
Abstract
Importance
Constant rates of head and neck cancer (HNC) and increasing rates of Human Papillomavirus (HPV)-driven oropharyngeal cancer highlight the need for increased awareness of HNC risk factors for primary and tertiary prevention.
Objective
To assess awareness of HNC and its risk factors, especially HPV, in patients with a confirmed or suspected HNC diagnosis and healthy controls.
Design
A cross-sectional survey was conducted.
Setting
The study was carried out at two university hospitals.
Participants
In total, 354 participants were included in the study, comprising 139 patients with confirmed HNC, 49 patients with suspected HNC, and 166 healthy controls.
Interventions/Exposures
Participants completed a questionnaire including HNC in general, its risk factors, and the role of HPV.
Main Outcome Measures
Primary outcomes were awareness of HNC risk factors and HPV-driven cancers. The evaluation was based on correct answers to knowledge questions.
Results
A general awareness of HNC was found in 70.3% of all participants. The major risk factors of HNC (smoking cigarettes and alcohol abuse, and HPV infection) were correctly identified in 63.3%, 39.5%, and 17.8%, respectively, with no statistical differences in the identification of the risk factors between the 3 groups. The correct recognition of HPV-associated cancer entities (cervical, anal, oropharyngeal, and vulvar/vaginal/penile cancer) was low, with 31.6%, 7.1%, 10.7%, and 13.6%, respectively. Notably, 63.0% of all participants were unaware of the possibility of an HPV vaccination.
Conclusion
Awareness of HNC and its risk factors, particularly alcohol and HPV, remains low across all groups, even among patients with a confirmed HNC diagnosis. Findings suggest a critical need for targeted educational efforts to improve primary and tertiary HNC prevention.
Relevance
Addressing gaps in HNC awareness can help in prevention and early diagnosis, reducing the HNC burden. Future studies should explore effective educational strategies tailored to at-risk populations.

Key Message
Awareness of head and neck cancer (HNC) risk factors among patients with a confirmed or suspected head and neck cancer diagnosis and healthy controls is limited with higher recognition of smoking as a risk factor (63.3%), but low awareness of alcohol (39.5%) and Human Papillomavirus (HPV) (17.8%) as contributing factors, highlighting a need for targeted education to improve primary and tertiary prevention.
Knowledge about HPV-driven cancers and HPV vaccination is low, potentially undermining the effectiveness of HPV prevention programs and underlining the need for increased public health initiatives focused on HPV awareness.
Strengthening patient education on HNC and its risk factors could significantly impact primary and tertiary prevention efforts, reducing future HNC incidence and improving outcomes for patients with a confirmed HNC diagnosis.
Background
Common head and neck cancer (HNC) subsites include the nose and paranasal sinuses, the oral cavity, pharynx and larynx, as well as the salivary glands. Around 3% of the cancer burden in the United States in 2022 was accounted for HNC. 1
Well-known risk factors of head-neck cancer are the use of tobacco and alcohol, as well as oncogenic (high-risk [HR]) human papillomaviruses (HPV) as a sexually transmitted infection, especially in oropharyngeal cancer. 2 HR-HPV infection can cause premalignant and malignant lesions on different sites, such as the uterine cervix, vulva, vagina, penis, the anus, and the head and neck region, with special remark to the oropharynx.2,3 Oropharyngeal cancers associated with HPV have increased in the last decades, while the incidence of HPV-independent HNC has decreased, especially in industrialized countries.4,5 Around 30% to 86% of oropharyngeal cancers are associated with HR-HPV, depending on the method applied.2,6-8 HR-HPV association of oropharyngeal cancers is often based on the overexpression of the cellular protein p16INK4A as a surrogate marker upregulated by the HPV oncoprotein E7.9,10 HR-HPV induced oropharyngeal cancers have different associated risk factors, namely less consumption of alcohol and cigarettes, as well as younger age, compared to non-HPV driven cancers. Furthermore, the prognosis of HR-HPV-driven oropharyngeal cancer patients is improved compared to their HPV-independent counterparts.11,12
Awareness of certain diseases includes the knowledge of the disease, its early symptoms, and its risk factors. The public awareness and understanding of HNCs, varying based on the respondents of surveys, has been identified in several previous studies.13,14 Especially the awareness of the link between HPV and oropharyngeal cancer has been analyzed. 15 Furthermore, the risk perception of smoking in causing HNC has been analyzed in smokers and nonsmokers. 16 However, suspected or confirmed HNC patients’ combined awareness of all HNC risk factors has not been investigated in previous studies. The awareness and the risk perception of HNC are essential as primary prevention of cancer and tertiary prevention of recurrence. Primary prevention of HNC might include the avoidance of substance abuse, such as cigarettes or alcohol and vaccination against HR-HPV.
