
Abstract
Background
Digital speech analysis affords robust markers of Parkinson's disease (PD). However, most studies target late-onset PD (LOPD), neglecting early-onset PD (EOPD) –an increasingly prevalent subtype. This proof-of-concept study tackles such gap.
Methods
We used machine learning to discriminate persons with EOPD (with symptom onset before age 50) and LOPD (with symptom onset after age 50) from healthy controls (HCs) through prosodic and articulatory features from natural speech.
Results
Maximal classification between patients and HCs was afforded by combined prosodic and articulation features in LOPD (AUC = 0.90) and by articulation alone in EOPD (AUC = 0.79), with chance-level discrimination between patient groups (AUC = 0.55). Motor severity (MDS-UPDRS-III) scores predicted by these features correlated with actual motor severity scores in both LOPD (r = 0.52, p < 0.001) and EOPD (r = 0.27, p < 0.001).
Conclusions
Digital speech markers offer markers of PD irrespective of age of onset.
Plain language summary title
Voice recordings capture motor symptoms in Parkinson's disease irrespective of age of onset
Plain language summary
One of the earliest symptoms in Parkinson's disease is abnormal speech. Most people living with this disorder present a softer voice, unclear pronunciation, or reduced variation in pitch. These changes can impact communication, confidence, and everyday life. New digital tools now allow researchers to measure speech automatically and objectively, offering a simple and affordable way to monitor these problems. However, most studies have focused on people whose Parkinson's symptoms begin after age 50 (late-onset Parkinson's disease). Little is known about speech changes in people whose symptoms begin earlier in life, before age 50 (early-onset Parkinson's disease).
In this study, we recorded natural speech samples from adults with early-onset Parkinson's, late-onset Parkinson's, and healthy adults. Participants were asked to describe what they had done since waking up—an easy, conversational task similar to everyday speaking. We then used computer-based methods to measure two aspects of speech: prosody (pitch, loudness, timing) and articulation (how clearly sounds are produced). Using machine-learning techniques, we tested whether these speech features could help distinguish people with Parkinson's from healthy adults and whether they could estimate the severity of movement symptoms.
Our results showed that speech could reliably identify people with Parkinson's in both groups. For the late-onset group, disease detection was maximal when combining prosodic and articulatory features. For the early-onset group, articulation alone worked best, though accuracy was somewhat lower. Importantly, speech features also related to the severity of patients' motor symptoms in both groups.
This study suggests that simple speech recordings can provide valuable insights into Parkinson's disease regardless of the age at which symptoms begin. With further research, digital speech analysis could support earlier detection, personalized care, and improved tracking of symptoms over time.
Introduction
Speech disturbances are among the commonest and earliest signs of Parkinson's disease (PD). Typically manifesting as hypokinetic dysarthria, these alterations affect 50 to 90% of patients across cohorts,1–4 compromising communication, self-image, and functionality.5–9 Digital tools can capture such deficits objectively and cost-effectively, providing scalable insights for disease identification, phenotyping, and monitoring.10,11 However, most studies target late-onset PD (LOPD), overlooking the nature of dysarthric patterns in early-onset PD (EOPD), an increasingly prevalent form of the disease.1,11–14 This proof-of-concept study tackles such a gap.
Following Movement Disorder Society criteria, EOPD cases are those whose motor symptoms onset before age 50,15–18 thus disrupting patients’ lives at a productive stage. 19 EOPD differs from LOPD in several aspects. For example, it involves longer disease duration, slower motor symptom progression, and greater postural and cognitive preservation, alongside motor fluctuations, behavioral issues, worse gait features, and higher functional disability.20–23 Conversely, core dysarthric features seem present in both groups. This is true of prosodic disturbances (e.g., monopitch, monoloudness) and articulatory decay, 1 though specific alterations (e.g., consonant mis-articulation) may be more significant in LOPD.11,24 Also, some such features predict motor symptom severity in both populations, attesting to their potential for patient monitoring and phenotyping across disease subtypes. 1
Articulatory and prosodic anomalies, then, would represent scalable PD features irrespective of age of onset. 1 Yet, evidence for this claim is very limited and it lacks subject-level robustness tests. Moreover, digital speech assessments comparing EOPD and LOPD are circumscribed to Czech, 1 calling for replications in phonetically different languages.25–27
These gaps can be tackled by combining digital speech tools with machine learning, an automated, cost-effective approach for detecting and monitoring different forms of PD. 28 In particular, recent works have validated digital measures of prosody (including speech timing and pitch-related features) and articulation (energy content during transitions between voiced and unvoiced segments).28,29 Their joint use on LOPD and EOPD enables fine-grained phenotypic comparisons, potentially revealing endpoints for interventions and trials involving both subtypes.
Here, we recruited carefully characterized persons with EOPD and LOPD and healthy controls (HCs), asked them to describe their routine, and automatically extracted prosodic and articulatory features from their recordings. We used machine learning to examine whether these features could identify patients in each group and predict their overall motor symptom severity, as captured via the Movement Disorders Society's Unified Parkinson's Disease Rating Scale part III (MDS-UPDRS-III) scale. 30 We hypothesized that prosodic and articulatory features would enable the detection of both PD subtypes, with more robustness for LOPD than EOPD. Also, we anticipated that these features would predict motor symptom severity in both groups.
