
Abstract
Treating a neurological disorder through the gut may seem counterintuitive, yet multiple lines of evidence highlight the gut's important role in Parkinson's disease (PD). Prodromal gastrointestinal symptoms, the presence of aggregated α-synuclein in enteric neurons, increased intestinal inflammation, and impaired epithelial barrier integrity all point to gut-level involvement in PD pathophysiology. The gut microbiome, markedly altered in individuals with PD, may be a key driver of these changes. Fecal microbiota transplantation (FMT) is currently the most effective strategy for achieving broad and durable modifications of gut microbiota composition. However, FMT is a complex, multi-step procedure requiring stringent methodological control. Modulating gut bacteria has demonstrated therapeutic potential in preclinical models of PD, and recent clinical trials have begun evaluating FMT in patients, although outcomes have been variable. In this review, we examine potential explanations for these divergent results, with a particular focus on methodological differences across trials. We also outline future directions for optimizing FMT study design in PD and discuss how these insights may guide the development of next-generation microbiota-targeted therapies.
Plain language summary
Treating a brain disorder by targeting the gut may seem surprising, but growing evidence shows that the gut plays an important role in Parkinson's disease (PD). Many people with PD experience digestive symptoms years before motor symptoms begin. In addition, the disease-related protein alpha-synuclein, inflammation, and a leaky gut barrier have been found in the intestines of people with PD. The community of bacteria living in the gut (the gut microbiome) is also markedly different in people with PD and may contribute to these changes.
Fecal microbiota transplantation (FMT) is a treatment designed to restore a healthier gut microbiome by transferring gut bacteria from a healthy donor to a patient. At present, this is the most effective available method for achieving sustained changes in gut bacteria. However, it is also a complex procedure that requires careful handling and standardized methods. Studies in animal models of PD suggest that changing gut bacteria can improve disease-related symptoms. Clinical trials in people with PD have explored FMT, but the results so far have been inconsistent.
In this review, we discuss possible reasons why studies of FMT in PD have produced mixed results, focusing especially on differences in how these studies were designed and conducted. We also highlight key considerations for future research and explain how a better understanding of these issues could help develop more targeted and effective bacterial-based treatments for Parkinson's disease.
Keywords
Parkinson's disease: a gut-first disorder?
Many people with Parkinson's disease (PD) suffer from symptoms that manifest along the entire gastrointestinal tract, including – in rostrocaudal order – drooling, dysphagia, gastroparesis, constipation, and defecatory dyssynergia. 1 Especially the high prevalence of constipation is striking, with up to 80% showing a slower colonic transit time. 2 The relationship between prodromal constipation and PD is well established through both retrospective and prospective studies showing that constipation can present many years before PD is diagnosed. 3 The occurrence of gastrointestinal symptoms that precede the onset of PD is only one argument to suggest that PD is a disorder of both the brain and the gut (Figure 1). Aggregates of α-synuclein, the pathological hallmark of PD, can be found in the enteric nervous system of patients up to 20 years prior to PD diagnosis, 4 and according to the Braak hypothesis precede brain pathology and subsequently migrate to the brain via the vagal nerve.5,6 The vagal nerve is the most important neuronal pathway connecting the enteric neurons to the lower brainstem. Interestingly, epidemiological studies show that full truncal vagotomy in humans is associated with a reduced risk of PD.7,8 Direct evidence of the prion-like migration of α-synuclein from gut to brain, with a protective role of vagotomy, has been shown in animal models using gut wall injection of α-synuclein fibrils; further long-term follow-up shows a phenotype that mimics the gradual development of non-motor and motor symptoms as seen in PD patients, as well as the characteristic degeneration of dopaminergic neurons. 9 In contrast, brain to gut migration of α-synuclein has been replicated as well in several animal models. 10 Current literature suggests morphological and functional changes to the integrity of the gut epithelial barrier in PD patients. 11 The question remains if an increased gut wall permeability can lead to the increased uptake of certain toxicants or pathogens and in this way play a role in disease onset or progression. Microbial components such as lipopolysaccharide (LPS; a component of the gram-negative bacterial cell wall) can induce local proinflammatory effects in the gut tissue; upon entering the circulation, however, they are highly immunogenic and trigger systemic inflammatory responses. 