
Abstract
Parkinson's disease (PD) is the fastest-growing neurodegenerative disorder worldwide, with projections exceeding 25 million people by 2050. Its burden, however, is unevenly distributed. Many low- and middle-income countries face rapidly rising prevalence alongside profound shortages in neurological workforce, infrastructure, and access to specialised care and essential therapies. This global “Parkinson's divide” reflects not merely a funding gap, but a structural mismatch between disease burden and health-system capacity. Traditional clinic-centred models cannot scale to meet this expanding demand.
This article argues that technology, when responsibly implemented, offers a structural response to this capacity gap. Telemedicine expands access by decoupling specialist expertise from geography. Wearable and domestic sensor-based technologies extend clinical visibility beyond episodic encounters, capturing real-world fluctuations, mobility changes, falls, and sleep disturbances. Artificial intelligence, positioned as augmented rather than autonomous intelligence, can transform high-volume longitudinal data into actionable insights that support triage, task-sharing, and continuity across distributed care networks. Mobile health platforms further strengthen patient agency through structured self-management and co-designed digital ecosystems.
Yet innovation alone is not sufficient. Impact depends on feasibility, interoperability, workforce development, governance, and equity-first design, particularly in resource-constrained settings. Embedded within hybrid care models and life-course brain health frameworks, digital technologies can shift PD management from episodic symptom control toward longitudinal stewardship of function and resilience, helping to convert scarcity into distributed capability and narrow global inequities in Parkinson's care for our future generations.
Plain language summary title
Closing the global gap in Parkinson's care: How technology can help
Plain language summary
Parkinson's disease (PD) is increasing rapidly worldwide. However, access to diagnosis, treatment, and specialist care is not evenly distributed. Many low- and middle-income countries face rising numbers of people with PD but have very few neurologists, limited infrastructure, and barriers to long-term follow-up. This imbalance creates a “Parkinson's divide” between those who can access high-quality care and those who cannot.
This article explains how technology, when carefully and responsibly implemented, can help reduce this gap. Telemedicine can connect patients to specialists without requiring travel. Wearable devices and smartphone-based tools can monitor symptoms in daily life rather than relying only on brief clinic visits. Artificial intelligence can help clinicians interpret large amounts of health data and prioritise patients who need attention most urgently. Mobile health applications can also support self-management, education, and communication between patients and care teams.
However, technology alone is not enough. Digital tools must be affordable, usable, and adapted to local contexts. They must also avoid increasing inequalities, especially in communities with limited internet access or digital literacy. When integrated into hybrid models that combine in-person and remote care, and aligned with broader brain health strategies, digital innovations can expand specialist reach and strengthen care systems.
Closing the global Parkinson's divide requires thoughtful system redesign. With careful implementation, technology can help convert limited resources into broader, more equitable access to Parkinson's care worldwide.
Keywords
Introduction
Parkinson's disease (PD) is the fastest-growing neurodegenerative disorder worldwide, with projections suggesting that the number of people living with PD will exceed 25 million by 2050.1–3 Yet the impact of this growth is profoundly uneven. Many low- and middle-income countries (LMICs) face an accelerating burden driven by population ageing and urbanisation, whilst simultaneously contending with limited access to neurological services and essential PD therapies.4,5 In this context, the “global Parkinson's divide” should be viewed not simply as a funding gap, but as a capacity gap; a widening mismatch between disease burden and the workforce, infrastructure, and care pathways required to deliver timely diagnosis and longitudinal management at scale.
Traditional clinic-centred models are structurally constrained in meeting expanding global demand, particularly where workforce shortages and fragmented referral systems persist. 6 Even in high-income settings, specialist shortages and fragmented pathways constrain access and continuity; in LMICs these limitations are compounded by geography, travel burden, and under-resourced health systems, resulting in delayed or entirely missed diagnosis, suboptimal treatment, and persistent unmet need.4,7–10 As global neurology faces broader workforce and service-delivery constraints, closing the Parkinson's divide requires more than additional resources; it requires a deliberate redesign of how care is delivered.
Technological innovation offers a practical route to redesigning Parkinson's care by converting scarce expertise into scalable reach. 11 Telemedicine can expand access beyond geographic constraints, wearable and sensor-based technologies extend assessment into real-world settings, mobile health (mHealth) platforms support structured self-management and task-sharing, and artificial intelligence (AI) can transform high-volume longitudinal data into actionable clinical signals.12–15 PD is particularly amenable to this transformation because many of its core manifestations are observable outside the clinic and fluctuate over time, rendering episodic visits an incomplete reflection of lived disease burden.16,17
Importantly, technology is not a substitute for clinical judgement or human connection.18,19 Rather, it provides complementary information and enables hybrid models that preserve person-centred relationships while extending specialist reach through remote consultation and decision support.20,21 Within such models, different modalities address specific structural constraints: telemedicine improves access; wearable sensors enhance visibility through continuous monitoring; AI supports scalability by distilling complex data into interpretable insights; and mHealth strengthens patient agency through education and adherence support. Together, these interdependent components form a coherent care architecture (Table 1). Their effectiveness, however, depends on feasibility; specifically, whether digital solutions can be sustainably integrated into local health systems with appropriate infrastructure, workforce capacity, regulatory alignment, and cost considerations.
Technology-Enabled roadmap for bridging the global Parkinson's divide.
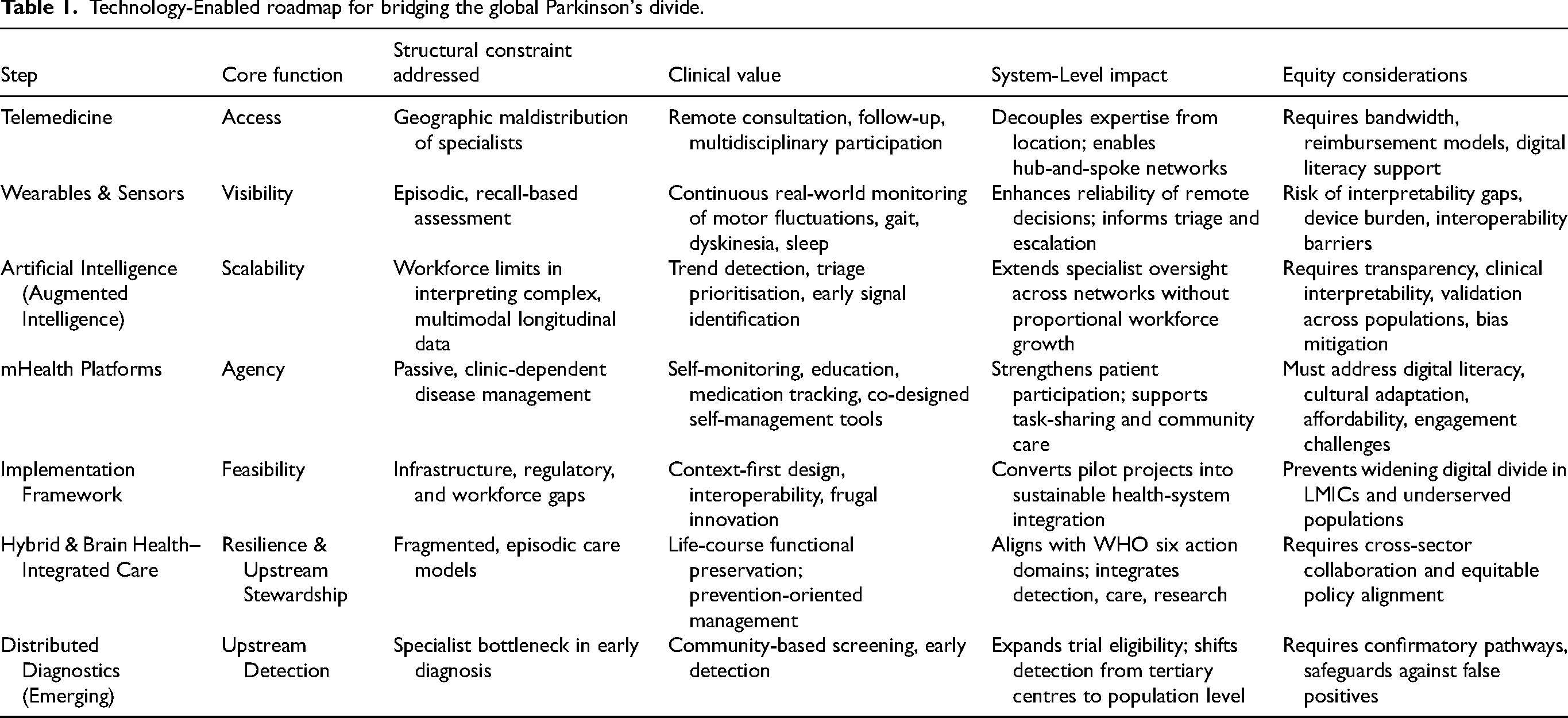
This article examines how the technological transformation of Parkinson's care can be strategically harnessed to reduce global inequities while embedding digital innovation within hybrid systems that promote long-term brain health and functional resilience. We synthesise evidence across telemedicine, and both wearable or domestic sensor-based monitoring, AI-assisted decision support, and mobile health interventions, and outline a pragmatic roadmap for scalable, equity-oriented care that seeks not merely to introduce new tools, but to rebalance capacity across health systems worldwide (Figure 1).