Methods
Participants
The study included 63 participants: 20 with LOPD, with symptom onset after age 50; 23 with EOPD, with symptom onset before age 50; and 20 HCs. All participants were recruited from the Movement Disorders Outpatient Clinic of the Neurology Service at the University Hospital in Porto Alegre, Brazil, between June 2021 and June 2022. To be included in the study, participants had to be native Portuguese speakers, possess normal or corrected-to-normal vision and hearing, be capable of consenting. Additionally, patients needed to possess an idiopathic PD diagnosis based on clinical UK Parkinson's Disease Society Brain Bank diagnostic criteria for PD (AFS),31,32 be under regular neurological follow-up (with no acute events), demonstrate clinical stability at the time of assessment, and confirm capacity to understand and perform the study's speech tasks. Exclusion criteria included a history of previous neurological events (such as stroke, traumatic brain injury, or neurodegenerative diseases other than PD), systemic, sensory or motor disorders, structural abnormalities affecting voice and speech, or severe uncompensated hearing loss; evidence of atypical or secondary parkinsonism; and a diagnosis of dementia or severe cognitive impairment. The age of onset cutoff for EOPD and LOPD was derived from Mehanna et al. (2022). 16 Clinical and sociodemographic data (sex, age, education, time of disease, age of onset, Hoehn and Yahr Disability Stage Scale, Levodopa equivalente daily dose (LEDD), and MDS-UPDPRS-III score) were collected from electronic medical records. HCs had no history of neurological or psychiatric disorders, nor self-reported or clinically identified speech or language impairments. Patients were assessed in the ON medication state (i.e., between 45 and 150 min after the last regular Levodopa intake). LEDD values were calculated using standardized conversion factors. 33
Standard dysarthria assessments were based on perceptual-auditory analysis. 34 Two speech-language pathologists independently listened to deidentified, group-agnostic speech samples from each patient, including sustained vowel production, syllable repetition, sentence repetition, and spontaneous speech. Each audio was rated on six dimensions (overall dysarthria severity as well as respiration, resonance, phonation, prosody, and articulation), each via a four-point scale (0 = normal, 1 = mildly impaired, 2 = moderately impaired, 3 = severely impaired). Additional ratings were gleaned from item 3.1 of the MDS-UPDRS-III, providing a single score based on an integrated perceptual assessment of intelligibility, articulatory precision, vocal intensity, and prosody. Scores range from 0 (normal) to 4 (severe impairment), reflecting the degree of dysarthria. The few cases of discrepancy between raters were settled by a third speech-language pathologist. Results revealed comparable perceptual dysarthria ratings between EOPD and LOPD participants (Table 1).
Participants’ demographic and clinical data.

Data presented as mean (SD), with the exception of sex. (a) p-values calculated via chi-squared test. (b) p-values calculated via independent measures ANOVA among LOPD, EOPD, and Healthy Controls. (c) p-values calculated via independent measures ANOVA between LOPD and EOPD. LOPD: late-onset Parkinson's disease; EOPD: early-onset Parkinson's disease; MDS-UPDRS-III: Unified Parkinson's Disease Rating Scale, part III; LEDD: Levodopa equivalent daily dose.
All groups were matched for sex, age, and years of education. Specifically, the LOPD patients were automatically selected via a stratified random selection, capped at +/- 3 participants relative to the EOPD group, followed by statistical verification of group comparability via Chi-squared tests for categorical variables and either Student's t-tests or Mann–Whitney U tests for continuous variables, depending on normality assessed via the Shapiro–Wilk test. A minimum significance level of 0.1 was considered to ensure no relevant differences between groups. Although not entered as a constraint in automated participant selection pipeline, MDS-UPDRS part III scores were incidentally matched between both patient groups –which allows tackling age of onset as a focal independent variable while circumvent age- and progression-related confounds. Both patient groups were also matched for dyskinesia status, established as positive if a patient (i) used amantadine and (ii) exhibited dyskinesia based on UK Parkinson's Disease Society Brain Bank diagnostic criteria or had a score above 0 on items 4.1 or 4.2 of the MDS-UPDRS-IV scales (tapping frequency and functional impact of dyskinesia, respectively). For details, see Table 1.
Speech elicitation
Participants were tested in a silent room. As in previous works,27,35,36 they were asked to respond to the following prompt: “What have you done today since you woke up?”, speaking at their normal pace and volume. 37 This is a validated, non-invasive, education-independent task,27,35,36 reflecting real-life communicative skills and enabling comparisons across populations beyond the limitations of more artificial tasks (e.g., syllable repetition). Recordings were obtained with a TASCAM DR-07X system and a KARSECT HT-9 microphone placed roughly 5 cm away from the participant's mouth. The recordings were sampled at 44.1 kHz and quantified at 16 bits.
Audio preprocessing
As in previous research, 28 speech signals were resampled to 16 kHz and amplitude-normalized to 0 dB (retaining gain levels) to address energy bias due to mouth-to-microphone distance variability. Microphone biases were eliminated via mean cepstral normalization. 38 Sections with examiner's voice were manually removed before preprocessing.
Feature extraction
Prosodic and articulatory features were extracted from each recording. As in previous works,28,39 to best characterize each dimension while avoiding speech-duration biases, we computed each feature's mean, standard deviation, kurtosis, and skewness.
