
Abstract
Background
In Parkinson's disease, abnormalities in reward-effort trade-offs are thought to underlie both apathy and bradykinesia. However, it remains unclear whether effort cost computations contribute to these symptoms independently of reward, and which exact effort costs are involved.
Objective
To assess whether effort-based decision-making in the absence of any explicit rewards differs between Parkinson patients and healthy controls and to explore whether putative differences are related to apathy or bradykinesia.
Methods
To address this, we developed a novel decision-making task that isolated physical effort costs from reward processing. Twenty-one Parkinson patients tested on and off dopaminergic medication, and 20 healthy participants, had to choose between two options that differed only in their requirements of force effort, either requiring larger total amounts of force or greater changes in force. We quantified participants’ preference for these different effort types and their sensitivity to changes in relative effort.
Results
Patients differed from healthy participants in both overall effort preference (P = 0.009) and sensitivity to changing efforts (P = 0.036), being more likely to choose options requiring overall lower force levels and more influenced by increasing requirements of changes in force. These effects were unaffected by dopaminergic medication. Importantly, sensitivity to increasing requirements for changes in force was associated with apathy (P = 0.004), but not bradykinesia.
Conclusion
Our findings suggest that, beyond well-known diminished responses to potential rewards, apathy in Parkinson's disease is related to aberrant effort cost computations, in particular those involving dynamic changes in movement, during decision-making.
Plain Language Summary Title
How effort influences decision-making in people with Parkinson’s disease and apathy
Plain Language Summary
Study purpose
Parkinson’s disease patients often present a slowing down of their movements, known as bradykinesia, as well as reduced motivation, described as apathy. One theory suggests that these may be related to how the brain weighs potential rewards against the required effort. However, it is unclear whether reduced sensitivity to reward or abnormal processing of necessary effort contributes to these symptoms or what kind of effort costs patients consider during movement.
The researchers’ approach
We developed a decision-making task relying solely on physical effort, independent of potential rewards. Participants repeatedly choose between two movement options differing only in the required effort; either to apply more force or to change the applied force to a larger extent. We quantified their preference for different effort types and sensitivity to changes in effort. Twenty-one patients with Parkinson’s disease were tested with and without their medication after 12 hours of withdrawal. These results were compared to 20 healthy controls who performed the procedure once.
What did we find?
Patients with Parkinson’s disease were more likely to avoid movement options that required increased physical effort, compared to the healthy controls. They also demonstrated greater sensitivity to increased requirement for changing the applied force. These effects were not altered by Parkinson’s medication, and were associated with a higher level of apathy, but not with the severity of bradykinesia.
What do the findings mean?
Our findings suggest that aberrant effort cost computations during decision-making, in particular those involving dynamic changes in movement are related to apathy, but not bradykinesia in Parkinson’s disease. This provides a better understanding of the mechanisms underlying different symptoms in Parkinson’s disease, which could lead to more precise treatment strategies.
Introduction
In everyday life, people constantly weigh whether the potential reward of an action is worth the associated effort. This can be conceptualized as optimization of utility, which is given by reward subtracted by effort. 1 Such trade-off between benefits and costs underlies many aspects of motivated behavior and has been shown to be altered in neuropsychiatric disorders such as Parkinson's disease (PD).2–10 PD is clinically defined by motor impairment including the hallmark symptom of slow movement - termed bradykinesia - but many patients suffer from debilitating ‘non-motor’ symptoms including apathy – a lack of motivation.2,11 Previous research in PD has shown that apathy may be linked to reduced reward sensitivity, whereas bradykinesia might be more closely related to abnormal effort computations.2,4–6,12–14 For example, when offering patients options with varying levels of rewards and efforts (typically tested by different levels of isometric grip force), PD patients with apathy are not incentivized by lower rewards suggesting diminished reward sensitivity. 2 A recent study found that PD patients with apathy showed reduced reward sensitivity and were less likely to accept offers with higher effort costs, which was related to structural changes in prefrontal cortico-basal ganglia ciruits. 15 Studies of bradykinesia show that patients are able to perform normal movement except from an abnormal movement duration, which could be explained by an increased sensitivity to effort costs.12,14 Indeed, it has been proposed that patients with PD move slowly due to an implicit, i.e., unconscious, unwillingness to exert effort. 14 Interestingly, PD patients are impaired in changing the applied force (either increases or decreases), e.g., during relaxation of grip force,16,17 suggesting that not only absolute force levels but also changes in force constitutes an effort cost in PD. 13 Thus, previous studies suggest that PD patients express abnormal reward and effort sensitivity, which might differently relate to, respectively, apathy and bradykinesia.
