
Abstract
The glymphatic system, a macroscopic waste clearance network in the brain, plays a vital role in maintaining neuronal health and brain homeostasis. Functionally analogous to the lymphatic system in other organs, the term “glymphatic” combines “glial” and “lymphatic.” This system facilitates the exchange of cerebrospinal fluid (CSF) and interstitial fluid (ISF) in the parenchyma, aiding in the removal of soluble proteins and metabolites while distributing essential nutrients and signaling molecules. Its functionality is closely tied to aquaporin 4 (AQP4) water channels, located primarily on astrocytic endfeet, which mediate water movement between the CSF and ISF. Proper glymphatic function relies on the cellular distribution of AQP4 channels and its astroglial endfeet polarization. Emerging evidence links glymphatic dysfunction to several neurodegenerative disorders, including Huntington's disease (HD). Understanding the role of the glymphatic system in HD pathogenesis could provide novel insights into disease pathogenesis and new therapeutic approaches. This review examines the connection between glymphatic dysfunction and HD, highlighting future research directions and therapeutic advancement for HD. It explores pharmacological interventions and lifestyle modifications aimed at optimizing glymphatic function to improve HD management.
Keywords
Introduction
Huntington's disease (HD) is a neurodegenerative disorder caused by an expanded CAG repeat in the huntingtin (HTT) gene, leading to the production of mutant huntingtin protein (mHTT). This aberrant protein accumulates within neurons and other cell types, contributing to neuroinflammation and progressive neurodegeneration. Despite advances in understanding HD pathogenesis, no approved treatments specifically target the mHTT gene or its aggregates. However, given the monogenic nature of HD, therapeutic strategies aimed at lowering HTT expression or enhancing mHTT clearance hold promise for alleviating disease progression. 1
While intracellular mechanisms such as the ubiquitin-proteasome system (UPS) and autophagy have been extensively studied for mHTT elimination, the glymphatic system may offer an alternative extracellular pathway for mHTT clearance. The glymphatic system, functionally mediated by the perivascular space and astrocytic aquaporin-4 (AQP4) polarization, facilitates the removal of metabolic waste from the brain via cerebrospinal fluid (CSF) and interstitial fluid (ISF) 2 exchange. Notably, mHTT has been detected in the CSF even before overt neurodegeneration in HD, 3 implicating that its clearance involves both passive release and active transport via the glymphatic system. In addition, our recent findings on impaired glymphatic function and reduced AQP4 polarization in HD mouse and patient brains indicate a potential role for glymphatic dysfunction in HD pathogenesis. 4
This review focuses on the implications of glymphatic dysfunction in HD, including current available neuroimaging techniques to assess glymphatic function, discussing pharmacological strategies to enhance glymphatic transport and modulate meningeal lymphatic vessels. Additionally, lifestyle modifications to optimize glymphatic activity are discussed, alongside future research directions aimed at leveraging this system for innovative HD therapies.
Glymphatic system: Anatomic compartments and biological function
Efficient clearance of metabolic waste and fluid homeostasis are critical for maintaining brain function. Historically, the central nervous system (CNS) was thought to lack a lymphatic system, leaving questions on how the brain manages protein clearance and immune responses. While CSF was known to play a critical role in metabolite exchange, the mechanisms underlying this process remained elusive. In 2012, Iliff et al. identified the glymphatic system, a brain-wide waste clearance system located in the perivascular space (PVS) and dependent on perivascular localized aquaporin-4 (AQP4) water channels. 2
The glymphatic system is an astroglial-dependent fluid exchange and drainage system comprising the PVS surrounding arteries, arterioles, capillaries, venules, and veins within the brain parenchyma. The PVS is structed as a coaxial system, within the inner cylinder formed by the vascular wall and the outer cylinder formed by glial limitans, which encase penetrating arterioles or perivascular astrocytic endfeet around capillaries. This system primarily includes three components: periarterial CSF inflow channels, astrocyte-mediated convective fluid transport supported by AQP4-polarized endfeet, and perivenous ISF outflow channels.
CSF enters the brain parenchyma via the PVS of penetrating arteries, often referred to as Virchow–Robin spaces5,6 and exchanges with ISF through glial basement membranes and astrocytic endfeet. Metabolic wastes and solutes from the interstitial space are directed into perivenous spaces and subsequently drain into meningeal lymphatic vessels (MLVs) and the perineural sheaths of cranial and spinal nerves for removal from the CNS.