In 2006, the US Food and Drug Administration approved the first HPV vaccination protecting against HPV-driven cancers. In Germany, HPV vaccination was introduced in 2007 for girls aged 12 to 17. 17 In 2014, the recommended age was reduced to 9 to 14 years. In 2018, the vaccination recommendation was extended to boys. 18 The growing evidence of HPV vaccination has been analyzed in several studies.19,20 However, the HPV vaccination rate of 40% in the target groups in Germany is below the essential herd immunity rate.20,21
This study assessed the current knowledge of risk factors of HNC in affected cancer patients, as well as in suspected cancer patients and a healthy control group. A deeper knowledge was assumed in patients with a confirmed HNC diagnosis. The knowledge of HPV-driven cancers and HPV vaccination was furthermore investigated. This study aims to assess the need for improvements in primary prevention and health education.
Methods
The cross-sectional study was conducted at two university hospitals in Germany. The anonymous questionnaire was developed and structured in four thematic sections, including (1) demographic data, (2) knowledge of risk factors of HNC, (3) knowledge of HPV-associated cancer entities, and (4) general knowledge of HPV and opinion toward vaccination. The complete questionnaire is provided in the Supplemental Material. Collected demographic data included gender, age, sexual orientation, educational degree, current occupation, and consumption of cigarettes and alcohol. The education degree was classified into no degree, lower educational level (including lower secondary school and secondary school), and higher educational level (including German A levels, university degree, doctoral thesis). Alcohol consumption was assessed by self-reported frequency categories (never, seldom, former, often (2-6 times/week), daily) and by the reported intake of beer, wine, and alcoholic spirits, or to indicate if they were abstinent, including the duration of abstinence and the number of prior years of regular consumption. Based on these data, alcohol abuse was defined as an average intake of more than 24g of pure alcohol per day (approximately 2 standard drinks per day), regardless of gender. Most of the questions required a single response, except for the questions asking for risk factors of HNC and HPV-associated cancer entities. According to the Helsinki Declaration, the study was approved by the respective local institutional ethical review boards.
The survey was conducted between April 2020 and July 2021. Participants were recruited within the two institutions during consultation hours and were assigned to one of the three groups: (A) known HNC, (B) suspected HNC based on clinical examination, (C) neither known nor suspected HNC (healthy controls). The healthy control group consisted of patients attending the consultations for non-oncological reasons, such as minor otolaryngology complaints. Participants were included based on a minimum age of 18 years, being legally in charge, having given approval to the study, and being able to understand German. To ensure a homogeneous study cohort of group A and group B, patients with tumors of anatomical sites associated with different etiological risk factors than those typically observed in squamous cell carcinomas, such as the salivary gland, were excluded from further analysis. Only fully completed questionnaires were considered.
Statistical analyses were performed using SAS version 4.0 and IBM SPSS statistical software version 27. Previously, the study size was calculated and comprehensibility was tested based on a pilot study performed on 25 randomly selected persons. The participants of the pilot study were not included in the final survey. Most collected data were demographic variables tested against the knowledge variables (knowledge of HNC and knowledge of HPV), representing the outcome. Groups A, B, and C were compared, and results were also stratified by demographic variables. Knowledge of risk factors of HNC and HPV-driven cancer entities was based on correctly identified responses to multiple choice questions summing up in a score. Chi2-test or t-test was used to identify the association between variables with a level of significance of .05.
