
Abstract
Background
The endocannabinoid system (ECS) is important for several neurophysiological functions, including the regulation of emotions and cognitive processes. The most abundant brain cannabinoid receptor is cannabinoid receptor type 1 (CB1R). Several preclinical studies in Parkinson's disease (PD) models suggest that modulating CB1R may impact cognitive processing. However, there are very limited studies of the relation between CB1R and cognitive processing in PD patients.
Objective
To explore the relationship between CB1R availability and cognitive dysfunction in PD with [18F]FMPEP-d2 positron emission tomography (PET).
Methods
A total of 23 individuals with PD underwent [18F]FMPEP-d2 PET to measure cerebral CB1R availability. Cognitive symptoms were evaluated using a standardized neuropsychological test battery covering various cognitive domains, such as episodic and working memory, executive functioning, language function, visuospatial function and attention, and were correlated with CB1R availability using voxel-wise regression analysis corrected for multiple comparisons using false discovery rate (FDR) at p < 0.01.
Results
PD patients with poorer performance in episodic memory tests showed lower CB1R availability, particularly in the cingulate, temporal, and visual cortices, and thalami. Also, PD patients with poorer executive functioning showed lower CB1R availability predominantly in the insulae, caudate nuclei, thalami, brainstem, and temporal cortices. No relationship was found between CB1R availability and language function, visuospatial function, or working memory capacity.
Conclusions
Decreased CB1R availability in PD patients is correlated with episodic memory impairment and executive dysfunction, suggesting that the ECS has a role in the pathophysiology of cognitive symptoms in PD.
Plain language summary title
Problems with Episodic Memory or Executive Functions are Related to Disturbances in Endocannabinoid System Functioning in Parkinson's Disease
Plain language summary
Why was the study done? The endocannabinoid system (ECS) is a network that helps regulate several brain functions like learning and memory, motor control, sleep and mood. The ECS involves endocannabinoids and type 1 cannabinoid receptors (CB1R). It has been observed that the ECS is not functioning properly in many neurodegenerative diseases, including Parkinson's disease (PD). However, it is not fully understood what symptoms the ECS dysfunction causes in PD.
What did the researchers do? The research team studied the relationship between brain ECS functioning and cognitive functions, such as memory, executive functioning, language function, visuospatial function and attention, in PD. The ECS functioning of the brain was evaluated with positron emission tomography (PET) which is an imaging technique that can measure different body functions in real time. [18F]FMPEP-d2 PET tracer binds to CB1R, providing information about CB1R availability in one’s brain.
What did the researchers find? Twenty-three subjects with PD underwent [18F]FMPEP-d2 PET and extensive neuropsychological testing. PD patients who performed poorly in episodic memory tests or executive function tests had lower CB1R availability in related brain areas. Instead, the performance in language or visuospatial functioning tests or working memory capacity did not have a relationship with CB1R availability.
What do the findings mean? PD patients with decline in episodic memory or problems with executive functions have decreased CB1R availability. The results have implications for the development of new treatments for Parkinson's disease.
Keywords
Introduction
Parkinson's disease (PD) is characterized by dopaminergic hypofunction in the basal ganglia, which is considered to lead to typical motor symptoms of PD. 1 However, PD is increasingly considered a multisystem neurodegenerative disease including also various non-motor symptoms, such as sleep and autonomic nervous system disturbances, anxiety, depression, and psychiatric symptoms.2–4 In addition, a broad spectrum of cognitive symptoms, ranging from mild cognitive impairment in PD (PD-MCI) to PD dementia (PDD, has been described. 5
The endocannabinoid system (ECS) is a widespread neuromodulatory system that plays an important role in various neurophysiological functions, such as motor control, 6 synaptic plasticity, 7 and neurodevelopment, 8 but also in cognitive processes 9 and the regulation of mood 10 and emotions. 11 Type 1 cannabinoid receptors (CB1R) are the most abundantly expressed cannabinoid receptors in the brain and are found in high densities particularly in the basal ganglia.12,13
Various pre-clinical studies suggest that cannabinoid agonists impair working memory and long-term memory formation, whereas cannabinoid antagonists and inverse agonists may enhance learning and memory. 14 Additionally, cannabinoid receptor activation is shown to decrease anxiety and have antidepressant activity. 15
So far, only one clinical study has investigated the relationship between CB1R availability and cognitive and behavioral symptoms in human PD. Decreased [18F]MK9470 binding in subjects with PD correlated with disturbances in executive functioning, episodic memory, speed and mental flexibility, and visuospatial functioning. No relationship was found between CB1R availability and mood or behavioral symptom scores. 16
We have previously studied the ECS in vivo in subjects with idiopathic PD using positron emission tomography (PET) and [18F]FMPEP-d2, an inverse agonist radioligand with a high affinity and selectivity for the CB1R. We showed that subjects with PD had lower CB1R availability compared to healthy controls, 17 and that gait, postural instability, and rigidity in PD were associated with lower CB1R availability, whereas tremor or bradykinesia were not. 18
This study aimed to further examine the ECS disturbances in PD in vivo by investigating the relationship between CB1R availability and cognitive symptoms in PD using [18F]FMPEP-d2 PET.
Methods
The study was approved by the Ethics Committee of the Hospital District of Southwest Finland and was conducted according to the World Medical Association Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects) and following Good Clinical Practice guidelines. All participants gave their written informed consent obtained according to the declaration of Helsinki.
