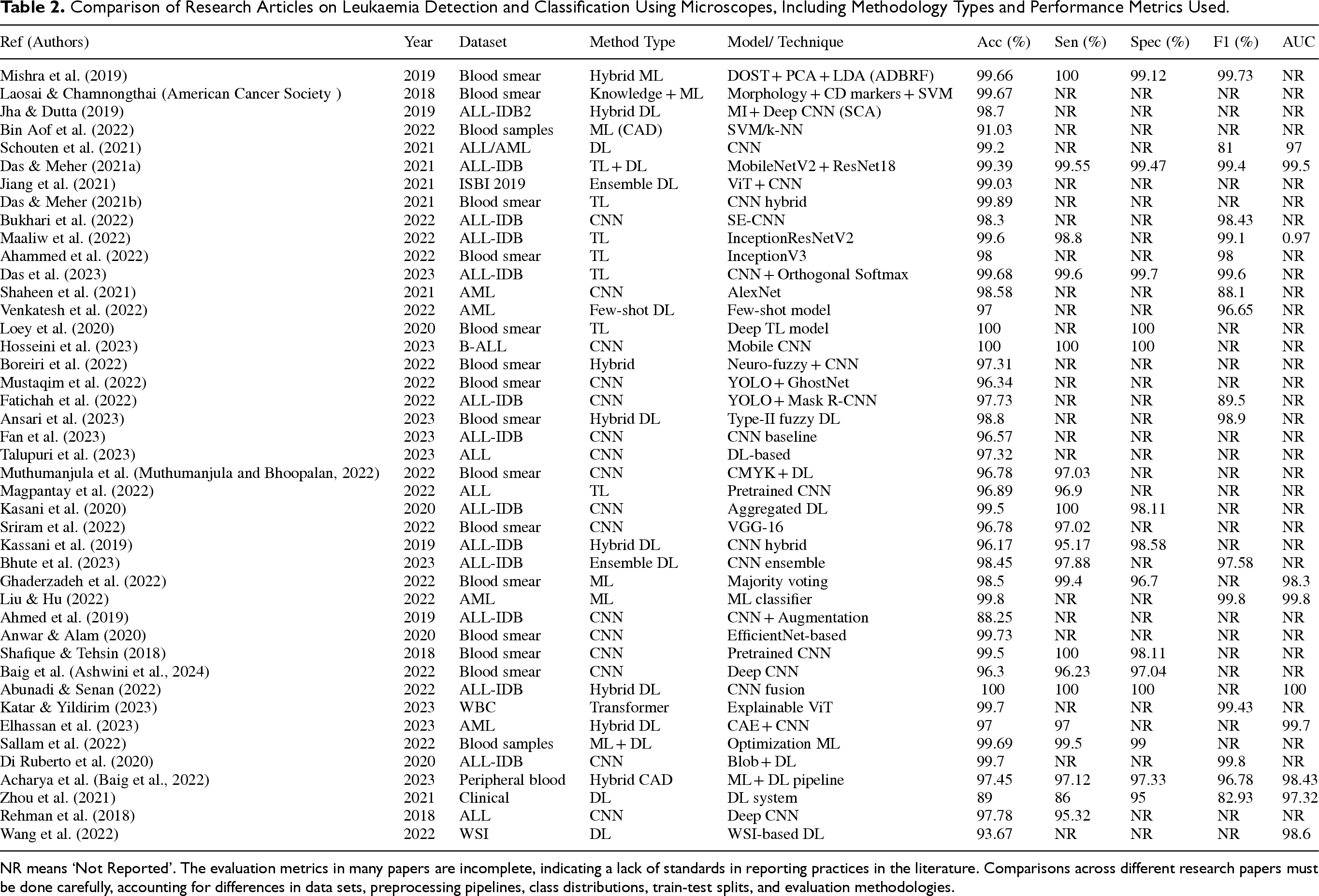
NR means ‘Not Reported’. The evaluation metrics in many papers are incomplete, indicating a lack of standards in reporting practices in the literature. Comparisons across different research papers must be done carefully, accounting for differences in data sets, preprocessing pipelines, class distributions, train-test splits, and evaluation methodologies.
The approach used in the review is mainly descriptive and comparative. The attributes obtained from the studies, including the type of datasets, methodological techniques, and performance measures, were then classified and examined for any patterns.
The studies were classified according to the datasets used (e.g., ALL-IDB, C-NMC) and whether they used handcrafted methods, CNNs, hybrid methods or Transformers. Comparative analyses were done to compare the performance.
In order to ensure unbiased results, studies that utilised the same data set were placed into context, and differences in the assessment methodology (such as lack of uniform training and testing data sets) were taken into account while interpreting the results. The accuracy, precision, recall, and F1 score measures were presented using minimum and maximum values, as well as representative values.
Statistical hypothesis testing was not used because the data, processing techniques, and evaluation methods used by the reviewed papers vary considerably. The goal here is to detect recurrent trends rather than conducting statistical analyses.
Apart from the accuracy measure, other measures were evaluated to ensure a fair assessment of model performance. Some of these measures include sensitivity (recall), specificity, precision, F1-score, and Area Under the Receiver Operating Characteristic Curve (ROC). Furthermore, where applicable, information on the validation method used, such as cross-validation and the holdout method, was analysed. This allows for a more holistic evaluation of the models’ performance using multiple metrics.
General Application Framework for Leukaemia Detection
To summarise the methodological patterns observed across the reviewed studies, Figure 2 presents a generalised workflow representing the commonly adopted stages in microscopy-based leukaemia detection systems.