Prosody
Speech prosody analysis includes pitch, loudness, and duration parameters.28,40 Pitch and loudness features are derived from fundamental frequency and sound pressure level contours computed from 40-ms time frames and 10-ms time shifts. 41 Duration-based features include the (a) duration, (b) ratio, and (c) number of speech segments, voiced segments, unvoiced segments, and pause segments. Speech and pauses are automatically detected using an energy-based voice activity detection algorithm. 38 Voiced sounds are extracted by selecting the speech frames with F0 ≠ 0, whereas unvoiced segments are derived by determining the signal segments not labeled as voiced or pause segments. 41
Articulation
Articulatory movements are modeled by measuring the energy content of transitions from unvoiced-to-voiced sounds (onset) and voiced-to-unvoiced sounds (offset). 29 Transitions are extracted by detecting voiced segments. Speech segments of 80 ms duration are taken to the left and right of the border between the voiced and unvoiced sounds, forming speech segments of 160 ms. Filterbank analysis is applied to the transitions to compute Mel/Gammatone Frequency Ceptrals Coefficients, which contain information about energy changes (in different frequency bands) when moving from one sound to another.28,29
Fusion
Feature vectors with prosody and articulation measures were concatenated to create a fusion vector representation. Concatenation was based on an early fusion approach, involving joint analysis of individual prosodic and articulation features –rather than the integration of outputs from the respective unidimensional classifiers. No weighting procedure to any of the features is applied to assign the same importance to all measures.39,42
Data analysis
