
Abstract
Worldwide, the incidence, prevalence, disability, and mortality associated with Parkinson's disease (PD) have increased substantially, placing an immense strain on healthcare systems across countries of all income levels, prompting the use of the term “Parkinson pandemic” to emphasize the urgent need for coordinated strategies to address its worldwide impact. This narrative review explores the regional differences in the dramatic increase in PD burden, along with its genetic, environmental, and socioeconomic determinants worldwide. Furthermore, it discusses the healthcare access in different regions and proposes strategies to combat this pandemic. The rising burden of PD is largely driven by population aging, increased life expectancy, and potentially by greater exposure to by-products of industrialization—such as pesticides, air pollution and heavy metals- and declining smoking rates, which vary across world regions. Differences in prevalence, demographic, genetic and lifestyle factors, the impact of urbanization and environmental risk factors, as well as inequality and disparities in access to care and healthcare services, have been outlined, mandating the development of tailored and region-specific strategies to mitigate the pandemic and reduce its burden globally and regionally. These strategies include exploring relevant genetic and environmental determinants, promoting research, increasing public awareness, facilitating early diagnosis and optimal management, improving access to healthcare services, supporting caregivers, encouraging the adoption of protective lifestyle factors, ensuring the availability of essential medications and controlling environmental exposures such as toxicants.
Plain language summary title
Global Burden of Parkinson's Disease worldwide
Plain language summary
Mapping the global burden of Parkinson's disease
The global burden of PD is increasing over the past decades worldwide, with estimated that about 12 million had PD in 2021 and might exceed 25 million by 2025. This global rise places an immense strain on healthcare systems across all countries, prompting the use of the term Parkinson Pandemic to emphasize the urgent need for coordinated strategies to address its worldwide impact. However, considerable regional variability in its burden exists, attributed to differences in prevalence, underlying genetic and environmental risk factors and its interaction, variable population aging and growth, life expectancy, lifestyle factors, awareness and early diagnosis as well as inequality and disparities in access to care and healthcare services. This review recognizes the determinants of PD pandemic and their variations across continents and discusses proposed strategies to combat this growing global challenge.
Regional differences of PD prevalence are well recognized. High-income countries reported high prevalence, while low-middle-income countries showed a greater increase over recent decades. Understanding genetic variations among populations might explain the variability of PD prevalence, explore disease pathogenesis and tailor future therapies. Additionally, environmental risk factors for PD show marked global variation, reflecting differences in industrialization, agricultural practices and regulatory frameworks, with higher risk in areas with intensive agriculture, industrial emissions, and heavy air pollution.
Comprehensive strategies to combat this pandemic include exploring relevant genetic and environmental determinants, promoting research, increasing public awareness, facilitating early diagnosis and optimal management, improving access to healthcare services, supporting caregivers, encouraging the adoption of protective lifestyle factors, ensuring the availability of essential medications and controlling environmental exposures such as toxicants.
Introduction
Parkinson's disease (PD), the second most common neurodegenerative disorder, is characterized by core motor features, as well as a broad range of non-motor manifestations, which together contribute to significant disability, reduced quality of life and increased disease burden.1,2 The underlying causes are thought to involve genetic factors, environmental exposures, or an interaction of both. 3
The Global Burden of Disease (GBD) study identified PD as the fastest-growing neurological disorder worldwide. Between 1990 and 2015, the prevalence of PD increased by approximately 117.8%, with the number of people with PD (PwPD) doubled to 6.2 million, followed by dementias (111.7%) and stroke (59.2%).4,5 It has been estimated that 11.77 million people had PD worldwide in 2021, with increased its burden over the past 32 years.6,7 This increase is largely driven by population aging, greater life expectancy, heightened exposure to by-products of industrialization, more public awareness and diagnosis and a decline in smoking rate.8–10 This global rise places an immense strain on healthcare systems across all countries, prompting the use of the term Parkinson Pandemic to emphasize the urgent need for coordinated strategies to address its worldwide impact.8,11
Although the Parkinson Pandemic is recognized as a global health challenge, considerable regional variability in its burden exists.4,10 This includes differences in prevalence, underlying causes, genetic and environmental risk factors, as well as inequality and disparities in access to care and healthcare services.6,12–14 Recent updates on the determinants of PD burden and access to healthcare have been reported across various different regions, particularly Africa, underscoring the importance of continuous monitoring of these determinants.13,15 Recognizing and understanding these variations is essential for developing tailored strategies that address local needs and optimize patient outcomes. 12
This narrative review explores the regional differences in the dramatic rise of PD epidemiology and burden, along with its genetic, environmental, and socioeconomic determinants worldwide. Furthermore, it discusses the healthcare access in different regions and proposes strategies to combat this growing global challenge.
Method and search strategy
Expert authors in different aspects of the topic were invited for this narrative review, representing diverse world regions. A literature search was conducted using PubMed and Scopus to identify relevant studies and reviews from May to December 2025. The following keywords were used; “Parkinson's disease” AND (“Pandemic”, OR “Global Burden” OR “epidemiology” OR “genetic” OR “environmental” OR “pesticides” OR “toxins” OR “aging” OR “lifestyle” OR “urbanization’ OR “access to care” OR “Africa” OR “America” OR “Asia” OR “Europe”. Additionally, backward citation tracking was performed by screening the reference lists of key studies and landmark reviews to identify further relevant publications.