12 Inflammation is increasingly being recognized as an important facilitator and aggravator of PD pathology, especially clear in preclinical models.13,14 PD patients exhibit a chronic subclinical colonic inflammation, represented by an elevated expression of pro-inflammatory markers and glial markers in gut biopsies. 15 The stool of PD patients contains elevated levels of inflammatory markers such as calprotectin, IL-1α, IL-1β and CRP.16,17 In a preliminary study including six patients with inflammatory bowel diseases (IBD), α-syn pathology was identified in the enteric nervous system, 18 although these findings require independent confirmation. Epidemiological studies show conflicting evidence regarding the association between IBD and the risk of developing PD. 19 Remarkably, one study reported that an increased risk was substantially reduced in patients with an early start of anti-inflammatory anti-TNF therapy. 20 Small intestinal bacterial overgrowth has been found to affect up to half of PD patients and has been associated with more severe motor fluctuations. 21
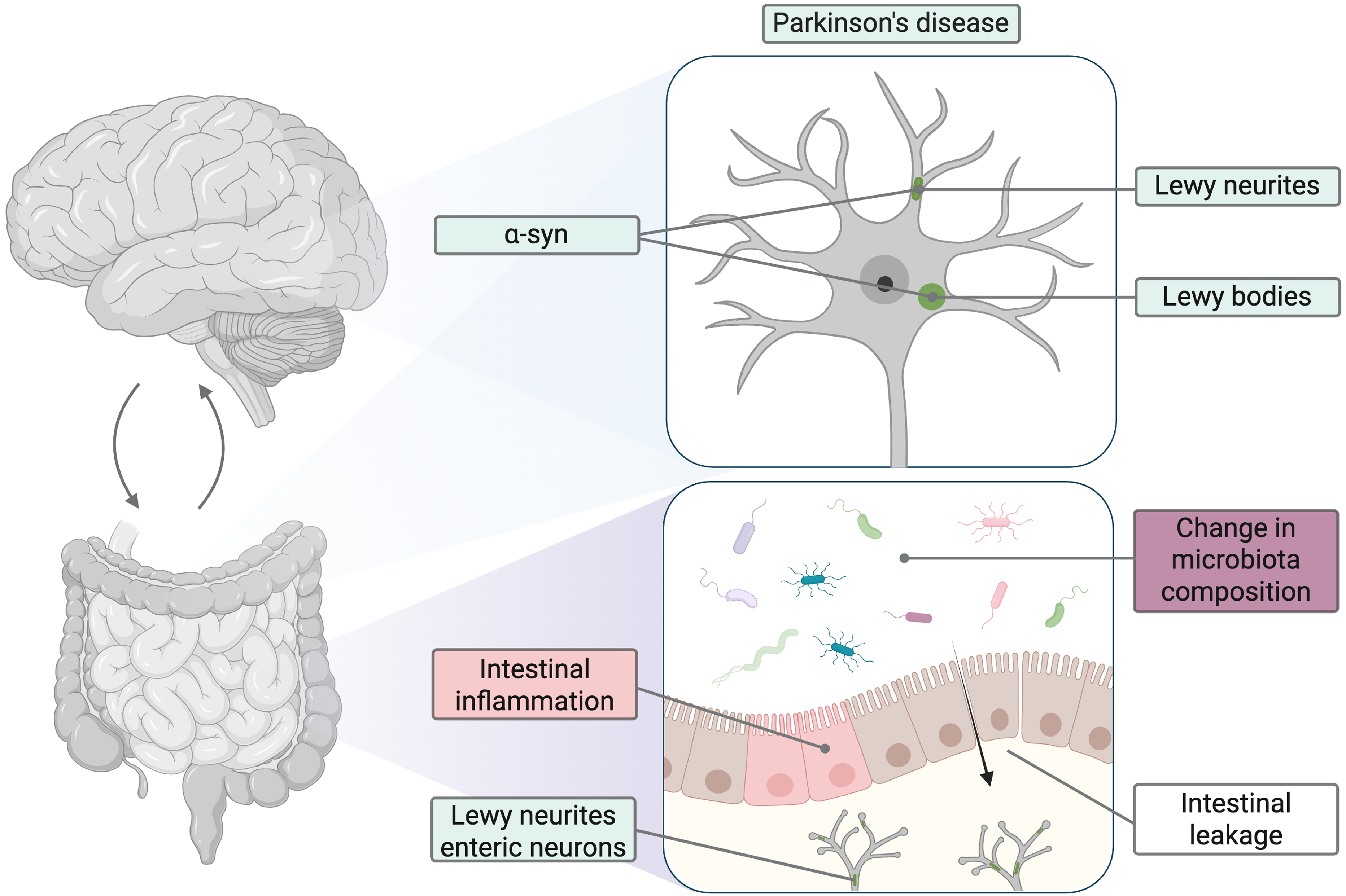
A central role for the gut in Parkinson's disease. Figure was created in BioRender by Vandendriessche (2026): https://BioRender.com/b0lzw74.
In recent years, attention has turned towards the gut microbiome as a driver of these gastrointestinal changes in PD. The gut microbiome consists of bacteria – along with fungi, viruses, and archaea – representing over 100 times as many genes as the human genome. 22 These microorganisms contribute to the regulation of gastrointestinal motility, facilitate nutrient absorption and metabolism, modulate the immune system and maintain intestinal health. 23 These gut microbiota influence the brain via three important pathways: the nervous system (including the vagal nerve and the enteric nervous system), the immune system, and the endocrine system. These bidirectional communication pathways are called the gut-brain axis. Gut bacteria can exert their effects through several methods including synthesising neurotransmitters (eg, GABA, dopamine), affecting dietary amino acids (eg, tryptophan and indoles), inducing cytokine and chemokine release, stimulating release of gut peptides and hormones from enteroendocrine cells, producing microbial metabolites such as short-chain fatty acids and secondary bile acids. There is also a growing interest in the role of bacteria-derived extracellular vesicles in microbiota-host interactions. 24 Interestingly, certain bacteria are able to produce amyloid-like curli that can induce aggregation of α-synuclein. 25
In a seminal paper by Sampson and colleagues, germ-free transgenic α-synuclein overexpressing mice showed reduced microglia activation, α-synuclein inclusions and motor deficits compared to animals with a physiological microbiome. Interestingly, treatment with microbiota-produced short chain fatty acids (SCFA) restored all major features of the disease in germ-free mice and colonization of these mice with the microbiome of PD patients aggravated the physical impairment, which was not the case with microbiota of healthy persons. 26 More recently, it has been shown that transplanting gut microbiota from PD patients is also capable of inducing gut inflammation and intestinal barrier disruption, and ultimately motor dysfunction and dopaminergic neurodegeneration in wild-type mice. 27
In recent years, extensive gut microbiota studies have been carried out in PD worldwide, and despite the differences in methodology, geography, and dietary preferences; several changes show up consistently compared to healthy controls, including increases in Lactobacillus, Akkermansia, and Bifidobacterium, and decreases in Prevotella, Roseburia, Blautia, and Faecalibacterium.28–31 Bacterial genera such as Akkermansia are mucus degraders and can thus reduce the permeability of the gut epithelial barrier. Several of the taxa that are reduced in abundance are known to be producers of the anti-inflammatory SCFA, which is confirmed by the decreased presence of fecal SCFAs in PD, contributing to a pro-inflammatory state.29,32 Intriguingly, the same trends were reproduced in patients with idiopathic rapid eye movement sleep behavior disorder, which is a highly specific prodromal symptom of PD and thus indicating that microbiome alterations precede the motor symptoms.33–35 While gut microbiota alterations are reproducible across cohorts, their global effect size remains modest, with PD disease status accounting for only a small proportion of total microbiome variability. 30 This suggests that disease-associated microbial signatures are subtle relative to dominant ecological drivers such as diet, medication, and host-specific factors.