Results
Population
A total of 398 participants completed the survey. Because of the recruitment during consultation hours, the dropout rate was rather low, with 15 patients. Of the 158 patients diagnosed with cancer and the 74 patients with suspected cancer, 19 and 25 patients, respectively, were excluded from further analysis because the anatomical localization of their tumor was associated with distinct pathogenetic risk profiles compared to squamous cell carcinomas, such as those observed in salivary gland tumors. In total, 139 (39.3%) participants were diagnosed with HNC prior to the survey. The most common localizations were oropharynx (70/139), larynx (40/139), and hypopharynx (5/139). HNC was suspected in 49 participants (13.8%), and 166 (46.9%) participants had neither a diagnosed nor a suspected HNC. In total, 211 male patients (59.6%) and 143 female patients (40.4%) completed the survey. The mean age was 55 (standard deviation [SD] = 17.7) years and differed between the 3 included groups (Tab. 1). On average, participants with a diagnosed HNC were older (65 years) compared to the participants with neither diagnosed nor suspected HNC (45 years) (P < .001). Most of the participants had a steady partner (53.4%) and fewer than or equal to 5 sexual intercourse partners in life (50.6%). Concerning the partnership status, a significant difference was identified between patients with HNC and healthy controls (P < .001). The number of lifetime sexual intercourse partners did not differ significantly between the three groups. The majority of participants (62.9%) had at least a secondary school degree; however, participants with confirmed HNC or with suspected HNC had a statistically significantly lower educational level (P < .001). Around 75.1% of participants were in active employment. Of 354 participants, 246 (69.5%) were former or current smokers (compare Table 1). Patients with confirmed HNC or suspected HNC were identified with a median of 30.0 (0-125) pack years compared to a median of 10.0 (0-88) for participants in the control arm. Current or former abuse of alcohol was detected in 29.5% of participants with HNC diagnosis and 26.5% of the participants with suspected HNC, respectively. In 74/139 (53.2%) of the HNC group p16INK4A-status was analyzed in tumor tissue. In 47.3%, p16INK4A was detected.
Demographic Data of Participants.

Abbreviations: HNC, Head and neck cancer; SD, Standard deviation.
Identification of etiologic factors of HNC
In total, 70.3% (249/354) of the respondents stated having some knowledge of HNC prior to the survey. Seventy-six percent of women compared to 66.4% of men stated to have some knowledge of HNC (P < .05). No differences could be identified based on family status, smoking or alcohol abuse, sexual orientation, or experience. Respondents indicated that they have heard of HNC in the media, through relatives or friends, by general knowledge, at school or their jobs, and via medical doctors.
The possible etiologic factors, cigarette consumption, alcohol consumption, and infection with high-risk HPV were correctly identified in 63.3%, 39.5%, and 17.8%, respectively. Participants with neither suspected nor diagnosed HNC identified all etiologic factors equal to those of patients with diagnosed or suspected HNC (Figure 1). No statistical significance of knowledge on each risk factor alone (P = .73, P = .53, and P = .84, respectively) or combined (P = .87) was identified between the three groups. Only a minority of participants (10.7%) were able to name all three risk factors correctly. No differences in general knowledge of the etiological factors of HNC based on gender, age, marital status, and cigarette consumption were detected between the three groups (diagnosed HNC, suspected HNC, neither). However, differences were found based on education level (P < .05). Participants with higher education had significant greater knowledge compared to those with lower or no education (P < .05). However, no differences of knowledge of participants with higher education were observed among the three groups (P = .61). Persons with daily or former alcohol abuse showed significantly higher awareness that alcohol is a risk factor for HNC (52.1% and 61.5%, respectively) compared to participants with regular/lower/no consumption (46.6%, 41.7%, and 31.3%, respectively) (P < .05). Current or former smokers associated excessive cigarette consumption in 66.4% with HNC compared to the none smokers with 56.5% (P = .079). Thirty-seven participants stated that either they or their children are vaccinated against HPV. Among them, 13/37 (35.1%) of those identified HPV correctly as a possible etiological factor in HNC compared to the unvaccinated participants with 50/317 (15.8%) (P < .005).