Prevalence and burden of Parkinson's disease across different regions
PD is rare before midlife and increases with age. Incidence ranges from 47 to 77/ 100,00 among persons aged 45 or older and 108 to 212/100,000 among persons aged 65 and older. 16 Prevalence estimates range from 1% of persons aged 45–54 to 4% of men and 2 percent of women aged 85 or older. 16 This male preponderance is observed in most populations worldwide. 17 In 2021, the GBD study ranked PD as eleventh worldwide among conditions affecting neurological health, based on age-standardized disability adjusted life years (DALYs). 7 The same study estimated that global prevalence increased by an estimated 273.9% from 1990 to 2021, with DALYs increasing to 7.47 million. 5 When examined regionally, PD ranked in the top ten most burdensome conditions for Central Asia, East Asia, Southeast Asia, North Africa and the Middle East, Andean Latin America and High Income North America. 7 Importantly, these estimates are by definition imprecise, since actual data are only available for a few locations internationally, and even then in many cases are incomplete. 7
Prevalence reflects both incidence and survival. Because survival in PD is generally for many years, prevalence can provide useful information on disease distribution. In high-income countries, PD was estimated to affect 254.2 per 100,000 persons in 2021, representing a 96% increase from 1990. 18 In upper middle-income countries, the estimates were similar – 247.6 PwPD per 100,000 population, but with a much greater change from 1990 of 350%. Lower middle-income countries (LMICs) and low-income countries (LICs) had lower estimated PwPD – 62.5 and 28.7 per 100,000 population, respectively. Nonetheless, these estimates represented a 94% increase in LMICs and a 33% increase in LICs compared to 1990. 18 Moreover, the prevalence of PD was projected to be 267 (230 to 320) cases per 100,000 in 2050, representing a 112% and 76% increase in the number of PwPD and PD prevalence from 2021 to 2050, respectively. 14
