
Abstract
Background
Osteoporosis and major osteoporotic fracture are more common in PD than controls, but evaluation of sociodemographic factors and preventive treatment is limited.
Methods
In a UK population-based nested case-control study, incidence rates of osteoporosis and major osteoporotic fracture were calculated, and risk factors and bone health treatments analyzed by multivariable regression.
Results
Falls, osteoporosis and major osteoporotic fracture were more likely before a diagnosis of PD compared to controls (P < 0.0001). After diagnosis, incident osteoporosis, HR 1.96 (1.90, 2.02) and incident fractures, HR 2.16 (2.11, 2.21) were more likely in PD than controls, both P < 0.005. Risks of fracture were increased in PD cases during 3 consecutive time periods post-diagnosis: 0–7 years, HR 2.15 (2.09, 2.21), 7–14 years, HR 2.36 (2.24, 2.48), and 14–21 years, HR 1.88 (1.62, 2.17), all P < 0.0001. Risks of osteoporosis and fracture increased with older age, female sex, greater deprivation and White ethnicity. In PD, anti-osteoporosis treatment was underutilized in men, OR 0.25 (0.24, 0.26) versus women, being lower than the relative risks of osteoporosis in men, HR 0.35 (0.32, 0.37) and fracture in men, HR 0.60 (0.57, 0.63). There was also underutilization of anti-osteoporosis treatment in the most deprived quintile, HR 0.85 (0.80, 0.90), despite significantly higher rates of osteoporosis, HR 1.14 (1.01, 1.28) and fracture, HR 1.17 (1.06, 1.30).
Conclusion
The increased bone health risks at all stages including the prodrome, and across multiple risk categories, emphasizes the need for early bone health assessment and increased anti-osteoporosis treatment rates.
Plain language summary
People with Parkinson's are more likely to experience falls, bone thinning (osteoporosis) and fractures (broken bones). Treatment is important to strengthen bones and reduce the number of fractures, but not all individuals who could benefit from bone treatment are prescribed it. We looked at how many people with Parkinson's have thin bones and fractures, how many had a scan to measure their bone thickness, and how many were prescribed treatment to help prevent fractures. We compared our findings between people with and without Parkinson's. Our study showed that people with Parkinson's are more likely to fall, have thin bones, experience fractures and undergo bone scanning before they are diagnosed with Parkinson's, compared to people without the condition. The risk of bone thinning and fracture was also greater after a diagnosis of Parkinson's compared to those without it. The hip was the most commonly broken bone. Bone thinning and fracture were more likely to occur in older people, women, more deprived areas and in those of White ethnicity. However, the effects of Parkinson's on bone health were still present in people with ‘lower risk’, meaning that everyone with Parkinson's should have a bone health assessment. As falls, bone thinning and fracture occur from the earliest stages of Parkinson's, it is important that bone health is assessed early, and that investigations and treatment are used when needed to help reduce the number of bone fractures.
Background
People with Parkinson's disease (PD) are twice as likely to develop osteoporosis 1 and major osteoporotic fracture1–3 compared to controls. The increased risk of osteoporosis in PD is multifactorial, due to reduced mobility and exercise, low body mass index (BMI), malnutrition, vitamin D deficiency and medication effects, including levodopa-related hyperhomocysteinaemia.1,4,5 Although women have a higher absolute risk of osteoporosis and osteoporotic fracture than men, the higher male PD prevalence results in almost as many hip fractures in male as female PD patients. 6 Treatments such as bisphosphonates increase bone density, reduce fracture risk and are cost-effective. 7 However, osteoporosis assessment and treatment are often suboptimal, particularly in the elderly and in men. 8
In a national audit of Parkinson's care, bone health assessment 9 significantly improved from around 40% of cases in 2019 to 60% in 2022, following the implementation of a bone health assessment and treatment algorithm 6 into routine Parkinson's clinical care. Despite this, bone health management remains heterogenous and lacks PD-specific advice, with treatments largely based on studies in the general population.10,11 The current work aimed to analyze bone health management in a larger population, using diagnostic, imaging and medication data from the Clinical Practice Research Datalink (CPRD). Comprising 69 million cases over 38 years,12,13 CPRD is one of the largest longitudinal primary care databases worldwide, is broadly representative of the UK population and has high diagnostic validity for Parkinson's, 14 hip and vertebral fractures. 15
With an ageing population, accurate incidence estimates of osteoporosis and fracture in PD are needed for healthcare planning. However, there is substantial heterogeneity in their incidence globally, with rates varying by ethnicity,16–18 socioeconomic status16,17,19–22 and rurality,23,24 and PD itself is associated with these factors. Although prior CPRD studies have defined factors associated with fragility fractures in conditions such as asthma, 25 their impact on bone health in PD is not well studied. We aimed to define the incidence of osteoporosis, major osteoporotic fracture and bone densitometry scanning (DXA), and to quantify anti-osteoporosis therapy use in incident PD. Additionally, we assessed the impact of sociodemographic factors on bone health in PD, and survival after fracture comparing PD and controls.
Methods
This population-based nested case-control study analyzed data from the CPRD Gold 12 and Aurum 13 June 2024 datasets, which represent 27.2% of the UK population aged 20 years and older. CPRD data were enriched with linked data from the Rural-Urban Classification, Indices of Multiple Deprivation (IMD), Hospital Episodes Statistics (HES), HES Diagnostic Imaging Dataset (HES-DID) (from 01/04/2012 to 31/10/2020) and the Office of National Statistics (ONS). The protocol and data access were approved by CPRD's Research Data Governance Process, and ethical approval granted by a National Research Ethics Service Committee. Individual patient consent was not required but general practices consented to data collation, processing and linkage.
Included cases were 20 years or older at diagnosis, had acceptable data quality 26 and were registered in CPRD for at least 6 months from 2003 to 2023. Read and SNOMED diagnostic codes in CPRD, and International Classification of Diseases tenth revision (ICD-10) codes in HES, were used to identify incident PD cases as previously described, 27 and subsequent incident osteoporosis and first-ever fracture. Incident cases were matched with up to two controls, without PD or dopaminergic medication use, by age (±2 years), sex and GP practice using incidence density sampling. The index date was defined as the date of PD diagnosis, and the same date was assigned to corresponding controls. Data were separately extracted from CPRD Gold and Aurum and then combined. Deduplication of data was performed following CPRD recommendations, to adjust for GP practices migrating from CPRD Gold to Aurum, and to exclude data from merging GP practices where there was evidence of duplication.
The primary outcomes were the relative risks, expressed as hazard ratios (HR), of incident osteoporosis and incident major osteoporotic fracture in PD. Secondary outcomes were the proportion undergoing DXA scans and receiving anti-osteoporosis therapy, and survival after fracture for PD cases and controls. For the time-to-event analysis, patients with osteoporosis or fracture prior to the index date were excluded and the first observation selected for cases with more than one fracture. Fractures were excluded when pathological (in cases with cancer) or traumatic (e.g., road traffic accident) (Supplementary Figure 1). Sites of major osteoporotic fracture included the spine, hip and upper limb (shoulder and forearm), as these are defined in clinical guidelines and have recognized morbidity and mortality.28,29 Major osteoporotic fractures of unknown site were classed as ‘unspecified’. DXA scans were identified using codes in CPRD and HES-DID, and vitamin D, calcium and anti-osteoporosis therapy (bisphosphonates, denosumab, strontium, raloxifene and teriparatide) were categorised from prescription codes.