However, as a limitation of previous studies, apathy has been investigated in decision-making studies (typically requiring a choice between two options), while bradykinesia is studied in motor control frameworks (typically analysing movement execution). Thus, an alternative hypothesis differentiating mechanisms underlying apathy and bradykinesia is that both are related to abnormal utility computations; apathy in the context of abnormal decision-making and bradykinesia in the context of motor execution. To disentangle the role of abnormal effort computations during decision-making in bradykinesia and apathy we developed a novel effort-based decision-making task where PD patients on and off dopaminergic medication, as well as healthy participants, repeatedly chose between two options that differed only in their physical effort requirements in the absence of any external rewards, see Figure 1. One option required maintaining a higher level of grip force (termed Increase), whereas the alternative option required lower levels of force but larger changes in force (termed Decrease). This design was based on the observation that PD patients are not only impaired in exerting larger levels of isometric force, but also in changing the applied force even during relaxation of grip force.16,17
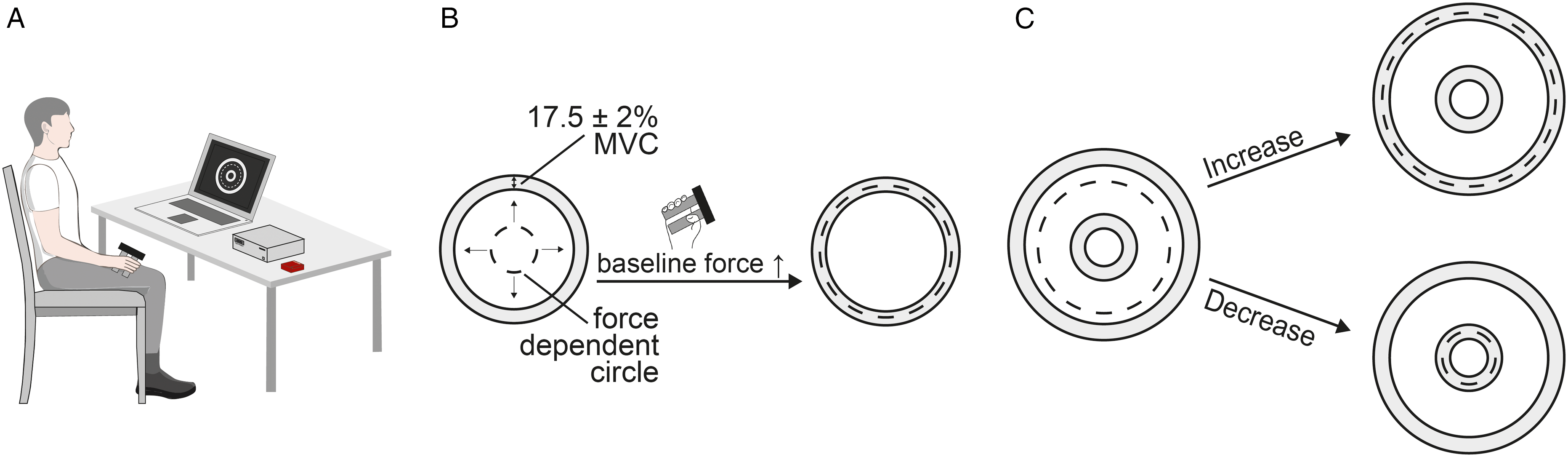
Experimental task. (A) An overview of the experimental setup. (B) During the initiation phase patients had to produce and maintain a certain baseline force (17,5% ± 2% MVC) indicated by a white ring. The exerted force was shown by a dotted ring with larger forces increasing this ring. If participants failed to reach the target baseline force after 10 s the trial was considered invalid. (C) The decision phase was initialised after participants maintained the target baseline force for 0.5 s (dotted line within the white target ring) and was preceded by brief black screen (0.5 s ± 0.25 s jitter) in which participants were instructed to maintain the baseline force. Patients had to choose between two options (Increase shown above, Decrease shown below) by moving the exerted force (dotted line) into the target ring and hold this force for 1 s.
Across trials, we systematically varied the difference between these two effort types (termed Effort-ratio; higher effort ratios indicate larger requirement for reductions in force compared to the overall force level) and analyzed how this affected participants’ choices. Using logistic regression, we estimated which option participants were more likely to choose and how strongly each participant's choices were influenced by changes in the effort ratio. We examined whether PD patients differed from healthy controls and whether this might be affected by dopaminergic medication. Finally, we explored how alterations in effort-based decision-making were related to apathy and bradykinesia, to better understand the mechanisms underlying deficits in motivation and motor control in PD.