The global Parkinson's divide reflects a structural mismatch between rising disease burden and limited health-system capacity, characterised by workforce scarcity, episodic care, and reliance on subjective assessment. Technology functions as a structural bridge toward more equitable and sustainable models of care through four interdependent pillars: Access (telemedicine), Visibility (wearable and domestic sensor-based monitoring), Scalability (artificial intelligence), and Empowerment (mobile health platforms). Together, these components enable continuous, data-informed, and equity-oriented care. The smartphone-based application CheckPD, developed in Thailand, exemplifies a domestic digital platform supporting objective motor assessment and scalable screening within national health systems. 22
Taken together, these considerations signal a necessary paradigm shift in Parkinson's care: from models constrained by episodic, clinic-based specialist encounters to hybrid systems enabled by connectivity and distributed expertise. Rather than attempting to replicate traditional in-person structures at larger scale, connectivity allows specialist oversight, longitudinal monitoring, and coordinated care to extend beyond institutional boundaries. This shift does not imply that remote care replaces in-person interaction, nor that it is universally preferable. Indeed, fully remote models may reduce the depth of face-to-face engagement and are unlikely to substitute entirely for direct clinical encounters. Instead, the goal is to rebalance how and where the relationship between patients and medical professionals is sustained; combining in-person evaluation with remote follow-up, monitoring, and shared decision-making. The sections that follow examine how this hybrid transformation can be translated into practice, beginning with telemedicine as an immediate and scalable mechanism for expanding access to Parkinson's expertise.
Telemedicine as the first bridge: expanding access to Parkinson's expertise
Telemedicine is the most immediately deployable technology for narrowing the Parkinson's divide because it addresses the core constraint in global care: limited specialist capacity distributed unevenly across geography. Rather than requiring new physical infrastructure, telemedicine reconfigures how expertise is delivered, shifting from “where the specialist is” to “where the patient is.” Importantly, telemedicine does not depend exclusively on advanced digital platforms. Simple, widely available modalities, including structured telephone consultations, email communication, and asynchronous messaging, can meaningfully extend specialist reach, particularly in settings where broadband connectivity or video capability is limited.
The rapid expansion of telemedicine during the COVID-19 pandemic demonstrated both its feasibility and its scalability across diverse health systems. Movement disorder services worldwide transitioned to remote care within weeks, maintaining continuity for people with PD through video visits, telephone follow-up, and remote monitoring solutions.12,23 These experiences accelerated regulatory adaptation, reimbursement reform, and clinician acceptance, while also revealing practical limitations that underscore the importance of hybrid models.24,25
The American Academy of Neurology (AAN) position statement recognises telehealth as an integral component of neurological care, spanning synchronous and asynchronous communication, remote monitoring, and interprofessional consultation, while emphasising equity, clinical standards, reimbursement, and regulatory oversight. 26 In this sense, telemedicine functions as an access bridge: it reduces travel burden, mitigates geographic barriers, and enables scarce specialist input to be distributed more efficiently across larger populations. Early telehealth programmes were designed to improve access for rural and underserved communities, and the field has evolved from hospital-and-satellite models to home-based and mobile delivery for chronic disease management. 24 Within the broader connectivity framework, telemedicine represents the first operational step toward expanding equitable access to Parkinson's expertise.
Telemedicine modalities in Parkinson's disease: Synchronous, asynchronous, and hybrid models
Contemporary telemedicine in PD encompasses a spectrum of modalities, including synchronous real-time encounters (video or telephone), asynchronous or “store-and-forward” approaches (such as symptom diaries, recorded videos, messaging, and device-generated reports), and hybrid models that integrate both. 27 The selection of modality is typically guided by patient capability, digital literacy, bandwidth, and the clinical purpose of the encounter. From a clinical standpoint, PD is particularly amenable to remote assessment because many core manifestations are visually observable. 28 Bradykinesia, tremor, speech changes, facial expression, and gait, can be readily evaluated via video, and elements of oculomotor and coordination testing are also feasible. In contrast, rigidity, and static and dynamic balance, remain challenging to assess remotely without trained assistance. 29 These limitations do not undermine the value of telemedicine; rather, they delineate where hybrid workflows and local support roles are required to assure diagnostic and therapeutic confidence. 30
Telemedicine as a capacity-building model: Beyond one-to-one visits
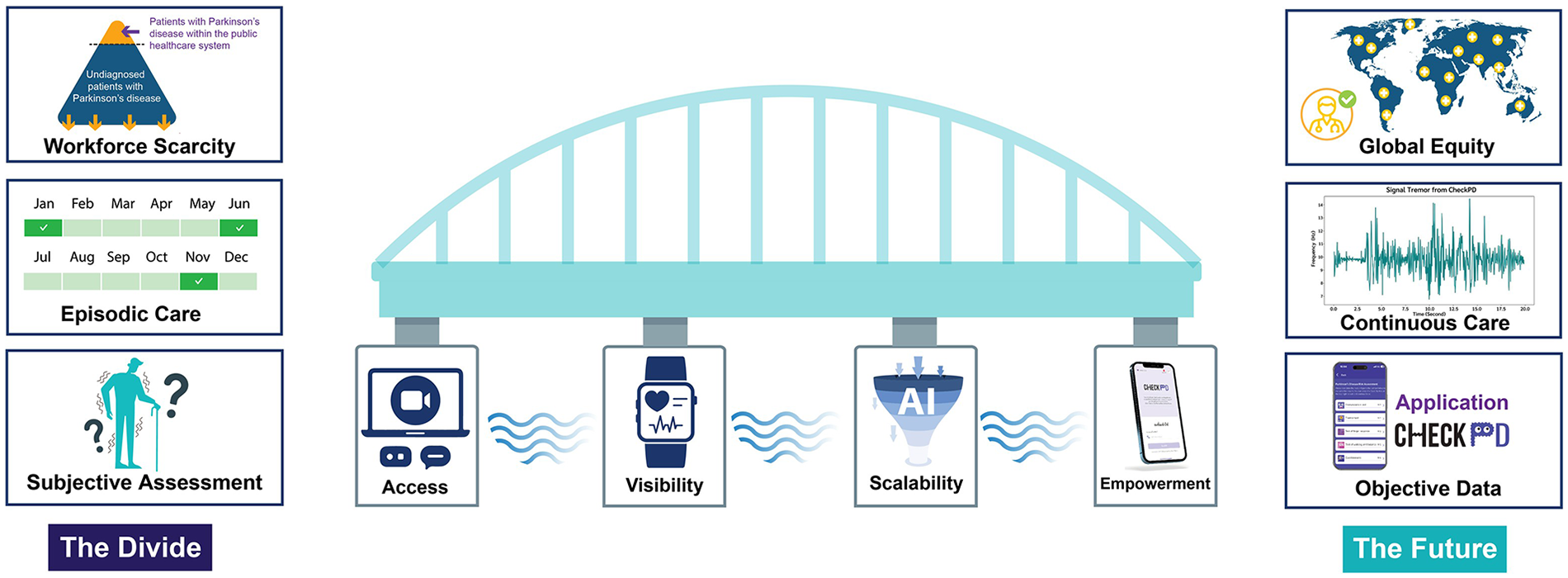
Telemedicine achieves its greatest impact when embedded within system-level care models that translate access into capacity at scale. Hub-and-spoke configurations allow specialist centres to support regional hospitals, primary care providers, and allied health teams through scheduled or on-demand teleconsultation, facilitating task-sharing, supervision, and standardisation of care; this includes peer-to-peer support delivered by specialists working within the hub, who supervise healthcare professionals locally working within the spoke model.21,31 Such models are particularly relevant in LMICs, where movement disorder specialists are scarce and concentrated in urban tertiary centres (Figure 2).