The expected increase in PD burden worldwide was attributed to aging (89%), population growth (20%) and increased prevalence (3%) between 2021 and 2050, with regional and national variability (Figure 1, Table 1). In 2021, East Asia reported the highest prevalence of PD (243.46 per 100,000 population), whereas sub-Saharan Africa (SSA) showed the lowest prevalence. Although the all-age prevalence of PD was lowest in SSA regions, Western and Eastern SSA showed the largest increase of PwPD number from 2021 to 2025, representing 292% and 246%, respectively, driven by population growth, aging, improved healthcare, increased awareness and diagnosis, increased life expectancy, and declining fertility rates. 19 Moreover, East Asia demonstrated the fastest increase in PD prevalence from 1991 to 2021, whereas Central Europe exhibited the slowest increase. 20 This rapid demographic shift is expected to be particularly devastating in SSA, given the current limitations in healthcare services, shortages of providers, and persistent economic challenges. 21
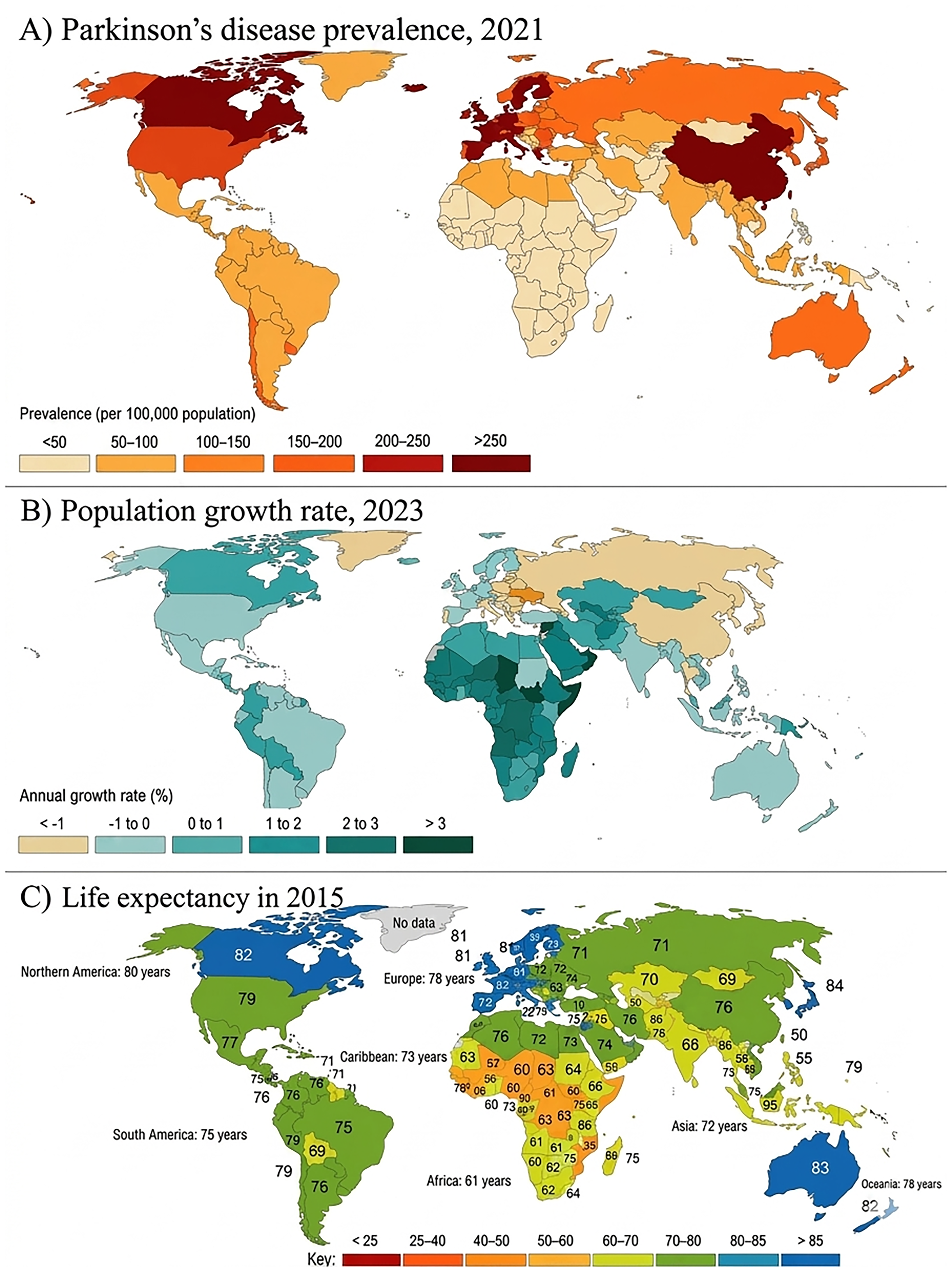
Prevalence of Parkinson's Disease and Its Determinants Across World Regions. (A) Worldwide Prevalence of Parkinson's Disease (2021) (https://ourworldindata.org/grapher/ parkinsons-disease-prevalence-ihme). (B) Population growth rate (2023) (https://ourworldindata.org/grapher/population-growth-rates?tab = map&time=2023). (C) Worldwide Life-expectancy (2015) (https://ourworldindata.org/life-expectancy-globally (access in 9th January 2026). IHME, Global Burden of Disease (2024) – with major processing by Our World in Data. Data access on 11th January 2026
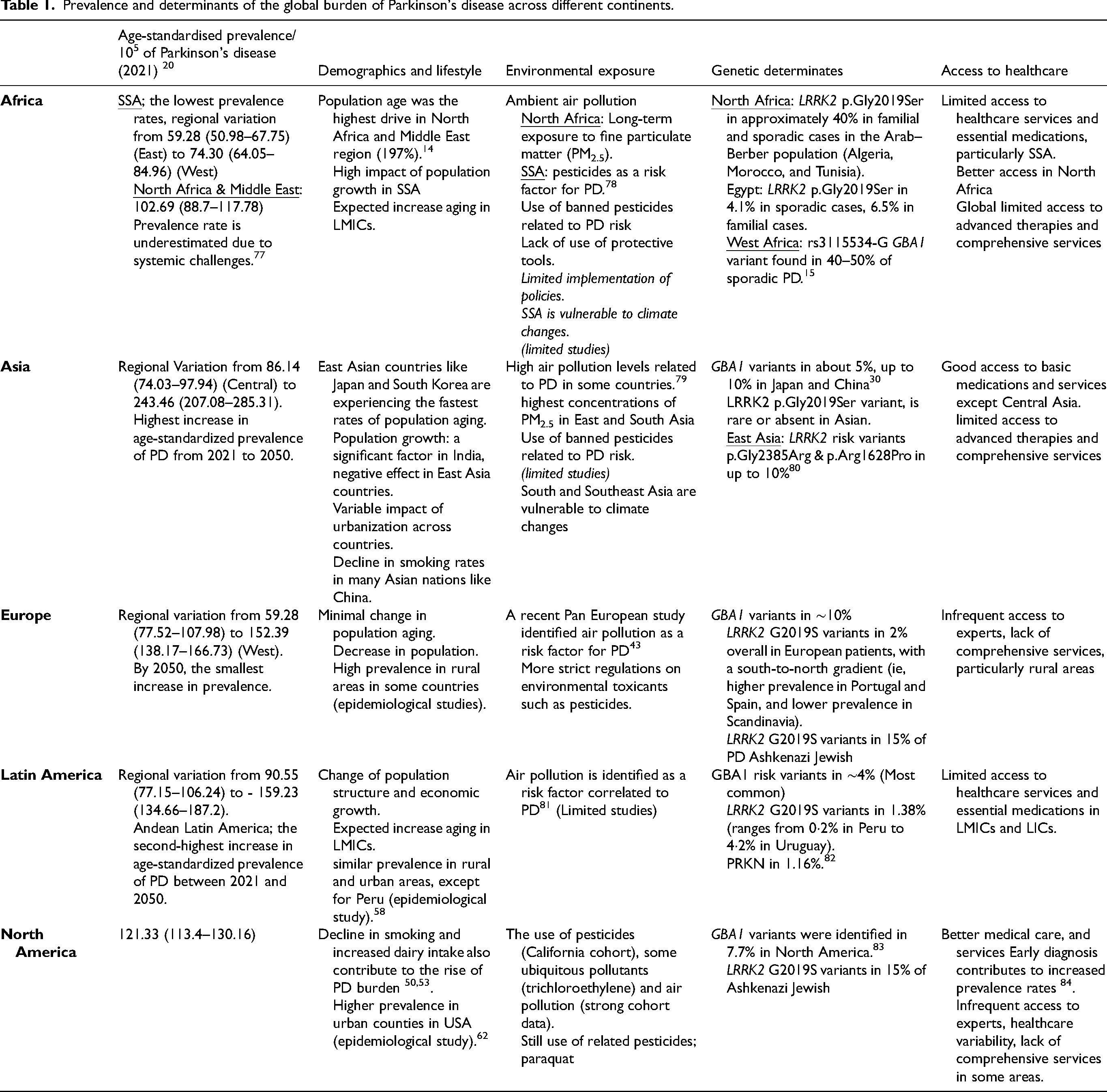
Prevalence and determinants of the global burden of Parkinson's disease across different continents.