Covariates were selected using a UK guideline 30 and included: self-reported sex, age group, body mass index (BMI), smoking status, alcohol consumption (excess defined from coding or >14 units per week), type 1 and 2 diabetes mellitus, steroids, anti-osteoporosis therapy, ethnicity, rurality and, for England, socioeconomic status. For BMI, smoking and alcohol consumption, the most recent observation was selected. The first and last prescription dates were used to determine exposure duration for anti-osteoporosis therapy and steroids. For steroids, prednisolone 7.5 mg per day (equivalent for other formulations) for at least 3 months was classed as high-dose in accordance with the UK National Osteoporosis Guidelines Group recommendations. 30 A CPRD algorithm designated ethnicity from CPRD and HES records as: White, African or Caribbean, Asian, Mixed or Other, or Unknown, and the secondary care record was used if different from primary care. Socioeconomic status was determined at a patient level using the Index of Multiple Deprivation (IMD), 31 a census-derived measure covering geographical areas of around 1500 individuals. It combines seven weighted domains into a composite score to allocate cases to one of five deprivation quintiles (IMD5, least deprived, through to IMD1, most deprived). Rurality was determined at a GP level using the Rural-Urban classification. 32
Statistical analysis
Crude incidence rates were calculated as the number of new cases per 1000 person-years. Baseline characteristics were compared between PD cases and controls by conditional logistic regression, with each case and matched control analyzed as separate strata.
The probability of incident osteoporosis and major osteoporotic fracture was plotted by Kaplan-Meier cumulative hazard curves. The end date was defined as the first date of osteoporosis or fracture, or for censored cases, the earliest of their last observation, transfer out date or death date. Cox regression was performed separately for incident osteoporosis and fracture to examine their associations with pre-defined covariates: PD diagnosis, age (under 70 years and 70 years and older at the index date), sex, ethnicity, rurality and deprivation quintile. Missing data for ethnicity and IMD were designated as ‘Unknown’. The multivariable models included variables where P was <0.1 in univariable modelling, and mutually adjusted for all included covariates and for smoking, alcohol, BMI, diabetes and high-dose steroid use. For each model, interaction terms were fitted between group (PD or control) and each covariate.
Based on the hypothesis that associations with osteoporosis or fracture would be stronger in women than men, in older than younger patients, and for White ethnicity than other ethnic groups, potential interactions were explored: sex×(age group, ethnicity, deprivation quintile, rurality), age group×(ethnicity, deprivation quintile, rurality) and ethnicity×(age group, sex, deprivation quintile, rurality). The proportional hazards assumption was tested formally and visually using Schoenfeld residuals and log-log plots. Due to minor convergence in log-log plots for age and PD diagnosis, follow-up was divided into three seven-year time intervals, and multivariable Cox regression performed to calculate HRs for each period.
Univariable and multivariable logistic regression were performed to examine whether sociodemographic factors predicted the use of anti-osteoporosis treatment in PD patients. Multivariable models mutually adjusted for included covariates: age, sex, ethnicity and deprivation quintile.
Survival following major osteoporotic and hip fracture was plotted using Kaplan-Meier curves, from the date of fracture to the date of death or final censor date. In a sensitivity analysis, survival differences were examined after adjusting for age and sex differences between the groups.
Statistical analyses were conducted in R (Version 2024.09.0 + 375) and Python (version 3.11.3), with results expressed as unadjusted and adjusted HRs with 95% confidence intervals. Findings are presented in accordance with RECORD recommendations. 33
Results
There were 120,248 cases of incident PD and 228,124 matched controls with a total of 1,765,909 person-years of observation. Cases and controls were closely matched for age, sex, dwelling and socioeconomic status (Table 1). BMI and rates of cigarette smoking and alcohol consumption were significantly lower in PD than controls (P < 0.0001; Table 1). At baseline, PD cases were significantly more likely to have a prior history of falls, osteoporosis, major osteoporotic fracture, DXA imaging, and bisphosphonate, vitamin D and/or calcium use (P < 0.0001; Table 1).
Baseline features of incident Parkinson's cases and controls, 2003 to 2023.
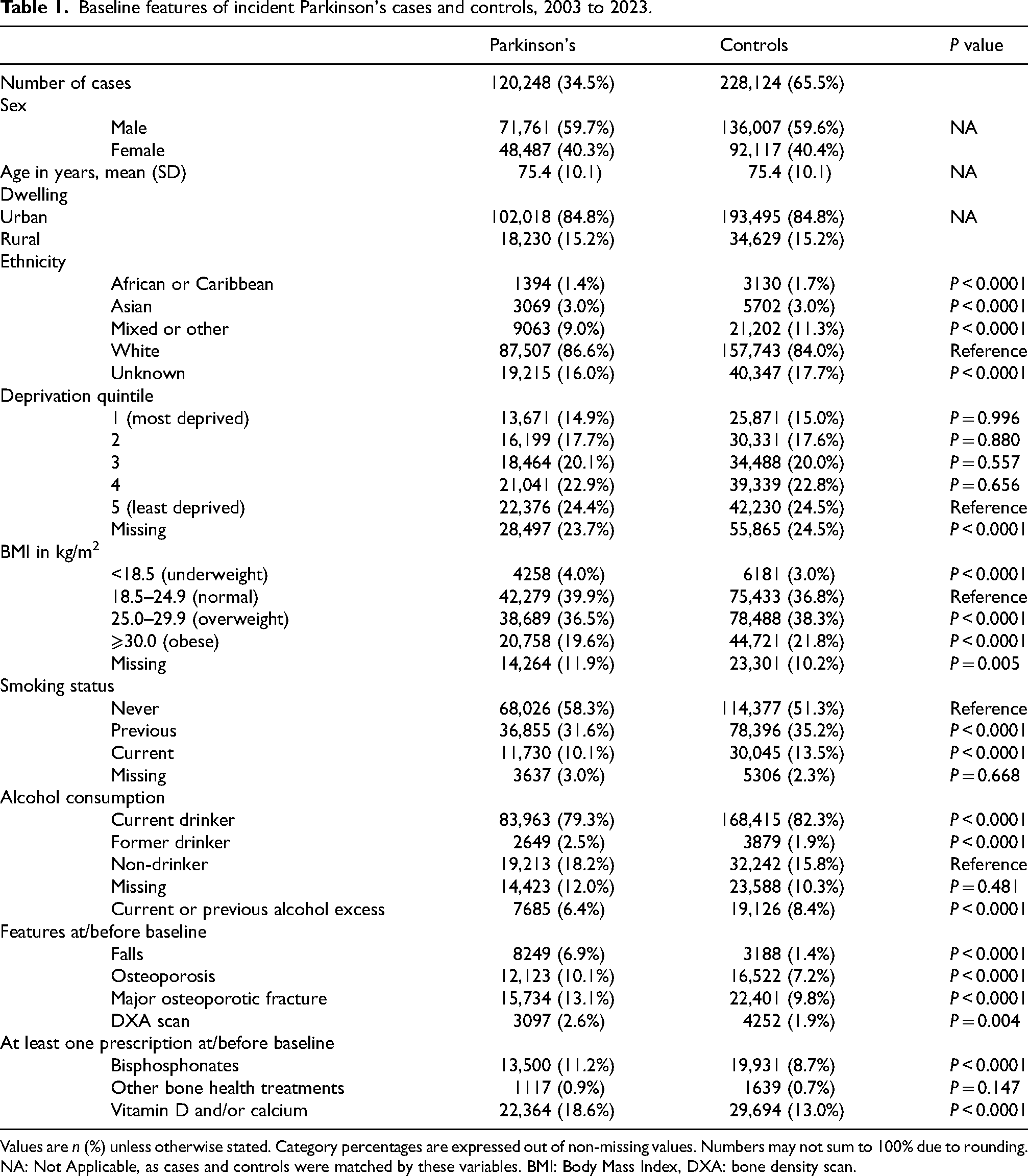
Values are n (%) unless otherwise stated. Category percentages are expressed out of non-missing values. Numbers may not sum to 100% due to rounding. NA: Not Applicable, as cases and controls were matched by these variables. BMI: Body Mass Index, DXA: bone density scan.