The biological function of the glymphatic system is to clear metabolic waste products and toxins, thereby supporting brain health and function. This clearance is especially active during sleep, 7 when an increase in interstitial space allows more efficient waste removal. Arterial pulsations driven by the cardiac cycle are believed to provide the driving force for glymphatic convective flow,8,9 while AQP4 polarization on astrocytic endfeet facilitates CSF-ISF circulation and exchange. Emerging evidence links glymphatic dysfunction to aging, neurodegeneration, and tramatic brain injury in rodent brains, and similar glymphatic activity has been confirmed in humans through MRI studies recently.10,11
In parallel, the MLVs are functionally linked to glymphatic system and have been shown to contribute to solute transport and immune surveillance.12–15 The regulation of glymphatic flow is influenced by factors such as arterial pulsations, body position, respiratory cycles, and levels of consciousness.7,16–19 Despite these insights, the precise mechanisms driving glymphatic fluid flow remain to be determined, warranting further investigation to fully elucidate this critical waste clearance system.
CNS lymphatic system: A pathway for solute exit from glymphatic flow
While the glymphatic system facilitates the drainage of ISF into CSF, the mechanisms by which solutes exit the CNS into the periphery were unclear until 2015. Two landmark studies (re)discovered lymphatic vessels within the dura mater of the meninges, identifying their role in draining CSF and macromolecules from the CNS to peripheral lymph nodes.12,13 Over the past decade, research has shown that MLVs are key components of glymphatic fluid drainage,12,14,15,20–23 though the exact routes and contributions of this system remain a topic of debate.
Rodent studies have demonstrated that the olfactory nerve's perineural sheaths, passing through the cribriform plate to cervical lymphatic vessels, serve as primary egress pathways for brain parenchyma solutes and waste. 24 Whether humans share similar routes remains uncertain. Louveau et al. (2015) provided critical insights by using fluorescent tracers in rodent brains, showing tracer transport along MLVs to deep cervical lymph nodes (dCLNs). Surgical ligation of cervical lymphatic vessels increased tracer accumulation in MLVs, affirming their role in CSF drainage. 13 These findings have since been corroborated by MRI and radiolabeled tracer studies in humans and non-human primates, highlighting MLVs as major efflux pathways for CSF/ISF.25–27
Despite this progress, the proportional roles of various glymphatic drainage routes, including meningeal lymphatics, the cribriform plate, and the rostral migratory stream, remain undefined. High-resolution imaging techniques, such as light-sheet fluorescence microscopy and advanced MRI, have provided whole-head imaging of MLVs in both humans and rodents, offering further evidence for a functional CNS lymphatic network.28–30
Although there is no direct anatomical link between the glymphatic system and MLVs, these systems interact functionally to form a waste clearance network. Together, they create a CSF drainage pathway: CSF → ISF → CSF → MLVs → dCLNs. 31 Additionally, traditional pathways, such as arachnoid granulations, and newer discoveries, like the nasopharyngeal lymphatic plexus (NPLP), also contribute to CSF outflow.32,33 The NPLP drains CSF through lymphatic vessels near the pituitary gland and cavernous sinus, connecting upstream lymphatic structures to dCLNs.
Additionally, the arachnoid cuff exit (ACE) points, formed by discontinuities as the bridging veins traverse the arachnoid barrier, create openings that permit the exchange of CSF and molecules between the subarachnoid space (SAS) and the dura mater, facilitating CSF drainage. 34 Recently, the NPLP has been demonstrated to serve as a major hub for the outflow of CSF to the dCLNs. 35 Research indicates that the NPLP is connected with upstream lymphatic vessels, including those near the pituitary gland and the cavernous sinus, as well as through the cribriform plate, where CSF is drained to the dCLNs via the deep cervical lymphatic vessels. These CSF drainage structures collaborate with the glymphatic system and the meningeal lymphatic system to jointly sustain the balance of cerebral fluids and the clearance of metabolic waste.
The advancements in the past decades in understanding the glymphatic-meningeal lymphatic-cervical lymphatic pathway have revolutionized our knowledge of CNS waste clearance, its implications in neurological disorders, and its potential as a therapeutic target. By elucidating these mechanisms, we move closer to developing strategies to modulate this system for treating neurodegenerative and cerebrovascular diseases.