Materials and methods
Ethics statement
All participants gave written informed consent to participate in the study, which was approved by the local ethics committee (State Medical Association of Rhineland-Palatinate, nr 2023-17242).
Sample size
There were no previous studies testing decision-making isolating physical effort costs in PD, which did not allow us to conduct a formal power analysis. Previous studies investigating effort costs during motor control or reward sensitivity during decision-making in PD had a sample size of ∼10–20 patients.4,5,12,14 We deemed a sample size of ∼20 PD patients appropriate given the need for dopamine withdrawal and associated discomfort for patients.
Participants
For this study, 23 patients with PD and 20 neurologically healthy participants were recruited from the Neurology Department at the University Medical Centre of Johannes Gutenberg University, Mainz, Germany. Exclusion criteria for patients were treatment with deep brain stimulation, intrajejunal or subcutaneous pump therapies, severe tremor prohibiting patients from using the dynamometer and clinically diagnosed dementia. Two patients of the 23 patients were excluded from the study due to incorrect calibration of the dynamometer resulting in a patient group of 21 (Supplementary Table 1) and a control group of 20 participants. Of the 21 patients, three patients performed only the ON measurement, and one patient only performed the OFF measurement (treated as missing data in the hierarchical regression model, see below). The healthy group was matched to the patient group regarding age (PD: mean 64.5 years, range: 58–72; HC: mean 61,9 years, range: 53–71; P = 0.289, independent samples t-test) and sex (7 female in PD group, 12 female in HC group, P = 0.122, Fisher's exact test). Patients’ motor symptom severity was assessed using the Movement-Disorder-Society-Unified Parkinson's Disease Rating Scale (MDS-UPDRS) Part III once on dopaminergic medication (ON) and once after overnight (12 h) withdrawal of dopamine (OFF). Bradykinesia scores were extracted as sum of items 3.4 to 3.8. As expected, motor impairment was significantly alleviated by dopaminergic medication (MDS-UPDRS-III OFF: 25.3 ± 10.7, ON: 16.9 ± 9.0, t = 4.698, P < 0.001, paired samples t-test). All participants were assessed using the Apathy Evaluation Scale (AES). Since this evaluation assesses symptoms over the last four weeks it was completed only once.
Experimental task and design
An overview of the experimental task and design is given in Figure 1. The tasks were presented on a Windows 11 laptop using PsychoPy 18 (version 2025.1.1). Participants’ force was measured using a dynamometer (MIE Medical Research, Leeds, UK), analogue-to-digital converted and transmitted to PsychoPy using a Labjack module (Labjack Corporation, Lakewood, CO, USA). To account for inter-individual variability in strength, at the beginning of each measurement the maximum voluntary contraction (MVC) was determined for all participants by performing three maximum voluntary contractions and force computed as percentage to the highest value (% MVC). MVC did not differ between PD patients on and off medication as well as healthy controls (all P > 0.05, t-tests) as expected, since PD is characterized by movement slowness, not weakness. The experimental task was designed to assess how PD patients assess effort costs during decision-making and comprised 60 trials each consisting of two main phases (Initiation and Decision phase, Figure 1). In the Initiation phase, participants had to exert a consistent baseline force (17,5% ± 2% MVC), indicated by a white ring, for 0.5 s (Figure 1B). The exerted force was shown by a dotted ring with larger forces increasing this ring. If participants failed to reach the target baseline force after 10 s the trial was considered invalid. After a brief black screen (0.5 s ± 0.25 s jitter) in which participants were instructed to maintain the baseline force the decision phase was initialised. During the Decision phase participants had to choose between two different movement options and adjust the initial force accordingly to the chosen target ring and maintain this force for 1 s. While one movement option required an increase in the sustained baseline force (termed Increase), a higher change in force to a lower level of force was required for the alternative option (termed Decrease), see Figure 1C. We chose these two effort costs (higher exerted force vs. higher change in force), since PD patients show deficits both in increases and decreases in force 13 and since subthalamic activity, which is abnormally modulated in PD,19,20 has been related to both effort costs.21–23 Participants were instructed to choose the movement option they perceived to require the least effort and underwent a short training session prior to the recordings to try out different movements beforehand. Patients were explicitly asked if they understood the task after the training session and the examiner made sure that participants sampled the different options (instead of always choosing the same option) prior to commencement of the recordings. If the participants did not choose an option within 5 s the trial was considered invalid, and the visual feedback “too slow” (German: “zu langsam”) was displayed (only 4.7% of all trials were invalid suggesting that choices were not affected by accuracy constraints). Otherwise no feedback was given. Both rings were linked to target values based on a specific percentage of MVC, with at least a 2% MVC distance to the baseline ring. Similar to studies in neuroeconomics varying reward ratios to infer utility, the relation between effort costs varied systematically across six levels with the Decrease option increasing its distance from the baseline circle compared to the Increase option in increments of 2% MVC, thus increasing the change in force that was required for reaching the circle. Both Increase and Decrease included a 2, 4, 6, 8, 10 and 12% change in force (6 possibilities for Increase and for Decrease) from the baseline of 17.5% MVC. Since the Decrease option had to be higher or equal to the Increase option (otherwise the Decrease option would both require lower overall force levels and smaller changes in force), the 12% Decrease option could be combined with a 12, 10, 8, 6, 4, or 2% Increase option, but the 10% Decrease option could only be combined with 10, 8, 6, 4, or 2% Increase option, etc. Thus, the minimum ratio was 1 and the maximum ratio was 6. We fixed the different pairs so that each combination (Decrease required the same change in %MVC, required 2%MVC more change compared to Increase, 4%MVC more change, 6%MVC more change, 8% more change or 10% more change) was presented 10 times resulting in 60 trials in total. The order of these combinations was randomized but kept constant across participants. The different possible cue combinations are illustrated in Figure 2. We also recorded kinematic data from participants’ response for analyzing how quickly participants increased (termed yank) and decreased their force (termed negative yank) when choosing either option.