Incidence rates and comparison of PD to controls
Osteoporosis and fracture were substantially more common in PD than controls. For osteoporosis, crude incidence per 1000 person-years was 16.8 (16.4, 17.1) for PD versus 9.3 (9.2, 9.5) for controls (Table 2), giving an overall HR of 1.96 (95% CI 1.90, 2.02) (Figure 1). For fracture, crude incidence per 1000 person-years was 27.2 (26.8, 27.7) for PD versus 14.3 (14.0, 14.5) for controls (Table 3), giving an overall HR of 2.16 (2.11, 2.21) (Figure 1). The HR was increased for osteoporosis and fracture for PD versus controls for all time periods. For osteoporosis, risks were increased in PD at 0–7 years, HR 1.93 (1.87, 2.01); 7–14 years, HR 2.12 (1.98, 2.27); and 14–21 years, HR 2.01 (1.67, 2.41), all p < 0.0001. Similarly, for fracture, the HR was increased in PD at 0–7 years, HR 2.15 (2.09, 2.21), 7–14 years, HR 2.36 (2.24, 2.48) and 14–21 years, HR 1.88 (1.62, 2.17), all p < 0.0001 (Supplementary Table 1).
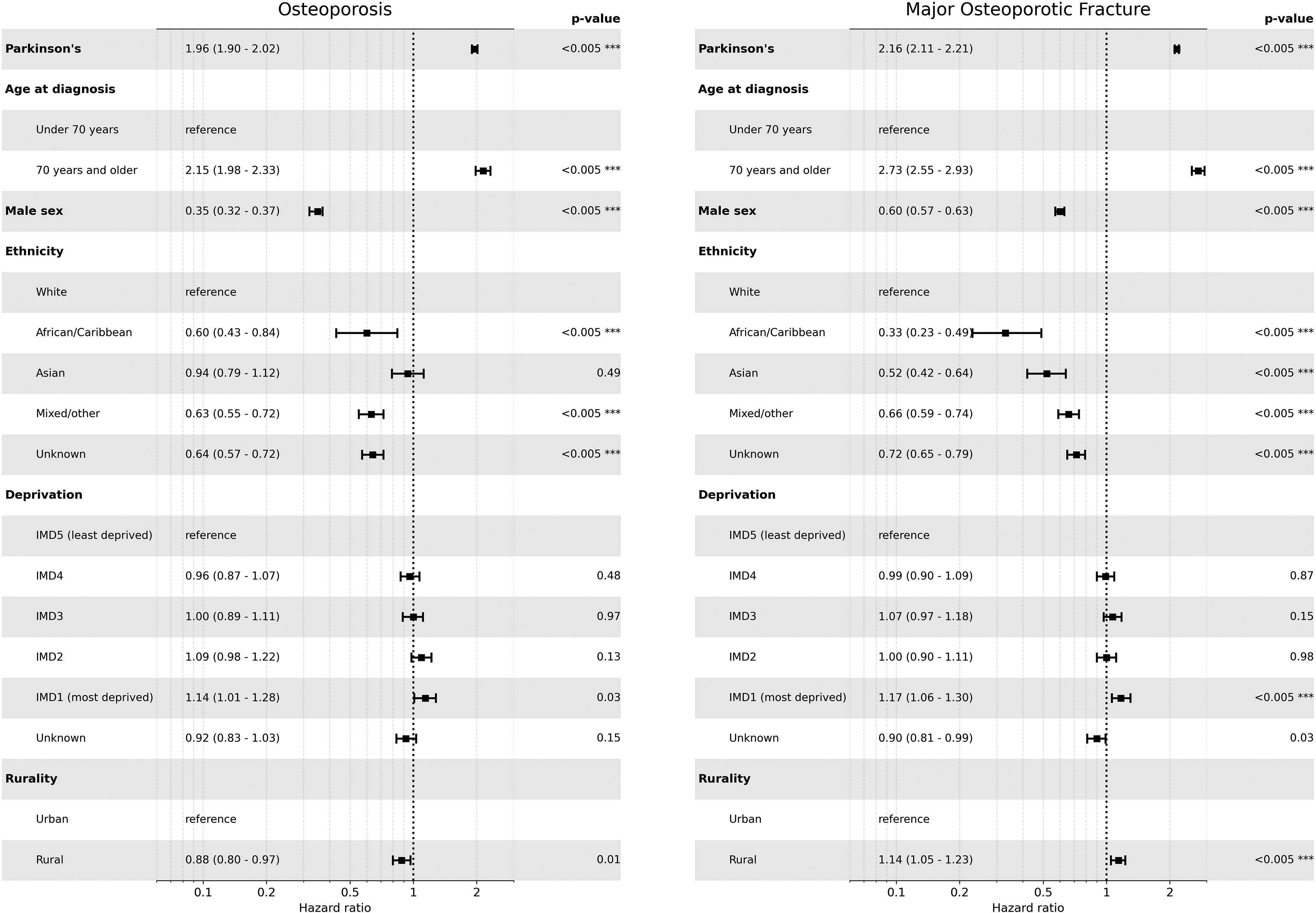
Sociodemographic factors associated with incident osteoporosis and major osteoporotic fracture in Parkinson's disease. The risks of osteoporosis and major osteoporotic fracture were significantly higher in Parkinson's cases than in matched controls, and increased with older age, female sex, greater deprivation and White ethnicity. Rurality was associated with a lower risk of osteoporosis, but a significantly increased risk of fracture. Hazard ratios are shown with 95% confidence intervals. *** indicates significant at p < 0.005. IMD: Index of Multiple Deprivation.