The above mentioned lines of evidence linking the gut and the brain in PD have led to a new hypothesis stating that disease onset can be either brain-first or body-first. 36 In the body-first phenotype, pathology is believed to start in the gut and emerging evidence suggests that the gut microbiome may play a pivotal role in PD pathogenesis and progression. 37 This framework has further increased the interest in the gut as an opportunity for diagnostic and therapeutic progress.
Fecal microbiota transplantation as a treatment to impact the gut-brain axis
Several treatments might influence the gastrointestinal health and the gut microbiota composition, including diet and nutritional supplements. It is thought that a healthy diet and regular exercise – besides their obvious health benefits – are also important factors for maintaining a healthy microbiome. 23 Dietary interventions can rapidly alter gut microbiota composition to a certain extent; however, diet adherence seems to be required to maintain changes in microbial diversity. 38
Dietary interventions using prebiotics (eg, fibers) that boost the SCFA-producing bacteria might have promise to restore this disbalance in SCFA production in PD. 39 Probiotics, including the administration of live gut bacteria, have shown promising potential in improving both motor and non-motor symptoms in PD. 40 Treatments with antibiotics have shown limited evidence for positive effects and published trials have mainly focused on treating PD patients with comorbid Helicobacter pylori infections or small intestinal bacterial overgrowth.21,41
Prebiotics, probiotics, postbiotics (eg, bioactive compounds produced by gut microbiota), and antibiotics can modulate the gut microbiota, but their effects are typically partial and difficult to sustain over time. Because the gut microbiota function as a complex and interconnected ecosystem, interventions targeting only selected components are often insufficient to induce durable ecosystem shifts. In contrast, fecal microbiota transplantation (FMT) may achieve comprehensive and long-lasting remodelling of gut microbial communities. 