Hub-and-spoke telemedicine model for scalable Parkinson's care. Schematic representation of a specialist “hub” connected to multiple peripheral “spokes,” including regional hospitals, primary care facilities, village health workers, and mHealth-enabled community nodes. Clinical data, triage information, and patient-reported inputs flow from the spokes to the hub for specialist oversight, while training, supervision, and expert guidance are distributed outward from the hub to strengthen local capacity. Teleconsultation functions as the central coordination mechanism, enabling task-sharing, peer-to-peer support, and standardisation of care pathways. This bidirectional model transforms access into scalable capacity and is particularly relevant in low- and middle-income countries, where movement disorder specialists are concentrated in urban centres and rural populations face limited direct specialist access.
Clinic-to-clinic telemedicine further addresses digital inequities by providing local infrastructure, trained support staff, and a controlled environment for remote assessment, particularly for patients who cannot reliably engage in home-based video visits. Experience from rural research networks has demonstrated the feasibility of this approach in medically underserved populations, explicitly linking telemedicine to improved access and equity rather than convenience alone. 32 Multidisciplinary telehealth models extend this logic by enabling participation of rehabilitation professionals, speech and language therapists, nurses, and palliative care teams within shared care pathways, reducing fragmentation and improving continuity across settings. 33
Evidence base: Feasibility, acceptability, and clinical applications
Across multiple domains of PD care, telemedicine has demonstrated consistent feasibility and high acceptability. 25 Telemedicine visits need not be limited to a traditional clinical encounter. Sensor-supported telehealth studies show that people with PD are able and willing to complete home-based assessments with high compliance, and that remote management can support therapy adjustments comparable to standard care when objective data streams are incorporated. 34 Similarly, multimodal telemedicine programmes integrating video visits with mobile applications, cameras, and wearable sensors have reported sustained adherence and important usability insights, highlighting that clinical value depends less on the video encounter itself than on thoughtful workflow integration. 33
Telemedicine has also been successfully applied beyond routine follow-up. Telemedicine-supported initiation and home titration of levodopa–carbidopa intestinal gel has been reported as feasible, resource-efficient, and well accepted, reducing hospital bed utilisation and accelerating optimisation in selected patients. 35 In deep brain stimulation (DBS) care, early experiences with remote programming combined with online consultation suggest that aspects of post-operative management may be delivered at a distance with acceptable safety and feasibility in carefully selected populations, an observation of particular relevance for regions where travel to implant centres represents a major barrier. 36
Multidisciplinary telehealth: rehabilitation, speech, swallowing, and palliative care
Telemedicine has expanded access beyond specialist neurological consultations to the multidisciplinary services essential for comprehensive PD care. Telerehabilitation programmes in PD are generally feasible and well accepted, particularly due to reduced travel burden, although outcomes are most robust when digital delivery is combined with therapist guidance or telecoaching rather than fully self-directed approaches.37–40 In low-resource settings, including parts of Africa, telerehabilitation and community-based rehabilitation supported by remote supervision offer practical strategies to address allied health workforce shortages. 41
Management of speech-language alterations represents one of the most established applications of telehealth in PD. Tele-delivered voice and speech therapies have demonstrated outcomes comparable to in-person care in selected populations, supporting telemedicine as a viable access bridge where specialist services are limited.42–44 Telehealth for swallowing requires a more cautious interpretation. Remote swallowing assessment is feasible and can achieve good diagnostic agreement when structured protocols and trained clinicians are used, but evidence supporting tele-delivered swallowing rehabilitation remains limited.45,46 Recent expert guidance highlights the emerging role of asynchronous telehealth tools to support clinician decision-making and continuity of dysphagia care, complementing synchronous telepractice and in-person assessment rather than replacing them. 47
Telemedicine has also been applied to neuropalliative care in PD, extending symptom management and psychosocial support to patients with advanced disease who face increasing barriers to clinic attendance. Together, these applications underscore telemedicine's role in expanding access to multidisciplinary PD care through hybrid, context-sensitive models that balance digital delivery with appropriate in-person support. 48
Limitations and design principles for sustainable telemedicine
Despite its advantages, telemedicine does not eliminate the capacity gap in PD care. One-to-one specialist video visits alone cannot scale to meet the projected global burden of disease. Effective telemedicine therefore requires deliberate design choices, including hybrid scheduling with periodic in-person assessment, task-sharing with trained local staff who can assist with examination and safety, and integration with complementary digital tools such as patient-recorded videos, symptom diaries, and remote monitoring technologies.12,26,49 In several jurisdictions, including the United States, physicians must be licensed in the state where the patient is physically located at the time of consultation, restricting cross-state care and limiting the efficient redistribution of specialist expertise. Reimbursement policies likewise remain inconsistent across regions and payers, creating uncertainty for providers and constraining sustainable implementation. These principles align with broader calls to view telemedicine as an extension of care models rather than a simple substitution for in-person visits.
Positioning telemedicine within the connectivity framework
Within the framework of bridging the global Parkinson's divide, telemedicine functions as the first bridge because it directly improves access to scarce expertise. At the same time, its reliance on episodic encounters highlights the limitations of snapshot-based assessment. This inherent constraint provides the rationale for the next stage of technological integration: wearable sensors and other remote monitoring tools that enhance the visibility of symptoms between (or instead of) visits, followed by analytic approaches that support the scalability of interpretation and decision-making. Together, this progression reflects a systems-level approach to capacity expansion that keeps equity, feasibility, and sustainability at its core.
Wearable and domestic sensor-based technologies as the continuous eye: Extending visibility beyond the clinic
Wearable and domestic sensor-based technologies address this structural limitation by extending clinical visibility beyond the clinic. Body-worn accelerometers, gyroscopes, and smartphone-based measures enable continuous, real-world monitoring of mobility, motor fluctuations, and activity patterns, transforming assessment from recall-based reporting to objective longitudinal measurement. 50 Importantly, recent waveform-based analytic approaches demonstrate that high-resolution sensor signals can capture physiologically meaningful motor signatures rather than simple summary counts.51,52 These advances suggest that wearables are evolving from passive activity trackers to tools capable of extracting biologically interpretable motor biomarkers. In the context of the global Parkinson's divide, this shift is not merely technological; it strengthens the reliability of remote and task-shared care models, particularly in settings where specialist review is infrequent.
Why “visibility” matters in PD: From recall-based care to real-world measurement
PD symptoms fluctuate across hours and days, and key decisions, such as optimising levodopa schedules to address wearing-off or troublesome dyskinesia, or identifying the best intervention to address falls and gait instability, are often made with incomplete information. Technology trend analyses highlight that clinician judgement is inherently subjective and patient diaries are constrained by recall and compliance, motivating the need for objective, remote monitoring to assess severity and progression in unsupervised environments. 53 In this framing, wearables function as a clinical visibility layer that complements telemedicine by making remote decisions more reliable.