Incidence rates for associations of osteoporosis with exposure to Parkinson's.
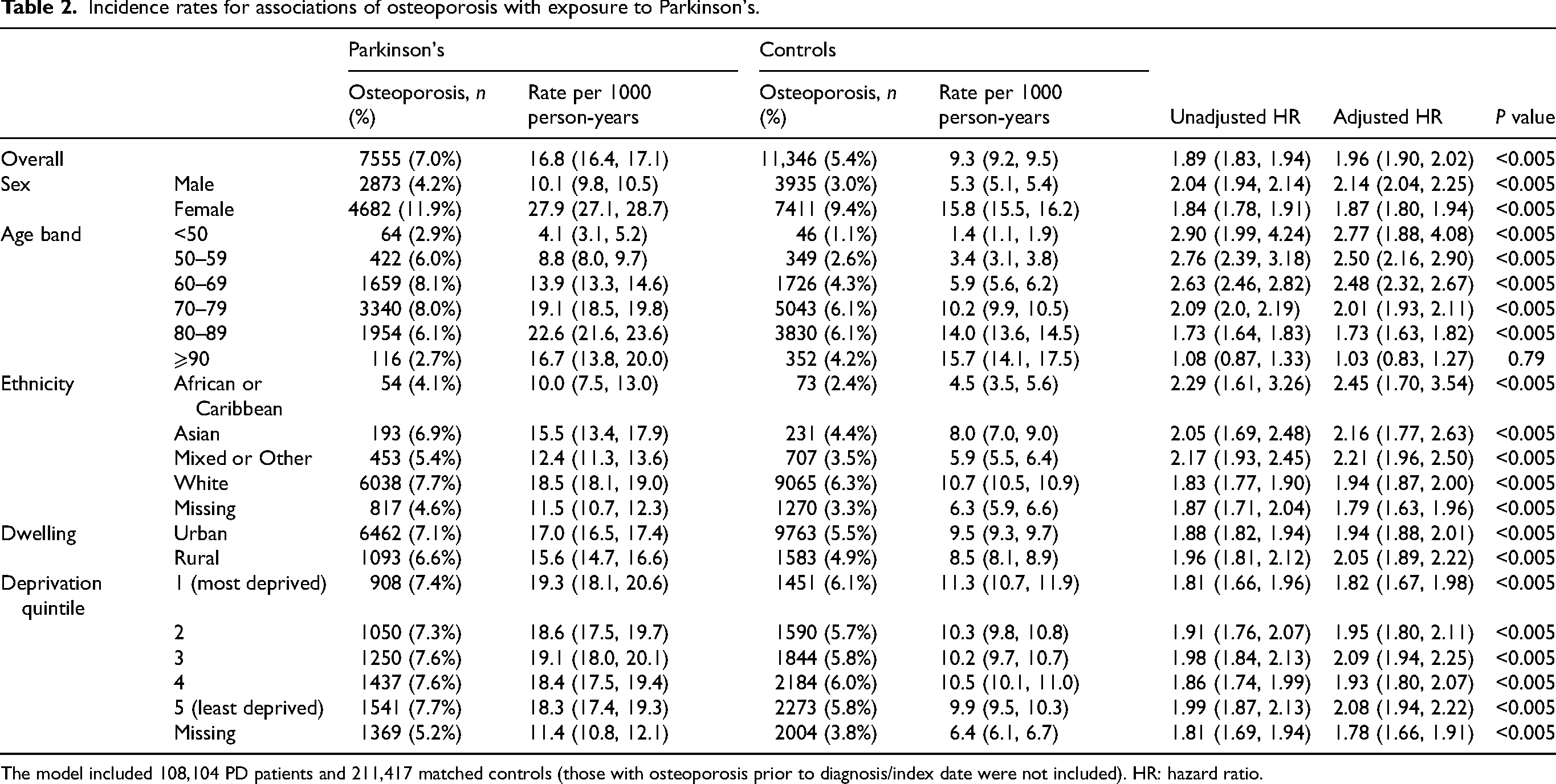
The model included 108,104 PD patients and 211,417 matched controls (those with osteoporosis prior to diagnosis/index date were not included). HR: hazard ratio.
Incidence rates for associations of major osteoporotic fractures with exposure to Parkinson's.
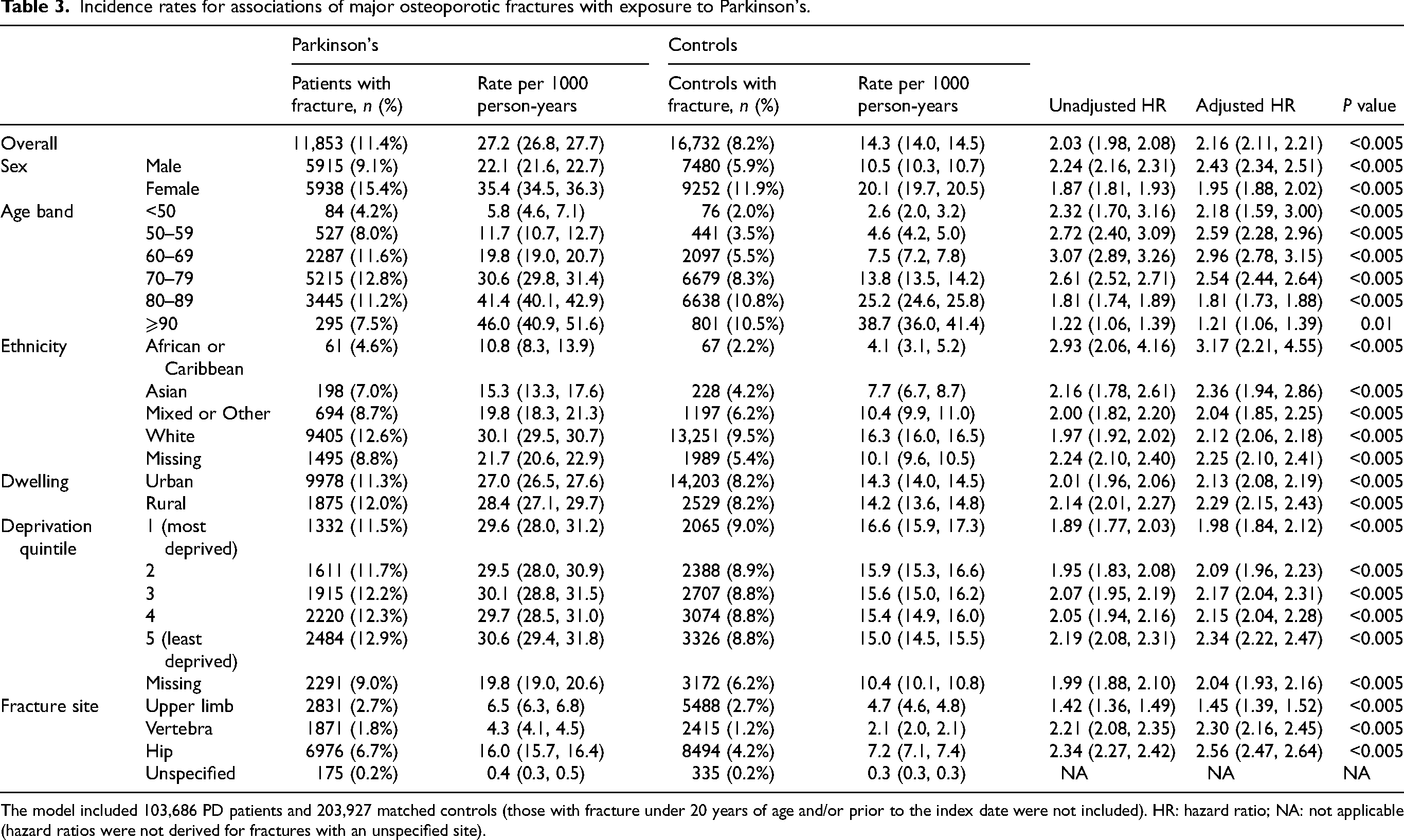
The model included 103,686 PD patients and 203,927 matched controls (those with fracture under 20 years of age and/or prior to the index date were not included). HR: hazard ratio; NA: not applicable (hazard ratios were not derived for fractures with an unspecified site).