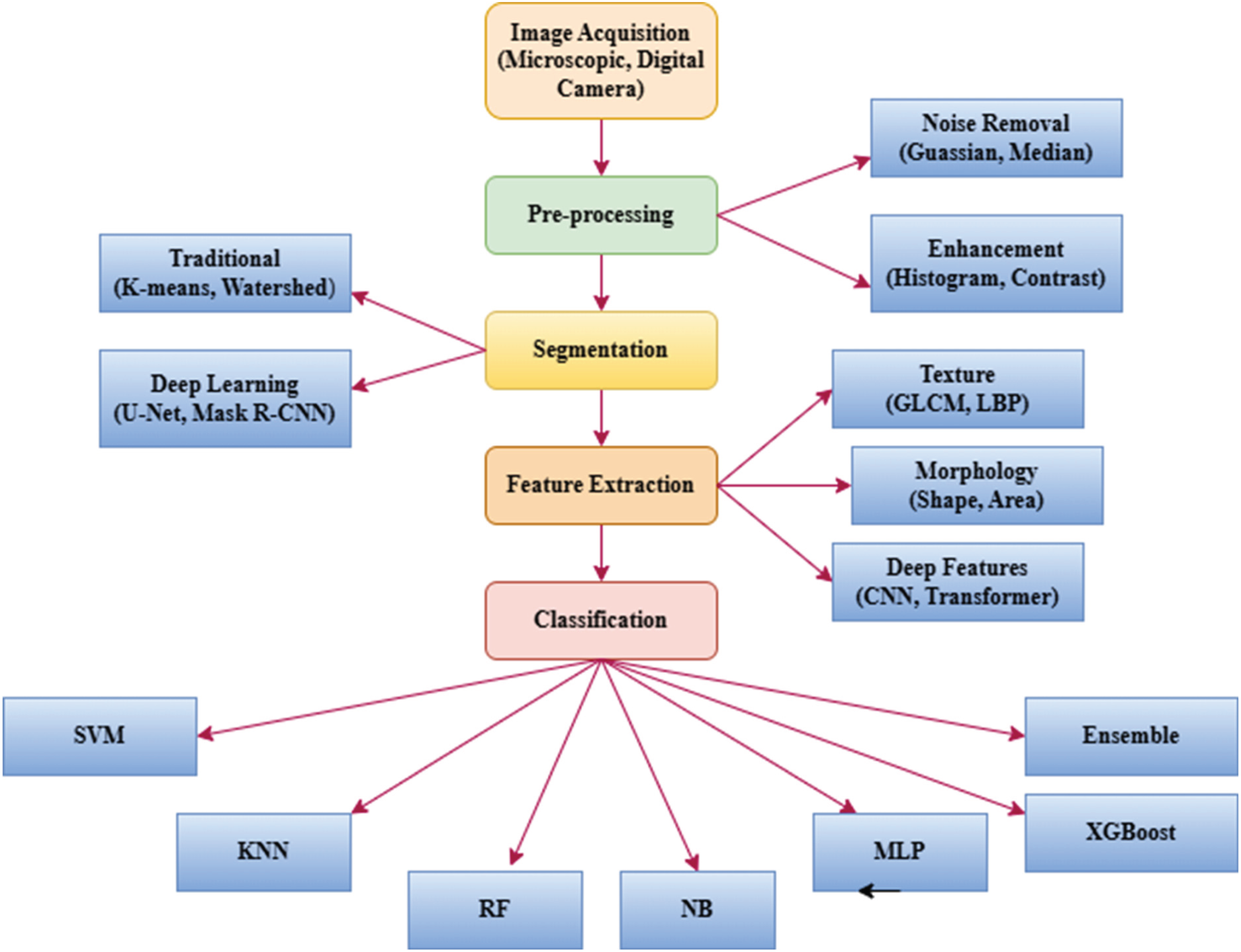
Generalised methodological workflow derived from commonly reported pipelines in microscopy-based leukaemia detection studies.
The framework usually consists of the following stages:
Peripheral blood microscopic smear images are obtained from open sources or from hospitals.
Data is preprocessed using steps such as noise reduction, colour normalisation, resizing and data augmentation.
Methods of feature extraction include: Handcrafted features: texture, shape and statistical features, deep features: features extracted using CNN, contextual features: features extracted using transformer/attention mechanism.
Hybrid methods include a fusion of handcrafted and deep features, generally integrated with either feature selection or dimensionality reduction.
Classification is done using machine learning or deep learning methods.
The decision support result includes either a leukaemia diagnosis, sub-classification, or severity evaluation.
The figure is intended to synthesise recurring methodological structures reported in the literature rather than propose a novel processing framework.
In conclusion, this chapter has presented a detailed and systematic PRISMA 2020-compliant methodology for reviewing the literature on leukaemia detection. The process of identifying and selecting appropriate literature ensured replicability and transparency in the selection process. In addition, the study proposes a generalisable framework of application that would allow for the synthesis of the various methodologies identified in the literature. This provides a coherent foundation for the comparative analysis introduced in the
Comparative Analysis of Literature Review
Overview of Leukaemia Detection Approaches
Automated leukaemia detection has evolved significantly over the past two decades, driven by advances in digital microscopy, medical image processing, and machine learning. As a result, time can be saved when executing on any dataset. Also, early computational systems relied mainly on handcrafted features extracted from peripheral blood smear images, followed by conventional classifiers such as k-nearest neighbours (KNN), support vector machines (SVM), and decision trees. These approaches focused on modelling morphological and textural characteristics of leukocytes, including nuclear shape, chromatin distribution, and cytoplasmic texture (Mishra et al., 2019; Ahmed et al., 2023).
The introduction of deep learning has led to the popularity of CNN models for automatic feature extraction from input images and enhanced leukaemia type classification. This has been explained in various studies such as (Abhishek, Santhanam, et al., 2022; Depto et al., 2023). In recent times, several frameworks have emerged that combine handcrafted features with deep learned features to leverage complementary data and increase robustness across varied data samples. This is illustrated in (Ahmed et al., 2023; Lakshmi Narayanan et al., 2025; Xu et al., 2024). Following this, the incorporation of transformer models and attention mechanisms comes next. Further extend this evolution by modelling long-range dependencies and contextual relationships within cellular structures (Lian et al., 2024).
This chapter systematically reviews and compares these methodological categories, emphasising their performance trends, dataset usage, and other difficulties faced.
Handcrafted Feature-Based Methods
Most early leukaemia detection systems relied heavily on handcrafted features derived from domain knowledge in haematopathology. Texture descriptors such as Grey Level Co-occurrence Matrix (GLCM), Local Binary Patterns (LBP), and Gabor filters were widely used to capture chromatin irregularities and cytoplasmic granularity (Mishra et al., 2019). CNN Morphological features, including nucleus area, perimeter, eccentricity, and roundness, were also shown to be effective indicators of leukemic abnormalities (Ahmed et al., 2023).
Various classifier structures like SVM, KNN, PNN, and NB have been extensively applied due to their interpretability. Some works also considered the majority voting approach, neuro-fuzzy techniques, explainable models, and morphology-based techniques for classifying microscopic blood smears (Bhute et al., 2023; Ghaderzadeh et al., 2022; Ding et al., 2023; Medical News Today, 2024). Furthermore, they gave satisfactory performance on small and controlled data sets such as ALL-IDB and ALL-IDB2. But their generalisation ability has been inadequate while handling huge and dispersed data sets (Abhishek et al., 2025). Though they perform poorly in terms of accuracy, they still have practical utility in resource-scarce settings where they can be utilised as supplementary components within hybrid systems, unlike modern deep learning techniques and handcrafted feature extraction methods.