The above features were used to classify between (1) LOPD patients and HCs, (2) EOPD patients and HCs, and (3) LOPD and EOPD patients. Such analyses employed a support vector machine with a linear kernel, a robust, generalizable, interpretable method. 43 Also, we tested whether speech features predicted patients’ motor symptoms severity as captured via MDS-UPDRS-III scores, upon removing outliers at 3 SDs from each group's mean.
We first used ElasticNet regressions (which combine the penalties of ridge and lasso regressions) 44 to predict MDS-UPDRS-III scores. Then, we ran Spearman's correlations between predicted and actual MDS-UPDRS-III values. For classifications and regressions, hyperparameters were optimized via a nested five-fold cross-validation strategy, with three folds used internally for optimization based on training set outcomes. For cross-validation, the training and testing sets were randomly generated ten times for model generalization, ensuring that the subjects’ samples were not mixed between the training and testing sets. Finally, we tested whether results were influenced by years since diagnosis as a proxy of treatment duration. To this end, we first examined whether classification between EOPD and LOPD changed significantly upon adding years since diagnosis as an additional feature, and whether the top five features in each EOPD-LOPD classifier correlated with such a variable. Second, we explored whether correlations between speech-predicted and actual MDS-UPDRS-III scores across those two groups were altered upon including years since diagnosis as a covariate.
All classification and regression analyses were run with (i) prosodic features alone, (ii) articulatory features alone, and (iii) the fusion representation. Correlations between predicted and actual values were corrected via the False Discovery Rate (FDR) method, based on the Benjamini-Yekutieli (BY) procedure, with a significance threshold of p < 0.05. 45