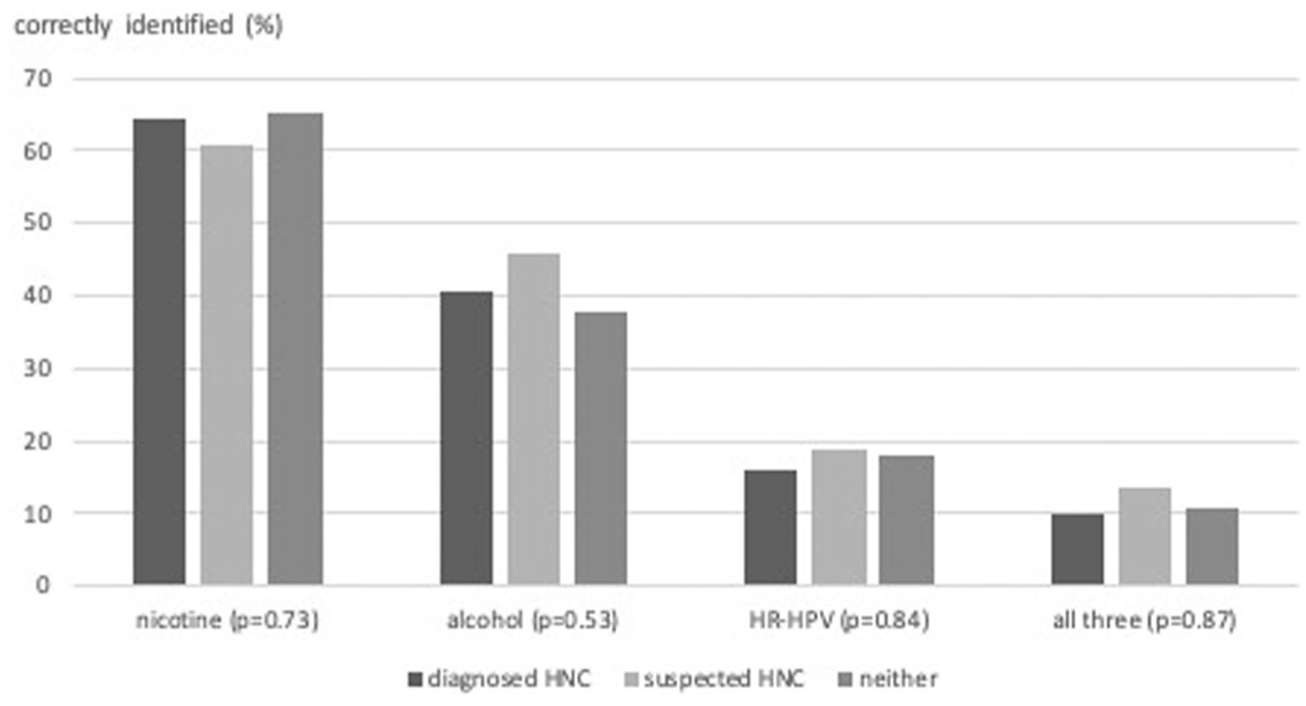
Identification of etiological risk factors of HNC (P-values analyze differences in knowledge between the 3 groups). HNC, Head and neck cancer.
The assumed knowledge of the participants was based on information they received via various media platforms or the internet in 30.2%, via professional medical advice in 18.6%, via relatives/friends in 11.9%, or others in 9.3%. Other sources were named to be schools, universities, and jobs.