CNN-Based Deep Learning Models
The advent of CNNs was a significant milestone for computerised leukaemia diagnosis, as the CNN prototype did not require manual feature extraction but learned a hierarchical representation directly from images. The CNN architectures VGG, ResNet, DenseNet, and Inception, amongst others, have been extensively used for either transfer learning or the design of task-specific models, as detailed in (Abhishek et al., 2022; Ahmed et al., 2019; Depto et al., 2023).
Several research works have achieved classification accuracies over 90% on standardised datasets for binary leukaemia detection (Das and Meher, 2021b; Bukhari et al., 2022; Maaliw et al. 2022, Das et al., 2023; Fatichah et al., 2022; Magpantay et al., 2022; Kasani et al., 2020; Anwar and Alam, 2020; Shafique and Tehsin, 2018). CNNs have further been generalised to classify multiple subtypes of leukaemia, with accuracy decreasing as the classes become increasingly unbalanced or similar (Sriram et al., 2022; Aziz et al., 2020; Islam et al., 2024).
Visualisation methods such as Grad-CAM have been widely applied to improve interpretability and clinical confidence in deep learning systems based on CNNs.
Hybrid Feature Learning Frameworks
Hybrid systems try to fuse both the discriminative capability of deep representations with the descriptive capability of handcrafted features. The convolutional neural network (CNN) embedding is concatenated with either texture-based or shape-based features, and then feature selection or feature extraction techniques such as principal component analysis (PCA), ReliefF, or genetic algorithms (Ahmed et al., 2023; Lakshmi Narayanan et al., 2025) are applied. With this approach, only the significant and non-redundant features are selected, as demonstrated in the literature, which shows that hybrid systems are better than individual-feature-based systems (Islam et al., 2024). Specifically, on the problem of classification on heterogeneous data sets and multi-classification of subtypes, hybrid systems exhibit increased robustness through reduced overfitting.
Moreover, hybrid models are particularly useful in clinical applications where the dataset is small or the classes are highly unbalanced. Other research efforts in recent times have focused on combining CAD techniques, digital image processing methods, and machine learning techniques guided by features in order to enhance robustness in leukemic diagnosis systems (Acharya et al., 2023; Dharani and Hariprasath, 2018; Jha et al., 2020).
Transformer and Attention-Based Approaches
Due to their impressive performance in natural language processing tasks, vision transformers have been introduced in the field of medical image processing. ViTs and hybrid CNN-T forms utilise self-attention capabilities to capture spatial dependencies in blood smear images.
The Leukaemia Detection Models based on the Transformer architecture exhibit higher sensitivity to context and understanding of cell morphology in more challenging scenarios that involve multiple cells and their interactions (Zhang et al., 2023; Lian et al., 2024; Elhassan et al., 2024; Rai et al., 2024; Talaat and Gamel, 2024). The attention mechanisms also enhance interpretability by highlighting diagnostically relevant regions, aligning well with explainable AI requirements (Salih et al., 2025).
Although computationally more demanding, Transformer-based frameworks represent a promising direction for future large-scale and multi-centre leukaemia studies.
Dataset Landscape and Benchmarking
The key characteristics of the most widely used datasets for automated leukaemia detection and classification are summarised in Table 1. The above comparison shows that there are differences in image resolutions, the number of images in the dataset, class distribution, and their use. Some benchmark datasets used publicly include ALL-IDB and ALL-IDB2. Conversely, bigger datasets, including C-NMC Leukaemia and Kaggle datasets, are becoming popular for deep learning models and mixed approaches due to higher variability and number of samples (Labati et al., 2011; Gupta and Gupta, 2019; Anilkumar et al., 2021; Kebaili et al., 2023; Ratley et al., 2020). Several recent studies using C-NMC and Kaggle-derived datasets have demonstrated the increasing use of transfer learning, lightweight CNNs, and augmentation-based frameworks for improving classification robustness (Muthumanjula and Bhoopalan, 2022; Ul Ain et al., 2022; Elhassan et al., 2022; Ansari et al. 2023, Tran et al., 2018; Rezayi et al., 2021).
The datasets used in the reviewed studies exhibit variability in annotation granularity, patient-level representation, and data splitting strategies. While datasets such as C-NMC provide patient-wise splits and multi-centre data, earlier datasets such as ALL-IDB lack standardised partitions, increasing the risk of data leakage and overestimated performance. Derived and pre-processed datasets (e.g., Kaggle versions) introduce additional inconsistencies, underscoring the need for standardised benchmarking practices.
The proportional distribution of dataset usage across the reviewed literature is presented in Figure 3, and the analysis indicates that ALL-IDB and ALL-IDB2 datasets dominate early- and mid-stage studies. In contrast, recent deep learning-based work increasingly employs larger datasets, such as the C-NMC Leukaemia dataset, ISBI/other public datasets and Kaggle collections, to improve model generalisation.