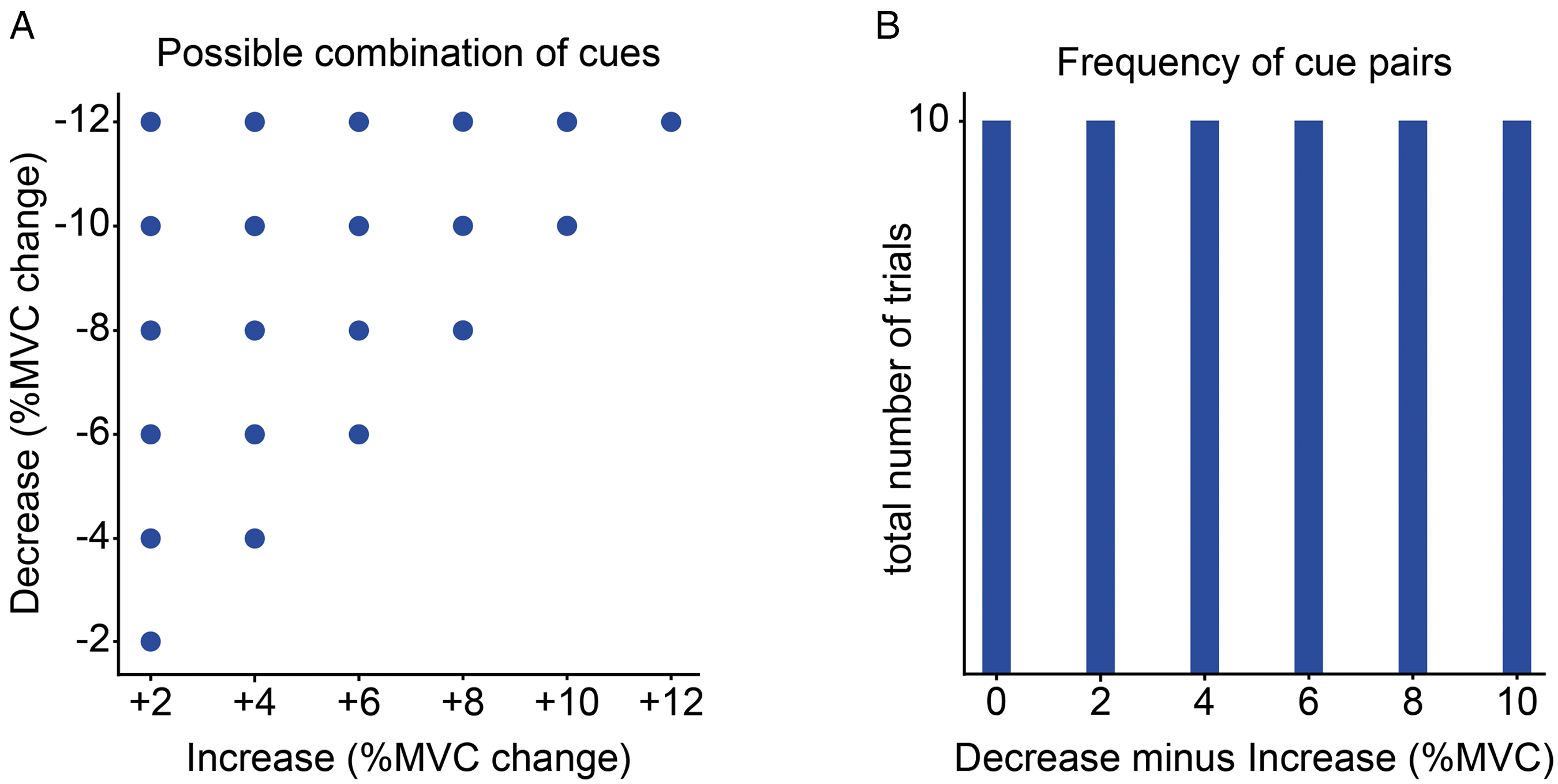
Possible cue combinations. (A) illustrates the possible combinations of the Decrease (y axis) and Increase (x axis) option. Both options ranged from 2 to 12% MVC change from the baseline force. (B) The possible differences between the Decrease and the Increase option ranged from 0-10% MVC, which were presented with equal probability. Of note, the Increase option could only be equal or less compared to the Decrease option. The different cue combinations resulted in a ratio between options that ranged from 1 (where both options had equal distance) to 6 (where Decrease required 6 times the change in force compared to Increase). The order of cue combinations was randomized but kept constant across participants.