Regional genetic determinants of Parkinson pandemic
Whilst the genetic determinants of PD cannot readily explain such rapid increases in the apparent global burden of PD, there are several indirect examples of how genetic study amplifies and reveals the burden. Age is an important factor in both genetic and sporadic forms of PD. As global ageing occurs, the number of variant carriers that will manifest clinical features also increases, and where better diagnosis, treatment and management occur, prevalence will increase as a function of improved survival. 22
In many populations, monogenic causes account for a minority of cases (e.g., 5–10% PD of European ancestry), but in some the proportion of cases that carry a pathogenic variant is much higher (for example, in Ashkenazi Jews, LRRK2 variants can be found in 15–25%). 23 When it comes to the study of sporadic PD, complex trait genetics has yielded insights mainly through genome-wide association studies (GWAS), which identify increasing loci as a function of sample size.23,24 The PD GWAS era has been dominated, until recently, by the study of cases and controls of European ancestry. This results in a skewed understanding of the mechanistic drivers of sporadic PD, whereby information is plentiful, but Europeans only comprise ∼15% of the global population. 25
Initiatives like the Global Parkinson's Genetic Program (GP2) are addressing this skewed understanding, through an enormous effort to accelerate sample collection and data generation from under-represented parts of the world. 26 This effort has spawned the first PD GWAS in West African cases and controls, 15 with several ancestry-specific GWASs anticipated in the next 12 months, the first multi-ancestry PD GWAS, 27 and new gene discovery (e.g., RAB32). 28
Genetic variants linked to PD showed considerable variation among different populations (Table 1). The p.G2019S LRRK2 variant is more frequent in the Ashkenazi Jewish population (sporadic, 10%; familial, 28%) and the North African population (sporadic, 30–34%; familial, 30–42%), than in Europeans, but it rarely observed in Asian populations (<0.1%). 29 The p.R1441G LRRK2 variant is most prevalent in the Basque region of Spain (sporadic, 2–4%; familial, 16–46%), whereas G2385R and R1628P are common in East Asia. 29 GBA1 variants are found in 5–15% of Europeans and a higher proportion of Ashkenazi Jewish patients, making GBA1 variants the most common genetic risk factor for PD. 30 The sole GWAS significant hit in the first West African PD GWAS was in an intronic segment of GBA1 (rs3115534-G), and this variant, whilst rare in Europeans, is present in more than 40% of patients in West Africa. 15 Taking variants in both LRRK2 and GBA1 as examples, these are associated with PD with later age at onset and age-dependent penetrance, so longer life expectancy increase the number of individuals that will manifest signs during their lifetimes. Furthermore, global migration patterns from areas of lower to higher income and transfer to alternative healthcare settings, likely increases genetic causes of PD being identified. This is particularly relevant to populations with common founder mutations such as Ashkenazi Jewish and North African Arab-Berber groups.29,30
As much as our understanding of PD genetics has increased, it is hard to explain how genetic factors in isolation could directly contribute to the increasing global burden of PD. However, investment, knowledge transfer and capacity building around the world results in greater awareness, better record keeping and more accurate diagnosis, which in turn may contribute to more identified cases. Considering genetic and environmental contributions in isolation is fundamentally flawed. There is increasing evidence that potentially important interactions occur between genetic variants and environmental / lifestyle exposures either by focusing on LRRK2 (e.g., interaction with caffeine and tobacco exposure) or polygenic risk score analysis.31–34 As such, a rising burden might be indirectly driven by genetic factors if these facilitate or fail to address pathogenic cascades initiated by stochastic events, stress or environmental exposures, including toxicants and infections. 26 There are specific examples of interactions between lifestyle factors and common variants for PD, 33 which warrant further detailed study, but systematic exploration of interactions and pathways acting between genes and environmental exposure has not been undertaken. 26
Environmental determinants of Parkinson pandemic across world regions
Environmental risk factors for PD show marked global variation, reflecting differences in industrialization, agricultural practices, and regulatory frameworks. The evidence base is heterogeneous across exposure categories: robust and consistent for pesticides and industrial solvents and emerging for ambient air pollution. 35 The following subsections summarize the strength of evidence, typical exposure scenarios, and key regional examples for each major exposure type.
Pesticides
Pesticides represent the best-established environmental risk category for PD. A pivotal early insight came from the accidental 1983 discovery that MPTP — a contaminant of illicit meperidine analogues — produced irreversible parkinsonism in humans by selectively destroying dopaminergic neurons of the substantia nigra, simultaneously implicating environmental chemicals in PD pathogenesis and providing the first translational animal model. 36 Subsequent prospective and case-control studies have consistently linked chronic pesticide exposure to elevated PD risk: paraquat and rotenone, herbicides that impair mitochondrial complex I and generate oxidative stress, are the most replicated agents, with experimental models confirming dopaminergic nigrostriatal degeneration that mirrors idiopathic PD.37,38 Typical exposure scenarios include occupational farm work, use of well water contaminated by agricultural runoff, and prolonged contact with treated crops; rural residence per se is not uniformly risky, but rural settings with intensive pesticide use confer substantially elevated risk. 39 Geographic hotspots include parts of the United States (particularly the Midwest and South), Latin America, and Asia's major agricultural belts, especially where paraquat and organophosphates remain in active use despite restrictions elsewhere. In sub-Saharan Africa, aggregate pesticide volumes are lower but the continued use of banned organochlorine compounds and very limited use of protective equipment during application create a disproportionate risk burden in rural communities. 40
Industrial solvents
Trichloroethylene (TCE) is the most thoroughly studied industrial solvent in the context of PD. Widely used in metal degreasing and dry cleaning, TCE persists as an environmental contaminant in air, soil, and groundwater near manufacturing and military sites. Occupational and community-level studies — including analyses of contaminated-water exposure among Camp Lejeune veterans — have demonstrated significantly elevated PD risk associated with TCE. 41 More recently, ambient TCE exposure from contaminated groundwater has also been linked to increased PD incidence in Medicare populations, extending risk beyond occupational settings. The mechanistic basis involves mitochondrial complex I inhibition, reproducing the biochemical insult seen with rotenone. Typical exposure scenarios include metal workers, dry-cleaning operatives, and residents near legacy industrial or military contamination sites. Geographically, evidence is concentrated in North America and Europe, though systematic surveillance of solvent-associated PD outside high-income settings remains limited (Table 1). 42
Ambient air pollution