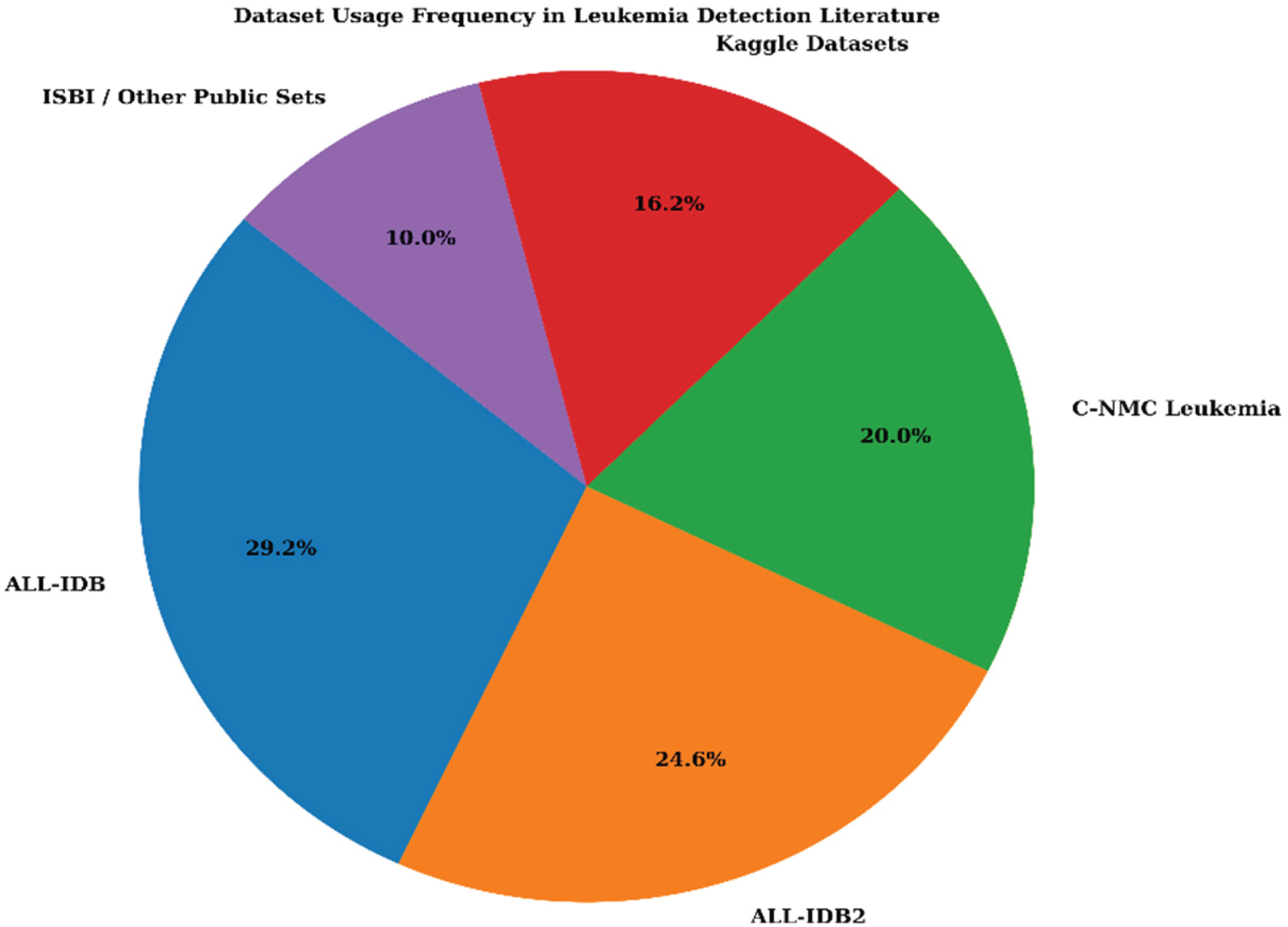
Dataset usage distribution across leukaemia detection studies reviewed, showing the relative dominance of ALL-IDB2, mainly ALL-IDB variants and the growing assumption of wide-reaching datasets.
Analysis of performance metrics for the described automated systems for leukaemia detection shows clear patterns linked to changes in the applied methodology. Overall, handcrafted feature-based algorithms achieve decent classification results, but those based on CNNs and hybrid algorithms deliver significantly better performance, especially with large datasets. The more recent methods based on Transformers and attention mechanisms also help improve discrimination by leveraging long-range dependencies in leukocyte images (Lian et al., 2024; Abhishek et al., 2025).
The structured comparison of representative studies published between 2018 and 2025 was analysed according to their methodological category, dataset usage, and reported accuracy. The findings are summarised using tabular and graphical representations, and Table 2 presents a comparative summary of 52 representative leukaemia detection studies, mapping each work to its employed methodology, dataset, and reported classification accuracy. The table also highlights the gradual shift from handcrafted feature-based pipelines toward deep learning, hybrid, and Transformer-enhanced architectures. There are various studies utilising CNNs and hybrid feature fusion that consistently report higher accuracy than traditional approaches, particularly when evaluated on larger datasets such as C-NMC Leukaemia and Kaggle collections (Lakshmi Narayanan et al., 2025; Islam et al., 2024; Rezayi et al., 2021).
Some papers may mention more than one experiment setup or dataset version; hence, there will be variation in the evaluation setup described in each related paper.
Table 2 presents the representative papers from the final analytical set, aiming to highlight the variety of methodologies and reporting evaluations used rather than provide an exhaustive listing of all included studies.
A comparative analysis of representative studies on automated leukaemia diagnosis using various datasets and techniques is presented in Table 2. The findings show an observable trend toward the use of more sophisticated approaches to solve the problem, with more recent techniques offering superior performance. Although most studies claim to have produced highly accurate models (in some cases, over 95% accuracy), further analysis using parameters such as sensitivity, specificity, F1-score, and AUC shows that there is still room for improvement.
It is also observed that ensemble approaches usually yield better, more consistent results than individual approaches. Nevertheless, the lack of consistency in the metrics used makes comparing results across studies difficult. All in all, the results highlight the importance of using multiple metrics to evaluate the efficacy of leukaemia diagnosis systems.
Comparing performances across studies remains difficult, as the proposed methodologies have been tested on diverse datasets with different class distributions, image resolutions, labelling schemes, and testing procedures. Thus, the presented results should be considered more as trends in the literature than actual benchmarking results.
The results presented in Table 3 can serve as a representative comparison of trends found in the literature, but not necessarily as proof that high accuracy levels represent good model performance.
Representative Performance Ranges are Reported Across Methodological Categories in the Reviewed Literature.