Awareness of HPV
The survey included the question on whether bacteria or viruses in general could cause cancer. In total, 55.4% (196/354) of the participants were not sure, 36.2% (128/354) assumed bacteria or viruses could drive cancer, and 8.5% (30/354) denied that cancer could be caused by bacteria or viruses. Free responses why bacteria or viruses could not be etiological factors of cancer included “mutations cause cancer,” “cancer is genetic,” “cancer is not an infection,” and “risk factors of cancers are not well known.” Participants were asked whether HPV infection is possible to be cured. The majority of participants were not sure (62.4%). However, 31.4% named a therapy for HPV infections is available.
Participants were asked to identify possible HPV-driven cancer entities. Cervical cancer was named as HPV-driven in 31.6% (112), anal cancer in 7.1% (25), oropharyngeal cancer in 10.7% (38), and vulvar/vaginal/penile cancer in 13.6% (48). Only three participants correctly identified all HPV-driven cancers (0.8%). Patients who were aware of risk factors of HNC demonstrated better knowledge of HPV-driven cancer entities across all affected anatomical sites (P < .001).
Women were asked in the survey whether they had papilloma, genital warts, or cervical dysplasia in a preventive gynecological examination. Twenty-one (14.7%) women stated that they had some alterations in the past. These 21 women had a better knowledge of HPV-driven cervical cancer (66.7%) than those women without any alterations (37.7%) (P < .05), but no differences in identifying