Results
Classifying LOPD patients and HCs
Prosodic and articulatory features, on their own, achieved AUCs of 0.84 and 0.89, respectively (Figures 1A–B), with higher specificity for prosodic features and a more balanced classification of each group for articulation. The fusion scheme achieved the maximal classification (AUC of 0.90), with good balance between sensitivity and specificity (Figure 1C).
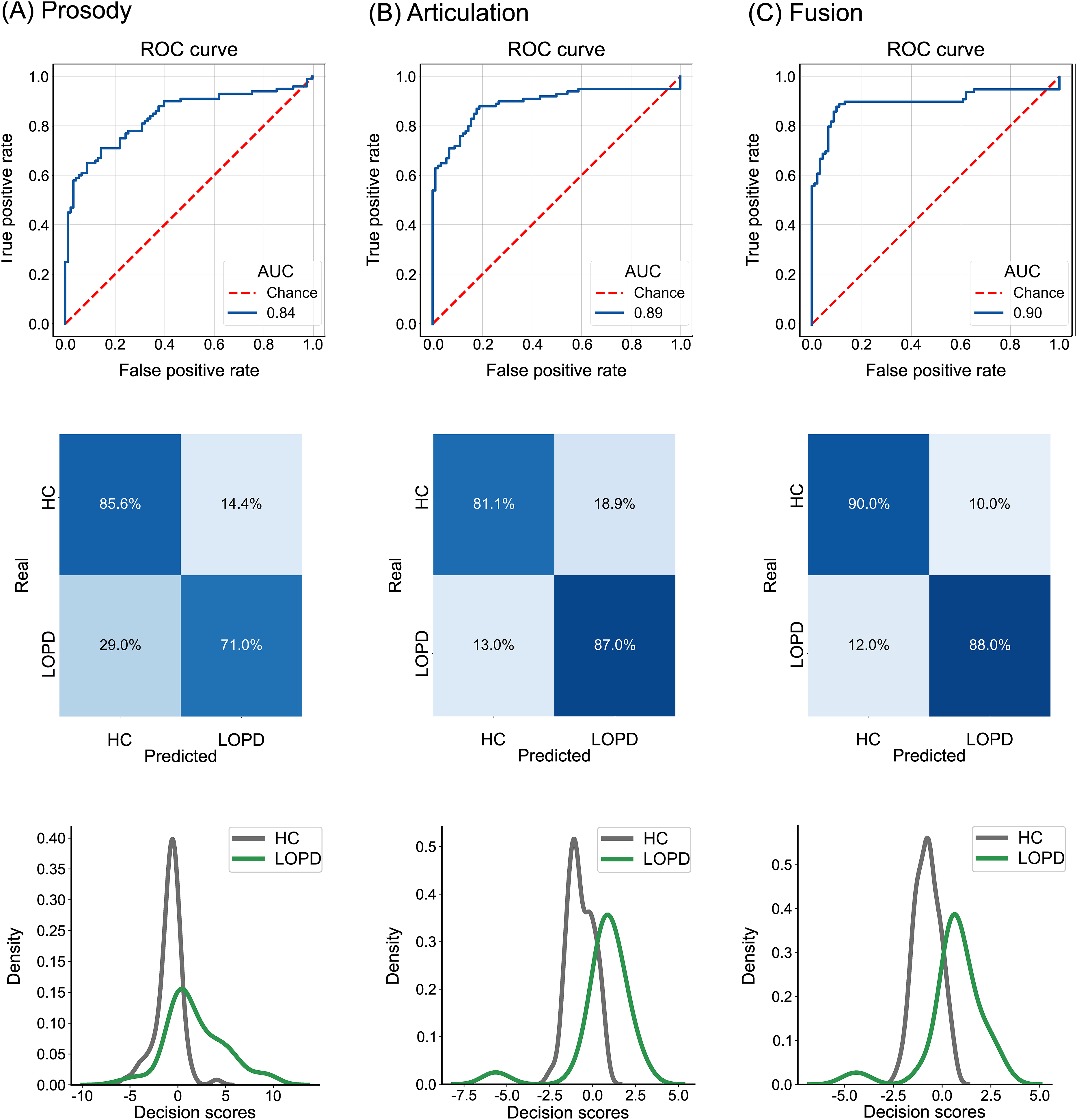
Classification between persons with late-onset Parkinson's disease (LOPD) and healthy controls (HCs). Panels show the best classifiers using (
Classifying EOPD patients and HCs
Classification between EOPD patients and HCs reached an AUC of .73 based on prosody (Figure 2A) and an AUC of .79 based on articulation, with a good balance between sensitivity and specificity (Figure 2B). Similar outcomes were obtained with the fusion scheme, although with a poorer balance (Figure 2C).
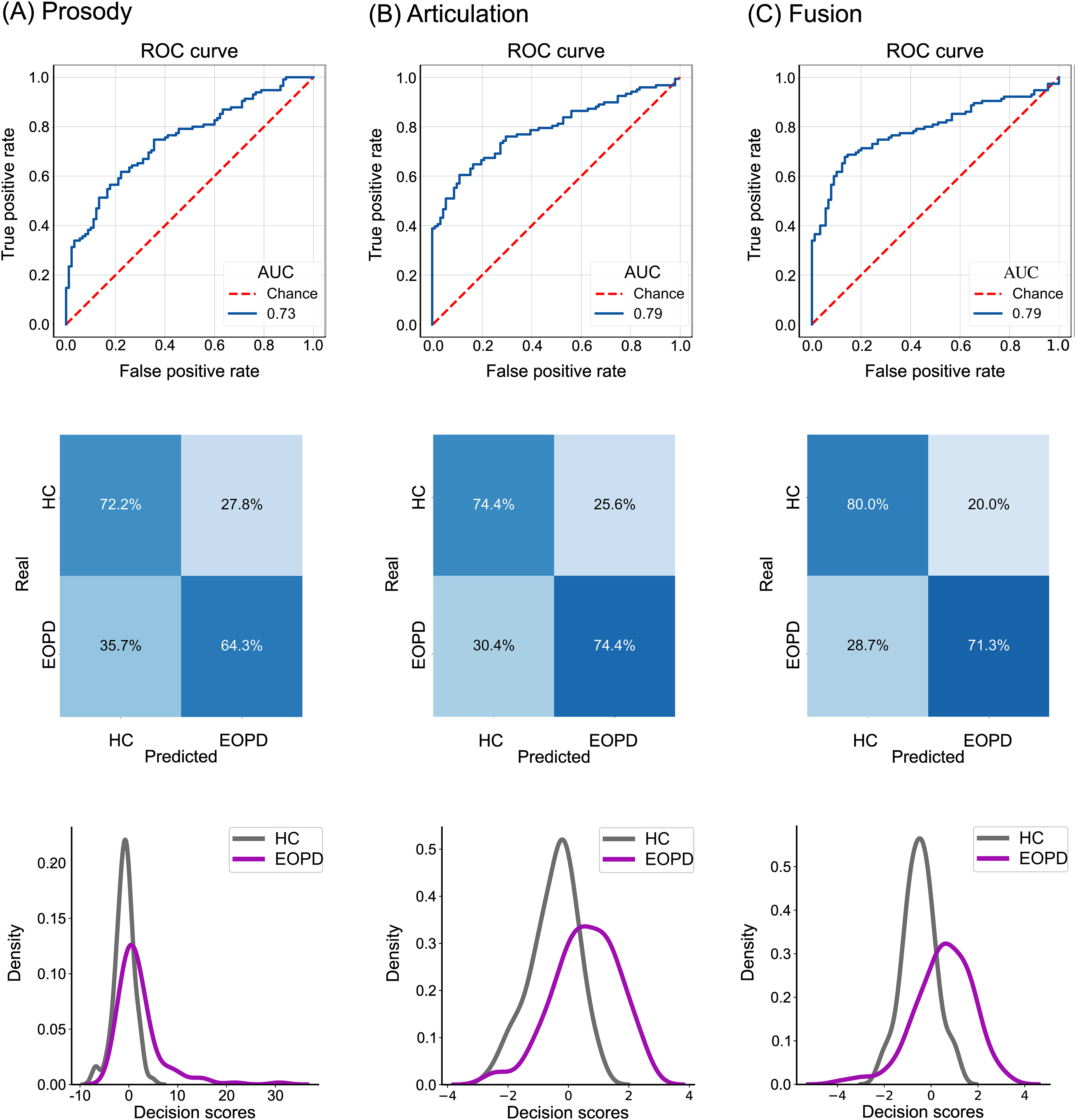
Classification between persons with early-onset Parkinson's disease (EOPD) and healthy controls (HCs). Panels show the best classifiers using (
Classifying LOPD and EOPD patients
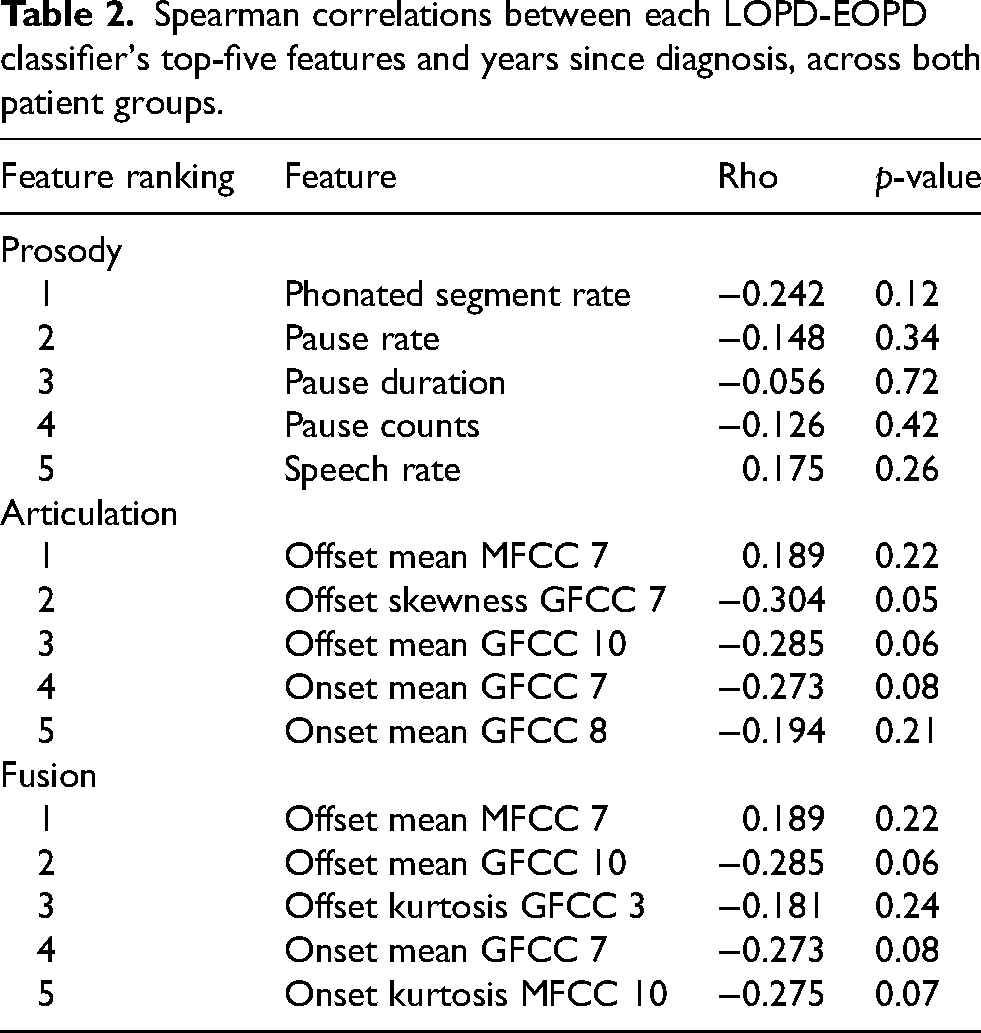
Classification between both forms of PD (Figure 3) was near chance when based on prosody (AUC = .0.55), articulation (AUC = .51), and fusion (AUC = .51). These results did not differ significantly from those obtained upon adding years since diagnosis as an additional feature in each classifier (prosody: AUC = .67, U = 23800, p = .59, RBC = −0.030; articulation: AUC = .52, U = 21842, p = .32, RBC = 0.055; fusion: AUC = .48, U = 20868, p = .08, RBC = 0.097). Moreover, upon collapsing both patient groups, correlations between each classifier's top-five features and years since diagnosis were not significant (Table 2).