Individual trials were separated by a short intertrial break. The duration of this break was adjusted so that short decision durations resulted in longer breaks so that the overall duration was fixed across participants. Average trial duration was 12 s resulting in a duration of 12 min for the whole recording. The patient group performed the recording once after overnight (12 h) withdrawal of their dopaminergic medication (OFF) and once on their normal dopaminergic medication (ON). The ON-OFF order was randomized and counter-balanced.
Statistical analysis
The statistical analysis was performed using generalized mixed-effects models (hierarchical regression) implemented in RStudio (v2025.09.1 + 401). The model included a random intercept, and fixed effects of Group (PD, healthy) and Effort-ratio (six levels). The dependent variable (choice) was binary, and models were fitted using a binomial distribution with a logit link function. PD patients ON vs. OFF medication were compared in a separate model including the factor Medication instead of Group, since healthy participants did not receive any medication. For testing putative effects of apathy scores (AES) and bradykinesia, we entered these as independent (continuous variables) into the model containing patients off medication (since AES was only assessed once) and included the interactions AES*Effort-ratio as well as bradykinesia*Effort-ratio. Analyses based on aggregated data were performed using t-tests for continuous data (age, MVC, AES, UPDRS, yank, negative yank) and Fisher's exact test for binary data (sex). The significance level was set to α = 0.05 (two-tailed). All scripts (R) for statistical analyses and illustrations, as well as compiled anonymized data (csv) are freely available on figshare: https://doi.org/10.6084/m9.figshare.32051271
Results
We investigated two main aspects of effort-based decision-making. First, whether participants generally preferred one effort cost over the other (reflected by an increased likelihood to choose the respective option) and second whether participants were sensitive to changes in effort costs (reflected by an increasing choice likelihood of the Increase option with increasing requirement of a change in force for the Decrease option; i.e., the slope of the regression). Based on a recently proposed framework of abnormal effort computations in PD, 13 we hypothesized that patients would be more sensitive to increases in requirements for changes in force compared to healthy people and explored whether this was more closely related to apathy or bradykinesia.
Analyzing participants’ choice behaviour we found a strong main effect of Effort-ratio (z = 5.193, P < 0.001), since participants were more likely to choose the Increase option if the Decrease option required an increasingly larger change in force (even though the required force level was lower). We also found a significant main effect of Group with patients being generally more likely to choose the Decrease option (z = 2.623, P = 0.009) and a significant interaction Effort-ratio*Group indicating that sensitivity to changes in the effort costs was different in patients compared to healthy people (z = −2.096, P = 0.036). Post-hoc tests showed that this interaction was driven by patients basing their choices on changes in the effort that they had to expend (i.e., an increasing likelihood of choosing the Increase option if the Decrease option required an increasingly larger change in force; main effect of Effort-ratio in ON: z = 4.198, P < 0.001; in OFF: z = 3.626, P < 0.001), while this was not the case in healthy participants (z = 1.372, P = 0.170), see Figure 3A and B. There was no effect of medication (z = 1.122, P = 0.262) or medication*Effort-ratio interaction (z = 0.252, P = 0.801). Results were identical regarding significance of effects when using the difference of force rather than their ratio (e.g., an 8% decrease vs. a 2% increase in force reflects a difference of absolute force change of 6, and a ratio of 4). We also controlled for putative order effects (whether the ON or OFF session was tested first), e.g., driven by practice effects, which did not show any effects of condition order (z = 0.358, P = 0.720). In addition, the differences were unlikely to be due to task difficulty or accuracy, since participants were unable to reach the target force in only 4.7% of trials and the number of invalid trials was not different between PD patients ON and OFF medication and healthy participants (all P > 0.05). Thus, PD patients showed marked differences in effort-based decision-making compared to healthy people, both regarding the type of effort costs they generally preferred and their sensitivity to changes in the effort costs that had to be expended. These differences were not affected by acute changes in dopaminergic medication and were unlikely to be due to practice effects or accuracy constraints.