the relevance of HPV in anal (P = .4), oropharyngeal (P = .6), or any other genital cancer (P = .07) were detected. Participants who were HPV vaccinated themselves or had vaccinated children identified the HPV-driven cancer entities cervical cancer, oropharyngeal cancer, and vulvar/vaginal/penile cancer more frequently (P < .05). However, no difference was detected between vaccinated and non-vaccinated participants regarding the recognition of HPV as an etiological risk factor for anal cancer (P = .79).
Comparing the three groups, participants with previously diagnosed HNC were less able to detect HPV-related cancers, except for oropharyngeal cancers (Figure 2).
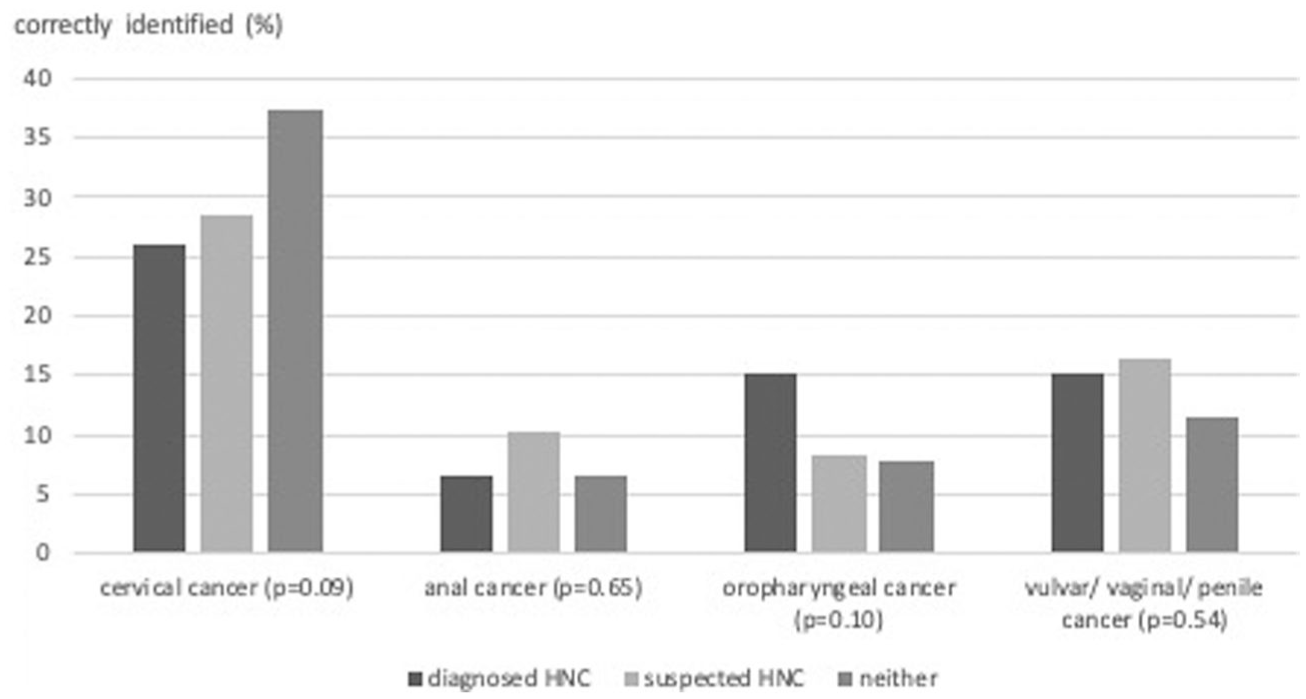
Knowledge of HR-HPV-driven cancer (P-values analyze differences in knowledge between the 3 groups). HR, High-risk; HPV, Human papillomavirus.
HPV Vaccination
The last part of the survey concentrated on HPV vaccination. Therefore, participants were asked whether a vaccination for HPV is available. Of 354 participants, 223 (63.0%) negated the possibility of HPV vaccination. A correlation between HPV awareness and the knowledge of the possibility of a vaccination could be identified (P < .001). Of 131 participants aware of HPV vaccinations, 72 (55.0%) responded that the vaccination is available for both boys and girls, while 57 (43.5%) assumed the vaccination is only available for girls (Table 2).
Awareness of HPV Vaccination (P = .236).
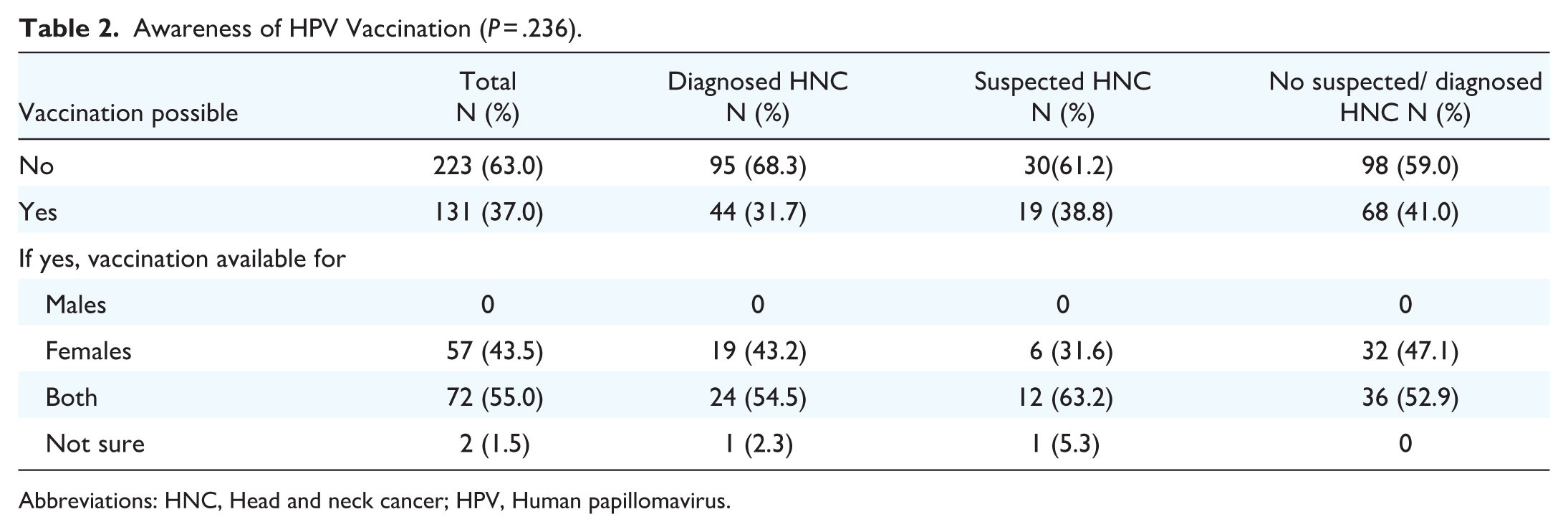
Abbreviations: HNC, Head and neck cancer; HPV, Human papillomavirus.