Long-term exposure to fine particulate matter (PM2.5) and traffic-related pollutants — including nitrogen oxides and carbon monoxide — has been correlated with PD incidence and mortality in large cohort studies across North America and Europe, with associations observed even at concentrations below current EU safety thresholds. Proposed mechanistic pathways include neuroinflammation and oxidative stress mediated by inhaled combustion-derived particles and transition metals. Hotspots have been identified in the Mississippi–Ohio River Valley in the United States and European urban–industrial clusters.43,44 Compared with pesticides and TCE, the epidemiological literature is more heterogeneous, with residual confounding and exposure measurement error representing ongoing methodological challenges. This exposure category is therefore best characterized as emerging and increasingly consistent at high pollution levels but not yet established as definitively causal in the same manner as the agents above. Notably, the mechanisms operating in rural agricultural zones (pesticide-dominated) and dense urban corridors (air pollution-dominated) are geographically distinct, and risk profiling should account for this heterogeneity.43,44
Other determinants of the Parkinson pandemic in different regions
Population aging
Every country worldwide is seeing an increase in both the number and proportion of older individuals in its population. According to the World Population Prospect 2024, by 2030, one in six people globally will be aged 60 or older. At that time, the proportion of the population aged 60 and above is expected to rise from 1 billion in 2020 to 1.4 billion. By 2050, the global population aged 60 and older is projected to double to 2.1 billion. Additionally, the number of people aged 80 or older is forecasted to triple between 2020 and 2050, reaching 426 million. 45 Aging is the most significant risk factor for developing PD, and the aging population is universally recognized as the predominant factor contributing to the rising prevalence and burden of PD across all countries and regions. The importance of population aging is supported by comprehensive decomposition analyses. These analyses suggest that between 2021 and 2050, population aging will be the leading factor (89%) contributing to the expected rise in global PD incidence. This far outweighs the contributions of population growth and changes in prevalence. 14 Additionally, a study examining PD trends in China found that the increase in PD-related mortality was largely due to an aging population. 46 The methodology used in this study isolates factors such as population growth, aging, and age-specific rate changes, showing aging as the main demographic driver of mortality trends. The increase in PD is expected to be heavily concentrated in older age groups, further confirming age as the primary risk factor. Populations over 80 years old are projected to see the highest increase in PD cases (196%) globally between 2021 and 2050. 14
While this shift toward older ages began in high-income countries (for example, in Japan, 30% of the population is already over 60 years old), it is now also significantly observed in LMICs. By 2050, two-thirds of the world's population over 60 will live in LMICs. 47 Besides, the effect of population aging on PD prevalence varies significantly by region, often correlating with socioeconomic development and the pace of demographic transition. 6 Countries in the middle range of the socio-demographic index (SDI) are projected to experience substantial growth, with the highest percentage increase in both all-age prevalence (144%) and age-standardized prevalence (91%) between 2021 and 2050. This might be caused by rapid aging, along with factors such as industrialization and increased life expectancy observed in these developing countries. In high-income countries, aging still drives the absolute increase in cases, but the projected rate of increase is generally lower compared to rapidly developing regions. High SDI countries are projected to have the lowest growth rate in the total number of PD cases (54% increase) compared to other SDI groups until 2050. 14 This is partially because these countries experienced significant population aging before 1980. 10
Population growth
Global population growth is expected to be the second major factor driving the increase in total PD cases, especially in countries with low SDI (Figure 1). Population growth is expected to contribute about 20% of the global increase in cases from 2021 to 2050. The impact of population growth on PD prevalence trends has been estimated to be highest in SSA. 14 The effect of population growth varies between genders. In the two decomposition analyses, population growth is expected to account for a higher percentage increase in female prevalent cases compared to males. 14 Population growth accounted for 44.16% of the increase in the number of prevalent PD cases. It was the single largest contributor to the rise in female cases, surpassing the effects of population aging (23.17%) and epidemiological changes (32.67%). 6 The longer life expectancy in women could be an explanation for this difference.
Increased life expectancy
While closely associated with population aging, increased life expectancy or longevity, causing more persons to survive, remains a distinct and vital factor that amplifies the rising prevalence of PD (Figure 1). Prior to the COVID-19 pandemic, global life expectancy experienced an increase of over six years between 2000 and 2019, subsequently resuming a gradual upward trajectory post-pandemic. Enhanced general health and improved therapeutic management of PD symptoms have contributed to higher survival rates and prolonged life expectancy for individuals with and without PD. The duration of PD disease has also significantly risen in recent decades. 48 This phenomenon helps explain regional variations in prevalence that demographics alone cannot. The higher prevalence of PD observed in individuals over 70 years of age in high-income countries, for example, is likely driven by the greater life expectancy in those regions. 47
Furthermore, in a modelling study for France, secular trends in life expectancy were projected to increase the survival of 65-year-old PD patients by about 3 years between 2010 and 2030 (from 14.8 to 17.8 years for women and 13.0 to 16.1 years for men at age 65). This increased longevity alone was projected to lead to a 12% increase in the age-standardized prevalence rate over 20 years. 49 The age-standardized years lived with disability rates of PD patients have been reported to increase globally, reflecting a gradual increase in the burden of disability as patients survive longer with the condition. 6 The convergence of these two trends, a longer overall lifespan for the general population and longer survival with the disease, creates a multiplier effect significantly increasing the total number of PwPD at any given time and imposing a greater long-term burden on global healthcare systems.
Lifestyle and behaviour factors
Globally, changes in prevalence unrelated to demographic factors (aging and growth) were projected to contribute 3% to the increase in cases between 2021 and 2050. 14 Alterations in common behaviours also influence prevalence projections, especially the decline in factors previously linked to protective effects.
Smoking or tobacco usage is strongly correlated with a decreased risk of developing PD, with odds ratios generally ranging from approximately 0.4 to 0.6 when comparing individuals who have ever smoked to those who have never smoked. 50 The global reduction in smoking rates is hypothesized to contribute to the increasing prevalence. A study estimated that, assuming a causal inverse relationship between smoking and PD, a lower prevalence of smoking could result in a 10% increase in PD burden by the year 2040 relative to estimates based solely on aging. 51 Another investigation examining trends in the United States indicated that a significant rise in PD incidence among males (particularly those over 70 years of age) between 1976 and 2005 may be partially attributable to decreased smoking in earlier decades. 52 Globally, a projected 20% decline in smoking prevalence by 2050 is expected to lead to a 2.1% increase in future case numbers. 14 In Asia, where smoking prevalence is decreasing dramatically due to smoking bans, this trend may lead to a further increase in PD cases.