What sensors measure: Clinically interpretable signals (and what remains hard)
Across interventional PD trials, digital health technologies (DHTs), including wearables and smartphone sensors, have focused predominantly on core motor domains: bradykinesia, tremor, postural instability, and gait (including freezing), with smaller numbers assessing activities of daily living (ADLs), nocturnal activity, axial symptoms, and motor fluctuations.54–56 This matters because these domains are exactly where workforce scarcity is most visible: impairment in these domains often drive disability, falls, caregiver burden, and treatment escalation. 57 Importantly, many DHT platforms still perform best in supervised or semi-structured settings; fewer are designed for continuous, home-based monitoring. Yet the latter are the ones with distinctive clinical value; enabling granular measurement during daily-life activities that conventional assessments cannot capture.58,59 A broad sensor literature supports feasibility for quantifying tremor, bradykinesia and dyskinesia during daily living, as well as long-term gait monitoring with ambulatory systems.16,60,61
Increasing measurement precision does not necessarily translate into greater clinical meaning. Recent analyses caution against the “single digital biomarker hypothesis”, which assumes that individual or composite digital metrics can adequately represent overall disease severity or progression. 62 PD is a multidimensional syndrome with heterogeneous motor and non-motor manifestations; improvements in a narrowly defined digital motor measure may therefore coexist with clinically relevant deterioration in unmeasured domains. In addition, real-world digital signals are vulnerable to contextual confounding, including daily activities, environmental factors, and comorbid conditions, limiting the interpretability of isolated metrics. These considerations underscore that the value of wearables lies not in replacing clinical judgement with singular scores, but in enhancing visibility through multi-domain, longitudinal, and context-aware measurement that complements telemedicine and in-person assessment.
From prototypes to deployable tools: Maturity, validation, and “what can travel”
A practical question for the Parkinson's divide is: which tools are mature enough to travel across settings? In a recent systematic review of DHTs inclusion in drug trials, most commercial DHTs were rated at higher technology readiness levels (TRL 7–9), with many carrying regulatory designations (e.g., FDA Class I/II; CE mark), yet only a minority met high methodological quality thresholds, with substantial heterogeneity in digital endpoints and validation strategies. 54 These findings suggest that regulatory designation and technical feasibility do not automatically translate into a deployable clinical infrastructure.
Moving from validation to deployment therefore requires greater standardisation of digital endpoints, reporting methods, and data-quality procedures. 63 Practical steps include device-agnostic definitions of clinically meaningful change, transparent reporting of sensor placement, sampling frequency, algorithm version, and missing-data handling, and harmonisation of outputs so that results can be compared across platforms and settings. Regulatory guidance on digital health technologies similarly emphasises fit-for-purpose selection, verification and validation, usability in the intended population, and data integrity across the full measurement pathway.
This distinction is highly relevant for LMIC implementation: 64 scalable sensor strategies are more likely to succeed when they rely on (1) minimal hardware, (2) durable workflows, and (3) outputs that map onto decisions non-specialists can support (e.g., flagging suspected wearing-off patterns for medication review, or identifying fall-risk trajectories for allied health referral).
Clinical use-cases: Making remote management actionable
Wearables create clinical value when they close a decision loop; linking continuous measurement to specific actions such as medication adjustment, referral triage, rehabilitation targeting, or advanced therapy consideration. Continuous monitoring of motor fluctuations, gait instability, or dyskinesia burden becomes actionable only when thresholds or trajectories are mapped to defined escalation pathways within hybrid care models.
In interventional trial settings, the Roche PD Mobile Application is presented as a scalable smartphone-based platform used in large multicentre studies (e.g., PASADENA), with sensor features reported as sensitive to treatment effects consistent with clinical bradykinesia subscores. 65 While trial-readiness does not automatically translate to routine care, it provides an important pathway: validation in controlled environments can de-risk later clinical adoption, particularly in settings where clinicians need confidence before changing workflows.
For the Parkinson's divide, the key question is not whether sensors can measure tremor or gait, but whether their outputs can guide decisions in settings where specialist capacity is limited. Actionable use-cases may include flagging suspected wearing-off for medication review, identifying rising fall risk warranting allied health referral, or detecting functional decline that prompts earlier specialist input. When embedded within telemedicine workflows and supported by defined triage protocols, wearables shift from passive measurement tools to active components of scalable care infrastructure.
Data overload, interpretability, and equity-by-design
A recurring barrier is not the quantity of data, but its clinical meaning. Even when devices are feasible and technically robust, many DHT outputs (e.g., gait variability indices, entropy measures, spectral power features) remain unfamiliar to clinicians and lack intuitive interpretability, which undermines confidence and limits routine use in therapeutic decision-making. 54
This interpretability challenge extends beyond statistical complexity to practical integration. Even well-validated digital metrics may fail to influence care if they do not map clearly onto therapeutic decisions, escalation pathways, or triage thresholds. For clinicians, particularly those working in non-specialist or resource-constrained settings, data must answer concrete questions: Is motor fluctuation worsening? Has fall risk increased sufficiently to warrant allied health referral? Is functional decline emerging that justifies medication adjustment? In practice, additional barriers compound this challenge: 66 fragmented platforms that require multiple logins, dashboards that present high-dimensional data without prioritisation, device burden that reduces adherence, and limited interoperability with electronic health records. Without integration into routine workflow and clear clinical anchoring, high-resolution digital outputs risk functioning as parallel information streams rather than embedded components of care. Building credibility therefore requires not only technical validation but also usability, workflow alignment, and outputs that translate into actionable decisions. In practical terms, this means that digital dashboards should prioritise clinically interpretable summaries rather than display undifferentiated raw data streams. Outputs should be linked to predefined care pathways, such as medication review for suspected wearing-off, referral to physiotherapy for rising fall risk, or specialist review for rapid functional decline. For use in non-specialist or resource-constrained settings, thresholds should be simple, transparent, locally validated, and accompanied by guidance on what action should follow.
Encouragingly, large initiatives such as Mobilise-D and IDEA-FAST are addressing these credibility gaps by aligning validation with clinical relevance and patient priorities. Mobilise-D is developing and validating digital mobility outcomes (e.g., gait speed) with regulatory collaboration, 67 while IDEA-FAST is developing digital measures of fatigue and daytime sleepiness; symptoms patients consistently identify as highly disabling yet poorly captured by conventional assessment, explicitly incorporating patient input and co-design.68,69 For a Parkinson's divide narrative, these programmes help model how “visibility” can be built responsibly: standardised, interpretable, and anchored to outcomes that matter to patients across contexts.
Bridge forward to AI: Visibility creates the need for scalability
Continuous monitoring generates richer signals but shifts the bottleneck to scalable interpretation; who interprets these streams, and how can interpretation scale when workforce capacity is limited? This naturally sets up the next section; AI as the scalability layer, supporting triage, summarisation, and decision support without displacing clinicians.