Study population
The study sample consisted of 23 subjects with PD (Table 1). Recruited participants fulfilled the UK Brain Bank Research criteria for the diagnosis of idiopathic PD. To confirm the clinical diagnosis of PD, all the participants underwent also [18F]FDOPA high-resolution research tomograph (HRRT) PET examination to ensure typical nigrostriatal dopaminergic hypofunction characteristic for PD. All subjects were on their individual standard antiparkinsonian medication. The details on the dopaminergic medication for each subject are presented in Supplementary Material. None of the participants were using hormone replacement therapy or any kind of cannabis products. This study is part of a larger research project for which patients with PD were recruited through an open advertisement in a patient magazine, as well as through notices posted on bulletin boards at neurology clinics within the Hospital District of Southwest Finland. The exclusion criteria have been described previously. 17
Demographic and clinical characteristics of participants.
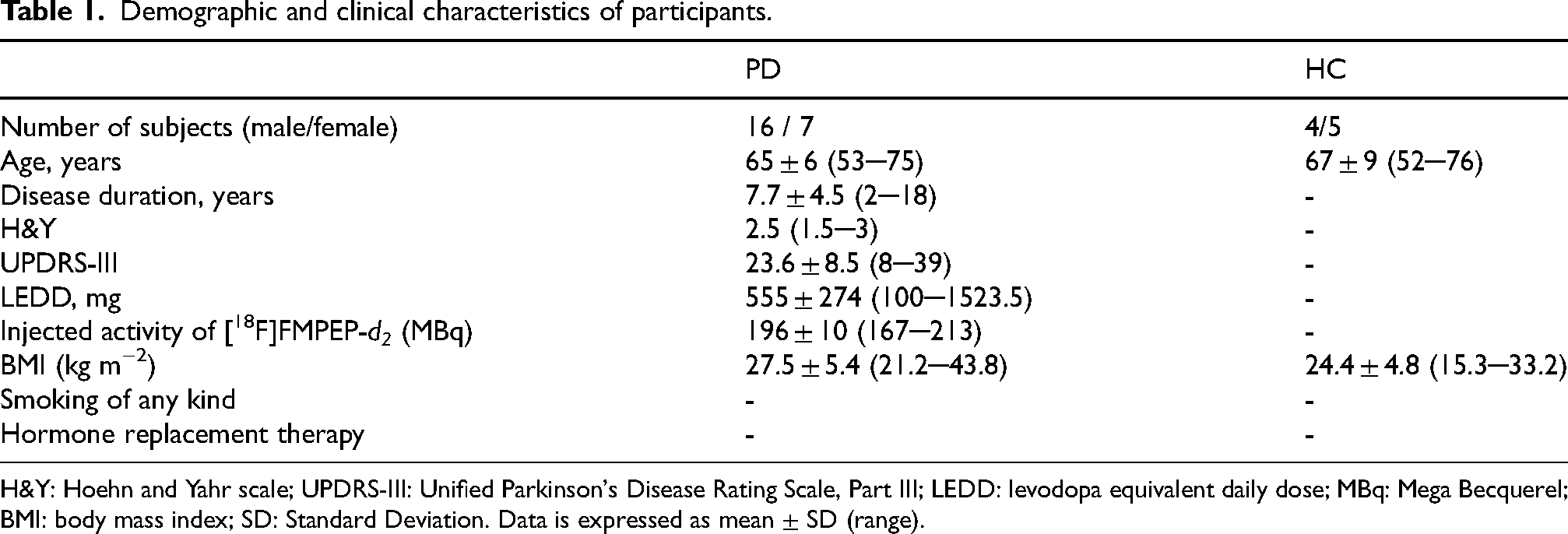
H&Y: Hoehn and Yahr scale; UPDRS-III: Unified Parkinson's Disease Rating Scale, Part III; LEDD: levodopa equivalent daily dose; MBq: Mega Becquerel; BMI: body mass index; SD: Standard Deviation. Data is expressed as mean ± SD (range).
In the current study, we focused on the relationship between neuropsychological test performance and CB1R availability. Because the neuropsychological evaluation was conducted under medication, the study sample included participants who also had [18F]FMPEP-d2 imaging performed while on medication. The study population consisted of the same participants as in our two previous studies,17,18 with the exception of one subject who only had an [18F]FMPEP-d2 scan done off antiparkinsonian medication. In addition, the sample included 8 participants, who only had an [18F]FMPEP-d2 done on medication, that were not included in previous studies.
Subjective cognitive symptoms were not specifically assessed during screening. Instead, cognitive status was determined based on the neuropsychological evaluation conducted in this study. However, considering the overall study protocol that was quite demanding and heavy for the participants, those with more severe cognitive or motor symptoms were unlikely to volunteer.
A group of 9 healthy subjects were used as control group (HC) for neuropsychological symptoms (Table 1).