In total, 37/354 (10.5%) of participants responded that either they or their children received any HPV vaccination. Participants who did not receive the vaccination were asked why they were not vaccinated. In 40.1% (127/317), the vaccination was not available at that time. A minority (2.2%) was not vaccinated due to the costs not being covered by their health insurance company. Other reasons were “no knowledge about HPV or the vaccination,” “no necessity,” and “questionable ingredients.” In the last survey question, participants were asked whether they would like to receive an HPV vaccination. Around 8.5% (30/354) denied it, while 35.6% (126/354) would like to receive the vaccination, and 55.9% (198/354) were unsure. Possible reasons why participants did not want to get vaccinated included the answers “too old,” “no effect,” “not enough information,” and “don’t get vaccinated in general.”
Discussion
HNC has a high cancer burden. 1 However, public awareness is still low as demonstrated in this study. Cancer awareness can be described as knowledge of certain cancer entities’ risk factors and early symptoms. Only 70.3% of the respondents in this study were aware of HNC in general. HNC affects men more often. 22 Interestingly, no certain demographic factors, except gender differences, could be associated with general HNC awareness. Given that many people were unaware of HNC, early but nonspecific symptoms like oral mucosal irritation and early onset of dysphagia or mucosal alterations might be misinterpreted, preventing early diagnosis and treatment.
Smoking cigarettes and alcohol abuse have been well established as possible risk factors of HNC. 23 Especially in the western countries, the consumption of cigarettes has declined in the last years, and so has the incidence of HNC, except for HPV-driven oropharyngeal cancers.4,5,24 In this study, the majority of participants (63.3%) were aware that smoking cigarettes was a risk factor for HNC. Possible explanations for this comparatively good awareness of this particular risk factor might be media campaigns and German governmental laws as the introduction of labeling cigarette packs with health warnings and daunting images that show possible health risks triggered by continuous cigarette consumption. 25 In contrast to a decline in the consumption of cigarettes, the nicotine consumption through other means has increased.26,27 However, the awareness of nicotine consumption, particularly through alternative forms such as e-cigarettes, was not specifically assessed. While the carcinogenic effects of cigarette smoking are well-documented, the evidence of the carcinogenic effects of nicotine consumption through alternative forms remains less conclusive. Surprisingly, alcohol abuse was identified in only 39.5% of the respondents as a potential risk factor for HNC. The public awareness of alcohol causing cancer in general is very low. 28 Interestingly, 52.1% and 61.5%, respectively, of participants with a current or former abusive consumption of alcohol correctly named alcohol abuse as one of the risk factors of HNC compared to participants with regular, but not daily/ lower or no alcohol consumption (46.6%, 41.7%, and 31.3%, respectively). These results may lead to the hypothesis that people who regularly consume alcohol have a particular awareness of the potential harm that alcohol abuse might cause. Health warnings on alcohol bottles might increase the awareness of alcohol as a potential risk factor for cancer. Oropharyngeal cancer is known to be associated with HPV. 2 The relevance of HPV in causing HNC was correctly identified by only 17.8% of all participants. HPV vaccinated participants or participants with vaccinated children were aware of the link between HPV and HNC, but not of HPV and anal cancer. These findings concerning HNC were not consistent with a previous report. 14 In former studies, up to 49% of the participants were aware of the association of HPV and HNC, especially oropharyngeal cancer.29,30 These differing results might be explainable with several demographic factors such as younger age, better local public and individual health education, country of origin, and different selections of participants. The awareness of the role of HPV in causing cancer depends on the HPV-driven cancer entity. In contrast, the association between cervical cancer and HPV is better known, with up to 45.6% in other studies.31,32