Numerous prospective studies indicate an inverse relationship between physical activity intensity and PD risk.50,53 Frequent moderate or vigorous physical activity is associated with a 34% reduction in PD risk. 50 Increased physical inactivity resulting from industrialization and urbanization contributes to the rising burden of PD. Given its protective role, promoting physical activity constitutes a justified intervention for primary prevention. If all individuals engaged in regular physical activity, the projected number of PD cases worldwide would decrease by 4.9% compared to the initial forecast for 2050. Assuming a 20% increase in the prevalence of physical activity by 2050, the future number of PD cases would decrease by 2.6%, corresponding to 0.65 million prevalent cases. 14
Changes in dietary patterns and metabolic health are increasingly recognized as modifiable risk factors contributing to the burden of PD. The intake of specific dairy products, particularly increased intake of milk, has been reported to be associated with a heightened risk of PD. 53 Conversely, adherence to a Mediterranean-style diet, characterized by high intake of fiber, vegetables, fruits, nuts, and low consumption of red meat, has been linked to a reduced likelihood of prodromal PD features and a delay in symptom onset. Furthermore, the relationship between the rising prevalence of T2DM and PD represents an emerging area of concern. Aside from the fact that these two conditions are often associated with similar unhealthy lifestyle factors, T2DM is generally acknowledged as a potential modifiable risk factor for PD. 54 A notable increase in PD risk among individuals with T2DM has been documented in several cohorts. Global industrialization and urbanization have led to lifestyle and dietary changes, including decreased physical activity and increased consumption of processed foods. These changes, in turn, contribute to an escalation in the prevalence of metabolic diseases such as T2DM, thereby augmenting the risk and progression rate of PD. 10
Urbanization
Research attempting to compare PD prevalence between urban and rural settings has produced inconsistent results. Some studies suggest that PD prevalence remains higher in rural areas in comparison to urban areas.55,56 Conversely, other research has observed increased PD prevalence in urban regions or has noted no significant difference.6,57 A door-to-door epidemiological study in six Latin American countries showed no significant differences between urban and rural areas, except for lower prevalence in urban areas of Peru. 58 In Asia, some epidemiological studies have reported higher prevalence of PD in urban areas in South Korea and Thailand, but the reverse has been reported in China.59–61 Similarly, a cross sectional study has reported higher prevalence in urban counties than in rural areas in United States. 62 In contrast, higher prevalence of PD has been reported in rural arears in European countries such as UK and Finland.63,64
One viewpoint suggests that rural living elevates the risk of PD in developed countries, whereas urban living increases the risk in developing nations. 53 Variations in prevalence rates between rural and urban areas may reflect issues related to healthcare access rather than the actual disease burden. 65 Numerous lifestyle and behavioural changes associated with urbanization are recognized as risk factors for PD. Urbanization, especially in rapidly developing regions and middle- to high-income countries, is also linked to increased environmental risk factors such as traffic-related air pollution and occupational exposure to solvents, contributing to the rising burden of PD.66,67 Nevertheless, to date, no study has been conducted to examine the impact of urbanization on the temporal trend of PD.
Healthcare access and awareness
The recorded rise in prevalence is also influenced by improvements in healthcare access, diagnostic capabilities, awareness and data collection especially in nations undergoing rapid socioeconomic transitions. 6 Advanced healthcare systems and diagnostic technologies in higher-income countries contribute to earlier and more accurate diagnoses. The GBD study estimated a 21.7% age-adjusted prevalence rise between 1990 and 2016, with some change attributed to better diagnosis and methodology improvements. 68
Limited access to healthcare services and essential medications has been widely reported in LMICs, particularly in SSA. 19 African countries face multiple challenges, including limited access to healthcare, poor availability and affordability of PD therapies, lack of neurologists, underdiagnosis, lack of patient support groups, misbeliefs about the illness, and a lack of epidemiological research. 10 These factors further exacerbate the burden of PD across Africa, particularly in SSA.13,19,69,70 A continental African survey showed that levodopa is available continually in only 46.4% of African countries, with lack of availability and affordability of other therapies, experts and different services. 13
A recent report indicated better access to neurologists and levodopa in Asian countries (up to 100%), while access to other therapies and services remains limited, particularly Central Asia. 71 A global survey of neurologists revealed that availability of PD therapies and services, apart from levodopa, correlated with national income, indicating less availability in LICs and LMICs across different regions. 72 Furthermore, while PwPD in high -income countries have access to basic medications and services, they still face significant barriers. These include infrequent access to experts, healthcare variability and a lack of comprehensive services such as mental health and rehabilitation, particularly in rural areas (Table 1).73,74
The concept known as the “ascertainment effect” describes how the interplay of public awareness, healthcare professionals’ knowledge, and diagnostic capacity influences reported prevalence rates. When these factors improve, the detection and reporting of cases increase, leading to higher recorded prevalence. 75 This explains the seemingly contradictory trends across different regions. In resource-limited settings, enhanced public awareness has markedly reduced the hidden burden of undiagnosed PD, exemplified by rapid development in countries like China, where the age-adjusted prevalence has doubled since 1990. 5 Conversely, in countries with well-established healthcare systems such as the UK, Finland, or the Netherlands, PD incidence has remained stable or even declined, indicating that once high diagnostic capacity and awareness are achieved, undercounting diminishes, and trends become more accurate. 76
Strategies and plans to combat the Parkinson's pandemic
PD has become a slow-moving global pandemic driven by aging populations, environmental exposures, and growing social and economic inequalities. 22 Some authors even argue that it is a human-made pandemic, largely preventable through environmental regulation and health system reform. 85 Yet, despite its accelerating global impact, PD remains absent mainly from coordinated international responses that have been mobilized for other non-communicable diseases such as cancer, cardiovascular disease, or diabetes. After decades of limited global attention, the World Health Organization (WHO) has only recently recognized the need for a concerted global response, calling for action through the Intersectoral Global Action Plan on Epilepsy and Other Neurological Disorders. 86 Addressing this silent pandemic requires a fair and coordinated global plan that focuses on prevention, early diagnosis, stronger health systems, and policies that include all global populations in the response to PD.