Methods to assess glymphatic function
MRI-based techniques have emerged as valuable tools for evaluate the function and dysfunction of glymphatic system in both human and animal models.36,37 These methods allow for the quantification of glymphatic clearance efficiency, offering insights into its function under healthy and pathological conditions. Early detection of glymphatic dysfunction can facilitate timely intervention, potentially slowing disease progression. However, measuring fluid dynamics in the brain remains technically challenging due to many factors, including (but not limited to) circadian rhythms 38 and anesthetic agents influence. Detailed reviews of currently used imaging methods/techniques to evaluate glymphatic function have been summarized in the previous reviewer articles.36,37,39,40 This section only briefly outlines several key in vivo imaging techniques with a focus on both experimental and clinically relevant approaches.
Two photon imaging
Two-photon microscopy is the first tool to evaluate the glymphatic pathway in rodents, suggesting that amyloid-β (Aβ) is cleared via this pathway. 2 Recent advancements in fluorescence microscopy have enabled minimally invasive and high-resolution imaging. For example, Sweeney et al. introduced transcranial fluorescence macroscopic imaging to track CSF transport in live mice without the need for invasive procedures. 41 However, limitations such as shallow penetration depth, invasiveness, and a narrow field of view restrict the applicability of two-photon imaging to human studies. 42
Diffusion tensor imaging (DTI)
DTI analysis along the perivascular space (DTI-ALPS) is proposed to assess glymphatic activity by measuring water diffusion within the perivascular spaces.43–45 A reduction in diffusivity may indicate glymphatic dysfunction. Intravoxel incoherent motion diffusion-weighted imaging (IVIM-DWI) has extended this approach, enabling the measurement of both Brownian motion and microvascular perfusion. This noninvasive technique offers insights into fluid dynamics around enlarged perivascular spaces and white matter hyperintensities, providing a promising avenue for clinical applications. 46 The DTI ALPS method is straightforward since the analysis method can be performed on standard DTI data or already collected DTI data. But APLS has been criticized based on the fact that contributions of the perivascular space in white matter should be small to negligible based on knowledge from histology.
Dynamic contrast-enhanced MRI (DCE-MRI)
DCE-MRI enables in vivo visualization of glymphatic function, often using gadolinium-based contrast agents (GBCA).47,48 While traditionally administered intrathecally, recent studies suggest intravenous administration may also effectively visualize glymphatic pathways, even in the presence of an intact blood-brain barrier (BBB).49,50 Gadobutrol, a macrocyclic contrast agent, has shown promise in enhancing dural lymphatic vessels and visualizing downstream glymphatic drainage. This approach represents a step forward in noninvasive imaging of the human glymphatic system. 28 However, caveats should be noted when using GBCA-based methods to investigate the glymphatic system. Hyperintensities or high post-GBCA signal changes do not always correspond to higher GBCA concentration because it depends on the pulse sequence and imaging parameters applied. 51 In addition, substantial partial volume effects from the blood compartment should be considered when interpreting the GBCA-induced signal changes in the brain. Moreover, intrathecal administration of the GBCA contrast can provide a direct assessment of CSF circulation in the brain. Nevertheless, the intrathecal procedure is more invasive and is not FDA-approved for human use.
Dynamic glucose-enhanced MRI (DGE-MRI)
DGE-MRI uses natural D-glucose and Chemical Exchange Saturation Transfer (CEST) imaging to assess glucose transport, tissue metabolism, and CSF clearance. By selectively labeling the hydroxyl protons in glucose, this method amplifies low-concentration signals, enabling precise detection of glymphatic flow. 52 Using a novel DGE-MRI technique, employing on-resonance variable delay multiple pulse (onVDMP) sequences,53–55 we found impaired glymphatic clearance in pre-symptomatic zQ175 HD mouse models. 4 This noninvasive method offers potential for early diagnosis and monitoring of glymphatic function in HD. The DGE-MRI method may have potential when assessing the glymphatic system in humans. However, further work is warranted, especially when moving towards patient studies. The small effect size should be addressed together with the confounding effects that appear due to motion.
These techniques highlight significant advancements in assessing the glymphatic system, with applications ranging from experimental studies to clinical diagnostics. With further validation and optimization, these non-invasive neuroimaging measures could pave the way for improved understanding and potentially new treatment of HD.
Role of glymphatic clearance in HD pathogenesis
The deposition of mHTT protein aggregates in neurons is a pathological hallmark of HD. 56 Similar to other neurodegenerative disorders, abnormal protein accumulation contributes to progressive neuronal dysfunction and cell death. The glymphatic system has been extensively studied in AD for its role in removing Aβ and other toxic proteins. However, its role in HD pathogenesis remains less understood.