42 In FMT, fecal material from a healthy donor is introduced into the gastrointestinal tract of a patient with the aim of restoring a balanced gut flora. International guidelines have been developed in an attempt to standardize the procedure including healthy donor selection and processing of the donor stool sample; however, considerable debate and methodological variability persist regarding patient selection, pre-intervention bowel preparation, method of delivery, and follow-up43,44 (Figure 2). FMT has been safely and successfully used for treating Clostridioides difficile infections, for which it is an approved indication. 45 In addition, FMT is being explored in other chronic conditions such as inflammatory bowel disease and depression.46,47 Long-term safety data (>1 year post-FMT) does not show specific issues or adverse events. 48 Although this safety is strongly dependent on strict donor screening, patient selection, FMT product processing and performing the procedure in a controlled environment.
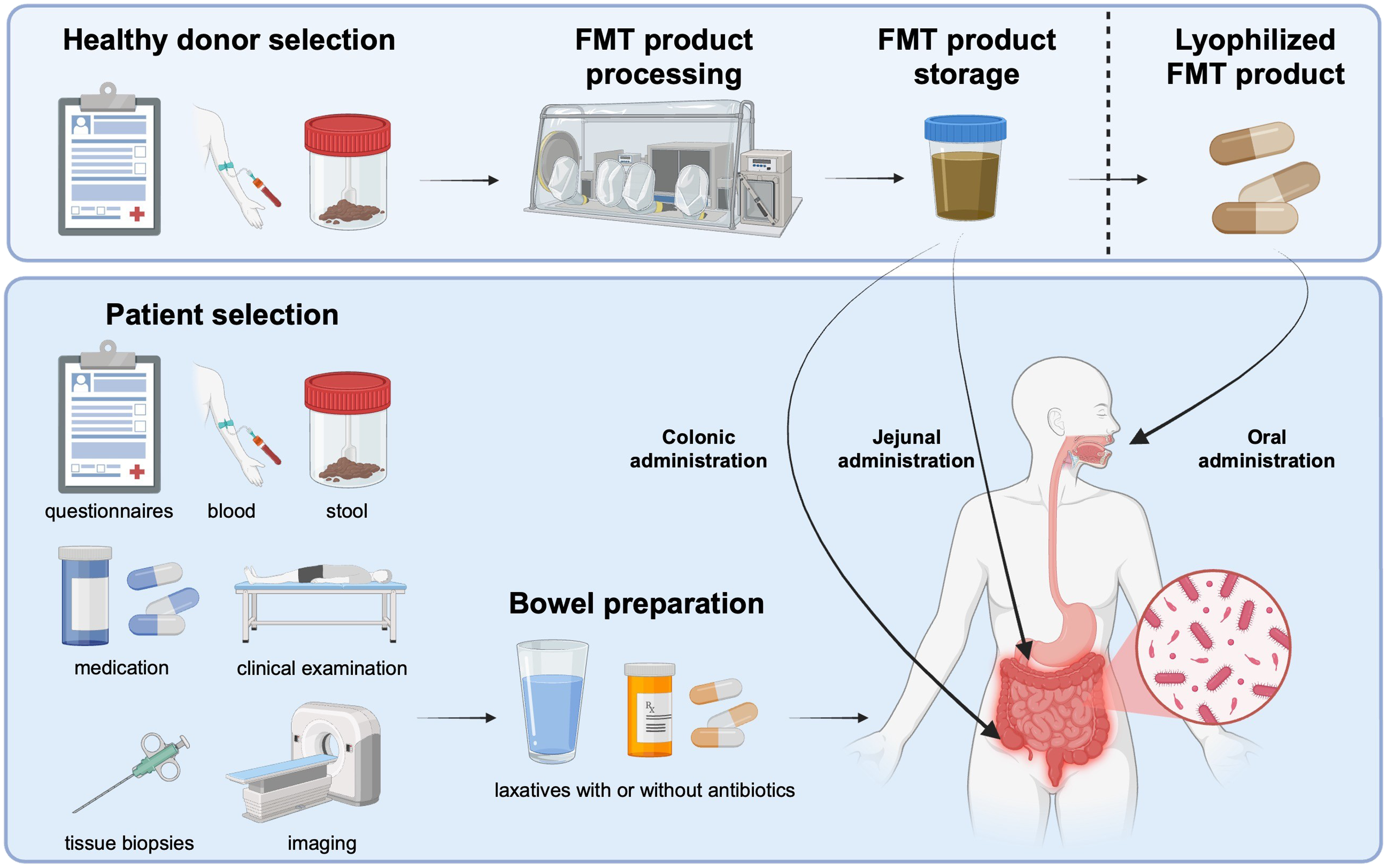
Methodological considerations in fecal microbiota transplantation. Figure was created in BioRender by Vandendriessche (2026): https://BioRender.com/u6spdqe.
A systematic search was performed until 08 March 2026 in PubMed and EMBASE using search terms including Parkinson's disease and fecal microbiota transplantation. Additional papers were found via references of the selected papers.
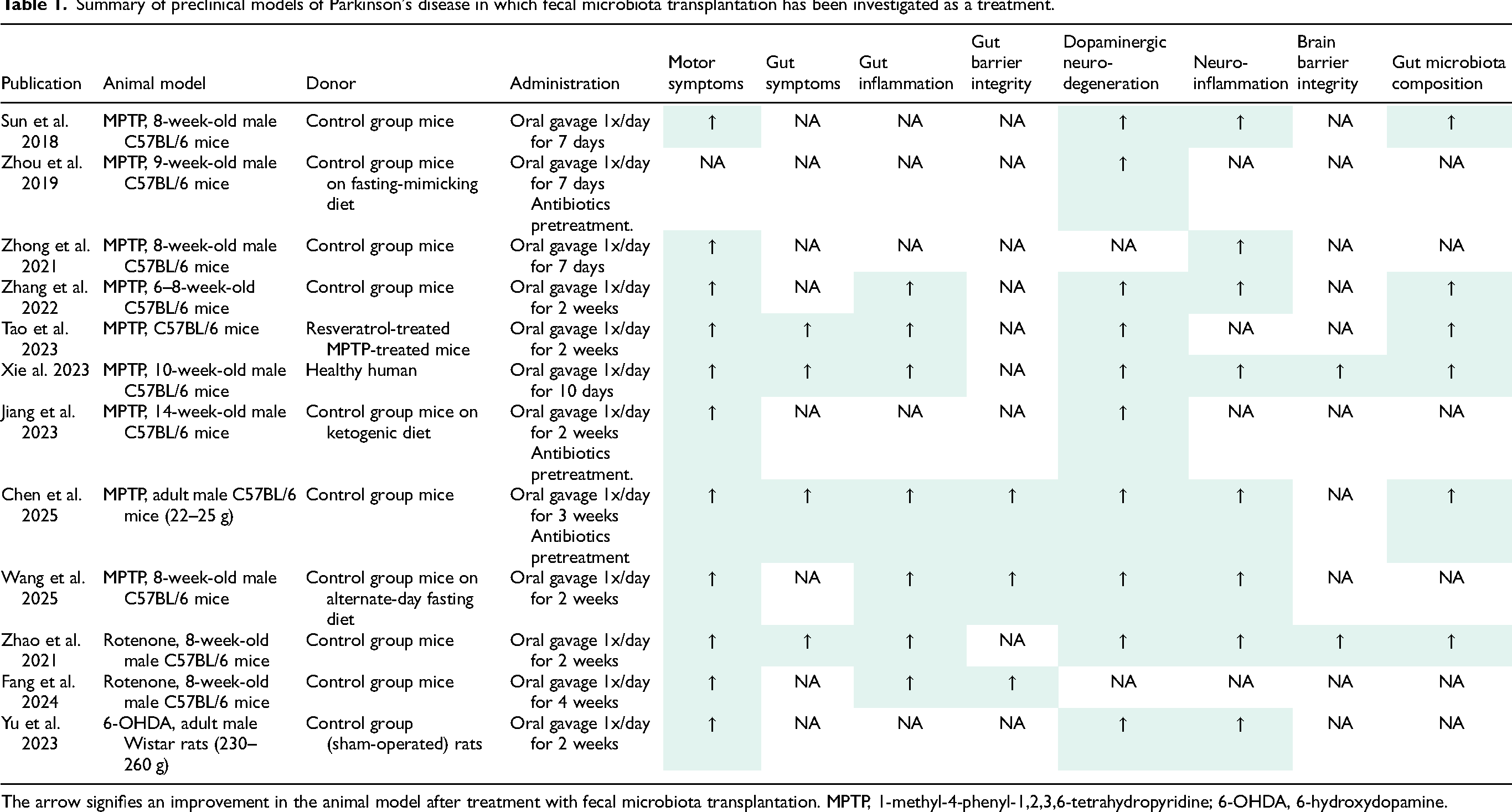
Table 1 summarizes the preclinical PD models where FMT was assessed as a treatment option.49–60 Several animal models showed improvement in both motor and nonmotor symptoms following FMT. At the level of the gut, there were also improvements in gut inflammation and gut epithelial barrier integrity, as well as in the composition of gut microbiota. More importantly, at the central nervous system there was a protective effect for dopaminergic neurodegeneration, neuroinflammation and the brain barrier integrity. Other preclinical studies have shown an exacerbation of symptoms and pathology after transplantation of human PD gut microbiota. In A53T α-synuclein transgenic mice, oral gavage with human PD patient gut bacteria led to an increase in intestinal inflammation, gut barrier dysfunction, neuroinflammation, α-synuclein aggregation and dopaminergic neurodegeneration. 61 Even in healthy wild-type mice, the transplantation of human PD stool led to motor symptoms, intestinal inflammation, gut and brain barrier dysfunction, and dopaminergic neurodegeneration when compared to transplanting healthy stool. 27
Summary of preclinical models of Parkinson's disease in which fecal microbiota transplantation has been investigated as a treatment.