The WHO developed a coordinated plan to guide public health actions in response to the growing global burden of PD. Based on this effort, they outlined six key domains that serve as a framework for addressing the Parkinson's pandemic.19,75 These domains cover prevention, awareness, care, research, and policy, offering countries a framework for designing local strategies. Together, they outline a global roadmap to reduce the burden of PD through coordinated action. 19 The following paragraphs summarize the main pillars of this framework and their implications for global action (Figure 2).
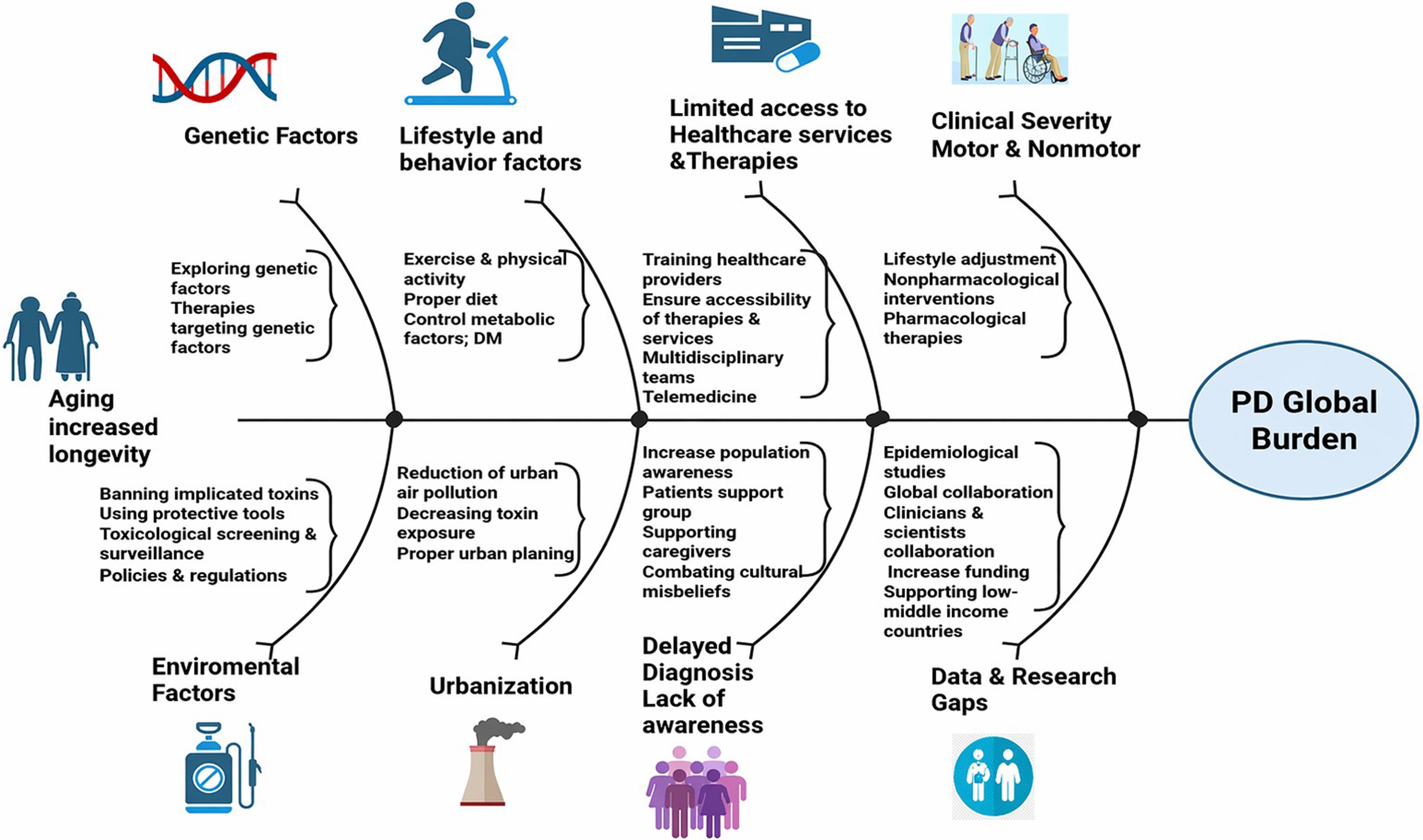
Determinants of the global burden of Parkinson's disease and proposed strategies to combat its pandemic.
Effective planning begins with reliable data, which are essential for understanding and addressing the global burden of PD. Recent proposals emphasize that prevention begins with measuring the disease. 85 Epidemiological surveillance through standardized measures of prevalence, incidence, DALYs, and mortality can provide meaningful comparisons across regions. Equitable representation by geography, ancestry, sex, and socioeconomic status is also critical to reveal disparities that remain hidden in aggregated global estimates. Creating national PD registries and linking them to wider non-communicable disease monitoring systems would improve data quality, strengthen policy planning, and help allocate resources more effectively at national and global levels.