Osteoporosis and fracture both increased with longer disease duration (Figure 2, Supplementary Table 2). By 5 years, the cumulative risk of fracture (all sites) was 12.2% (11.9, 12.5%) in PD versus 6.1% (6.0, 6.3%) in controls, which increased to 29.6% (28.9, 30.3%) in PD versus 14.4% (14.1, 14.6%) in controls by 10 years, and to 50.3% (48.6, 51.9%) in PD versus 25.9% (25.3, 26.5%) in controls by 15 years (Figure 2). PD cases had more fractures at all specified sites than controls (Figure 2, Table 3). The hip was the most common fracture site in PD, accounting for 58.9% of fractures versus 50.8% in controls (P < 0.001). Crude hip fracture incidence per 1000 person-years was 16.0 (15.7, 16.4) in PD versus 7.2 (7.1, 7.4) in controls.
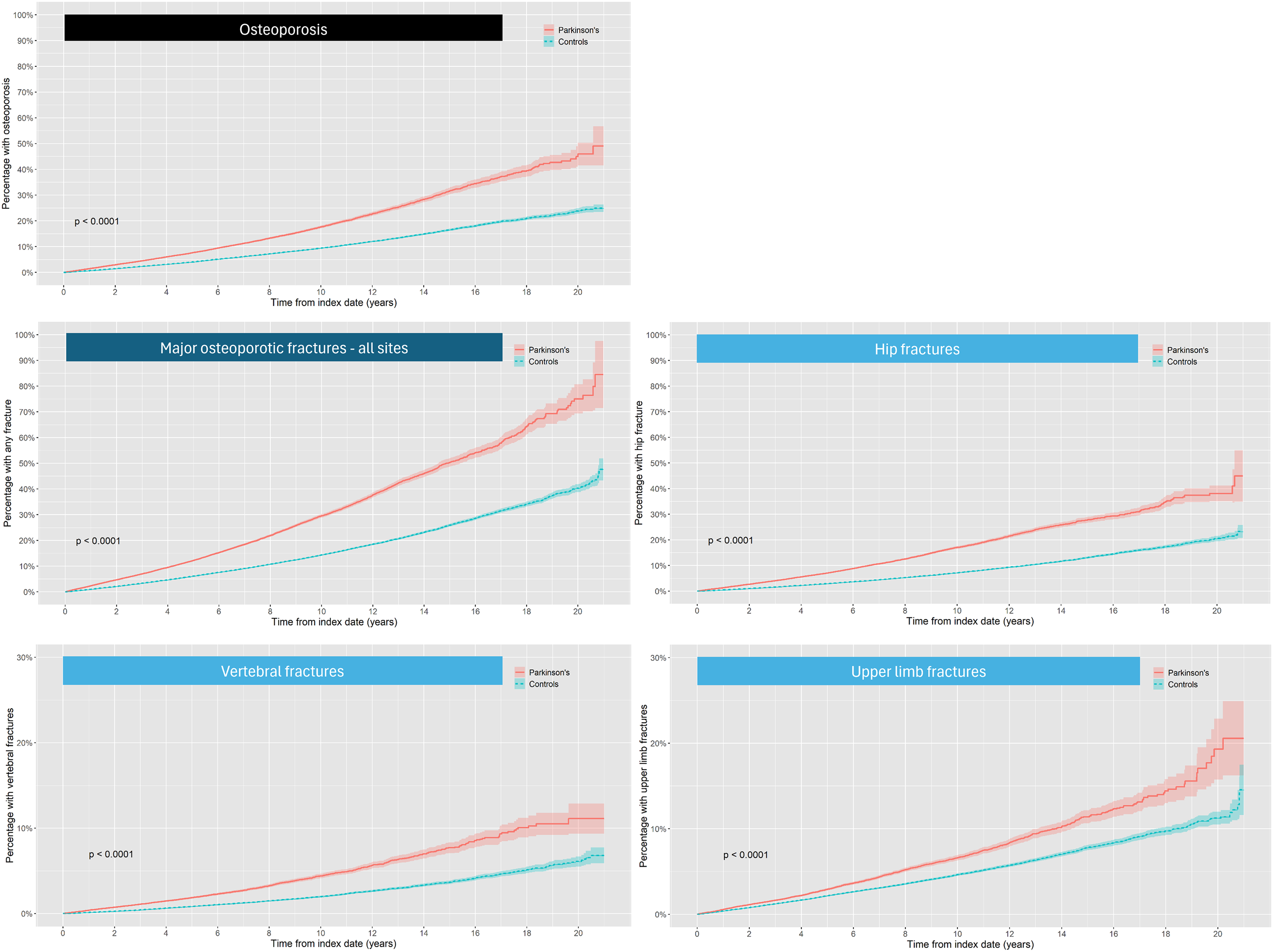
Cumulative hazard graphs of osteoporosis, major osteoporotic fracture and site-specific fracture in Parkinson's cases and controls. Compared to matched controls, PD cases had a significantly more osteoporosis and major osteoporotic fractures overall and at specified sites. Risks progressively increased with disease duration. Lines are shown with 95% confidence interval (lighter shading).