The glymphatic system relies on astrocytic AQP4 channels to facilitate CSF influx and ISF exchange, promoting the clearance of brain metabolic waste and molecules. Studies suggest that altered AQP4 localization on astrocytic end-feet disrupts glymphatic function in neurodegenerative conditions,57,58 impairing waste clearance and exacerbating neurodegeneration. Additionally, other protein clearance mechanisms, such as the proteasome and autophagy-lysosome systems, are often overwhelmed or dysfunctional in HD due to cellular stress, further contributing to toxic protein accumulation. 59
Astrocytic dysfunction in HD is associated with impaired neuronal support, neurotransmitter dysregulation, and heightened neuroinflammation. Notably, AQP4 dysregulation reduces glymphatic efficiency, 4 potentially accelerating mHTT aggregation and neurodegeneration. Restoring AQP4 localization on the astrocytic endfeet and efficient glymphatic transport may provide therapeutic benefits by improving metabolic waste clearance and cellular homeostasis.
Beyond waste clearance, the glymphatic system also distributes essential nutrients, such as glucose and amino acids, critical for maintaining the brain's high metabolic demands. 60 İt has been reported that glymphatic function declines with age,61–63 and evidence suggests the disruption of glymphatic system may interfere with therapeutic efficiency, such as antisense oligonucleotide (ASO) distribution, and exacerbate HD progression. 64 Another study reports that secretion of mHTT from cells in the brain, followed by glymphatic clearance from the extracellular space, contributes to mHTT in the CSF. 3
To determine whether the glymphatic system is disturbed in the HD brain, particularly in the premanifest stage, we combined an in vivo measure of CSF clearance capacity by DGE-MRI 52 with fluorescence-based imaging of CSF tracer influx in a widely-used zQ175 knock-in HD mouse model. We observed that CSF clearance efficiency and glymphatic function were impaired in the zQ175 HD mice, prior to the manifestation of motor deficits and detectable striatal atrophy. 4 Further mechanistic study indicated that AQP4 perivascular localization, 4 a key contributor to glymphatic function, was significantly reduced in both HD mouse and human brains. The decline of glymphatic function in premanifest HD mice suggests that treatments directed at restoring normal glymphatic transport and waste removal from the brain may become a preventive or therapeutic approach for HD (Figure 1). These findings set the premise to further investigate the role of glymphatic function in HD pathogenesis as a potential therapeutic target as well as an early biomarker for this devastating disease.
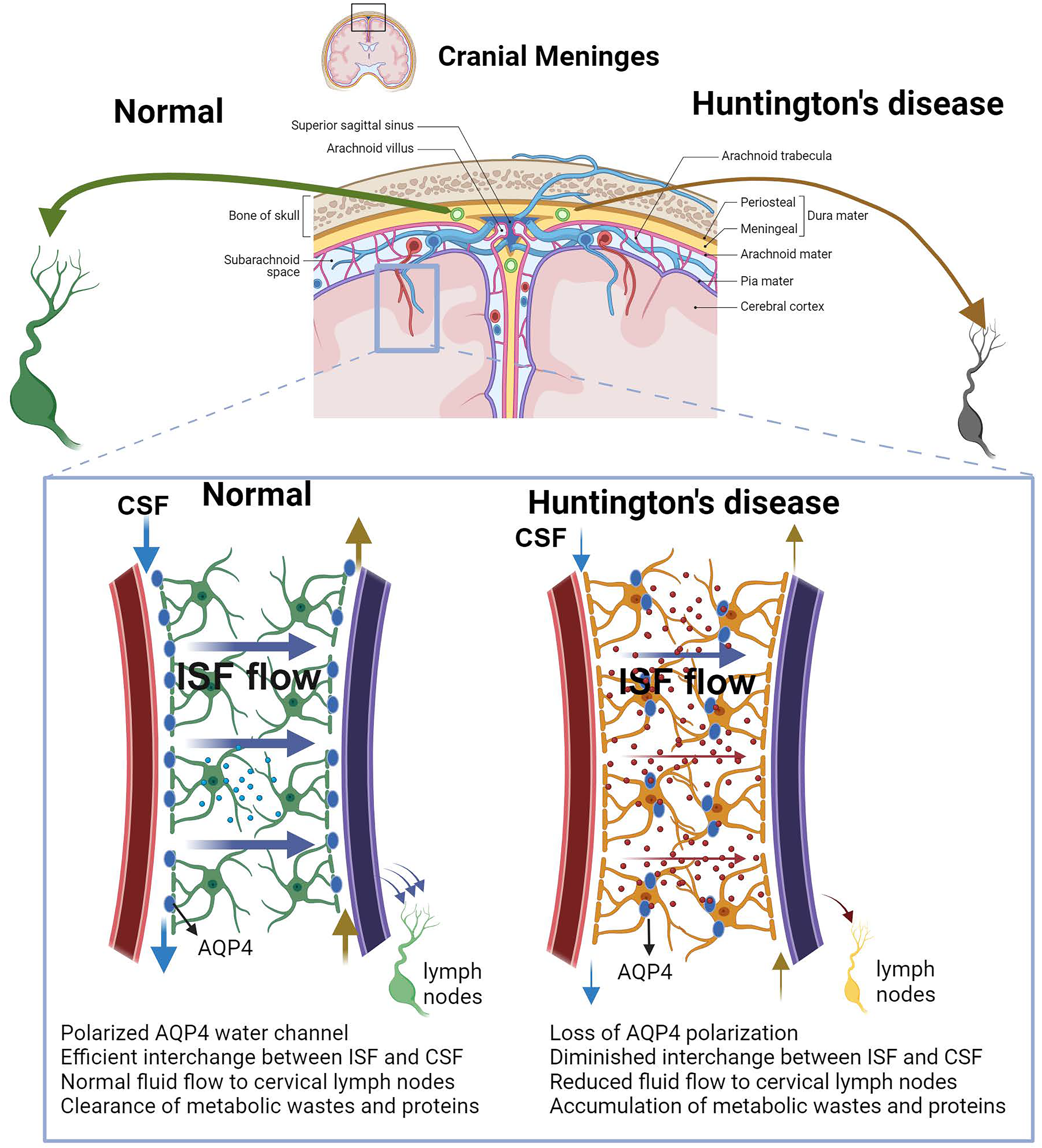