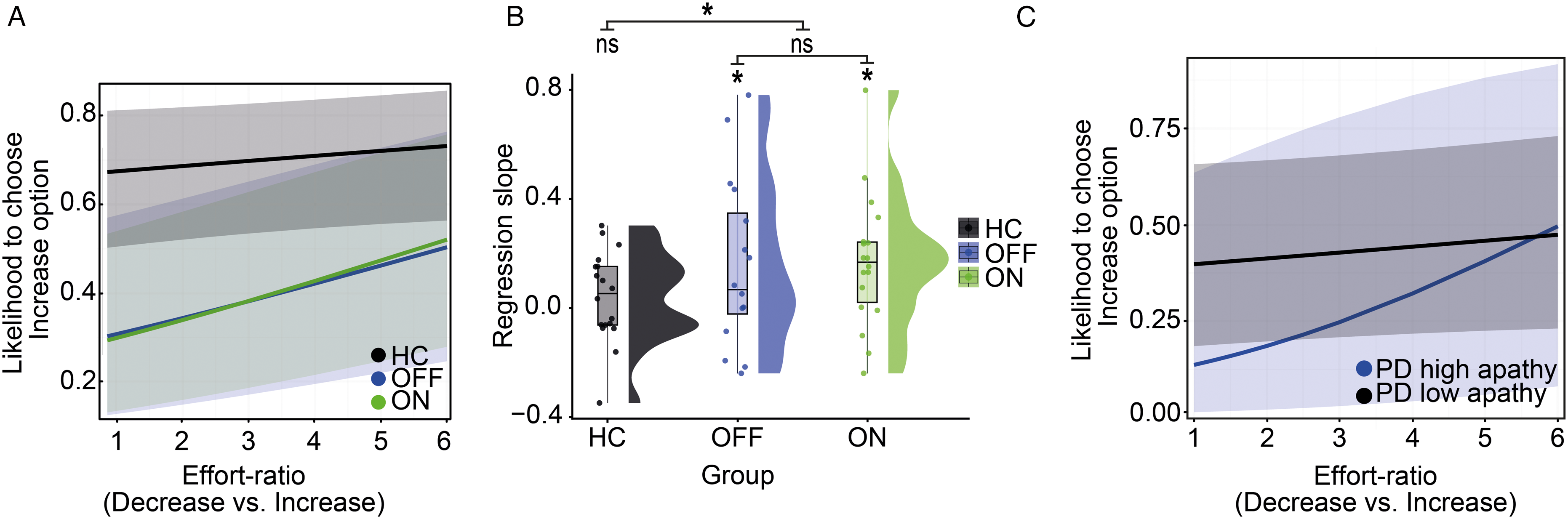
Behavioral results. (A) Predicted probability of choosing (binary) the Increase option (requiring an increase from the baseline force) as a function of effort-ratios (i.e., the Decrease option requiring larger reductions in force ranging from 1 (both options with same distance from the baseline circle) to 6 (Decrease option 6* further away from the baseline circle compared to the Increase option) for the three tested groups (healthy control = HC, in black; patients off dopaminergic medication =OFF, in blue; patients on dopaminergic medication = ON, in green) from a generalized mixed-effects model using a binomial distribution with a logit link function. Shaded areas represent 95% confidence intervals. (B) For visualization purposes raincloud plots were computed showing individual slopes of each participant (dot plot, distribution, mean and standard deviation; grey =healthy participants, blue =patients off dopaminergic medication, green = patients on dopaminergic medication). Of note, these values were derived from individual, i.e., non-hierarchical, logistic regression models, since effort-ratio was modeled as fixed effect in the hierarchical model. Data from two participants in each group are missing, since in these participants individual models could not be computed (due to insufficient data for one of the options). Results are visualized by the asterisks for significant (P < 0.05) and “ns“ for non-significant. (C) Same as A, but after dividing the patient group (off medication) into a low (black) and high (blue) apathy group after a median split. Results showed significant effort sensitivity in the high apathy group (P = 0.001), while there was no significant effect for patients with low apathy scores (P = 0.244). Shaded areas represent 95% confidence intervals.