Raising awareness and strengthening advocacy are important complements to surveillance efforts. Integrating PD into national public health agendas and broader non-communicable disease frameworks can help mobilize political commitment and resources for prevention and care. 4 Increasing public and professional awareness, through media campaigns, training programs for neurologists and other healthcare providers for early diagnosis and proper care, promoting healthier lifestyle patterns, strengthening patients’ support groups, is also key to reducing stigma, improving recognition of early symptoms, and shortening diagnostic delays, which remain substantial in many low- and middle-income countries. Education campaigns should leverage community engagement, patient-led initiatives, and digital media. 75 Including PD within disability and workplace-rights policies would further enhance social protection for individuals living with the disease and their caregivers.
Interventions targeting modifiable environmental and lifestyle factors are required to address the burden of PD. Policies should prioritize stricter regulation of pesticides and industrial solvents, such as paraquat and trichloroethylene, and of air pollution, all of which contribute to dopaminergic neurotoxicity. 87 Applying the precautionary principle is essential, shifting the responsibility for demonstrating chemical safety from researchers to manufacturers and regulators. 85 Stronger toxicological screening and surveillance systems are necessary to identify and mitigate exposures linked to PD, including biomonitoring programs to track population exposure to neurotoxic agents. Promoting protective healthy behaviors, including regular physical activity, can further lower risk. 88 Effective prevention also depends on intersectoral collaboration among health, environment, and labor sectors to align environmental safety and occupational health standards.
Improving timely diagnosis and effective treatment is crucial to lessen the growing global burden of PD. Strengthening primary care capacity through targeted education, task-sharing, and telemedicine can improve early detection and continuity of care, particularly in LIMCs.89–92 Digital health tools, including wearable sensors and artificial intelligence, can support remote monitoring, early detection, and more precise clinical decisions in PD care. 93 However, evidence quality remains limited in some aspects and several populations. Additionally, several challenges exist including loss of personal communication, limited technology savvy, insufficient and restrictive regulations in several countries, limited infrastructure and internet quality in LICs, patient acceptance and lack of reimbursement.90,91,94
Expanding access to essential medications, especially universal access to levodopa, is a critical step toward equity in care. Affordable, culturally adapted care models should integrate rehabilitation, mental health, and palliative care to address the full spectrum of patient needs. 3 Equally important is recognizing the burden carried by caregivers, who represent a central component of PD's social and economic impact. Providing caregiver education, psychosocial and financial support, and access to community-based resources should be a core element of comprehensive care strategies. Building a trained multidisciplinary workforce and involving non-specialist health professionals can further extend the reach and sustainability of PD care across diverse health system settings. Expanding tele-education can strengthen training for healthcare professionals in resource-limited regions, while closing the digital divide ensures these innovations benefit all populations equally.89,91
Advancing research and strengthening scientific capacity are key to closing global gaps in Parkinson's disease knowledge and care. Expanding and coordinating networks such as GP2 can improve data diversity and promote fair collaboration across regions. 26 Promoting studies led by researchers from LMICs or minority groups, along with the development of biobanking and genetic–environmental research tailored to local populations, will generate evidence that is both globally relevant and locally actionable. 95 Sustainable funding mechanisms and collaborations among LMICs are needed to strengthen infrastructure and scientific independence among currently underrepresented populations. 96 Research should focus on understanding the causes of PD through large-scale studies linking genes, environment, and exposures. It should also drive innovation in biomarkers, regenerative medicine, and artificial intelligence tools to improve early diagnosis and personalized care. 85 Finally, open-access data sharing and transparent, ethical governance of research resources are critical to ensuring inclusivity, reproducibility, and global benefit from PD research efforts.
Coordinated global action is essential to mitigate the growing burden of PD. 85 All efforts should align with the WHO Intersectoral Global Action Plan for Neurological Disorders 2022–2031, which calls for integrating PD into national non-communicable disease, aging, and disability strategies. 86 Countries should also include PD in insurance and reimbursement policies and ensure levodopa and other essential medicines are accessible through national formularies.19,75 Strengthening collaboration among key stakeholders can foster coordinated advocacy and knowledge exchange among the International Parkinson and Movement Disorder Society, the WHO, the World Federation of Neurology, and patient advocacy organizations. Expanding international funding mechanisms, such as the Michael J. Fox Foundation Diversity, Equity and Inclusion in Parkinson's Disease Research (DEI) initiative, Unitaid, and the Research on Interventions for Global Health Transformation (RIGHT) programme, will be crucial to supporting equitable research, workforce training, and access to care, ensuring that progress against PD benefits populations in all regions. 19
Several limitations affect accurate assessment of the global burden of PD. These include significant data gaps and the lack of hospital and population-based studies, particularly from LMICs and LICs, leading to reliance on less accurate modelled estimates. Furthermore, heterogeneity in methodology of data sources, along with disparities in diagnostic accuracy, genetic studies, mortality estimates and data collection and registry across regions, result in underestimation of global burden in LMICs. Additionally, the interplay of environmental, lifestyle, urbanization and genetic factors remain insufficiently studied and dissected, with limited understanding of relative contribution of these determinants.
Conclusion
PD has become a major global health priority that demands coordinated and cross-sector action. Addressing this challenge requires a shift from reactive management to proactive prevention, early detection, and system-wide preparedness. The growing burden of PD highlights both a moral and economic imperative to ensure that all populations, regardless of geography or resources, benefit from advances in research and care. Differences in prevalence, demographic, genetic and lifestyle factors, the impact of urbanization and environmental risk factors, as well as inequality and disparities in access to care and healthcare services, have been partially identified, mandating the development of tailored and region-specific strategies to mitigate the pandemic and reduce its burden globally and regionally. However, further studies and collaborative research are warranted. Furthermore, Global collaboration guided by the WHO framework is essential to prevent the burden of PD from surpassing the capacity of health systems worldwide.
Footnotes
Authors’ contributions
Study conception and design: Shalash A
Data acquisition, Data analysis and interpretation, Drafting of the manuscript: all authors
Critical revision of the manuscript for important intellectual content: all authors
Study supervision: Shalash A
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.