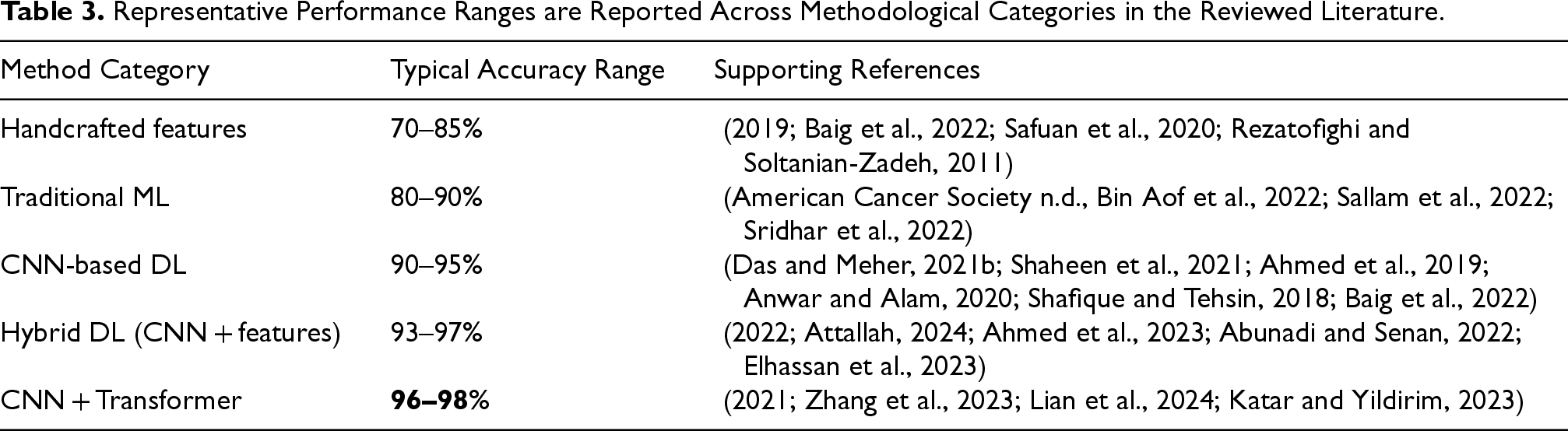
Representative Performance Ranges are Reported Across Methodological Categories in the Reviewed Literature.
Upon further scrutiny, the progression of performance for automated leukemic detection was evaluated, and typical accuracy values for these studies were determined and plotted to establish trends over time and across methodologies. As the values are derived from disparate sources, the purpose is not to benchmark one method against another but to display general trends, as indicated by Figure 4.
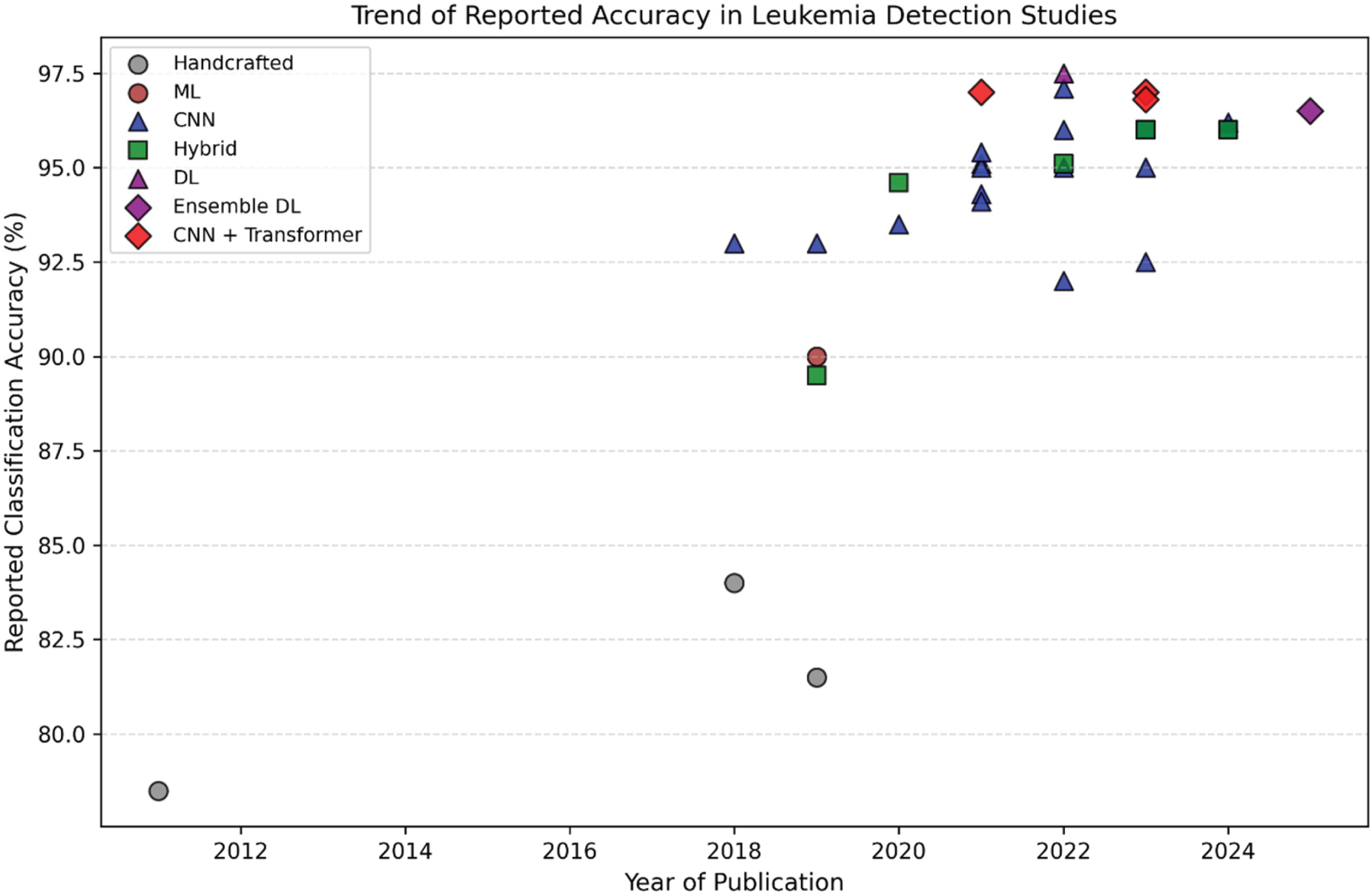
Temporal review of the mentioned performance metrics reported in selected studies on leukaemia classification based on various methodologies.
While accuracy remains the most common metric in such research, sensitivity, specificity, F1-score, and AUC have become increasingly popular for better understanding of results in imbalanced datasets.
To offer a comprehensive perspective on performance trends in the literature reviewed, an analytical visualisation framework was developed. While the dashboard in Figure 5 aims to provide a comprehensive perspective on performance trends across the literature reviewed, it does not focus on accuracy values. Instead, the dashboard aims to provide a comprehensive perspective on performance trends in the literature reviewed.
“Analytical visualisations are indicative of literature-driven trends and not representative of normalised similarity across various experiments.”