Evaluation of neuropsychological symptoms
Cognitive and neuropsychological symptoms were evaluated using a standardized neuropsychological test battery covering various cognitive domains, such as episodic memory, executive functioning, language function, visuospatial function, visuomotor speed, and working memory. Specifically, we used Mini-Mental State Examination (MMSE) as a measure of general cognitive functioning. To assess functioning in specific cognitive domains the following 12 tests were used: Episodic memory functions: Logical memory I and II tests from Wechsler Memory Scale -Revised (WMS-R) and CERAD (Consortium to Establish a Registry for Alzheimer's Disease) Wordlist learning (sum of three trials). Language functions: Semantic fluency (vegetable fluency, 60 s) and the Similarities subtest from Wechsler Adult Intelligence Scale-Revised (WAIS-R). Executive functions: The difference in time taken to complete Trail Making Test Part B minus Part A (TMT B-A; set-shifting cost), the difference in time taken to complete Stroop inhibition minus Stroop color naming (Stroop inhibition-naming; inhibition cost), Phonemic fluency (letter S, 60 s) and Alternating fluency (animal and furniture, 60 s).Working memory: The Digit span subtest from WAIS-R was used. Visuospatial functions: The Block design subtest from WAIS-R was used. Visuomotor speed: The Digit Symbol subtest from WAIS-R was used. In addition, Geriatric Depression Scale (GDS) was used to assess possible depressive symptoms. One of the subjects did not undergo MMSE or CERAD Wordlist learning.
Determination of PD-MCI status
PD-MCI status was determined by using Level 1 criteria by Litvan et al. (2012). 19 MCI was operationalized as two or more out of 12 tests falling below −1.5 SD of the mean score in the control group.
Cerebrospinal fluid (CSF)
Providing a CSF sample was part of an optional sub-study. Of the 23 participants, 15 provided a CSF sample. CSF samples were centrifuged and aliquoted before being stored at −80 °C and transferred to the Clinical Neurochemistry Laboratory, University of Gothenburg, on dry ice. Alzheimer's disease (AD) biomarkers of amyloid beta 1–42 (Aβ42), total tau (tTau), and phosphorylated tau (pTau) were measured using the Elecsys® βAmyloid (1–42), Elecsys® Total-Tau (tTau) and Elecsys® Phospho-Tau (181P) CSF assays.
Radiochemistry
[18F]FMPEP-d2 was prepared as described previously. 20 The radioligand was obtained in high radiochemical purity (> 95%) and had a molar activity of 200 ± 15 MBq/nmol at the time of injection.
Imaging procedures
Structural magnetic resonance imaging (MRI) was performed with a 3 T scanner (Philips Ingenuity TF PET/MR, Philips Medical Systems, Cleveland, OH, USA) and utilized in the analyses as described previously. 17 The [18F]FMPEP-d2 examinations were performed with a HRRT PET scanner (Siemens/CTI, Knoxville, TN, USA) as described previously 17 for a total emission data scan range of 0–60 and 90–120 minutes. Concomitant blood sampling was performed as described previously. 17
PET imaging analyses
PET data processing and kinetic modelling was carried out as described previously. 17 The voxel level [18F]FMPEP-d2 distribution volume (VT) images, calculated with Logan's method within a 30–120 min period, were normalized to MNI152 space using clinical toolbox, 21 and spatially smoothed using a 8 mm full width at half maximum Gaussian filter. Details of imaging procedures and analyses are provided also in Supplementary Material.
Statistical analyses
Statistical analyses were performed using SPM12 software (Statistical Parametric Mapping, Wellcome Trust Centre for Neuroimaging, London, UK) running in MATLAB (The MathWorks, Natick, MA). Associations between [18F]FMPEP-d2 VT and with different neuropsychological test scores were investigated with multiple regression. No grand mean scaling or global normalization was done. An explicit mask was used. Levodopa daily equivalent dose (LEDD) was set as a covariate. All results were corrected at the voxel level for multiple comparisons using false discovery rate (FDR) at p < 0.01 and the cluster extent threshold was set such that only significant clusters were displayed. To control multiple comparisons for the large number of tests, p-values were adjusted using the Benjamini-Hochberg method. An FDR of q < 0.05 was considered significant. The statistical patterns were visualized using MRIcroGL software (https://www.nitrc.org/projects/mricrogl).
Conventional statistics were performed with IBM SPSS Statistics program (version 27). Shapiro-Wilks's test and visual inspection of Q–Q plots were used to test the normality assumption. Outcomes of neuropsychological assessments between PD and HC groups were compared using two-sample t tests or non-parametric Mann-Whitney U tests as appropriate. Correlations between different neuropsychological test scores and age, sex, disease duration, Hoehn and Yahr (H&Y) scale and Unified Parkinson's Disease Rating Scale Part III (UPDRS-III) were assessed with Pearson's r correlations or Spearman's rho as appropriate.
Results
Outcomes of neuropsychological assessments are summarized in Table 2. No significant differences between the PD and HC groups were observed in any of the cognitive tests. Three PD subjects were defined as PD-MCI. None of the controls fulfilled the MCI criterion.
Results of neuropsychological assessments in participants. Means and SDs in healthy controls, 1.5 SD and the gold-standard −1.5 SD cut off for impairment, and means and SDs in subjects with PD.