Artificial intelligence as a force multiplier: Scaling expertise without replacing clinicians
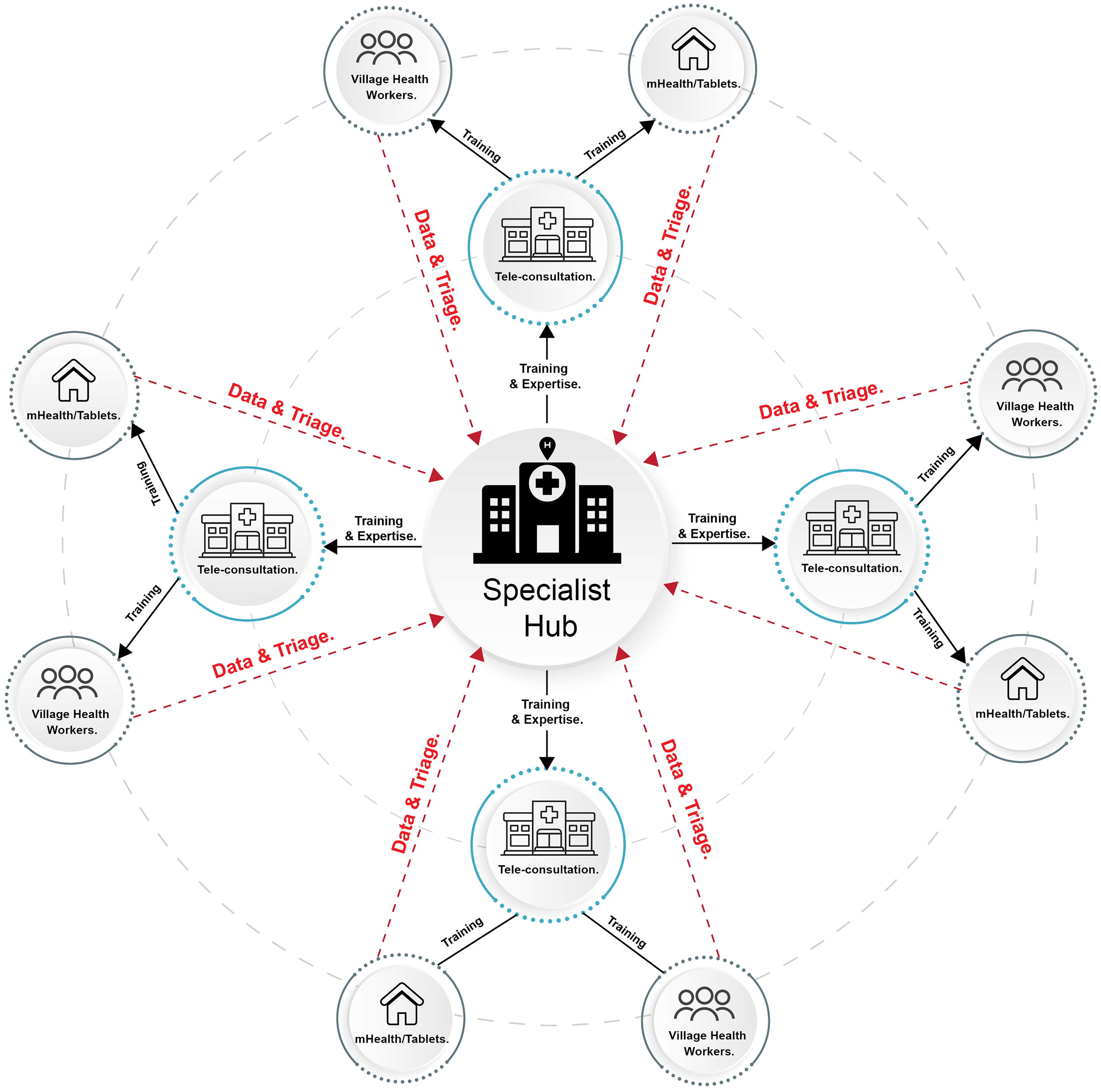
Wearable sensors and remote monitoring extend clinical visibility beyond episodic encounters, but visibility alone does not resolve the capacity constraints inherent in PD care. As longitudinal data accumulates across large patient populations, the central challenge shifts from data collection to interpretation at scale (Figure 3). Without analytic support, continuous monitoring risks overwhelming clinicians rather than enabling more timely and equitable care. 70
Wearable sensors and smartphone-based platforms generate high-frequency raw digital signals (“big data”), including accelerometry and task-based motor recordings. Artificial intelligence (AI) processes these streams into structured, interpretable outputs (“smart data”) that support triage, risk stratification, and clinical decision-making within hybrid care models. CheckPD, a smartphone-based platform developed in Thailand, illustrates how locally adapted digital tools in low- and middle-income countries can translate real-world data into actionable reports (e.g., “at risk” vs “no risk”), supporting scalable and equitable expansion of Parkinson's expertise. 22
Human clinicians excel at contextual reasoning and complex decision-making but are poorly suited to continuous, high-frequency data triage across large patient populations. 71 In this context, AI should be understood as an enabling layer that supports scalability across technology-enabled care models. By summarising complex data streams, identifying clinically relevant change, and prioritising patients for review, AI allows limited specialist expertise to be applied more efficiently across growing cohorts. Importantly, this role is complementary rather than substitutive: AI augments clinical judgement and supports decision-making, while responsibility for diagnosis and treatment remains with clinicians. 71
Artificial intelligence for early detection and longitudinal monitoring: From patterns to action
The need for AI-enabled interpretation is particularly evident in the early detection of PD because clinically meaningful change often emerges insidiously. 72 Growing evidence indicates that motor abnormalities, including changes in gait rhythm and variability, arm swing asymmetry, finger tapping dynamics, speech and voice features, and nocturnal motor activity, can precede clinical diagnosis by years and may remain undetectable during routine neurological examination.73–78 Identifying such signals in real-world settings requires analytic approaches capable of integrating multimodal data across time, distinguishing disease-related patterns from ageing, comorbidity, and contextual variability. 72 AI methods are well suited to this task, supporting the detection of deviations from individual baselines that may warrant early referral, closer monitoring, or preventive intervention.22,79
Beyond early detection, AI plays a critical role in longitudinal disease monitoring, where treatment response, symptom fluctuation, and progression unfold nonlinearly over months and years.80–82 In PD, clinically actionable change may present as shortening of ON time, increasing gait instability, rising dyskinesia burden, or fragmentation of sleep; patterns that are difficult to recognise through episodic assessment alone. AI systems can summarise continuous data streams, identify clinically relevant trends, and prioritise patients for review, thereby converting data abundance into actionable insights that inform medication adjustment, allied health referral, or advanced therapy consideration.58,59
Augmented intelligence for clinical decision support: From data to shared judgement
As AI is introduced into PD care, its most appropriate and immediately useful role is as augmented intelligence, sometimes described as co-intelligence; systems designed to work with clinicians rather than replace them.83,84 In contrast to fully autonomous models, augmented intelligence emphasises human oversight, transparency, and shared judgement, positioning AI as a cognitive aid that enhances clinical reasoning while preserving accountability and patient–clinician relationships. 71
In practical terms in PD, augmented intelligence supports clinicians by organising, summarising, and contextualising complex longitudinal data generated through telemedicine, wearable sensors, and patient-reported inputs. Rather than presenting opaque risk scores or binary outputs, such systems aim to highlight clinically relevant changes, such as emerging wearing-off patterns, increasing gait instability, rising dyskinesia burden, or deviations from an individual's baseline, thereby supporting more informed and timely decision-making. This approach aligns with the realities of PD care, where management decisions are rarely algorithmic and must be individualised, iterative, and responsive to patient priorities. 85
In our view, augmented intelligence is particularly valuable in hybrid and remote care models, where direct physical examination may be limited and clinical decisions increasingly rely on indirect evidence. By synthesising multimodal data into interpretable summaries, AI can reduce cognitive load, mitigate information overload, support consistency across providers with varying levels of expertise, as well as patients to mitigate the impact clinician bias.62,86 This is especially relevant in settings where PD care is delivered by general neurologists or non-specialist clinicians. In such contexts, AI systems trained on specialist-validated datasets can embed expert-derived thresholds, pattern recognition, and escalation criteria into routine workflows, thereby extending specialist-informed decision support without requiring continuous direct oversight. Importantly, augmented intelligence reframes AI outputs as structured inputs into shared clinical judgement rather than autonomous determinations of care. Decisions regarding diagnosis, treatment adjustment, referral, or escalation remain clinician-led, informed by patient context, preferences, and values. In this sense, augmented intelligence strengthens, not weakens, the human dimensions of PD care, enabling clinicians to focus attention where it is most needed while maintaining responsibility for outcomes. 87 By anchoring AI within a co-intelligent model of care, this approach creates a clear bridge between individual-level insight and system-level scalability, ensuring that AI contributes meaningfully to capacity expansion without eroding trust or autonomy.
AI for system-level scalability: Extending specialist reach across care networks
Beyond individual-level detection and monitoring, the most transformative role of AI in PD care lies at the system level. Health systems facing widening gaps between disease burden and specialist capacity require mechanisms that allow expertise to be distributed across networks of non-specialist providers, community services, and hybrid care pathways. 21 In this context, AI functions as an infrastructure tool that supports scalability by enabling population-level oversight rather than case-by-case specialist review.