The schematic illustrates the anatomy and function of the glymphatic system and meningeal lymphatic vessels under normal conditions and in Huntington's disease (HD). The glymphatic system consists of periarterial cerebrospinal fluid (CSF) inflow channels, astrocytes-mediated fluid and solute exchange between CSF and interstitial fluid (ISF) via convective flow (ISF flow), and perivenous ISF outflow channels. CSF from the subarachnoid space is flowed into the brain parenchyma via periarterial space, after the fluid exchange, ISF with metabolic wastes ultimately drain out of the brain via meningeal lymphatic vessels and reach to the cervical lymph nodes. Aquaporin-4 (AQP4) polarized on the astrocytic end-feet facilitate CSF-ISF exchanges. In HD, the loss of AQP4 polarization on astrocytic end-feet significantly impairs CSF-ISF exchange and overall glymphatic. This results in reduced clearance of neurotoxic solutes and inflammatory factors, leading to accumulation of abnormal protein accumulation and subsequent neurotoxicity.
In human studies, assessing PVS provides valuable insights into the functionality of the glymphatic system. Chan et al. (2021) investigated the association between dilated PVS and HD severity, finding that increased PVS volume in the subcortical forebrain correlates with more advanced disease stages, 65 suggesting PVS as a potential imaging biomarker for HD progression. Valdés Hernández et al. utilized structural neuroimaging to differentiate between individuals at risk for HD and those with manifest disease in Colombian families, the results indicated that striatal grey matter volume, global brain atrophy and PVS burden may serve as differential indicators of disease manifestation in HD. 66 Bulk et al. conducted a pathological characterization of T2*-weighted MRI contrast in the striatum of HD patients and identified large focal hypointensities within the striatum of HD patients. Upon histological examination, these large focal hypointensities frequently colocalized with enlarged PVS. 67 Chan et al. also examined cerebrovascular reactivity in HD patients, reporting impairments in cerebrovascular reactivity and dilated PVS that may contribute to disease pathology and progression. 68 Coleman et al. assessed PVS morphometry across the white matter in HD using MRI and reported relatively preserved PVS morphometry across the global white matter of pre-HD and early-HD, while subtle morphometric abnormalities are implied but require confirmation in a larger cohort of HD subjects. Collectively, these studies underscore the significance of PVS and glymphatic function in HD, offering avenues for future research into their roles as biomarkers and therapeutic targets for HD.