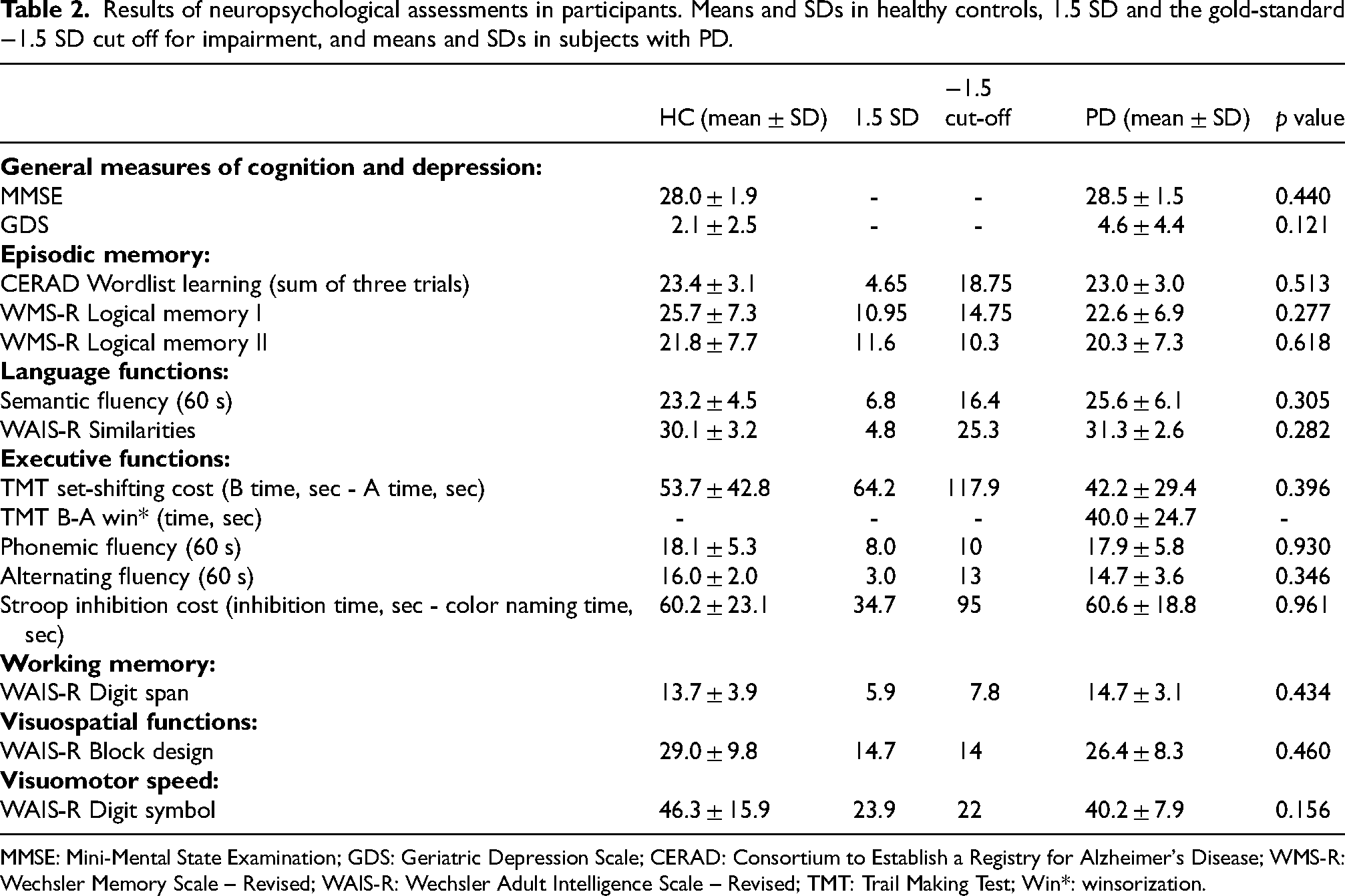
MMSE: Mini-Mental State Examination; GDS: Geriatric Depression Scale; CERAD: Consortium to Establish a Registry for Alzheimer's Disease; WMS-R: Wechsler Memory Scale – Revised; WAIS-R: Wechsler Adult Intelligence Scale – Revised; TMT: Trail Making Test; Win*: winsorization.
PD patients with poorer performance in episodic memory showed lower CB1R availability primarily in the cingulate, temporal, and visual cortices and thalami (Figure 1). More specifically, a statistically significant positive correlation was observed between [18F]FMPEP-d2 VT and WMS-R Logical memory I. Two clusters (p < 0.001, Tpeak−level = 5.07, kE = 166 177, q = 0.006; p = 0.007, Tpeak−level = 4.75, kE = 42 916, q = 0.008) comprised of thalami, temporal cortices, cingulate cortices, orbitofrontal cortices, primary visual cortices, and visual association cortices. Also, a statistically significant positive correlation was observed between [18F]FMPEP-d2 VT and WMS-R Logical memory II. A cluster (p < 0.001, Tpeak−level = 5.12, kE = 288 007, q = 0.002) comprised of cingulate cortices, temporal cortices, dorsolateral prefrontal cortices, primary visual cortices, precunei, lingual gyri, and right thalamus. Additionally, a statistically significant positive correlation was observed between [18F]FMPEP-d2 VT and CERAD Wordlist learning. A cluster (p = 0.01, Tpeak−level = 4.03, kE = 54 481, q = 0.01) comprised of primary and secondary visual cortices, lingual gyri, cerebellum, brainstem, inferior temporal gyri, and right hippocampus and parahippocampal gyrus.