At scale, AI-enabled systems can support prioritisation across large cohorts by identifying patients with emerging signs of PD who require specialist evaluation or those with established PD who require timely escalation of care, thereby allowing limited specialist resources to be allocated more efficiently. Such approaches are particularly relevant in LMICs, where movement disorder specialists are scarce and care is often delivered by general neurologists or primary care teams.88–91 By embedding AI-assisted summaries and alerts within telemedicine and wearable-enabled workflows, specialist expertise can propagate through hub-and-spoke or networked models of care without requiring proportional increases in workforce size. 92 As such, this role of AI is organisational rather than diagnostic. Its value lies in supporting care coordination, triage, and task-sharing, rather than generating autonomous clinical decisions. When aligned with clearly defined care pathways, AI can help stabilise workloads, reduce inequities in access to specialist review, and improve continuity across settings, directly addressing the capacity mismatch that underpins the Parkinson's divide.
Trust, governance, and equity: Conditions for responsible scaling
The ability of AI to function as an infrastructure-level enabler in PD care depends not only on technical performance, but on trust, governance, and equitable design. Reviews of AI-enabled approaches in PD and digital neurology consistently emphasise that systems must be transparent, clinically interpretable, and validated across diverse populations to avoid embedding bias or exacerbating existing inequities, particularly in low-resource settings.93–95 Models trained predominantly on data from high-income countries risk poor generalisability when deployed in contexts with different demographics, comorbidity profiles, care pathways, and technological access. The central question is not whether AI can detect PD in controlled datasets, but whether it can do so equitably across diverse populations and health systems without amplifying structural disparities.
From a global health perspective, equity-aware AI design requires deliberate attention to feasibility, data representativeness, and deployment context. Lightweight models that operate on intermittent or low-bandwidth data, integrate with existing telemedicine platforms, and produce outputs that can be acted upon by non-specialist providers are more likely to achieve real-world impact than complex systems that depend on continuous high-resolution data streams or proprietary infrastructures. Algorithms trained predominantly on Western cohorts may perform differently in populations with distinct anthropometrics, habitual gait patterns, comorbidities, and environmental exposures. Without deliberate validation across diverse settings, AI deployment risks embedding structural bias into triage and referral systems.96,97 Data privacy and governance must also be addressed from design through deployment.98,99 Responsible AI-enabled PD care should incorporate data minimisation, transparent consent processes, role-based access, secure storage and transmission, clear accountability for secondary data use, and ongoing monitoring for performance drift. In cross-border or hub-and-spoke models, governance arrangements should clarify where data are stored, who can access them, how long they are retained, and how patients can understand or challenge AI-supported recommendations. Governance frameworks that ensure human oversight, accountability, and ongoing performance evaluation are therefore essential to prevent automation from amplifying, rather than mitigating, disparities.100,101
Together, these considerations reinforce that AI's contribution to Parkinson's care is not determined by algorithmic sophistication alone, but by how responsibly it is embedded within health systems. When aligned with principles of transparency, equity, and clinical accountability, AI can support scalable, hybrid models of care that extend specialist oversight while remaining sensitive to local constraints and global diversity. 102
mHealth & empowerment: The patient as partner (agency)
If telemedicine addresses access, wearables enhance visibility, and AI supports scalability, mobile health (mHealth) introduces a complementary dimension that is equally critical to narrowing the Parkinson's divide: agency. In PD, the lived experience of symptoms and the day-to-day adjustments in medication timing, activity levels, rest, and coping strategies occur primarily outside the clinic. While formal treatment decisions remain clinician-led, they are increasingly informed by patterns, behaviours, and symptom fluctuations that unfold in patients’ daily environments. 103 Sustainable care models therefore require not only specialist reach, but meaningful patient participation in observing, reporting, and responding to their condition between consultations.
Sustainable patient agency in PD is not achieved through information provision alone, but through structured, theory-informed self-management approaches that are co-designed with people living with the condition. Recent work developing a facilitated self-management toolkit for PD demonstrated the value of iterative co-design involving patients, carers, and multidisciplinary professionals, resulting in a personalised, asset-based platform that integrates symptom review, goal setting, behaviour change techniques, and structured supporter sessions. 104 This model illustrates that empowerment is most effective when digital tools are embedded within relational support, cultural adaptation, and shared decision-making frameworks, with the concept proposed in early-onset patients. 105 In this sense, mHealth should not be conceptualised as a standalone application, but as part of a co-designed ecosystem that strengthens partnership between patients, carers, and healthcare systems.
From monitoring to activation: Strengthening self-management
In chronic neurological diseases, empowerment is not merely informational; it is behavioural. Digital tools that allow patients to visualise symptom patterns, recognise wearing-off phenomena, or track response to exercise can improve insight into disease fluctuations and encourage proactive communication with care teams. 106 Such structured self-monitoring may also reduce reliance on retrospective recall during consultations, enhancing clinical efficiency while reinforcing shared decision-making.
Evidence from digital health studies suggests that patient activation improves when tools are intuitive, provide meaningful feedback, and are linked to clinician engagement rather than operating independently.107,108 In PD specifically, app-based platforms that combine tracking with structured education have demonstrated feasibility and high user engagement, particularly when co-designed with patients and tailored to their lived experience.109,110 These observations reinforce that mHealth supports agency not by replacing clinicians, but by strengthening the partnership between clinic and home.
Cultural adaptation and context sensitivity
From a global health perspective, empowerment cannot be separated from context. Tools designed for high-income, digitally literate populations may not translate directly to settings where smartphone access is variable, literacy levels differ, or cultural perceptions of chronic disease shape health behaviours. The risk is that poorly adapted mHealth interventions widen the Parkinson's divide by benefiting only those already digitally advantaged.
Equity-oriented mHealth design therefore requires deliberate attention to language, health literacy, and cultural norms. 111 Simplified interfaces, multilingual content, voice-based instructions, and offline functionality can enhance inclusivity. In Southeast Asia, locally developed PD applications have demonstrated improved engagement when co-created with patients, caregivers, and community clinicians, ensuring that educational materials reflect regional beliefs, caregiving structures, and healthcare pathways. 22 These examples illustrate how mHealth can strengthen agency without imposing a uniform technological model across diverse contexts.
mHealth as an enabler of task-sharing and community care
Beyond individual empowerment, mHealth platforms can support broader task-sharing strategies. Structured symptom reports, digital medication logs, and standardised self-assessments can assist non-specialist providers in monitoring patients between specialist consultations. 112 In LMIC settings, where neurologist density remains low, such tools may allow community health workers or general practitioners to deliver more confident and consistent PD care under remote supervision. In this sense, mHealth contributes to capacity expansion not only by activating patients, but by strengthening communication across the care network. 113 When patient-reported data are integrated into telemedicine workflows and supported by AI-assisted triage, the result is a multi-layered system in which agency, access, visibility, and scalability reinforce one another.
Limitations: Engagement, digital fatigue, and sustainability
Despite its promise, mHealth is not inherently empowering. Engagement often declines over time, particularly when applications provide limited feedback or require excessive manual input. 114 Digital fatigue, privacy concerns, and socioeconomic barriers can further limit sustained use. Moreover, many applications remain pilot projects without long-term integration into national health systems or reimbursement frameworks.
For mHealth to meaningfully reduce the Parkinson's divide and enhance patient agency, it must move beyond isolated innovation toward sustainable implementation. This includes interoperability with electronic health records where available, alignment with clinical guidelines, and integration into hybrid care pathways rather than functioning as optional add-ons. 115
Implementation challenges: The reality check (feasibility)
The preceding sections have outlined how telemedicine can expand access, wearables can enhance visibility, AI can support scalability, and mHealth can strengthen patient agency. Yet none of these advances guarantee equitable impact. Whether technology narrows or inadvertently widens the Parkinson's divide depends in large part on implementation.116,117
These constraints are most visible in LMICs, where workforce shortages and infrastructure gaps amplify the capacity imbalance.2,117 In such settings, feasibility becomes the decisive test of innovation: can digital solutions operate within systems with intermittent connectivity, constrained budgets, and evolving regulatory environments? Technologies that assume continuous broadband access, availability of specialised hardware, or high levels of digital literacy may inadvertently widen inequities if deployed without adaptation. 118 Implementation, therefore, must consider the context-first, ensuring that digital models are robust, affordable, and aligned with local capacity. Only then can technological innovation translate into structural sustainable care models rather than isolated demonstration projects.