In the follow up research, it would be important to clarify factors that impair or enhance the glymphatic function in order to map the time course of pathological changes in the glymphatic function in HD progression. We have found that redistribution of astrocytic AQP4 is one of the molecular events occurred in HD brain. 4 It has been established that glymphatic clearance is primarily active during sleep.69,70 Coincidentally, HD patients suffer from circadian rhythm disorders. 71 Thus, it is interesting to study whether improving the sleep quality of HD patients is an effective approach to improve glymphatic function and slow disease progression.
In addition, studies have collectively suggested that drainage of CSF through dural MLVs is important as a final exit route for the clearance of Alzheimer's disease related proteins produced in ISF.20,72 Although the contributions of dural MLVs to CSF macromolecule drainage in the context of difference CNS diseases remains a topic of debate. It is crucial to conduct in-depth investigations into how clearance by MLVs is regulated and involved in HD pathogenesis.
Recently, parenchymal border macrophages are shown to influence vascular pulsation presumably by participating in the metabolism of the extracellular matrix, thereby regulating CSF flow. 73 In line with this discovery, it has been demonstrated that the chemical ablation of parenchymal border macrophages leads to the increased accumulation of Aβ and tau, suggesting its crucial role in the progression of AD pathology.73,74 Further research is needed to gain a better understanding of whether parenchymal border macrophages influence CSF transport and glymphatic function in HD and how neuro-immune interaction at the glymphatic systems regulate one another.
While the majority of current therapeutic interventions for HD primarily target mHTT genetically, one critical research challenge is to determine whether enhancement of brain endogenous clearance pathways could be also a therapeutic strategy for this devastating disorder.
Modulators of glymphatic system: Potential therapeutic strategies for HD
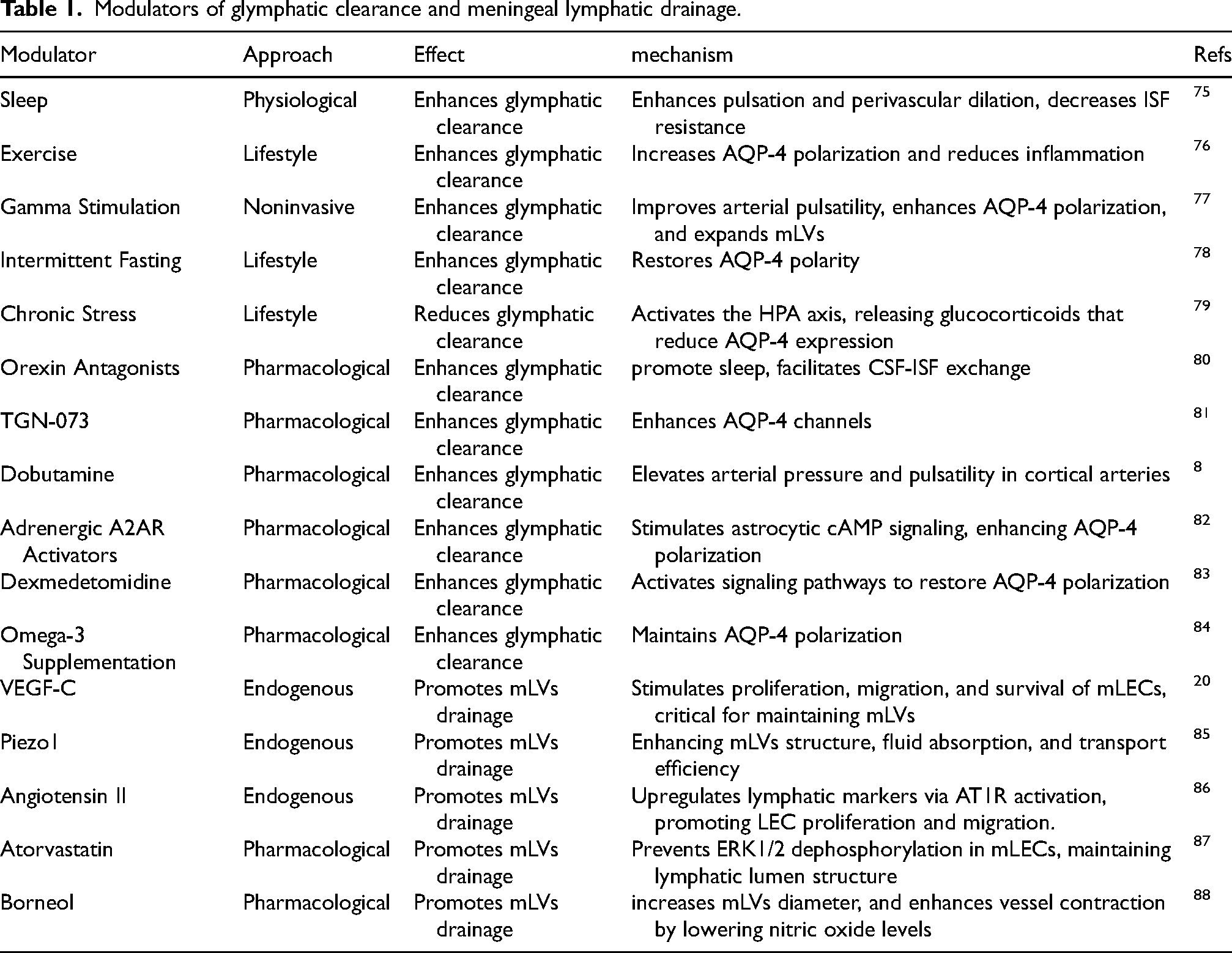
Interventions targeting glymphatic function through physiological factors and pharmacological modulations hold therapeutic potential for HD (Table 1).