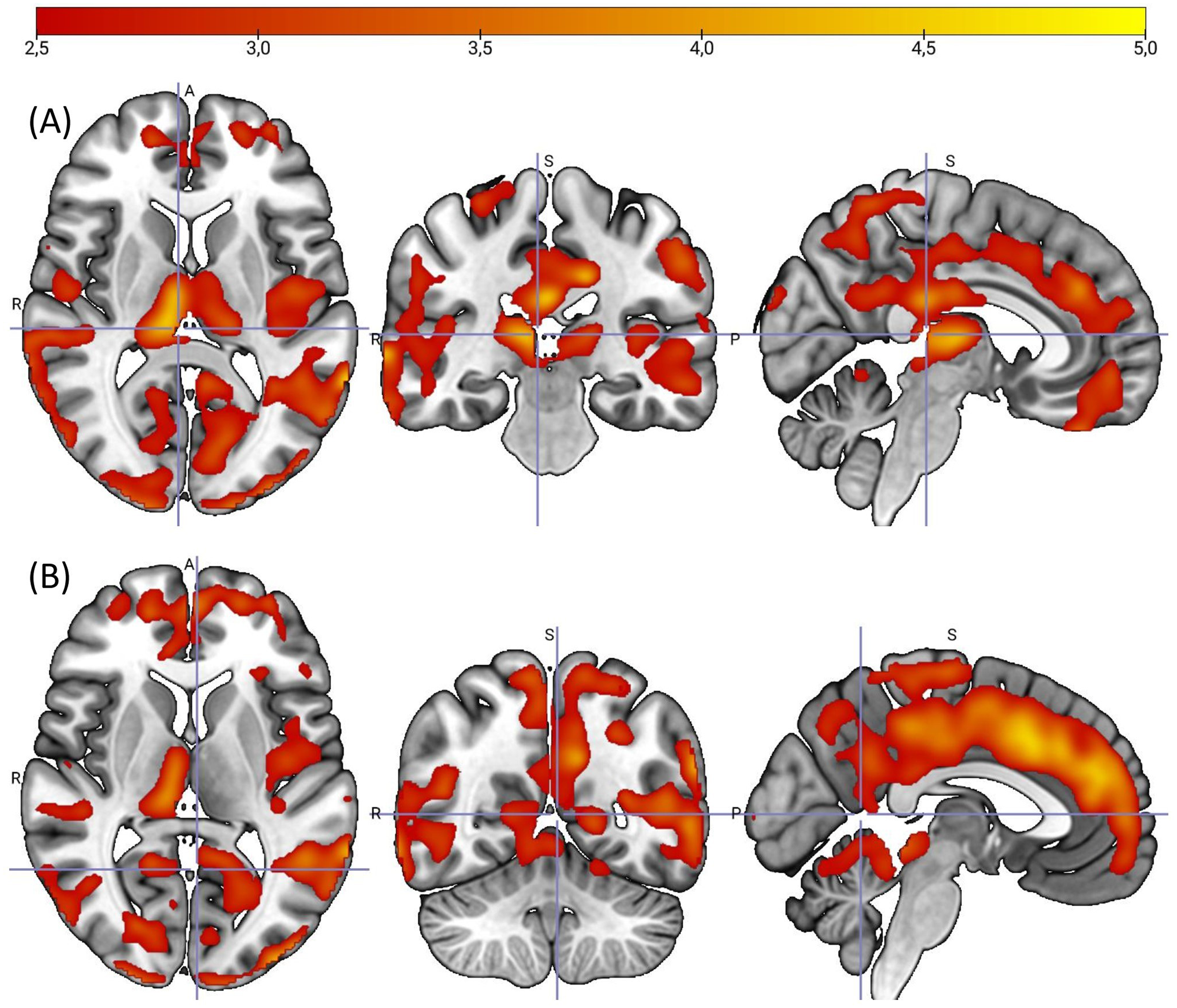
Whole-brain statistical parametric mapping analysis shows positive correlation between type 1 cannabinoid receptor availability (distribution volume) and WMS-R logical memory I (A) and II (B) tests in subjects with Parkinson's disease. Color bar represents t value, which corresponds to the level of significance at the voxel level. A, Anterior. P, Posterior. S, superior. R, right.
PD patients with poorer executive functioning showed lower CB1R availability in several brain regions (Figure 2). Specifically, a statistically significant negative correlation was observed between [18F]FMPEP-d2 VT and TMT B-A. A cluster (p < 0.001, Tpeak−level = 5.11, kE = 229 035, q = 0.004) comprised insulae, caudate nuclei, thalami, brainstem, lingual gyri, and predominantly right temporal cortex. TMT B-A score had one extreme outlier value (132, z-score > 3) that was winsorized, to correspond to the next highest value (83, z-score < 2) in the dataset before the statistical analysis to reduce the confounding effect. Without the winsorization, the results were almost the same. The main difference was that without the winsorization the significant cluster was larger (p < 0.001, Tpeak−level = 6.23, kE = 397 421) and also covered most of the cingulate cortices.