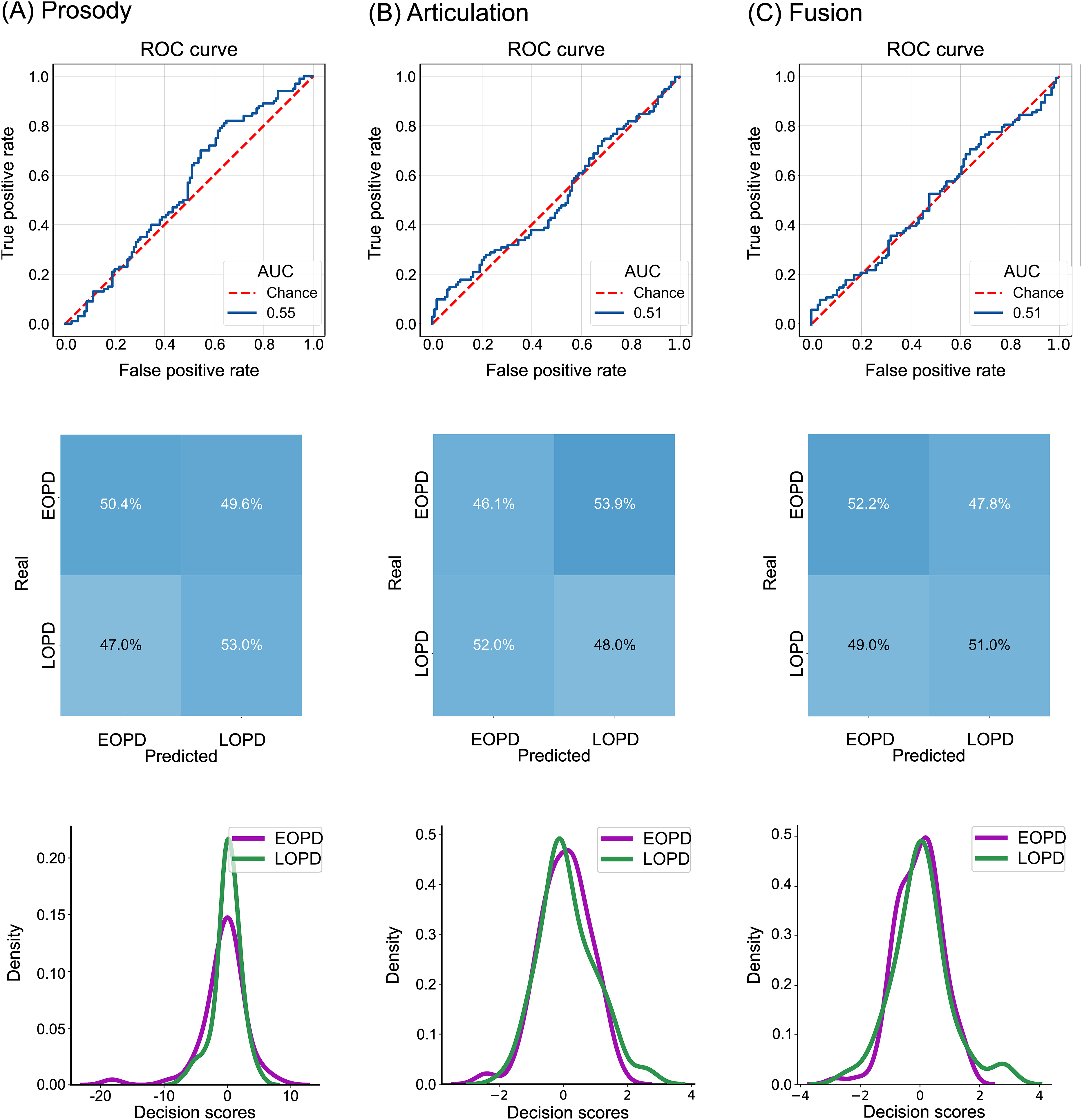
Classification between persons with late- and early-onset Parkinson's disease (LOPD, EOPD). Panels show the best classifiers using (A) prosodic features, (B) articulatory feature, and (C) their early fusion. AUC: area under the ROC curve.
Spearman correlations between each LOPD-EOPD classifier's top-five features and years since diagnosis, across both patient groups.
Predicting motor symptom severity
Significant correlations were observed between patients’ MDS-UPDRS-III scores and those predicted by speech features (Figure 4). In the LOPD group, these emerged through the articulation (p < 0.001, r = 0.35) and the fusion (p < 0.001, r = .53) model. The same models yielded significant correlations in the EOPD group (articulation: p < 0.001, r = 0.29; fusion: p < 0.001, r = 0.23). Results remained nearly identical upon covarying for years since diagnosis, both for the LOPD group (articulation: p < 0.001, r = 0.40; fusion: p < 0.001, r = .54) and the EOPD group (articulation: p < 0.001, r = 0.33; fusion: p < 0.001, r = 0.25).