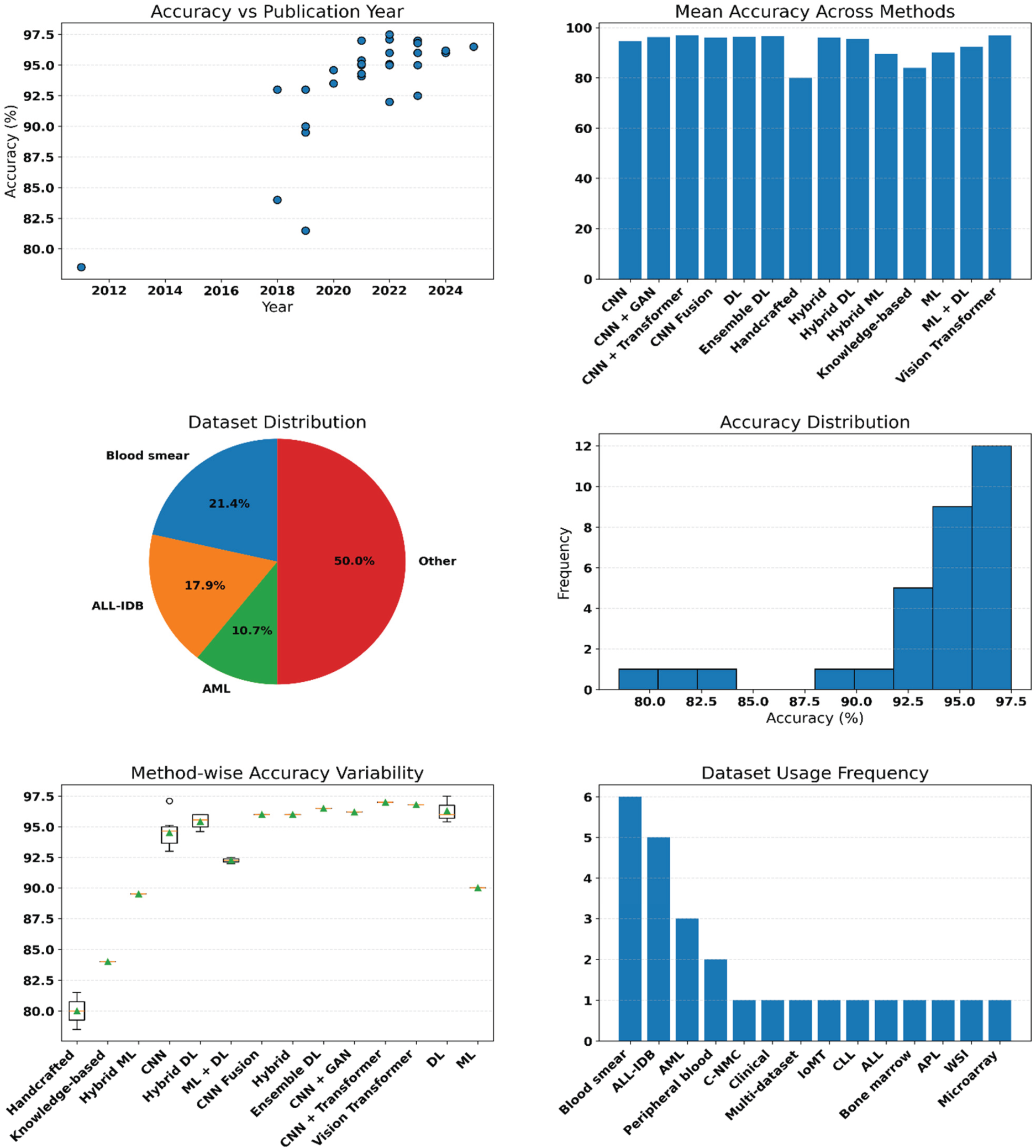
Analysis of performance measures in the reports on studies for detecting leukaemia. This diagram illustrates trends in accuracy over time, average performance by methodology category, data set distribution, accuracy distribution, methodology diversity, and data set utilisation. These visualisations show literature trends rather than experimental comparisons.
There are several notable observations from Figure 5: first, temporal variations in the accuracy distribution indicate increasing accuracy, implying maturity in the methodologies used; second, the accuracy distribution highlights the performance-saturation characteristics of benchmarks. Thirdly, the variability of methodology shows reduced variation in both hybrid and Transformer methodologies. Fourthly, there is a notable dominance of a few benchmarking datasets in the datasets utilisation charts.
There was a clear increase in automated leukaemia detection accuracy in Section 3.7, driven by hybrid models and CNN-Transformers. The improvements made should not be blindly accepted, as there is significant variance in performance across different method categories. Based on the graphs depicting trends in accuracy and the box plots, several open issues need to be addressed to improve the robustness and generalisation of the proposed solutions. This section critically examines the key open challenges, limitations, and research gaps identified from the reviewed literature.
Dataset-Related Challenges
While the prevalence of deep learning approaches continues to grow, data constraints remain a major limitation in the development of automated leukaemia detection algorithms. A relatively large number of works still use small benchmark datasets like ALL-IDB, among others, and the images contained within them do not contain enough diversity in terms of stain conditions, imaging devices, and patients’ characteristics. This over-reliance contributes to optimistic performance estimates that may not generalise to real-world clinical settings.
The problem of class imbalance is also a concern in the classification of multi-subtype leukaemia, where the rare subtypes are naturally underrepresented. The data augmentation and synthetic sampling methods, which are commonly used to counter this problem, may introduce distributional bias and cannot serve as a complete substitute for the clinically representative data.
Methodological Limitations
Improvements in CNN, Hybrid, and Transformer architectures have brought significant gains in feature extraction capacity. Nevertheless, it is evident from the overlapping distributions of accuracy values in the box plots for each model in Figure 5 that further improvements in performance come at a lower rate of return. This also indicates that the improvements may be increasingly constrained by dataset characteristics and data quality rather than by the model design. Moreover, many studies lack comprehensive ablation studies to support design choices and feature fusion strategies, and hyperparameter sensitivity and overfitting are important concerns, especially when complex models are trained on small datasets. These concerns indicate the need for more systematic experimentation, rigorous validation, and reporting practices.
Evaluation and Benchmarking Issues
Standardisation in evaluation protocols is another shortcoming in the current literature. The use of randomised train-test data splits and the lack of validation on external data can lead to bias in results and performance overfitting of models, since there is no validation on external data. There is a problem of over-reliance on accuracy as the main metric for evaluation, regardless of class imbalances, despite having other metrics like precision, recall, F1-score, and ROC–AUC that provide a more comprehensive assessment. Recent studies have increasingly incorporated ensemble learning, transfer learning, and subtype-specific classification frameworks to improve robustness and multi-metric evaluation performance (Rajpurohit et al., 2018; Karar et al., 2022; Abhishek et al., 2022; Liu and Hu, 2022).