In line with previous studies,5,6 patients in our cohort did not only show motor impairment, but also had significantly higher apathy scores compared to healthy people (t = 2.952, P = 0.006, independent samples t-test). Thus, the observed difference in effort-based decision-making between patients and healthy people might be due to apathy or to motor impairment. To disentangle these two possibilities, we entered patients’ bradykinesia as well as apathy scores into the generalized mixed effects model. We found a significant interaction between apathy scores and Effort-ratio (z = 2.942, P = 0.003), but not between bradykinesia and Effort-ratio (z = −0.409, P = 0.682), nor any main effects of bradykinesia or apathy scores on patients’ choice preferences. Again, results were identical regarding significance of effects when using the difference of force rather than their ratio (see above). Furthermore, control models containing total MDS-UPDRS-III, tremor or rigidity scores instead of bradykinesia scores showed highly similar results (all statistical results are listed in Supplementary Table 2). We also analyzed the kinematics of force adjustments, which showed that patients expressed slower changes in force, in particular regarding decreases in force (termed negative yank) and, less pronounced, for increases in force (termed yank) when choosing an option (negative yank: OFF vs. HC: t = 2.929, P = 0.006; ON vs. HC: t = 2.730, P = 0.010; ON vs. OFF: t = 0.571, P = 0.572; yank: OFF vs. HC: t = 1.706, P = 0.097; ON vs. HC: t = 1.724, P = 0.094; ON vs. OFF: t = 0.085, P = 0.933). These kinematic changes were not related to apathy (negative yank: rho = −0.045, P = 0.865; yank: rho = 0.268, P = 0.298).
Post-hoc analyses of patients’ behaviour during decision-making separating patients into a high apathy vs. low apathy group using a median split showed significant effects of Effort-ratio in the high apathy group (z = 3.228, P = 0.001), which was significantly different compared to healthy participants (z = −3.342, P < 0.001), while the low apathy group did not express sensitivity to changing effort costs (z = 1.164, P = 0.244), which was similar to that observed in healthy people (z = −0.129, P = 0.897), see Figure 3C. Thus, sensitivity to changing effort costs, but not patients’ general preference for choosing options with lower force levels, was related to apathy and could not be explained by differences in motor function.
Discussion
Apathy is a debilitating symptom in neuropsychiatric and neurodegenerative disorders such as PD and has been linked to abnormal utility computations.2–6 In particular, a reduced sensitivity to rewards has been demonstrated in PD patients suffering from apathy,4–6 while abnormal effort computations have mainly been linked to bradykinesia.12–14 It has been suggested that both bradykinesia and apathy could be viewed as abnormal computations of utility costs, with diminished reward responses reflecting apathetic symptoms and abnormal effort computations driving bradykinesia. 13 Interestingly, PD patients do not only show deficits in the production of overall force levels, but also in changes of force even if this would result in lower force levels, e.g., during grip force relaxation,16,17 which we also observed in our current study. However, physical effort is rarely studied independently from reward, and apathy and bradykinesia have mainly been studied in separate fields (decision-making vs. motor control). Here, we demonstrate that PD patients show marked alterations in effort-based decision-making even if no extrinsic reward is present. We found that patients, but not healthy participants, showed sensitivity to changes in the exact effort that they had to expend, so that they were more likely to increase the exerted force when the other option required increasingly larger changes in force, even though this would have required overall lower force levels (i.e., relaxation of the exerted grip force). This finding is in line with our a-priori hypothesis that PD patients express abnormal effort computations related to dynamic movement (i.e., changes in movement such as relaxation of isometric force16,17 or halting of movements 24 ) based on previous behavioural studies investigating motor execution. 13 Importantly, we found that this effort sensitivity reflected apathy rather than bradykinesia when studied in a decision-making framework. Thus, for disentangling mechanisms underlying apathy and bradykinesia the functional domain (decision-making or motor execution) might be more critical than the specific focus of utility computation, i.e., whether it pertains to effort or reward. In line with this, a recent study found that PD patients with apathy are less likely to accept offers with low rewards and offers requiring high effort, thus expressing abnormal reward and effort processing. 15
We also found a strong group effect in that healthy participants generally preferred the Increase option. At first glance, this might seem counterintuitive, since, as noted above, patients were more affected by required changes in the applied force levels. One possible explanation is that, for healthy individuals without motor deficits, the effort costs were perceived as relatively minor and therefore exerted less influence on their choices. The required force levels ranged from ∼ 5% to 30% MVC, and while in patients the range of choice probability was centred around the indifference point (at which each option was chosen with equal likelihood, see Figure 3A and C), this range may have been insufficient to elicit comparable sensitivity in healthy participants who do not express any motor symptoms. Furthermore, we did not find any correlations between overall effort preference and clinical symptoms suggesting that apathy is more closely related to sensitivity to changes in effort costs rather than general effort preference.