Demographic factors in relation to osteoporosis and fracture
Age, sex, ethnicity, deprivation and rurality were significantly associated with both osteoporosis and fracture (Figure 1). Increasing incidence rates were evident across all age bands except osteoporosis in the very elderly with PD (Tables 2 and 3). Osteoporosis was significantly less likely in African or Caribbean, and Mixed or Other ethnicities, compared to White and Asian ethnicities in whom the risk of osteoporosis was equivalent (Figure 1). Major osteoporotic fracture was significantly more common in White than other ethnicities. Both osteoporosis and fracture were significantly more likely in the most deprived IMD quintile. Rural living was associated with a significantly lower risk of osteoporosis, HR 0.88 (0.80, 0.97, P = 0.01), but a significantly higher fracture risk, HR 1.14 (1.05, 1.23), P < 0.005 (Figure 1).
Several interactions were identified: for osteoporosis, men of African or Caribbean ethnicity had a lower relative risk than women, HR 0.62 (0.42, 0.92), P = 0.02; additionally, the increased risk of older age was greater for individuals of Mixed or Other ethnicity compared to those of White ethnicity (osteoporosis HR 1.22 (1.10, 1.40), P = 0.01; and fracture HR 1.22 (1.09, 1.37), P < 0.005).
PD-attributable risks
Osteoporosis and fracture were significantly more likely in PD than controls for both sexes, all ages, ethnicities, dwellings and deprivation quintiles (Tables 2 and 3). However, the increased risks of osteoporosis were greater in men with PD compared to male controls, HR 2.14 (2.04, 2.25) P < 0.005, than in women with PD compared to female controls, HR 1.87 (1.80, 1.94) P < 0.005. This was also true for fracture: men with PD had an HR of 2.43 (2.34, 2.51) compared to male controls, while women with PD had an HR of 1.95 (1.88, 2.02) compared to female controls. Similarly, the increased risks of fracture were greater in PD cases of African or Caribbean ethnicity, HR 3.17 (2.21, 4.55) P < 0.005, compared to their controls, in contrast to an HR of 2.12 (2.06, 2.18) P < 0.005 for PD cases of White ethnicity compared to their controls.
DXA scans
The DXA scan rate was higher for PD at 13.6 (13.3, 13.9) scans per 1000 person-years than in controls at 7.4 (7.3, 7.6) scans per 1000 person-years. Similarly, the DXA scan rate was higher in women with PD at 21.7 (21.1, 22.4) than in men with PD at 8.1 (7.7, 8.4) per 1000 person-years. Similar patterns by sex were observed for controls: women 13.0 (12.7, 13.3) vs. men 3.6 (3.5, 3.7) scans per 1000 person-years.
Treatment
Anti-osteoporosis therapy was significantly more likely in PD than controls, OR 1.35 (1.33, 1.38), P < 0.0001 (Table 4). Treatment was significantly less likely in men than women with PD, OR 0.25 (0.24, 0.26) (Table 4), being lower than the relative risk of osteoporosis, HR 0.35 (0.32, 0.37), and fracture, HR 0.60 (0.57, 0.63) (Figure 1). Treatment rates were lowest in the most deprived quintile, OR 0.85 (0.80, 0.90), compared to the least deprived, P < 0.0001 (Table 4) despite having higher rates of osteoporosis, HR 1.14 (1.01, 1.28), P = 0.03, and fracture, HR 1.17 (1.06, 1.30), both P < 0.005 (Figure 1). Treatment rates in PD by demographic factors are in Supplementary Table 3. Therapy persistence rates were similar for PD and controls (Supplementary Table 4). Secondary preventive treatment was used more than primary prevention, both in PD (secondary 33.2% of cases, primary 15.9%) and controls (secondary 30.5% of cases, primary 12.6%) (Supplementary Table 4). In PD cases with both osteoporosis and fracture, treatment rates were 63.4% in men compared to 77.9% in women.
Multivariable modelling of sociodemographic factors associated with anti-osteoporosis treatment in PD.
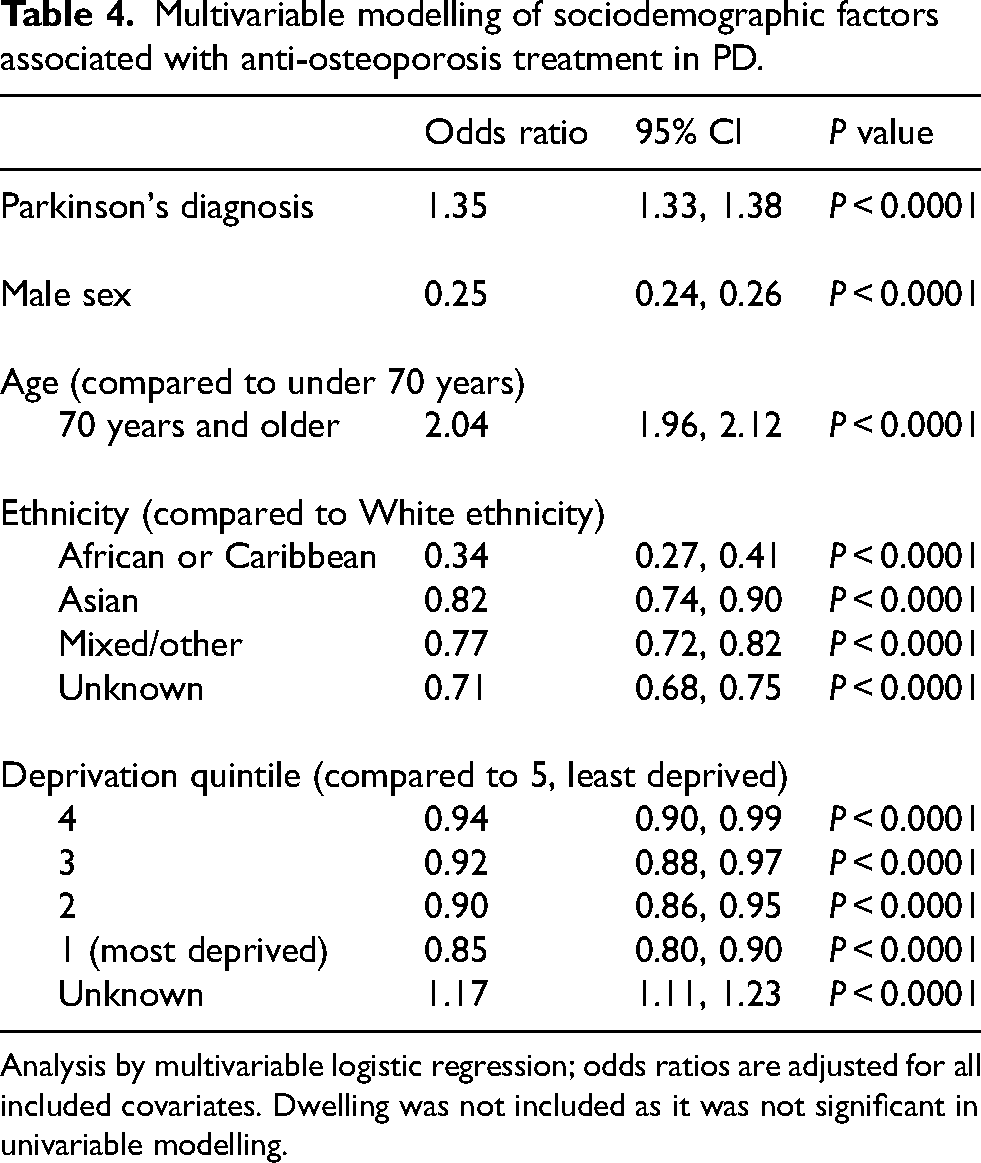
Analysis by multivariable logistic regression; odds ratios are adjusted for all included covariates. Dwelling was not included as it was not significant in univariable modelling.