The lack of standardised benchmarks and common assessment frameworks makes it difficult to make fair comparisons across studies. As seen from the variation in accuracy values reported across similar methodological groups, preprocessing pipelines, and validation approaches. Differences in these factors play a pivotal role in determining performance results.
Explainability and Clinical Trust
Although explainable AI approaches, such as Grad-CAM and attention maps, have been used in recent research, their use is rather limited, as the visualisations produced were purely qualitative and not rigorously validated by domain experts. From a clinical point of view, however, it must be noted that such visualisation techniques might not necessarily help in gaining the required amount of trust, especially when considering that most works did not take into account haematologist-in-the-loop assessment and user-centred validation, which are absolutely necessary for practical applications.
Computational and Deployment Constraints
The growing adoption of Transformer-based and ensemble approaches creates further challenges in terms of computing resources and requires considerable training capacity. The models may have longer inference times, thus limiting their suitability for implementation in low-resource clinical environments. Real-time application of edge computing and diagnostics remains an unexplored domain in the literature on leukaemia detection.
Additionally, most papers focus on offline evaluation, giving lower priority to aspects such as workflow integration, privacy and system-level testing. It is critical to address these deployment challenges to transition from experimental prototypes to clinically usable systems.
Summary of Challenges and Research Gaps
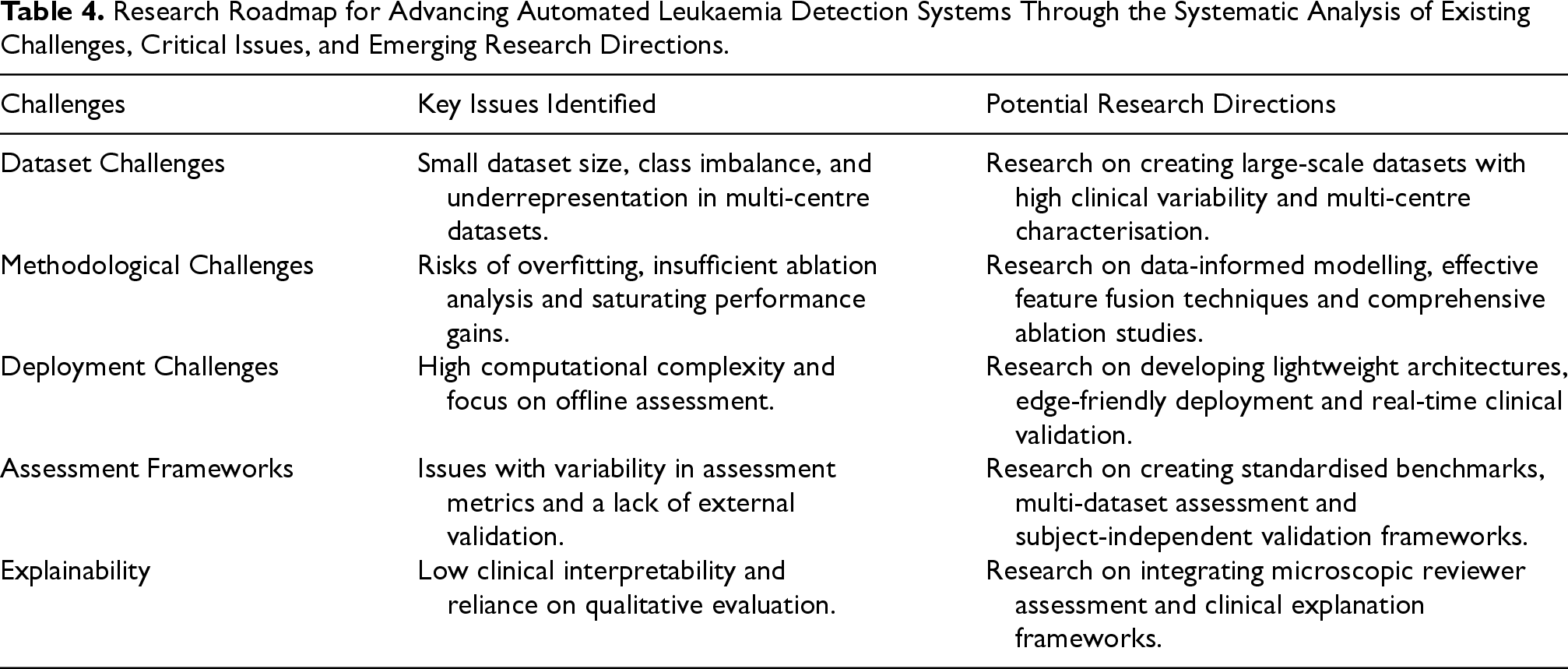
To ensure the identified limitations are consolidated, Table 4 below summarises the major. challenges identified in the literature reviewed, along with possible research directions to address them.
Research Roadmap for Advancing Automated Leukaemia Detection Systems Through the Systematic Analysis of Existing Challenges, Critical Issues, and Emerging Research Directions.
Research Roadmap for Advancing Automated Leukaemia Detection Systems Through the Systematic Analysis of Existing Challenges, Critical Issues, and Emerging Research Directions.
To overcome these obstacles, it is essential to ensure that future advances in automated leukaemia detection translate into reliable, interpretable, and clinically deployable diagnostic systems.
This review mainly focuses on the literature related to the use of microscopy-based leukaemia detection techniques and does not cover all other non-imaging approaches such as gene expression analysis, flow cytometry, or omics integrations. Although several recent studies have investigated mutation prediction, bone marrow analysis, whole-slide imaging, and flow cytometry-assisted AI systems (Rehman et al., 2018; Safuan et al., 2020; Eckardt et al., 2022; Huang et al., 2020; Ko et al., 2018; Eckardt et al., 2022; Wang et al., 2022; Kumar et al., 2020; Ouyang et al., 2021; Chandradevan et al., 2020) these modalities were outside the primary microscopy-focused analytical scope of the present review.
With regard to the problems and gaps presented in Section 4, the following section outlines promising areas for future research and a roadmap for building more accurate, operational automated leukaemia detection systems. The roadmap focuses on data-driven development, evaluation, explainability, and real-world integration, all of which are important for achieving clinical relevance through algorithmic advances.
Dataset-Centric Research Directions
The future research path must focus on creating large-scale, representative datasets that capture real-world variability in staining techniques, imaging modalities and patient populations. Multi-centre data collection and the collaborative sharing of datasets are essential for mitigating the issues associated with single-source datasets, which are currently prevalent in the literature.