Modulators of glymphatic clearance and meningeal lymphatic drainage.
Modulating physiological factors to intervene in the glymphatic system
Sleep regulation
Sleep plays a critical role in clearing metabolic waste from the brain. During sleep, intercellular space increases by approximately 60%, enhancing the convective flux of ISF within brain tissue and significantly improving CSF-ISF exchange. 7 Sleep disturbances profoundly affecting the quality of life and potentially exacerbating disease progression in HD. HD patients often have disrupted circadian rhythms, resulting in fragmented sleep patterns and diminished restorative sleep. 89
The glymphatic system exhibits a pronounced diurnal rhythm. Maintaining these rhythms is essential for efficient waste clearance. 38 Additionally, during non-rapid eye movement (NREM) sleep, slow-wave neural activity induces fluctuations in cerebral blood flow, which are coupled with macroscopic oscillations of CSF, further regulating CSF outflow. 90 These processes collectively enhance metabolic waste clearance through the glymphatic system.
Dysregulation of circadian in HD may compound neurodegenerative processes by impairing glymphatic function.91,92 Addressing sleep abnormalities could improve glymphatic clearance efficiency and may provide a new avenue for mitigating functional decline in HD patients.
Very low-intensity ultrasound
Very low-intensity ultrasound (VLIUS) has been show to stimulate neurogenesis in the mouse brain. 93 A recent study evaluated various ultrasound intensities and found that a spatial peak temporal average intensity (Ispta) of 3.68 mW/cm² effectively promoted CSF tracer influx into the mouse brain. 94 This enhancement of interstitial substance clearance was mediated through activation of the transient receptor potential vanilloid 4 (TRPV4)-AQP4 pathway. Mechanistic investigations further revealed that VLIUS stimulation promotes AQP4 translocation to the cell surface and modulates astrocytic cell volumes within the glia limitans, without causing observable side effects. 94 Given its non-invasive nature, exploring this strategy in the context of HD could hold therapeutic promise for improving glymphatic function and neurodegenerative outcomes.
Gamma sensory stimulation
40 Hz sensory stimulation has been shown to be safe, tolerable, and capable of efficiently inducing gamma activity in both mouse and human brains. 95 This stimulation has demonstrated the ability to reduce amyloid pathology, mitigate tauopathy, and improve cognitive performance in mouse models of AD.96,97 Recent findings indicate that gamma sensory stimulation enhances CSF influx and ISF efflux, while also increasing AQP4 polarization in AD mice, 77 suggesting a mechanism by which it facilitates amyloid clearance through improved glymphatic function. Future studies of the effect of gamma sensory stimulation on HD progression may provide a new, noninvasive treatment approach for HD.
Physical exercise
Studies have shown that voluntary exercise stimulates the expression of AQP4 protein, redistribute AQP4, and expedites solute macromolecule clearance within the glymphatic system, thereby reducing the Aβ deposition.76,98 Aging is linked to a decline in glymphatic system efficiency, partially attributed to diminished pulsation in cerebral artery walls.2,62 Modulating these physiological factors that influence glymphatic system function may partly involve changes in cerebral artery pulsation penetrability. Furthermore, identifying novel mechanisms that influence cerebral artery pulsation penetrability and facilitate CSF flow into brain tissue could have significant implications for promoting the clearance of metabolic waste.