The digital divide within the Parkinson's divide
System-level feasibility challenges are mirrored by patient-level inequities that risk compounding the Parkinson's divide. 9 Even where national digital infrastructure is expanding, access to and effective use of technology remain uneven across age, geography, income, education, and disability. Many people living with PD are older adults who may have limited digital literacy, reduced confidence using smartphone applications, or motor and cognitive impairments that complicate device interaction. 119 Rural communities may experience unstable connectivity, and device ownership alone does not guarantee functional usability or sustained engagement. 120
Evidence from under-represented groups suggests that digital literacy, rather than culture per se, is often the primary barrier to meaningful digital self-management. 121 Confidence with technology, prior exposure, assistive needs (e.g., visual or auditory impairment), affordability, and ongoing technical support frequently determine engagement. However, structural inequities remain highly relevant: access to assistive technologies, reliable broadband, multilingual platforms, and culturally adapted content continues to be unevenly distributed. Digital health systems developed primarily in high-income settings may inadvertently assume seamless smartphone navigation, wearable synchronisation, and portal-based communication; assumptions that risk excluding precisely those populations with the least access to specialist neurological care. 122 For digital innovation to narrow rather than widen inequity, feasibility must be operationalised at the design stage.123,124 This includes offline functionality, low-bandwidth compatibility, simplified interfaces, multilingual and culturally adapted resources, and compatibility with assistive technologies. These features are not enhancements; they are equity safeguards. Without deliberate inclusive design, technology-enabled PD care risks reinforcing existing disparities under the banner of innovation.
Workforce capacity: Technology does not replace training
Technology does not eliminate human capacity constraints; it reshapes them. Telemedicine-supported referral systems and digital triage models can strengthen specialist networks, but require parallel investment in workforce training and workflow redesign. Recent analyses of digital referral pathways highlight that technology improves continuity only when embedded within clear governance structures and defined escalation pathways. 118 In LMICs especially, AI and digital tools must augment non-specialist providers rather than replace clinical judgement. 94 AI in global health contexts is most impactful when it strengthens existing systems rather than attempting to bypass them.
Regulatory, infrastructure, and interoperability barriers
Digital health implementation faces persistent systemic barriers. As shown in the field of telemedicine as the example, different challenges were identified, including legal uncertainty, reimbursement limitations, licensing constraints, lack of insurance coverage, insufficient bandwidth, and ambiguity in IT infrastructure.33,125 These challenges are amplified in cross-border teleconsultation and remote device programming scenarios. Furthermore, interoperability remains fragmented. 126 Overcoming these barriers requires treating interoperability, privacy, and workflow integration as core design requirements rather than downstream technical problems.
Practical steps include adopting open data standards and application programming interfaces where feasible, mapping device outputs to clinically meaningful concepts, and designing dashboards that can integrate with existing electronic health records or low-resource alternatives. Standards such as HL7 Fast Healthcare Interoperability Resources (FHIR) provide one route for structuring and exchanging health information electronically, although implementation must be adapted to local infrastructure and regulatory capacity. 127 Privacy safeguards should include data minimisation, secure transmission, role-based access, locally appropriate consent processes, and clear accountability for data stewardship. Finally, implementation should proceed in stages: local needs assessment, workflow co-design, small-scale usability testing, training of clinicians and support staff, evaluation of implementation outcomes, and scale-up only when feasibility, safety, cost, and equity effects are demonstrated.
Frugal innovation and context-first design
Addressing implementation barriers requires contextual discipline rather than technological maximalism. AI applications in resource-poor settings have demonstrated that success depends on building intelligence into existing systems rather than replacing them. 128 In PD care, this principle suggests prioritising: (1) Smartphone-based tools over proprietary hardware, (2) Hybrid care models over fully digital substitution, and (3) Scalable platforms compatible with low-bandwidth environments. Digital self-management interventions in LMIC contexts show that usability, cost, and integration into daily life determine uptake more than technical sophistication. Frugal innovation, designing robust, affordable, adaptable systems, is therefore central to narrowing the Parkinson's divide.
From pilot projects to sustainable systems
Digital health initiatives often remain confined to demonstration projects. For technology to structurally reduce inequity in PD, implementation must be accompanied by outcome evaluation, cost-effectiveness analysis, and health-system alignment.123,129,130 Evidence from digital literacy research in PD suggests that without targeted support, digital expansion may preferentially benefit higher-income, technologically confident populations. 119 Feasibility, therefore, is the bridge between innovation and equity. Embedding digital tools within pragmatic trials, co-designed service models, and policy-aligned reimbursement structures is essential to avoid deepening disparities. Evaluation should therefore extend beyond clinical accuracy to implementation outcomes, including acceptability, adoption, appropriateness, feasibility, fidelity, implementation cost, penetration, and sustainability. 131 Measuring these outcomes is especially important in LMICs, where a tool that performs well technically may still fail if it is unaffordable, poorly integrated into workflow, or unusable by the intended workforce or patient population.
A global roadmap: From technological innovation to brain health–integrated Parkinson's care
Closing the global Parkinson's divide requires more than digital adoption. It requires coordinated redesign: aligning technology with workforce development, governance, financing, and public health priorities. This section outlines a pragmatic roadmap for embedding digital innovation within hybrid care architectures that are scalable, equity-oriented, and aligned with global brain health strategies.
Hybrid care and responsible scaling
Hybrid care models represent the operational backbone of a technology-enabled PD system. Rather than replacing in-person care, hybrid configurations combine periodic face-to-face evaluation with structured telemedicine follow-up, remote monitoring, and digitally supported triage. In doing so, specialist expertise becomes distributed across networks of general neurologists, primary care providers, allied health teams, and community settings, rather than remaining concentrated in tertiary centres. 21
For such systems to narrow inequities rather than widen them, scaling must be deliberate. Digital tools must be usable across varying levels of connectivity, literacy, and workforce capacity.122,132 Human oversight, interoperability, and sustainable financing are not secondary considerations; they are preconditions for equity. In this framing, success is measured not by technological sophistication, but by improved access, preserved function, and reduced disparities across populations. A pragmatic sequence for responsible scaling is therefore needed. First, the clinical problem and target population should be defined locally. Second, the digital tool should be validated in the intended population and workflow. Third, outputs should be integrated into clear care pathways with assigned responsibilities for triage, escalation, and follow-up. Fourth, privacy, governance, and reimbursement arrangements should be established before broad deployment. Finally, scale-up should be accompanied by continuous monitoring of clinical outcomes, implementation outcomes, and equity effects.
This roadmap aligns closely with the six action domains proposed by the WHO to reduce global disparities in PD. 4 Strengthening hybrid models directly addresses inequities in diagnosis, treatment, and care; telemedicine and workforce extension strategies mitigate neurological workforce shortages; mHealth and awareness initiatives contribute to advocacy and empowerment; and data-enabled systems support improved disease burden measurement and research capacity. By embedding digital innovation within public health architecture rather than isolated pilot projects, technology becomes a practical instrument for advancing these global action priorities across diverse health systems.
Looking forward, the concept of distributed diagnostics for early detection of individuals at high-risk for or with early PD offers an additional strategic lever to reduce global disparities. 133 Emerging models propose leveraging personal digital health technologies, community-based testing platforms, non-traditional clinical venues (such as pharmacies, dental and optometry services), and scalable biomarker assays to identify prodromal or early-stage PD beyond specialist clinics.11,22 Such approaches may expand access to secondary prevention strategies and early evaluation in regions with limited neurological workforce capacity. However, distributed detection must be coupled to ethical safeguards, confirmatory pathways, and specialist referral networks to avoid harm from false positives or inequitable follow-up access. When integrated within hybrid care systems, distributed diagnostics may help shift Parkinson's care upstream; transforming detection from a specialist bottleneck to a population-level capability.