Survival after major osteoporotic and hip fracture
Major osteoporotic fractures occurred on average 4.0 years earlier in PD than controls, while hip fractures occurred 5.1 years earlier (Supplementary Table 5). Survival after fracture was significantly worse in PD cases than controls, even after age and sex adjustment (Supplementary Table 5, Supplementary Figures 2 and 3). For major osteoporotic fracture, median survival was 4.0 (3.9, 4.2) years in PD, compared to 10.7 (10.0, 11.6) years for controls. For hip fracture, median survival was 3.2 (3.1, 3.4) years in PD, compared to 8.2 (7.3, 9.2) years for controls.
Discussion
This large representative population-based study confirms and extends previous findings that PD patients have a significantly higher risk of both osteoporosis and major osteoporotic fracture than matched controls.1–3,34,35 The long follow-up duration afforded a detailed comparison of risk in PD relative to controls for early, middle and later disease, and is a novel finding. The relative risk of fracture declined 14 to 21 years after a PD diagnosis, presumably reflecting reduced mobility in more advanced PD, and there was no evidence of an exponentially increased fracture risk after 10 years of disease. 36 Our finding of significantly more falls, osteoporosis and fracture before a PD diagnosis in cases than controls is consistent with reports of increased risks of injurious falls, 37 fracture37,38 and traumatic brain injury 39 5 to 15 years before a PD diagnosis. The findings during prodromal and earlier disease challenge the concept of falls and fractures as later manifestations of progressive motor impairment in PD. Instead, more subtle motor and non-motor features begin during the PD prodrome,40–43 and affect bone health throughout the disease course. Accordingly, falls and fractures should be explored as a component of algorithms to identify prodromal PD, 44 and bone health assessment should be a part of both initial and ongoing PD management.
Our incidence rate of 27.2 per 1000 for major osteoporotic fracture in PD is higher than the 16.5 per 1000 reported from the US, 45 but those cases were younger and only those with procedural repairs were included. Our incidence rate is lower than a Taiwanese rate of 39.5 per 1000, 36 but that had a higher proportion of females and was limited to people aged 40 years and older, so rates were also higher in controls, making their hazard ratio similar to ours. Our finding that the risk of major osteoporotic fracture in PD is more than doubled is consistent with several meta-analyses.1–3 Collectively these findings indicate a substantial risk of fracture attributable to PD, making bone health assessment an essential component of best clinical care for PD.
Hip fractures represented almost 60% of incident major osteoporotic fractures in PD, which was more than 8% higher than in controls. Prior studies largely concur with the hip as the most common fracture site in PD.2,46–49 Although one study reported the upper limb as the commonest site, their cases were younger and it was hypothesized that their lower hip fracture numbers might reflect the protective effect of a higher BMI in US patients. 45 Earlier suggestions that hip bone mineral density was differentially reduced relative to other sites in PD 50 have not proven accurate, 1 suggesting that falls (with loss of protective arm extension due to bradykinesia) and low BMI are more likely culprits for the increased fracture risk in PD than selective hip bone architectural change. Given its associations with prolonged hospitalization, 51 impaired quality-of-life 52 and increased mortality,53–58 an excess relative risk of hip fracture in PD has significant clinical implications.
The risk of osteoporotic vertebral fracture was approximately doubled in PD compared to controls, and was second to hip fracture in terms of risk attributable to PD. Although a prior study also found a doubling of risk of neck and trunk fractures in PD, non-fragility fractures were included. 36 A South Korean study found that the increased risk of vertebral fracture in PD was lower at 1.7, potentially relating to their larger proportion of women (59% vs. 40%). 59 Vertebral fractures are inevitably underestimated,34,60 as only one-third present clinically and their radiological presence may be undocumented. 61 Accordingly, vertebral fractures are likely to be the second commonest osteoporotic fracture in PD and are important to prevent given their association with back pain and postural and gait impairment. 62
The well-known increased risks of osteoporosis and fracture conferred by PD were present in both sexes and increased with age as expected, 1 but were greater in men than women with PD when compared with controls. Although a prior meta-analysis found no sex differences in fracture, fracture sites varied across the included studies. 2 In a subsequent meta-analysis, the increased relative risk of hip fracture conferred by PD had overlapping confidence intervals between the sexes, likely due to heterogeneity in sample size and follow-up duration. 35 Our findings concur with a more recent meta-analysis that found the relative risk of hip fractures to be greater in men than women, 34 and with a large population-based UK study that had similar conclusions for all osteoporotic fracture sites. 63 This higher relative risk in males than females should be factored into clinical management (e.g., falls prevention and anti-osteoporosis therapy).
Deprivation
Osteoporosis and fracture incidence varied by deprivation, with significantly higher rates in PD cases from the lowest socioeconomic group. Although low socioeconomic status, measured at an individual rather than area level, was associated with increased fracture risk in the general population in a recent meta-analysis, 20 results in PD are conflicting. Low income was associated with fracture in one study, 36 while another identified no associations between household income and osteoporosis or vertebral fracture. 59 Compared to composite measures such as IMD, income may not be a good surrogate for deprivation. As smoking, 64 alcohol excess, 65 malnutrition and physical inactivity 66 are linked with deprivation and poor bone health, 67 these factors likely contribute to associations between deprivation, osteoporosis and fracture risk. Although we did not have data on malnutrition or physical activity, our models adjusted for other important lifestyle factors mediating this association, including smoking and alcohol intake.
Ethnicity
We confirmed significant variation in both osteoporosis and fracture risk by ethnicity. Compared to White PD cases, individuals of African or Caribbean ethnicity and other ethnic minority groups had substantially lower osteoporosis and fracture incidence, confirming findings in the general population.16,68,69 However, when compared to controls, PD cases of African or Caribbean ethnicity had a higher relative risk of osteoporosis and fracture than PD cases of White ethnicity. A similar higher relative risk of fracture in Black than White individuals was suggested in diabetes mellitus, but those studies were underpowered to reach a definite conclusion.70,71 We observed a novel interaction between ethnicity and age, highlighting the need for special attention for older individuals of Mixed or Other ethnicity, in whom risks of osteoporosis and fracture were significantly increased. Increased relative risks of fracture in groups with lower absolute risk have been reported previously in younger than older cases for both rheumatoid arthritis 72 and asthma. 25 Comparing those with and without PD, the magnitude of relative risk estimates for osteoporosis and fracture may be accentuated by having a lower baseline risk. However, the practical significance is that the adverse effect of PD on bone health means that ‘lower risk’ sub-groups should be included in bone health assessments.