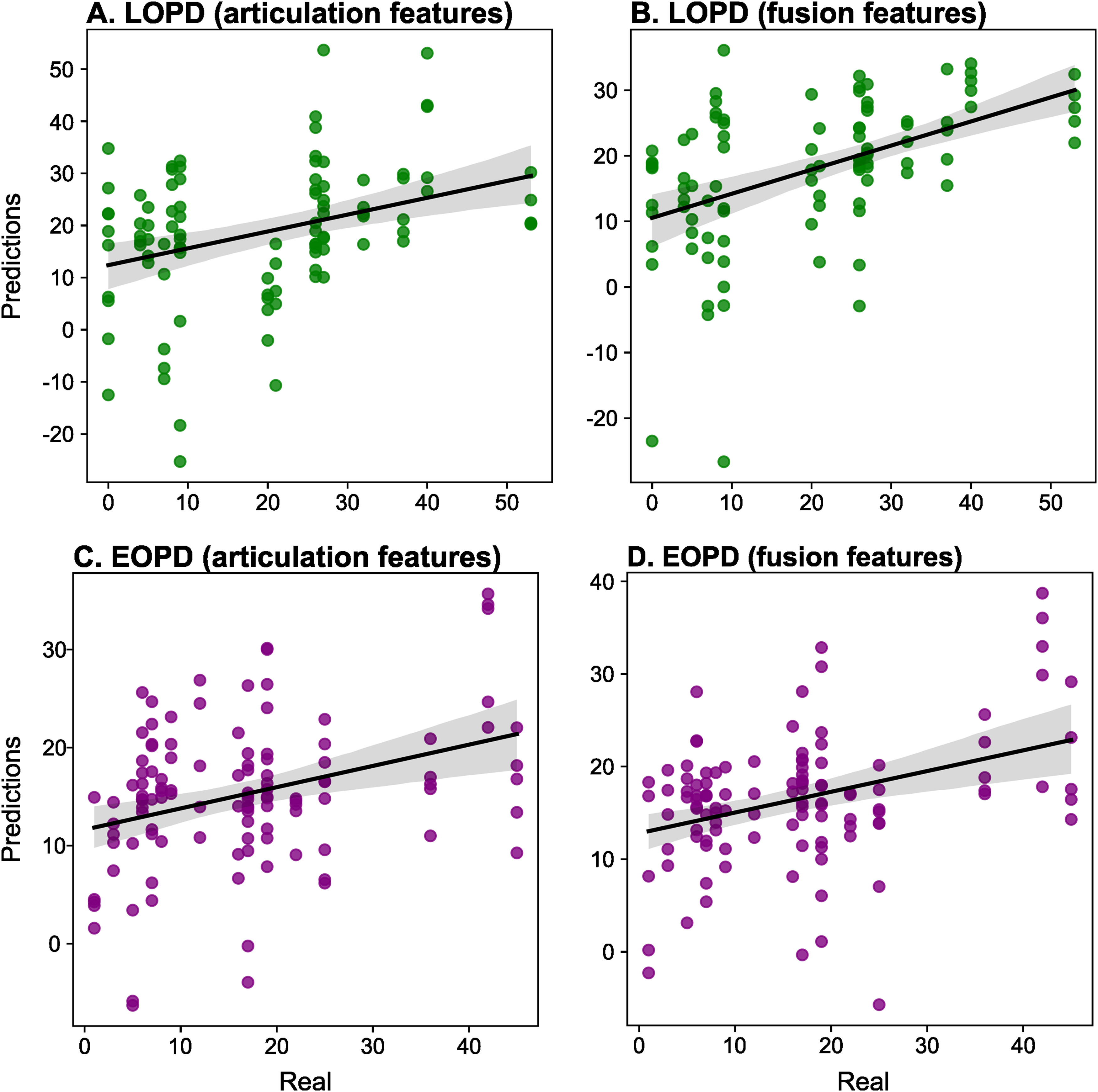
Correlations between real and predicted MDS-UPDRS-III scores, corrected for multiple comparisons, in (
Discussion
This proof-of-concept study used digital prosodic and articulatory measures to identify persons with LOPD and EOPD and predict motor symptom severity. Robust results were obtained in both populations, driven by the combination of both features in LOPD and by articulatory measures in EOPD. Below we discuss these findings.
LOPD patients were discriminated from HCs by both prosodic and articulatory features, especially when combined. Our findings align with those of Rusz et al., 1 who found specific prosodic (monopitch) and articulatory (consonant articulation) deficiencies in LOPD. Extending such results, our multi-feature approach shows that robust patient identification can be attained through integrative measures of each dimension. Indeed, the same approach identified LOPD patients upon combining prosodic and articulatory features (alongside phonemic features), underscoring the relevance of multivariate analyses for disease detection. 28 Also, while Rusz et al.'s results stemmed from group-level comparisons, our machine-learning framework attests to these markers’ subject-level consistency, as required in precision medicine settings.31,32,46
Both dimensions were also sensitive to EOPD, with best results for articulatory features. Articulatory decay had been previously reported in the only digital speech assessment of EOPD, 1 reinforcing its role as an age-of-onset-independent marker of PD. Indeed, such speech articulation impairments do not correlate with age at onset, whether using perceptual or acoustic evaluation, 47 and they have been perceptually described as altered in both LOPD and EOPD.2,34,48 Yet, note that, in our study, classification scores for EOPD were roughly 10 points lower than those of LOPD. This suggests that prosodic and articulatory alterations may not be as systematic in early-onset cases as implied in previous works.49,50
Predictions of motor symptoms also yielded partly differential patterns. MDS-UPDRS-III scores were best predicted by combined prosodic and articulatory features in LOPD and by articulatory features in EOPD. Rusz et al. 1 showed that specific articulatory deficits correlated with postural instability/gait difficulty, but no attempt was made to examine correlations for LOPD and EOPD separately. Our study is the first to indicate that motor symptom severity may be best captured by different speech dimensions in each group, informing personalized monitoring protocols. However, this possibility requires more systematic testing.