Pharmacological modulation of glymphatic functionality
Targeting AQP4
Genetic deletion of AQP4 in murine models results in a marked reduction in CSF influx into the brain parenchyma. 9 In our recent study, glymphatic influx and AQP4 polarization were significantly impaired in premanifest zQ175 HD mice, 4 supporting the critical role of AQP4 in brain waste clearance. Rectifying AQP4 polarity through genetic or pharmacological approaches holds considerable therapeutic potential for HD.
One promising approach involves a nucleic acid-based drug that overexpresses Dystrophin 71 (DP71), which has been shown to improve brain edema by enhancing the co-localization and interaction of AQP4 with DP71, thereby restoring AQP4 polarity. 99 Additionally, pharmacological inhibition of Matrix Metalloproteinase-9 (MMP9) using GM6001 has been demonstrated to restore AQP4 polarity, re-establish contacts between the basement membrane and astrocyte end-feet, and provide neuroprotective effects in a Parkinson's disease model. 100 These interventions promote metabolic homeostasis and suggest that restoring AQP4 polarity is a promising strategy to enhance glymphatic system function. Testing these AQP4 modulators in HD models could provide novel insights and therapeutic avenues for addressing glymphatic dysfunction in HD.
Targeting norepinephrine receptor
The use of norepinephrine receptor antagonists (such as prazosin, propranolol, and atipamezole) has been shown to enhance CSF influx into brain tissue, effectively clearing cellular debris. 82 This process helps mitigate tau accumulation, reduces neuroinflammation, and alleviates cerebral edema. Additionally, research has demonstrated that the glucocorticoid dexamethasone, in combination with the selective α2 adrenergic receptor agonist dexmedetomidine, promotes CSF influx into brain tissue and enhances glymphatic system function. 83 However, further studies are needed to better understand the specific mechanisms driving these effects before applying to HD.
Targeting the meningeal lymphatic vessels (MLVs)
Glymphatic system is functional linked to MLVs. Impaired function of the MLVs can disrupt the exchange between CSF and ISF, hindering the clearance of pathological macromolecules and metabolic waste from the brain. 20 Treatment with vascular endothelial growth factor C (VEGF-C) has been shown to enhance the exclusion of large molecules by MLVs in CSF, particularly in aged mice. 20 Additionally, increasing VEGF-C levels through the transplantation of cranial precursor cells in murine models promotes the growth and development of MLVs. This restoration of MLVs function leads to the normalization of intracranial pressure and improved cognitive function, with the beneficial effects largely attributed to the VEGF-C secreted by cranial precursor cells. 101
The Piezo-Type mechanosensitive ion channel component 1 (Piezo1) protein mediates the transduction of mechanical signals into electrochemical signals, which facilitates intracellular signal transduction. Yoda-1, a Piezo1 agonist, improves CSF flow dynamics, promotes MLVs growth and maintenance, and enhances cerebral waste clearance and immune functionality. 85 Additionally, borneol, a naturally occurring bicyclic monoterpene with high lipophilicity that crosses the BBB, has been shown to enhance MLVs clearance, facilitating the entry of large molecules into dCLNs and improving cognitive abilities in AD mouse models. 88 In conclusion, VEGF-C presents significant therapeutic potential, warranting investigation into its efficacy for treating HD.
Future questions and directions
The glymphatic system plays a critical role in CSF circulation and metabolic waste clearance, processes increasingly implicated in HD. Future research on addressing the following questions will overcome current challenges and refine therapeutic strategies for HD.
By addressing these questions, we can advance glymphatic-focused therapies, paving the way for more effective management of HD.
Concluding remarks
The glymphatic system represents a promising avenue for understanding and potentially mitigating HD. Dysfunction in this system impairs CSF circulation and metabolic waste clearance, which may contribute to the accumulation of mHTT aggregates. Sleep disturbances, common in HD patients, could exacerbate glymphatic dysfunction, highlighting the critical role of sleep in supporting glymphatic efficiency and overall brain health. Research has unveiled the multifaceted involvement of glymphatic dysfunction in neurodegenerative conditions, but several key questions remain on the precise role in HD. Therapeutic interventions aimed at enhancing glymphatic flow, such as AQP4 modulators, VEGF-C, or sleep optimization, hold promise in mitigating disease progression. A multidisciplinary approach integrating glymphatic-focused treatments with traditional HD therapies could offer a more effective approach to treating HD and improving quality of life for HD patients.
Footnotes
Acknowledgments
The authors have no acknowledgments to report.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by National Institute of Health R01NS124084, R01NS127344, R21NS135139, and The Bev Hartig Huntington's Disease Foundation (to W.D).
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.