Further, future datasets should enable detailed leukaemia subtype identification, longitudinal studies of disease progression, and the inclusion of paediatric and adult cases. Rather than focusing on synthetic data augmentation, there should be emphasis on balanced data collection and standardised annotation protocols validated by haematology experts.
Model Development and Learning Strategies
Although current hybrid and CNN-Transformer models are performing well, the future research agenda should move from architecture optimisation to data-efficient and generalizable learning approaches. Some of the important areas include self-supervised and weakly supervised learning, which can effectively leverage large amounts of unlabelled clinical data.
Additionally, model complexity also needs to be considered from the point of interpretability and computational efficiency. The use of lightweight models, attention-sparse transformers, and hybrid models offers promising prospects for building highly efficient models with minimal resources.
Evaluation, Benchmarking, and Reproducibility
To make effective comparisons across different research results, future work must adopt standardised evaluation approaches, such as independent split testing, cross-dataset validation, and the presentation of performance measures beyond accuracy. Moreover, effective evaluation measures, such as cross-dataset validation and the presentation of multiple performance metrics, would make the process more reliable.
Moreover, the creation of benchmark leaderboards for different types of leukaemia detection systems that have fixed training and test splits would add value to the experiments.
Explainability and Human-in-the-Loop Systems
Explainable artificial intelligence needs to go beyond post-hoc explanation visualisation and focus on clinically relevant interpretability frameworks. Future studies should incorporate explanation frameworks consistent with haematological diagnostic standards and that facilitate decision justification.
Validation by a haematologist-in-the-loop during both model development and evaluation will help to improve clinical acceptability and usability. Also, the explanation interfaces and feedback mechanisms are promising areas for closing the gap between algorithmic results and clinical reasoning.
Clinical Translation and Deployment Pathways
Concerning clinical deployment, the following considerations should be considered in future research: inference time, system hardware demands, and compatibility with current laboratory information management systems. Edge-friendly machine learning models and privacy-oriented learning paradigms like federated learning could be useful for ensuring safe clinical deployment.Prospective validation studies and pilot studies in clinical settings are necessary to assess system robustness, user acceptance, and compatibility with clinical workflows. Legal mandates and ethical issues should be addressed early in the design process to ensure readiness for a clinical translation.
Research Roadmap for Automated Leukaemia Detection
Based on these recognised weaknesses and gaps in current research, an action plan for developing an automated diagnosis of leukaemia from its infancy to a mature system is presented below.
This step involves the creation of multicenter databases that are clinically oriented, systematic, well-labelled, and balanced in their subtypes. The significance of establishing sound data foundations cannot be overstated since it forms part of the solution to the problems associated with biased datasets and generalisation of the models.
Stage two is geared towards designing highly efficient, hybrid learning models along with interpretable model architectures that are light in weight. The use of ablation studies, robustness tests, and validation is essential in making the systems stable.
Benchmarking across data sets, the use of multiple metrics for evaluation, and the implementation of explainability methods based on the evidence are emphasised at this stage. Standardised evaluation methodologies are required in order to compare performances fairly.
The last stage deals with translational issues such as edge-compatible and real-time inference algorithms, human-in-the-loop decision-making systems, future clinical validation, and regulation. All these aspects determine the viability of such implementation in reality. Together, this roadmap forms an important basis for future research that will lead to the development of clinically viable leukaemia detection systems utilising AI.
Implications for Research and Practice
Key Analytical Insights
This literature review has major implications for researchers and professionals developing AI solutions for automated leukaemia detection. The main implication of this comparison study is that the nature of the data set plays a far greater role in determining efficiency. The complexity of the model architecture serves only to reemphasise the need for a data-driven research approach to developing generalizable and reliable diagnostic systems. Moreover, the literature review points to several challenges that persist in the field, including dataset bias, inconsistent benchmarking, insufficient cross-validation, and limited clinical validation. The above constraints affect the translational validity of existing AI models. The future roadmap proposed in Section 5 requires a paradigm shift towards the development of AI models that are more clinically relevant, focusing on standardised datasets, robust benchmarking, and explainability.
Emerging Research Questions
Several research questions have not been addressed adequately based on the literature reviewed.
What are the data collection procedures, annotation standards and sources of variation in widely used benchmark datasets like ALL-IDB and C-NMC? How do dataset-specific biases affect the ability of models to generalise to unseen data?
How can performance benchmarking be standardised across diverse studies? To what extent are subject-independent, cross-dataset and external clinical evidence examined?
Which procedural modifications are needed for evolving systems that are more clinically relevant, less prone to staining variability and capable of handling greater computing loads and regulatory considerations?
How can explainable AI methods be strongly verified by haematology experts? And what are the current limitations of visualisation-based explanation methods?
Are preprocessing pipelines, dataset splits and evaluation protocols correctly documented to enable replicable research?
Broader Research Impact
These considerations point to a broader trend in the field, shifting from performance improvement to robustness, interpretability and clinical relevance. Also, these research questions must be addressed to ensure that future AI-based leukaemia detection systems have a positive clinical impact.
Conclusion
This review offered a systematic, dataset-focused and analytical review of automated leukaemia detection methods, critically assessing the transition from handcrafted feature-based methods to modern CNN, hybrid, and Transformer models. Through comparative visualisation and descriptive analysis, it showed that the dataset's characteristics drive performance improvements, the evaluation method, and validation practices rather than solely by the model's complexity.
The results of the analytical review show a progressive convergence of studies toward higher accuracy, with decreasing variability in recent years for hybrid and Transformer models; however, the overlapping performance distributions and dataset usage patterns also indicate that there are still challenges related to dataset bias, inconsistent benchmarking, a lack of external validation, interpretability, and deployment feasibility. These challenges collectively point to the performance gap between experimental results and a clinically viable diagnostic system.
Controlling these challenges will require a paradigm shift in research focus from performance optimisation to data-driven research, standardised evaluation, clinically grounded interpretability, and real-world validation studies. The systematic research roadmap outlined in this review offers a helpful guide for future research aimed at developing robust, reliable and clinically feasible AI-assisted leukaemia detection systems.
The results of this review collectively point to a paradigm shift in the field, one that emphasises robustness, interpretability, and clinical applicability over performance optimisation, and this shift is necessary to ensure that future progress leads to clinical impact.
Footnotes
Ethical Approval
The authors do not require any ethical approval.
Authors’ Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Code Availability
The code will be made available on request.
Data Availability
Data will be made available on request.