Treatment
We found several pointers to underutilization of anti-osteoporosis treatment in PD cases, as observed elsewhere.73,74 Although treatment rates were around one-third higher in PD than controls, osteoporosis was twice as common in PD. This treatment gap was greater in PD for men than women: women were 4 times more likely to be on anti-osteoporosis treatment, while having 1.7 times more major osteoporotic fractures than men. Anti-osteoporosis treatment was especially underutilized in PD cases in the most deprived quintile, despite significantly higher risks of both osteoporosis and fracture, highlighting this group for special attention. There was less osteoporosis but more fractures in rural compared to urban dwellers, but equivalent rates of anti-osteoporosis therapy; this might be explained by underdiagnosis of osteoporosis and/or lifestyle differences, and merits further investigation. Anti-osteoporosis treatment was more than twice as likely as secondary than primary prevention, both in PD and controls, which is consistent with other reports.73,74 As PD is an independent significant risk factor for osteoporosis and fractures, there is a need to apply a Parkinson's-specific approach to the management of bone health,10,11,73 and following this approach would result in a major shift from secondary to primary prevention.
Mortality
PD patients had shorter survival following major osteoporotic and hip fracture than controls. Most studies of survival after fracture in PD examined only hip fractures and findings are inconsistent.75–79 Earlier short-duration studies showed no difference in mortality following hip fracture between PD cases and controls at six months 80 and one year. 81 Our findings are in agreement with more recent studies that found that PD independently predicts longer-term mortality over six 77 and eight years. 75
Limitations
There are some limitations: case ascertainment and events such as falls relied on diagnostic codes, which may be inaccurate or incomplete. Increased osteoporosis incidence could relate to better screening in PD compared to controls, although this does not explain the higher rates of osteoporosis in PD before diagnosis. Calcium and vitamin D may be purchased without prescription, and parenteral therapies given in hospital may not be recorded in primary care. Imaging data from HES-DID were unavailable from November 2020 to December 2023 inclusive, so overall rates of DXA scan use are an underestimate. Miscoding of PD as atypical parkinsonian disorders could overestimate the proportion with falls at baseline, but we excluded cases with diagnostic codes for other parkinsonian disorders 27 and the proportion of cases with baseline falls, osteoporosis and fracture is too high to be explained by atypical parkinsonism given their relative rarity. As in a previous CPRD analysis, 25 a small proportion of fractures had no specified site, which affects quantification, and osteoporosis and vertebral fractures are both likely to be underascertained.16,25
Conclusion
Combining primary and secondary care data, this is one the largest studies of osteoporosis and major osteoporotic fracture in PD, and its representative sample allows for generalization to the wider PD population. PD-attributable risks are increased in both sexes but especially in men. Risks of fracture are independently increased both in the most deprived and in those living rurally, highlighting these groups for additional attention. Bone health assessment is needed early in the disease course, with a shift in focus from secondary to primary prevention, and a measurable aim of increased treatment rates.
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X261429758 - Supplemental material for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study
Supplemental material, sj-docx-1-pkn-10.1177_1877718X261429758 for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study by Sacha E Gandhi, Katherine A Grosset, Prasanth A Iruthayaraj, Lance Lee, Cathal Doyle and Donald G Grosset in Journal of Parkinson's Disease
Supplemental Material
sj-docx-2-pkn-10.1177_1877718X261429758 - Supplemental material for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study
Supplemental material, sj-docx-2-pkn-10.1177_1877718X261429758 for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study by Sacha E Gandhi, Katherine A Grosset, Prasanth A Iruthayaraj, Lance Lee, Cathal Doyle and Donald G Grosset in Journal of Parkinson's Disease
Supplemental Material
sj-docx-3-pkn-10.1177_1877718X261429758 - Supplemental material for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study
Supplemental material, sj-docx-3-pkn-10.1177_1877718X261429758 for Early bone health assessment is indicated in Parkinson's: Risk factor analysis in a UK population-based cohort study by Sacha E Gandhi, Katherine A Grosset, Prasanth A Iruthayaraj, Lance Lee, Cathal Doyle and Donald G Grosset in Journal of Parkinson's Disease
Footnotes
Acknowledgments
This work is part of a service improvement project supported by Parkinson's UK, and has extensive input from an expert multidisciplinary team including medical, specialist nursing, therapists and people with Parkinson's. We thank Syed Hussain of Parkinson's UK for help in data handling.
This study (protocol 24_003867) is based in part on data from the Clinical Practice Research Datalink, obtained under license from the UK Medicines and Healthcare products Regulatory Agency. The data is provided by patients and collected by the NHS as part of their care and support. Hospital Episode Statistics (HES) and Office for National Statistics (ONS) data: Copyright © 2023, re-used with the permission of The Health & Social Care Information Centre. All rights reserved. The interpretation and conclusions contained in this study are those of the authors alone.
Ethical considerations
Both the study protocol (24_003867) and access to data were approved by the CPRD's Research Data Governance Process. Informed patient consent was not necessary for this work. Ethical approval for observational public health research was granted to CPRD by the UK Health Research Authority (HRA) Research Ethics Committee. We confirm that we have read the Journal's position on issues involved in ethical publication and affirm that the work is consistent with those guidelines.
Consent to participate
Individual level patient consent to participate was not required but GP practices consented to the collation, processing and linkage of deidentified data.
Consent for publication
Not applicable
Author contributions
1. Research project: A. Conception, B. Organization, C. Execution;
2. Statistical Analysis: A. Design, B. Execution, C. Review and Critique;
3. Manuscript Preparation: A. Writing of the first draft, B. Review and Critique;
Sacha E Gandhi: 1B, 1C, 2A, 2B, 2C, 3A, 3B
Katherine A Grosset: 1A, 1B, 1C, 2A, 2C, 3B
Prasanth A Iruthayaraj: 1B, 1C, 2A, 2B, 2C, 3B
Lance Lee: 1B, 1C, 2A, 2C, 3B
Cathal Doyle: 1A, 1B, 1C, 2C, 3B
Donald G Grosset: 1A, 1B, 1C, 2A, 2C, 3B
Funding
The authors received grant support from Parkinson's UK via their institution for the research, authorship and/or publication of this article.
Declaration of conflicting interest
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: This work was performed under a CPRD multi-study license, paid for by Parkinson's UK. The academic team defined the design, analysis methods and interpretation of the data. Employees of Parkinson's UK worked collaboratively with the academic team, but the academic team had a primary role in writing the report and in the decision to submit for publication.
Parkinson's UK provided grant funding for the Tracking Parkinson's study and the Bone Health Improvement in Parkinson's project for which DGG was a principal investigator. SEG received financial support from these grants for research time in preparation for the submission of a PhD thesis.
KAG and DGG have received consultancy payments from Parkinson's UK related to this research. PAI, LL and CD are employees of Parkinson's UK.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.