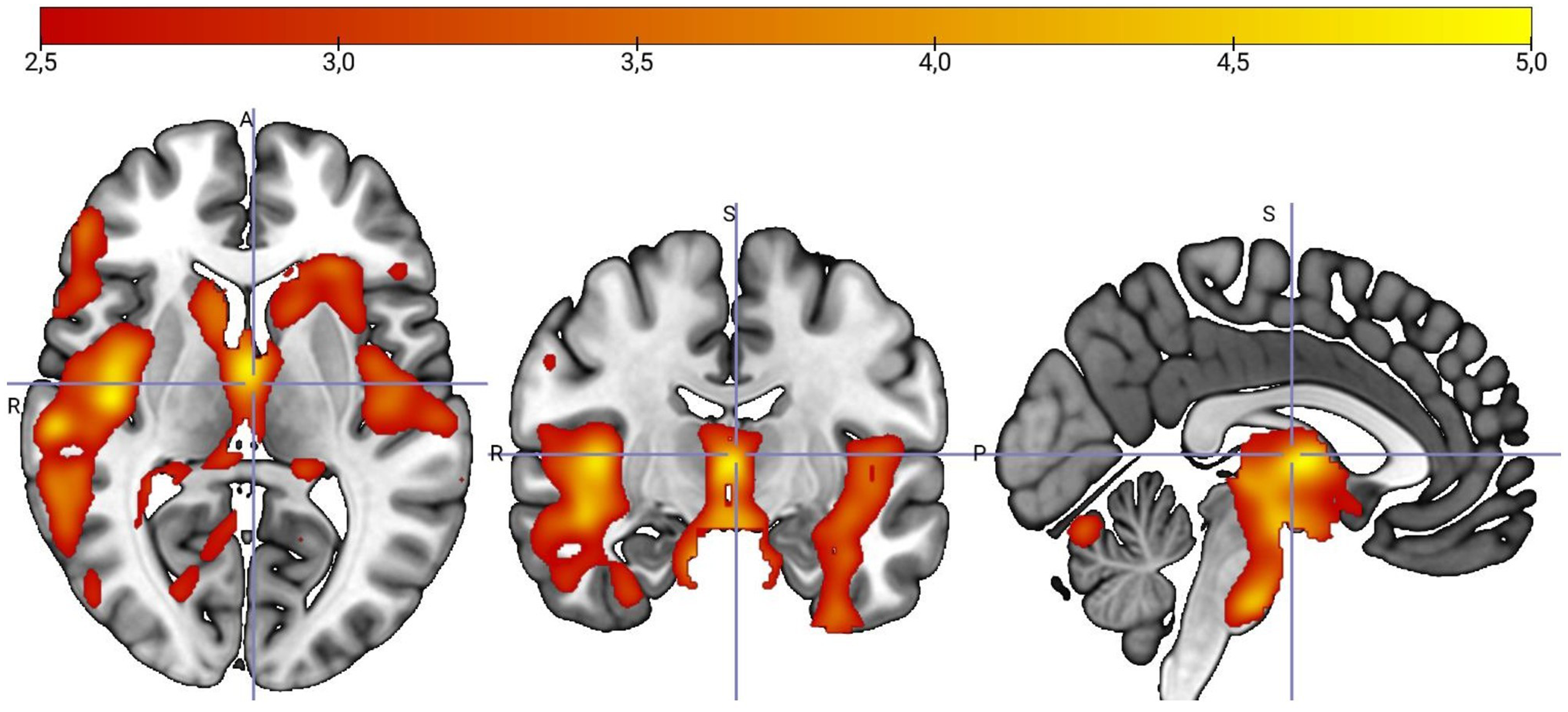
Whole-brain statistical parametric mapping analysis shows negative correlation between type 1 cannabinoid receptor availability (distribution volume) and the difference in time taken to complete Trail Making Test Part B minus Part A (TMT B-A) in subjects with Parkinson's disease. Color bar represents t value, which corresponds to the level of significance at the voxel level. A, Anterior. P, Posterior. S, Superior. R, Right.
Following FDR correction, all the above results remained significant. Results were also essentially replicated using correction for partial volume effects. Details of supplementary analyses are provided in the Supplementary Material.
No relationship was found between [18F]FMPEP-d2 VT and GDS, MMSE, Stroop test, Alternating fluency, Phonemic fluency, Animal Semantic fluency, or WAIS-R Digit Symbol, Block design, Similarities or Digit span scores. Additionally, age, sex, disease duration, H&Y scale or UPDRS-III score did not correlate with any of the neuropsychological test scores.
CSF biomarkers
One of the 15 participants that provided a CSF sample had all three AD biomarkers (Aβ42, tau, and p-tau) abnormal, and four had two abnormal AD biomarkers (Aβ42 and either tTau or pTau). Due to the small subsample, reliable correlation analyses between CSF biomarkers and neuropsychological test scores or [18F]FMPEP-d2 VT could not be studied.
Discussion
We found that PD patients with lower CB1R availability, particularly in the cingulate cortex, temporal cortex, thalamus, and primary and secondary visual cortices, had worse performance in episodic memory measures. Also, PD patients with poorer executive functioning in TMT B-A showed decreased CB1R availability predominantly in the insula, caudate nucleus, thalamus, brainstem, and temporal cortex. These results provide further evidence for ECS dysfunction in the cognitive symptoms of PD.
Already in the early stages of PD, around 40% of patients present MCI in multiple domains,22,23 with deficits being most prominent in the domains of memory and executive functions.23,24 Increasing evidence also suggests that MCI seen in the early stages of the disease might also be a powerful predictor of subsequent dementia progression.25,26 However, the neurochemical and neuropathological bases of cognitive deficits of PD is not fully understood, including theories of nigrostriatal dopamine denervation, noradrenergic deficit, cholinergic disturbances, and cortical Lewy body formation among other things. 25 Our findings suggest that the ECS might have a role in the development of cognitive symptoms in PD.