The above results bear clinical implications. First, relative to LOPD, EOPD involves a higher prevalence of rigidity as the initial symptom, 51 more frequent familial antecedents, 52 and slower motor symptom progression. 53 Our findings suggest that phenotypic differences between both disease variants are also present in their dysarthric profiles, highlighting the need for tailored assessments in each case. Second, current findings underscore the potential of automated measures, especially considering that perceptual dysarthria ratings may overlook differentiations between LOPD and EOPD. 1 Third, our results are the first to show that digital speech measures can contribute to patient identification in a Portuguese-speaking cohort. This meets the call for testing the cross-cultural generalizability of speech markers in PD, a challenge emphasized in recent literature.25,27,43 Finally, multivariate prosody and articulation measures emerge as candidate as endpoints for clinical trials in both LOPD and EOPD.54,55
Although replicable results have been reported with comparable Ns, 1 our study had a limited sample size, mainly driven by the low prevalence of EOPD and the need to balance this group with the others. Of note, we attenuated this limitation by performing nested cross-validation with five folds in the external loop and four folds in the internal one, maximizing the extraction of information from the modeled phenomenon and enabling ulterior tests on external corpora. Future works should test whether our results are replicated over larger cohorts. Second, our goal to circumvent both age- and severity-related confounds led to the recruitment of EOPD patients with mild symptomatology after several years since diagnosis. This sample was thus typified by slow progression calling for replications of our study in EOPD cohorts with more advanced symptomatology. Third, the impact of medication merits deeper investigation. Both patient groups were matched for dyskinesia status (which is typically influenced by levodopa) and results were largely uninfluenced by years since diagnosis (itself a proxy of years under medication). Still, adherence data were unavailable and the sample size was moderate, inviting new studies on how pharmacological factors modulate speech patterns in LOPD and EOPD. Fourth, while our results extend Rusz et al.'s findings on Czech 1 to a typologically different language, further cross-linguistic testing is required to evaluate the generalizability of the proposed markers. Finally, applying our approach in longitudinal designs would be vital to assess its sensitivity to disease progression in both LOPD and EOPD.
Overall, digital speech metrics seem to afford scalable markers of both LOPD and EOPD. These disease subtypes would present with partly shared dysarthric phenotypes, enabling both disease detection and severity prediction. Further work along these lines can inform precision medicine approaches across PD phenotypes.
Footnotes
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional ethics committee under number 2019-0789.
Consent to participate
All participants provided written informed consent.
Consent for publication
All participants consented to their data being published in fully anonymized fashion.
Author contributions
MRO: Conception, organization, execution, statistical analysis, writing of the first draft, review, and critique. DE-G: statistical analysis, design, execution, figure design, writing of the first draft, review, and critique. TA-V: statistical analysis, data curation, figure design. VBS: execution, data collection, data curation, writing of the first draft, review, and critique. ALB: execution, data collection, data curation. IM: review and critique. JRO-A: conception, statistical design, statistical analysis, figure design, review and critique. AMG: conception, organization, statistical design, figure design, writing of the first draft, review and critique.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Adolfo M García is an Atlantic Fellow at the Global Brain Health Institute (GBHI) and is partially supported by the National Institute On Aging of the National Institutes of Health (R01AG075775, 2P01AG019724); Agencia Nacional de Investigación y Desarrollo (FONDECYT Regular 1250317, 1250091); Agencia Nacional de Promoción Científica y Tecnológica (01-PICTE-2022-05-00103); and the Multi-partner Consortium to Expand Dementia Research in Latin America (ReDLat), which is supported by the Fogarty International Center and the National Institutes of Health, the National Institute on Aging (R01AG057234, R01AG075775, R01AG21051, and CARDS-NIH), Alzheimer's Association (SG-20-725707), Rainwater Charitable Foundation's Tau Consortium, the Bluefield Project to Cure Frontotemporal Dementia, and the Global Brain Health Institute. Ignacio Mata. receives funding from the National Institutes of Health (NIH) 1R01NS112499-01A1, The Michael J. Fox Foundation, and the Aligning Science Across Parkinson's initiative. The study was also partly funded by CODI (UdeA) through grant # PI2023-58010; the Brazilian government, through the doctor scholarship kindly awarded to Vanessa Brzoskowski dos Santos by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES); and Fundo de Incentivo à Pesquisa e Eventos (FIPE) of Hospital de Clínicas de Porto Alegre (HCPA), under number 2019-0789. The contents of this publication are solely the authors’ responsibility and do not represent the official views of these institutions.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data availability
Maira Rozenfeld Olchik, Daniel Escobar-Grisales, Juan Rafael Orozco-Arroyave, and Adolfo M. García take responsibility for data integrity and analytical accuracy.