Considering the evidence discussed above and the beneficial effects of microbiota modulation in preclinical models of PD, there is a growing interest in FMT as a potential treatment for PD. Table 2 shows the currently published clinical studies that investigated FMT as a treatment for PD. This includes two case reports,62,63 five open-label studies,64–68 and six placebo-controlled randomized clinical trials69–73 (RCT). All publications reported FMT to be safe and well-tolerated with adverse events limited to mild transient gastrointestinal symptoms such as abdominal discomfort, flatulence, and diarrhea. The case reports and open-label studies show positive effects on motor and nonmotor symptoms up to their final follow-up visit (range: 3–12 months) except for the open-label study by De Sciscio and colleagues. The latter study reports beneficial effects on daily off-time and nonmotor symptoms at 2 months post-FMT, which was not sustained at 6 months. 67 Here, we will focus on the results of the randomized clinical trials assessing the outcomes of FMT in PD.
Summary of the clinical studies investigating the effect of fecal microbiota transplantation in patients with Parkinson's disease.
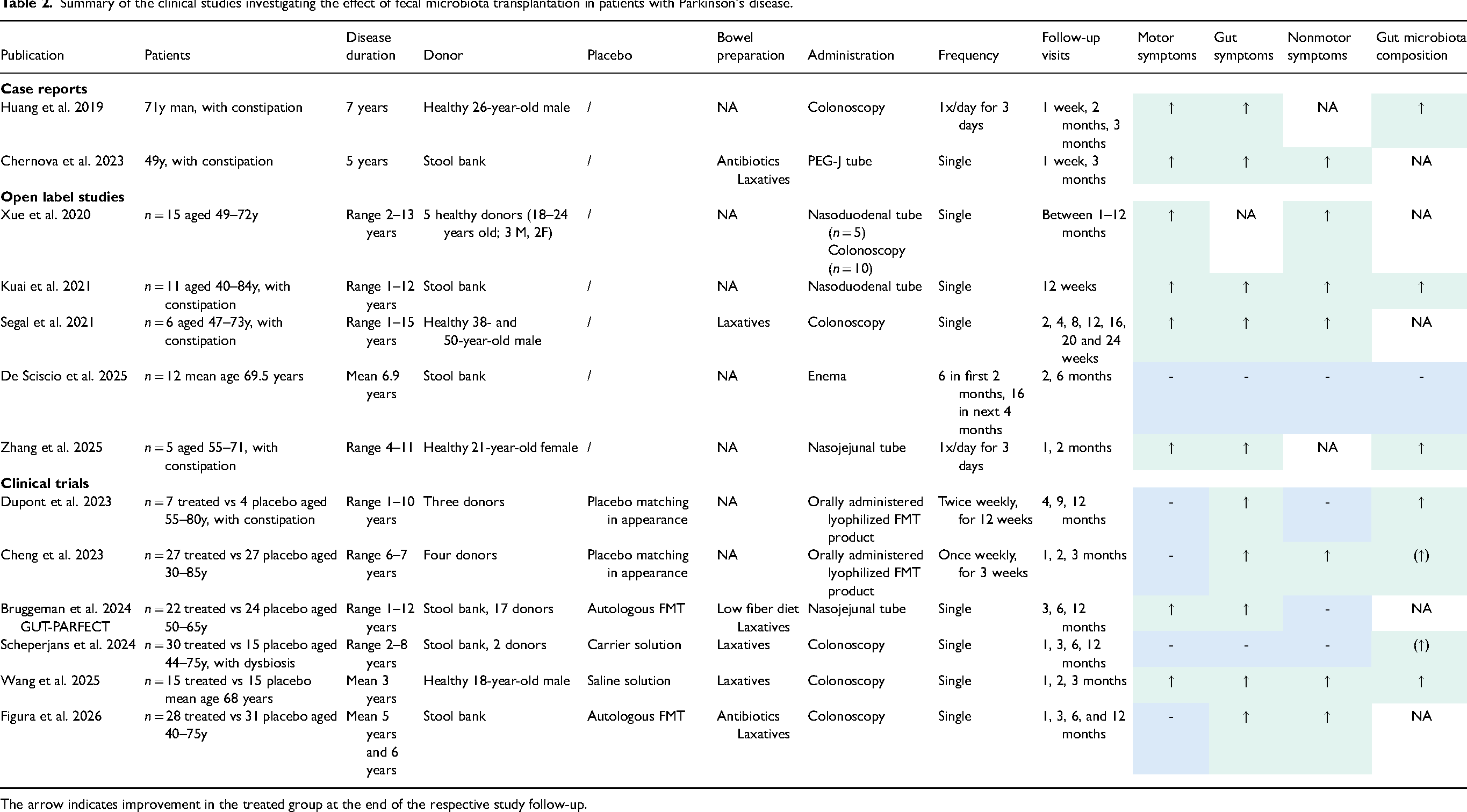
The arrow indicates improvement in the treated group at the end of the respective study follow-up.