In contrast to previous studies testing reward-effort trade-offs4–6,25 we did not find any effects of dopaminergic medication. This could suggest that dopamine is more closely related to reward processing than effort computations.26,27 In real-world scenarios different options typically do not only comprise different effort costs but are also related to some sort of reward. Thus, while our novel task allowed us to assess physical effort costs in the absence of rewards, this might be less ecologically valid compared to reward-effort trade-offs tested in previous studies. Alternatively, the overnight (12 h) withdrawal might not have been sufficient, since the majority of the included patients received dopamine agonists (Supplementary Table 1), which has a longer half-live than levodopa and has been shown to alleviate apathy (albeit less pronounced than its beneficial effect on bradykinesia)28,29 or by the long duration response of levodopa. 30 This could be addressed in future studies with longer dopamine withdrawals that optimally combined several paradigms testing reward and effort sensitivity separately in the same patient group. Such studies should optimally also comprise larger samples, since, while the sample size of the current study was similar to previous work, the statistical power for detecting interaction effects and inter-individual variability might have been insufficient.
This study focused on the effects of physical effort costs on decision-making in PD. Another important effort cost to consider during decision-making is cognitive effort. Previous studies have demonstrated that similar reward-effort trade-offs pertain to cognitive requirements of tasks, which are also affected in PD patients with apathy.31,32 In our study, reaching the target ring of the Decrease option might have been perceived as more effortful because of increased accuracy constraints requiring increased attentional motor control. Thus, unlike previous studies, the current task assessed decision-making related to motor control mechanisms and beyond mere physical effort this might also have comprised attentional and other resources. Task performance might also be affected by patients’ cognitive abilities to understand task instructions. To address this, all patients performed a training session to familiarize themselves with the task, which was kept as simple as possible, and the width of the target rings of both options had the same width (2% MVC) minimizing differences in accuracy constraint. We did not find any changes in accuracy for both options, with overall very low error rates (<5% of trials). Future studies could address this more directly by comparing options with different requirement for attentional control and motor accuracy, and by including standardized cognitive assessments.
Taken together, our study demonstrates abnormal effort-based decision-making in PD even in the absence of extrinsic rewards and suggests that abnormal effort cost computations, in particular those involving dynamic changes in movement, are linked to apathy. These results inform future studies of motor control and decision-making regarding the effort costs that should be considered and contribute to a better understanding of the mechanisms underlying distinct symptoms in PD, which might help refining treatment strategies tailored to individual symptoms.
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X261457805 - Supplemental material for Abnormal motor control effort costs in Parkinson's disease patients with apathy
Supplemental material, sj-docx-1-pkn-10.1177_1877718X261457805 for Abnormal motor control effort costs in Parkinson's disease patients with apathy by Johannes Schönhals, Moaz Al Ajia, David Meder, Gabriel Gonzalez-Escamilla, Nils Schröter, Sergiu Groppa and Damian M Herz in Journal of Parkinson's Disease
Supplemental Material
sj-docx-2-pkn-10.1177_1877718X261457805 - Supplemental material for Abnormal motor control effort costs in Parkinson's disease patients with apathy
Supplemental material, sj-docx-2-pkn-10.1177_1877718X261457805 for Abnormal motor control effort costs in Parkinson's disease patients with apathy by Johannes Schönhals, Moaz Al Ajia, David Meder, Gabriel Gonzalez-Escamilla, Nils Schröter, Sergiu Groppa and Damian M Herz in Journal of Parkinson's Disease
Footnotes
ORCID iDs
Ethical considerations
All participants gave written informed consent to participate in the study, which was approved by the local ethics committee (State Medical Association of Rhineland-Palatinate, nr 2023-17242).
Consent to participate
All participants gave written informed consent to participate in the study.
Consent for publication
Not applicable
Author contributions
DMH and DM conceptualized and designed the experiments. DMH and SG supervised the research project. JS and MAA recruited the participants and conducted the experiments. DMH and JS prepared the manuscript and created the visual data representation. MAA, DM, GGE, NS and SG critically reviewed and revised the final manuscript. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Deutsche Forschungsgemeinschaft, Parkinsonforeningen, Deutsche Gesellschaft für Parkinson und Bewegungsstörungen, Danmarks Frie Forskningsfond, Lundbeck Foundation, (grant number 565021148, A1311, 1052-00054B, R336-2020-1035).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.