The ECS has been studied in PD more with regard to motor symptoms27,28 rather than cognition. Some pre-clinical PD model studies have demonstrated that modulating the CB1R may improve cognitive processing. In one study, pretreatment with cannabidiol (CBD) (0.5 mg/kg) ameliorated memory deficits induced by reserpine administration in rats. 29 In another study, blockade of CB1R significantly attenuated social memory impairments and depressive-like behavior in a rat model of premotor Parkinson's disease. 30 Research on CBD use in human PD has reported a reduction in anxiety, psychotic symptoms, and sleep disturbances.31–33 One pilot study evaluating cannabinoids for the treatment of non-motor symptoms in patients with PD showed an improvement in the overall non-motor symptom burden, especially reflected by an amelioration of anxiety and sleeping problems, after treatment with a synthetic cannabinoid nabilone. 34
Our findings also support the previous observations of the study using [18F]MK9470, 16 as we also saw correlations between CB1R availability and episodic memory and executive functioning. Notably, in the [18F]MK9470 study, they used proportional scaling to the global [18F]MK9470 binding value to examine relative changes in CB1R availability, whereas we observed absolute changes in [18F]FMPEP-d2 binding. In the [18F]MK9470 study, disturbances in episodic memory (Rey Auditory Verbal Learning Test) were associated with a relative decrease in CB1R availability in middle cingulum and superior medial frontal gyrus. They also found that performance on the Digit Symbol substitution test, a measure of visuospatial function, executive function, and processing speed, was positively correlated with relative CB1R availability in middle cingulum, precuneus, thalamus, premotor cortex, and inferior orbitofrontal gyrus. Additionally, in line with our findings, they also did not find a significant relationship between CB1R availability and Stroop test scores. Methodological differences and demographic factors might explain why our findings are seen in somewhat wider brain areas.
The observed brain areas with decreased CB1R availability are related to episodic memory function and executive functions. The cingulate cortex acts as a bridge between neocortical areas and the hippocampus,35,36 a key structure for episodic memory formation.36–38 Whereas the visual cortex is involved in encoding and recalling visual episodic memories by interacting with the hippocampus to represent and retrieve visual information from past events.39–41 The temporal cortex and thalamus are essential for both encoding and retrieving episodic memories.42–47 In turn, interactions between the thalamus and prefrontal cortex are crucial in cognitive processes,48,49 and what is more, the prefrontal cortex is known to be the main control center for executive functions.50–52 The insula is thought to act as a bridge between internal and external information, at the crossroads of cortical and subcortical neural hierarchies, integrating multi-modal stimuli and regulating brain network activity. 50 The insula has also been proposed as a gatekeeper of executive control. 50 Additionally, the temporal cortex plays a crucial role in executive function, particularly in semantic control, like processing the meaning of words and understanding the context of events.53–56
In addition to PD, alterations in the ECS have also been described in other neurodegenerative disorders such as AD. Evidence from animal models remains inconsistent, possibly reflecting differences in model-specific pathology.57,58 In humans, postmortem studies report reduced cortical CB1R density, whereas in vivo imaging findings are less consistent.59–61 This discrepancy may indicate stage-dependent changes, as increased CB1R activity has been observed in early AD in select hippocampal and frontal cortical regions, followed by reductions at more advanced stages. 62 Beyond receptor-level alterations, dysregulation of endocannabinoid-metabolizing enzymes 63 and reduced cortical levels of anandamide have also been reported in AD. 64 Additionally, lower anandamide levels correlate with greater cognitive impairment and increased amyloid-β42 burden. 64
In the current study, 15 of 23 participants provided a CSF sample to study AD biomarkers. Among these 15 participants, five had two or three abnormal AD biomarkers, so a potential contribution of amyloid pathology to the present findings cannot be excluded. Concomitant AD-related pathology is common in PD, particularly in patients who develop cognitive impairment. 65 At the same time, amyloid-β accumulation, especially reductions in CSF Aβ42, may also reflect age-related processes rather than disease-specific mechanisms. 66 Furthermore, cognitively intact patients with PD may already exhibit abnormal AD-related CSF biomarkers, and reduced Aβ42 levels have been associated with an increased risk of subsequent cognitive decline. 67 In this context, it is conceivable that a subset of participants in the present cohort may be in a preclinical phase of cognitive deterioration. However, given the cross-sectional design, this interpretation remains speculative and warrants confirmation in longitudinal studies incorporating both biomarker and clinical follow-up.
A relation between CB1R availability and cognitive decline has also been found in cannabis users68–71 and patients with first-episode psychosis. 72 Instead, no relationship between CB1R and cognitive functions was found in Huntington's disease, but association with behavioral functions was seen. 73 Altogether these findings suggest that the involvement of ECS in relation to cognitive functions varies in different neurodegenerative disorders.
We have previously demonstrated the effect of dopaminergic medication on the ECS, as we discovered that when the subjects with PD were off their usual antiparkinsonian medication, the CB1R availability was significantly decreased compared with being on medication. 17 The functional interaction between the dopaminergic system and the ECS has also been observed in a few other studies.74,75 In our current study, all the participants were on their individual standard antiparkinsonian medication during neuropsychological testing and [18F]FMPEP-d2 PET imaging. Considering these aspects, LEDD was included as a covariate in the analyses. Regarding other medication potentially affecting the ECS, two participants were using escitalopram. Since chronic use of antidepressants may modulate the CB1R availability, 76 we additionally replicated the analyses without these two participants and the results remained essentially the same. Another limitation of our current study is a relatively small sample size.
It is unlikely that the observed results are due to possible brain atrophy. More profound brain atrophy has been observed in PD with a distinctly longer disease duration and disease severity77,78 compared with our study sample (average disease duration of 7.7 ± 4.5 years, H&Y score 2.5 and UPDRS-III score 23.6 ± 8.5). Results were also essentially replicated using correction for partial volume effects (see Supplementary Material). Moreover, none of the neuropsychological assessments showed significant group differences between PD and HC, indicating that the cognition of our PD subjects was still rather good. More specifically, three out of 23 PD subjects were defined as PD-MCI. As the number of PD-MCI subjects was so small, group level analyses between PD-MCI and PD-NC (Normal Cognition) were not conducted.