Dupont et al. 2023 69 performed a randomized, double-blind, placebo-controlled clinical trial in the USA treating 11 mild-to-moderate PD patients with constipation with either an orally administered lyophilized FMT product or a matching placebo. The product was ingested twice weekly for 12 weeks and study visits were organised at 4, 9, and 12 months after starting the treatment. This trial assessed safety and gut microbiome changes as primary endpoints. Beta diversity of the gut bacteria was significantly increased in the active treatment group compared to the placebo group during treatment and 1 month after completing the treatment (4 months time-point). The treatment improved constipation, which was confirmed by objective measurements of gut transit and motility via SmartPill. Motor symptoms, scored via the Unified Parkinson's Disease Rating Scale (UPDRS) part 3 in an off-medication state, only showed transient improvement at 1 month in both the treated group (median reduction of 37.5%) and the placebo group (median reduction of 38%). Nonmotor symptom improvement was not found via the standardized questionnaires Geriatric Depression Scale (GDS), Parkinson Anxiety Scale (PAS), Non-Motor Symptom Scale (NMSS), Parkinson's Disease Questionnaire (PDQ-39).
Cheng et al. 2023 70 conducted a randomized, single-blind, placebo-controlled clinical trial in China treating 54 mild-to-moderate PD patients with either an orally administered lyophilized FMT product or a matching placebo. The product was ingested once weekly for 3 weeks and study visits were organised at 1, 2, and 3 months after starting the treatment. Primary endpoints at last study visit were changes in the Movement Disorders Society revision of the UPDRS (MDS-UPDRS), including total score and subscores of parts 1, 2, 3, and 4. A significantly larger decrease of the MDS-UPDRS total score was observed in the treated group at 3 months (group × time effect, B = −6.56, 95% CI −12.98 to −0.13, p < 0.05). Motor symptoms, scored via the MDS-UPDRS in an on-medication state, did not show significant improvement. The active treatment group exhibited significant improvements in gastrointestinal symptoms at 3 months as assessed by stool frequency (times per week) and dedicated questionnaires IBS-SSS, GSRS, and IBS-QOL. Additional significant improvements were found for scores on the Montreal Cognitive Assessment (MoCA). After 3 consecutive weeks of FMT or placebo intervention, the alpha and beta diversity in gut microbiota did not change significantly. However, several microbial species were notably altered in the active treatment group and showed positive correlations with the improvement of gastrointestinal and motor symptoms.
The GUT-PARFECT trial 71 was a randomized, double-blind, placebo-controlled clinical trial in Belgium treating 46 mild-to-moderate PD patients with either healthy donor stool or their own stool (placebo; autologous FMT). The FMT product was administered once via a nasojejunal tube and study visits were organised at 3, 6, and 12 months. The primary endpoint at last study visit was the change in the MDS-UPDRS motor score (MDS-UPDRS part 3) during an off-medication state. After 12 months, the MDS-UPDRS motor score significantly improved by a mean of 5.8 points (95% CI −11.4 to −0.2) in the active treatment group and by 2.7 points (−8.3 to 2.9) in the placebo group (p = 0.0235). The active treatment group showed significant improvements in the radiopaque pellets tests, which is an objective test for measuring colon transit time. 2 No significant changes were found for the other MDS-UPDRS scores, levodopa-equivalent daily dose (LEDD), and dedicated questionnaires for nonmotor symptoms (NMSS), quality of life (PDQ-39), constipation (Wexner constipation scale), depression (GDS), anxiety (PAS), apathy (Lille Apathy Rating Scale), sleep (Parkinson's Disease Sleep Scale), cognition (MoCA). The exception was a significantly worse fatigue in the active treatment group, as scored on the Parkinson's Fatigue Scale.
Scheperjans et al. 2024 72 performed a randomized, double-blind, placebo-controlled clinical trial in Finland treating 45 mild-to-moderate PD patients with gut dysbiosis with either healthy donor stool or a carrier solution (placebo). The FMT product was administered once via colonoscopy in the caecum and study visits were organised at 1, 3, 6, and 12 months. The primary endpoint at 6 months was the change in the MDS-UPDRS 1-3 (motor score in off), which did not differ between the groups (0.97 points, 95% CI −5.10 to 7.03, p = 0.75). No improvements were seen in the healthy donor group for gastrointestinal function as assessed by stool diaries and the radiopaque pellets test. Secondary outcomes and post-hoc analyses showed stronger increase of dopaminergic medication (LEDD) and better results for certain motor (timed-up-and-go test in off, MDS-UPDRS part 3 off axial score) and non-motor outcomes (NMSS, number of complete and spontaneous bowel movements) in placebo compared to active treatment group. While the active treatment induced stronger, donor dependent, microbiota changes, dysbiosis resolved more frequently after placebo.