Integrating brain health into technology-enabled PD care
The transformation of PD care should be aligned with a broader shift toward brain health across the life course. 134 Brain health, increasingly defined as preservation of multidimensional function across the life course, has been articulated in international frameworks from WHO and major neurological societies and is highly relevant to PD. All of these brain health frameworks emphasise integrated, prevention-oriented, and system-level approaches to neurological health across the lifespan rather than siloed disease management.135–138 Importantly, this does not imply a uniform clinical pathway. PD is biologically and clinically heterogeneous, with variable motor subtypes, non-motor burden, progression rates, and treatment responses. A brain health framework therefore provides a shared organising principle, not a single algorithm. 139 It encourages, for example, coordinated attention to modifiable determinants of dementia, such as vascular health, sleep, physical activity, mood, and social engagement, while allowing care models to remain personalised, context-sensitive, and responsive to individual trajectories.
With this framework in mind, technology-enabled care provides a practical mechanism to operationalise this brain health perspective within the context of PD care and prevention. 140 Wearables can promote and monitor mobility and activity; telemedicine can extend access to multidisciplinary care; mHealth platforms can support education and behavioural change; AI may assist in identifying early deviations that warrant preventive intervention. In this model, digital innovation becomes a vehicle for sustaining neurological function rather than merely managing symptoms. Integrating brain health reframes PD care from episodic intervention to longitudinal stewardship of function (Figure 4). It reinforces the principle that narrowing the Parkinson's divide requires not only expanding specialist reach, but strengthening resilience across communities and life stages.

A roadmap for bridging the global Parkinson's divide through technology-enabled hybrid care. This schematic illustrates the progression from the current global Parkinson's divide, characterised by rising disease burden and limited specialist resources, towards more equitable and sustainable models of care. The pathway highlights sequential and interdependent components: telemedicine as the first bridge to expand access; wearables and sensors to extend visibility beyond the clinic; artificial intelligence to scale expertise without replacing clinicians; mHealth to strengthen patient agency; and context-sensitive implementation to ensure feasibility and equity. These elements converge in integrated, hybrid models of Parkinson's care aligned with broader brain health principles. Thailand is highlighted as one illustrative example of a low- and middle-income country (LMIC) where national digital initiatives are being developed to operationalise such approaches. The inclusion is intended to demonstrate feasibility in real-world LMIC contexts, rather than to suggest a singular or exclusive model. Similar context-adapted strategies are emerging across diverse regions, underscoring that scalable, equity-oriented solutions can be locally developed and globally relevant.
Summary and outlook
PD is expanding at a pace that traditional models of care cannot accommodate. The global Parkinson's divide is not simply a disparity in funding or technology; it is a structural mismatch between disease burden and health-system capacity. Attempting to scale conventional, clinic-centred neurology to meet rising global demand is neither feasible nor sustainable.
The technological revolution in healthcare offers an alternative pathway. Telemedicine improves access by decoupling specialist expertise from geography. Wearables enhance visibility by extending assessment beyond episodic encounters. Artificial intelligence supports scalability by transforming continuous data into actionable insights. mHealth strengthens agency by positioning patients as informed and engaged partners in longitudinal care. When guided by feasibility, interoperability, workforce development, and equity-first implementation, these components form a coherent framework for redesign rather than isolated innovations.
Yet technology alone is insufficient. Its value depends on disciplined system integration and must align with broader brain health principles that prioritise preservation of function, risk modification, resilience, and life-course stewardship rather than episodic symptom control or disease-specific management. Such integration ensures that innovation strengthens neurological capacity rather than fragments it. Closing the Parkinson's divide therefore requires intentional system transformation. It demands cross-sector collaboration, context-sensitive implementation, responsible governance of AI, and sustained investment in workforce development alongside digital infrastructure. The goal is not a fully digital future, nor a nostalgic return to traditional models, but a hybrid, networked system capable of converting connectivity into equitable reach.
The globalisation of PD requires a globalised response. When responsibly implemented, technology can convert scarcity into distributed capability, expand specialist oversight without proportional workforce growth, and embed brain health principles into everyday care. Bridging the global Parkinson's divide is ultimately not a technological challenge alone; it is a systems challenge. Technology becomes transformative only when it strengthens the human and institutional foundations of neurological care worldwide.
Footnotes
Author contributions
RB: Conceptualisation; Methodology; Visualisation; Formal analysis; Writing – original draft, review & editing
RS: Writing-review & editing
WM: Writing-review & editing
AJE: Writing-review & editing
TTL: Writing-review & editing
APh: Writing-review & editing
HK: Writing-review & editing
APi: Writing-review & editing
BRB: Conceptualisation; Writing-review & editing
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the following grants; the Thailand Science Research and Innovation Fund (Program Management Unit for Competitiveness, C01F670185), the National Economic and Social Development Council, Thailand Center for Excellence for Life Sciences (TC (ERP) 31/2568), National Research Council of Thailand (N42A680591, N35E680087), Ratchadapiseksompotch Fund (RA-MF-22/69) and the Center of Excellence grant (CE68_028_3000_004), both awarded by Chulalongkorn University, and the Thai Red Cross Education and Research Committee Fund.
Competing interests and financial disclosures of all authors
RB has received grants from the following agencies: The Thailand Science Research and Innovation (TSRI, Programme Management Unit for Competitiveness, C01F670185), the National Economic and Social Development Council of Thailand, Thailand Centre of Excellence for Life Sciences (TC (ERP) 31/2568), the National Research Council of Thailand (N42A680591, N35E680087), and Chulalongkorn University (CE68_028_3000_004). He is also supported by the Royal Society of Thailand, has provided consultancy services, and has received honoraria and lecture fees from industries such as Britannia, Ipsen, Teva-Lundbeck, and Mitsubishi-Tanabe. Bhidayasiri holds patents for various innovations, including a laser-guided walking stick, a portable tremor device, technology for monitoring during the night (NIGHT-Recorder), an electronic diary for Parkinson's disease symptoms, as well as the Parkinson insole and shoe, and anti-choking mugs. Furthermore, his copyrighted works comprise the mobile application for screening Parkinson's disease (Check PD), ChulaPD ADL Questionnaire, and a daily activity diary for Parkinson's disease. RBS has received grant support from the NIH, Parkinson's Foundation, Michael J. Fox Foundation for Parkinson's Research, Acadia Pharmaceuticals, Bial Pharmaceuticals, and the CHDI Foundation and personal compensation for participation on Data Safety and Monitoring Boards for HEALEY ALS and AskBio. AJE has received grant support from the NIH and the Michael J Fox Foundation; personal compensation as a consultant/scientific advisory board member for Mitsubishi Tanabe Pharma America (formerly, Neuroderm), Amneal, Acorda, Abbvie, Bial, Supernus (formerly, USWorldMeds), NeuroDiagnostics, Inc (SYNAPS Dx), Intrance Medical Systems, Inc., Merz, Praxis Precision Medicines, Citrus Health, and Herantis Pharma; Data Safety Monitoring Board (chair) of AskBio; and publishing royalties from Lippincott Williams & Wilkins, Cambridge University Press, and Springer. He is co-inventor of the patent “Compositions and methods for treatment and/or prophylaxis of proteinopathies” with which he cofounded REGAIN Therapeutics to fund preclinical studies. He has no financial relationship with the company and has relinquished the right to any personal income from future treatments. Dr Espay owns no stock in any pharmaceutical company with which he has a scientific advisory relationship. He serves on the editorial boards of the Journal of Parkinson's Disease, Journal of Alzheimer's Disease, European Journal of Neurology, Movement Disorders Clinical Practice, and JAMA Neurology. Others report no disclosure.