Longitudinal studies indicate that individuals who later develop dementia already exhibit hypometabolism at baseline in the visual association cortex, posterior cingulate, and caudate nucleus, with deficits becoming more widespread as cognitive decline progresses. 79 Similarly, reduced metabolism in posterior and temporal regions predicts subsequent cognitive decline. 80 Thus, there is a partial regional overlap between reduced CB1R availability and previously reported hypometabolic patterns in PDD. Further investigation of the relationship between CB1R availability and metabolic alterations in PD and PDD could be achieved through longitudinal studies combining [18F]FMPEP-d2 and [18F]FDG PET imaging.
In conclusion, our study suggests that PD patients with more impaired episodic memory functioning and executive functioning have lower CB1R availability in related brain areas. We cannot conclude that reduced CB1R availability can predict cognitive decline in PD, without a follow-up study. More studies with larger sample sizes, longitudinal study designs, and participants at different stages of PD are needed to further understand the relationship between ECS and PD symptoms, and determine whether ECS-targeting medication could benefit in managing the non-motor symptoms of PD.
Supplemental Material
sj-docx-1-pkn-10.1177_1877718X261457830 - Supplemental material for Deficits in episodic memory and executive functions in relation to CB1 receptor availability in Parkinson's disease
Supplemental material, sj-docx-1-pkn-10.1177_1877718X261457830 for Deficits in episodic memory and executive functions in relation to CB1 receptor availability in Parkinson's disease by Riikka M Ajalin, Haidar Al-Abdulrasul, Jouni M Tuisku, Mira Karrasch, Jussi Hirvonen, Anna K Kirjavainen, Henrik Zetterberg, Juha O Rinne and Anna E Brück in Journal of Parkinson's Disease
Footnotes
Acknowledgment
The authors acknowledge all the participants for their willingness to participate in this study, and the expert staff at Turku PET Centre for their work in radiochemical production and imaging procedures. Research nurse Ulla Kulmala is acknowledged for her excellent work as a study coordinator and technical assistant.
Ethical considerations
The study was approved by the Ethics Committee of the Hospital District of Southwest Finland (ref. 153/1801/2013) and was conducted according to the World Medical Association Declaration of Helsinki (Ethical Principles for Medical Research Involving Human Subjects) and following Good Clinical Practice guidelines.
Consent to participate
All participants gave their written informed consent obtained according to the declaration of Helsinki.
Consent for publication
Not applicable.
Author contributions
1. Research project: A. Conception, B. Organization, C. Execution.
2. Statistical Analysis: A. Design, B. Execution, C. Review and Critique.
3. Manuscript Preparation: A. Writing of the first draft, B. Review and Critique
RA: 1C, 2A, 2B, 3A, 3B
HA: 1C, 3B
JT: 1C, 2B, 3B
JH: 2C, 3B
MK: 2C, 3B
AKK: 1C, 3B
HZ: 1C, 3B
JOR: 1A, 1B, 2C, 3B
AB: 1A, 1B, 1C, 2C, 3B
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: RA was supported by grants from The Finnish Movement Disorders Association, The Finnish Medical Foundation sr, Finnish State Research Funding (VTR) and Turku University research funds. HA was supported by grants from the Finnish Movement Disorders Association and Helsinki University research funds. JT was supported by grant from Finnish State Research Funding (VTR). HZ is a Wallenberg Scholar and a Distinguished Professor at the Swedish Research Council supported by grants from the Swedish Research Council (#2023-00356, #2022-01018 and #2019-02397), the European Union’s Horizon Europe research and innovation programme under grant agreement No 101053962, and Swedish State Support for Clinical Research (#ALFGBG-71320). JOR was supported by grants from the Academy of Finland research grants (#310962), the Sigrid Juselius Foundation and Finnish State Research Funding (VTR). AB was supported by grants from the Finnish Movement Disorders Association and Finnish State Research Funding (VTR).
Declaration of conflicting interests
HZ has served at scientific advisory boards and/or as a consultant for Abbvie, Acumen, Alamar, Alector, Alzinova, ALZpath, Amylyx, Annexon, Apellis, Artery Therapeutics, AZTherapies, Cognito Therapeutics, CogRx, Denali, Eisai, Enigma, LabCorp, Merck Sharp & Dohme, Merry Life, Nervgen, New Amsterdam, Novo Nordisk, Optoceutics, Passage Bio, Pinteon Therapeutics, Prothena, Quanterix, Red Abbey Labs, reMYND, Roche, Samumed, ScandiBio Therapeutics AB, Siemens Healthineers, Triplet Therapeutics, and Wave, has given lectures sponsored by Alzecure, BioArctic, Biogen, Cellectricon, Fujirebio, LabCorp, Lilly, Novo Nordisk, Oy Medix Biochemica AB, Roche, and WebMD, is a co-founder of Brain Biomarker Solutions in Gothenburg AB (BBS), which is a part of the GU Ventures Incubator Program, and is a shareholder of CERimmune Therapeutics (outside submitted work). The other authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
The data that support the findings of this study are available from the corresponding author, upon reasonable request. The data are not publicly available; they contain information that could compromise the privacy of research participants.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.