Wang et al. 2025 73 conducted a randomized, double-blind, placebo-controlled clinical trial in China treating 30 mild-to-moderate PD patients with either healthy donor stool or saline solution (placebo). The fresh FMT product was administered once via colonoscopy and study visits were organised at 1, 2, and 3 months. The primary endpoint at last study visit was the change in the UPDRS 1-3, which is not reported clearly. The active treatment group showed a significant improvement of the UPDRS 3 scores from baseline to 3 months (group × time effect, B = −8.80, 95% CI −13.79 to −3.81, p < 0.05). In addition, the active treatment significantly improved constipation (complete spontaneous bowel movements and Bristol stool scale) and other nonmotor symptoms as assessed by UPDRS 2, NMSS, PDQ-39, Hamilton Anxiety Scale, Hamilton Depression Scale. Significant alterations were seen in the gut microbiota and fecal metabolites in the active treatment group.
Figura et al. 2026 74 performed a randomized, double-blind, placebo-controlled clinical trial in Poland treating 59 PD patients with either healthy donor stool or their own stool (placebo; autologous FMT). The FMT product was administered once via colonoscopy and study visits were organised at 1, 3, 6, and 12 months. The primary endpoint at last study visit was the change in MDS-UPDRS part 3 during an off-medication state, which did not differ significantly between groups (1.50 points, 95% CI −4.28 to 7.28, p = 1.00). The active treatment group did show significant improvements in MDS-UPDRS part 3 in an on-medication state, MDS-UPDRS part 2, MoCA, and MDS-NMS.
Outcome measures
Although safety was satisfactory, there was no reproducible and sustained efficacy across trials. However, direct comparison between the published studies is limited due to the differences in methodology. Furthermore, assessing the effect of a gut microbiota-modulating therapy is complicated by other factors that can influence the microbiome, such as diet and (dopaminergic) medication. The primary outcome measure most often used in PD studies worldwide is the (MDS-)UPDRS, particularly part 3 assessing motor symptoms in an off-medication state. However, most published FMT trials are underpowered to clearly investigate this. Moreover, a recent meta-analysis recommended a follow-up duration of at least one year to fully capture the treatment difference between placebo and intervention groups in PD. 75
Non-motor symptoms are typically assessed using standardized questionnaires, although more objective measures such as the radiopaque marker test provide greater accuracy. Across published randomized clinical trials, five out of six report improvements in gastrointestinal symptoms, including constipation, following FMT. In the GUT-PARFECT study, reductions in constipation were observed prior to improvements in motor symptoms, suggesting that restoration of gut function may precede and potentially facilitate subsequent neurological improvement. This is in agreement with previous clinical trials that showed that FMT treatment can relieve constipation symptoms in patients with idiopathic slow transit constipation both at short-term76,77 and long-term (1 year) follow-up. 78 There is a bidirectional association between colon transit time and gut microbiota perturbations with certain microbiota impacting gut motility. 23 Interestingly, a study with laxatives in PD patients showed a decrease in the worsening of rigidity. 79 Several randomized clinical trials report at least a temporary improvement of symptoms in the placebo group, underscoring the need for caution when interpreting findings from open-label studies. Notably, placebo groups typically undergo bowel preparation (eg, with laxatives), which may contribute to the observed placebo effects. Additional studies are therefore warranted to clarify the impact of laxatives on symptom profiles in PD.
Healthy donor selection
A strict protocol for selecting healthy donors is essential for safety, as well as allowing for reproducibility of clinical results.43,44 At the moment, it is still unclear what a ‘healthy’ microbiome entails, and thus it is even more unclear what the gut microbiome of a healthy donor should be in the context of PD. Post-hoc analyses of FMT trials are needed to investigate if some healthy donors induce better clinical effects than others, which is somewhat clearer for other indications such as inflammatory bowel diseases. 80 Interestingly, mice that were transplanted with gut microbiota from aged mice performed better on motor tests and exhibited less dopaminergic neurodegeneration after injection with MPTP, compared to transplantation with stool from young mice. 81 This raises the question if PD patients, who are often older, should be transplanted with gut microbiota from young healthy people.
Patient selection
All randomized clinical trials to date have included mild-to-moderate PD (Hoehn & Yahr stages 1–3), excluding patients in more advanced disease stages, where the potential for therapeutic benefit may be diminished due to greater neurodegeneration. Inclusion and exclusion criteria were designed to minimize confounding factors that could alter gut microbiota composition such as recent exposure to antibiotics or probiotics. A key unanswered question is whether patients should be preselected for FMT. Post-hoc analyses of published studies are warranted to identify responders and non-responders, along with their clinical and microbial profiles. Important considerations include whether to prioritize patients with constipation or specific gut microbial profiles, those with a body-first rather than a brain-first phenotype, or individuals with particular genetic backgrounds. Moreover, future studies could even consider prodromal PD, such as patients with idiopathic rapid eye movement sleep behavior disorder.
FMT procedure
The FMT procedure consists of several steps (Figure 2) that can be adapted as needed. Potential donors should go through a strict selection procedure including a medical interview and analyses of blood and stool to screen for infectious diseases, medication use, as well as comorbidities. Preparation of the FMT product starts with the collection of the stool sample by the healthy donor while preventing contamination. Time between stool collection and further processing should be kept to a minimum and during storage the sample should be kept cool and in an anaerobic environment. Anaerobic processing of the stool sample is considered essential to preserve anaerobic bacteria. 82 However, this practice is not yet part of standard FMT procedures, and its necessity in the context of FMT for PD remains uncertain. 83 The FMT product is most often stored frozen until use, however one open label study used fresh material that was transplanted within 5 h. 73 The orally administered lyophilized/freeze-dried FMT products are less invasive to use, however, the impact on microbial survival and effective engraftment is still unclear compared to the more classical ways of FMT administration. 84 While both nasojejunal and colonic FMT routes are equally effective for treating C. difficile infections, different considerations are warranted when trying to impact the gut-brain axis. Indeed, nasojejunal administration might be preferred for PD due to the significant role of the vagal nerve, which only innervates two-thirds of the colon. 85 Additionally, the higher engagement of the immune system in the small intestine might be relevant. 86 Furthermore, colonic FMT is less likely to alter gut microbiota composition in the small intestine compared to nasojejunal FMT. A disadvantage of nasojejunal administration is that it is technically challenging and less well tolerated. 87 In addition, the potential (negative) impact on small intestinal bacterial overgrowth should be considered. If targeting the microbiome of the upper gastrointestinal tract is essential, administering FMT products via enema would be less likely to induce positive effects. 67 However, paradoxically the open label study by Xue and colleagues found greater motor symptom improvements in the group receiving colonic FMT compared to the group receiving nasojejunal FMT. 64 Pretreatment with bowel lavage, and even antibiotic conditioning, may enhance engraftment. 88 The impact of laxatives post-FMT on the sustainability of the microbial engraftment and the clinical symptoms in PD, as discussed above, is still unknown. Finally, another topic of debate is the choice of placebo for which most studies use a saline or carrier solution, while in the GUT-PARFECT trial and the trial by Figura et al., the placebo group was treated with an autologous FMT, which has been shown to induce significant alterations in the gut microbiome. 89
Change in gut microbiota composition
Gut microbiota analyses in the current trials have largely relied on 16S rRNA sequencing, which provides only a broad overview of bacterial community composition and lacks strain-level resolution and functional insights obtainable through metagenomic sequencing. Understanding the functional output of the gut bacteria is critical for elucidating the mechanistic pathways through which FMT may exert therapeutic effects in PD. Confirmation of microbial engraftment is also essential, both to verify successful FMT and to determine whether and when repeat administrations may be necessary. 90 Although only a limited number of studies have assessed the gut microbiome one year after FMT, the available data indicate that microbial profiles remain similar to those of the healthy donors, suggesting that repeat FMT is not required within the first year post-treatment. 91
Mechanistic endpoints
If therapeutic benefits of FMT are confirmed, further investigation will be essential to elucidate the specific mechanisms by which the microbiota exert their effects. The development of more objective markers would help distinguish true clinical improvement from placebo responses. In particular, improved biomarkers for inflammation, gut and brain barrier integrity, neuronal cell loss and overall disease progression are needed. Importantly, FMT has been shown to induce remission of gastrointestinal inflammation in clinical trials for IBD, demonstrating its capacity to modulate immune and barrier functions.80,92 Moreover, several preclinical studies indicate that gut bacteria can influence the pharmacokinetics of levodopa, the gold standard medication for PD, highlighting an additional mechanism through which microbiota-targeted interventions may affect clinical outcomes.93–95 While the long-term hope is that microbiota-based therapies may ultimately contribute to disease-modifying therapies, this line of research may also lead to the optimization of dopaminergic treatments.
Future perspectives
Although FMT may appear straightforward at first glance, the procedure involves multiple critical decisions, and strict adherence to safety and methodological standards is essential. As a result, designing and executing an FMT trial is complex, time-consuming and challenging to fund, particularly given the limited interest from pharmaceutical companies. Greater consensus on trial methodology is needed to facilitate comparison across studies and to ensure that reported benefits can reliably be reproduced. Several FMT trials in PD are currently underway, reflecting growing interest in the field.96,97 There is a clear need for adequately powered, multi-centric clinical trials that include patients across a broader range of disease stages, incorporating a follow-up of at least 12 months, and integrating more mechanistic endpoints. Such endpoints should include patient profiling (clinical features and blood-based biomarkers related to inflammation, disease progression—such as extracellular vesicles—and levodopa pharmacokinetics), intestinal phenotyping (including assessments of gut inflammation, barrier integrity, and enteric α-synuclein aggregation), and detailed microbiome profiling (both compositional and functional analyses). These efforts will be essential for identifying patients most likely to benefit from FMT and for selecting optimal healthy donors, ultimately improving treatment efficacy in PD.
Looking ahead, FMT procedures are expected to evolve toward more targeted therapies, potentially involving defined microbial consortia rather than whole-stool preparations. The development of sophisticated biotherapeutic microbial cocktails or pharmacological strategies will become increasingly important, particularly if specific microbial or metabolic targets can be identified. Addressing these challenges represents a substantial but potentially transformative step toward reshaping therapeutic strategies for PD.
Take-home messages
FMT is being investigated as a potential treatment for neurological disorders, especially in Parkinson's disease.
All current trials show that FMT is a safe procedure Clinical response is variable (including positive effects in placebo groups) The differences in methodology make it difficult to compare studies. More consensus is needed. Optimized multicentric studies are needed, including mechanistic endpoints
There are still many open questions:
What is the best method for FMT administration? What makes an ideal donor? What makes an ideal acceptor/patient?
Footnotes
Ethical considerations
Not applicable
Consent to participate
Not applicable
Consent for publication
Not applicable
Funding
AB was supported by the Research Foundation Flanders (FWO) (1S47418N, 3S001918). Previous FMT in PD research of the authors was funded by support from the Flemish PD patient organizations (VPL and Parkili) and a grant from the Biocodex Microbiota Foundation (2019 National Research Grant). Future FMT PD research of the authors is funded by the Flemish Institute for Biotechnology (VIB), through the VIB Grand Challenges Projects.
Declaration of conflicting interest
The authors are investigators of the GUT-PARFECT trial. The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.