Patients with a previously diagnosed HNC did not have a significantly better prior knowledge of the potential risk factors than the other two groups. Previous studies on different cancer entities have reported similar results, underlying the necessity of the education of every single affected person by the clinicians at the point of diagnosis. 33 Education should reduce risk factors as tertiary prevention. In this context, tertiary prevention refers specifically to the reduction of established behavioral risk factors, particularly smoking cigarettes and alcohol abuse, following cancer diagnosis. Targeted patient education has the potential to support the risk-reducing behaviors and improve the long-term outcome. The ways affected people want to receive their information might differ based on their backgrounds and their cancer (stage) and should therefore be adapted individually.34,35
HPV awareness appears to be relevant when it comes to vaccination. Parents being more aware of the possible consequences of HPV infections intend to get their children vaccinated more often. 36 In Germany, HPV vaccination was introduced in 2007. However, 15 years later, only a minority has been vaccinated, which is not sufficient for herd immunity. In our study, only around 37% of participants were aware of HPV vaccination. Of those who were aware of HPV vaccination, only 55% knew that the vaccination is available for both boys and girls, and only 10.5% of participants were either vaccinated themselves or had vaccinated children. Since 2018, the recommendation of the German “Robert-Koch-Institut” (responsible for vaccination recommendations in Germany) has been expanded, including boys and girls aged 9 to 17 years. 18 For comparison, HPV vaccination was introduced in 2006 for girls aged 11 and 12 and in 2011 for both boys and girls in the United States. The Advisory Committee on Immunization Practices recommends routine HPV vaccination at 11 or 12, with the possibility to start at age 9 and catch-up vaccination is advised up to age 26.37,38
The necessity of rising HNC awareness has been outlined before, leading to early treatment. A possible way leading to better awareness is the awareness month. During the specific month for certain cancer entities people get educated via different ways about possible early symptoms or risk factors.39,40 Furthermore, extensive media or social media prevention campaigns may lead to rising cancer or vaccination awareness. In 2013, the European Head and Neck Society launched the “make sense campaign” to raise awareness of HNC. Usually, this theme week takes place once a year, mainly at large medical centers, to inform patients about HNC and its risk factors. 41 However, this campaign’s primary prevention impact is not yet sufficiently analyzed. So far, screening programs have been well established for other cancer entities, with health insurance usually covering the costs. However, no regulated screening program has yet been established for HNC. Further programs and studies should evaluate the necessity of screening programs for HNC.
Strength and Limitations
To the best of our knowledge, this is the first study assessing the awareness of HNC and HPV in patients with a confirmed or suspected HNC diagnosis. We compiled the survey in 354 patients, enabling us to control for confounding factors, such as age, gender, sexual orientation, marital status, and cigarette and alcohol consumption. The data on the knowledge of risk factors in HNC allowed us to highlight the necessity of improving primary and tertiary prevention in HNC. We further investigated the awareness of HPV and vaccination in causing cancer in the cohort, providing more targets for health education. However, this study has several limitations that may affect the generalizability of the findings. First, only participants who were patients or relatives of patients at the otolaryngology departments were included, which might have been prone to selection bias. Furthermore, patients who were not able to understand German were excluded from this analysis. This exclusion may lead to an underrepresentation of individuals from lower socioeconomic backgrounds, who are known to be at higher risk for HNC. Consequently, the generalizability of our findings, particularly with regard to awareness of risk factors in more socioeconomically diverse populations, might be limited. The participants selected for this study are most likely urban dwellers and might have higher health-literacy. Consequently, a selection bias was created, limiting the generalizability to broader, more diverse populations. Further studies should aim to include participants from a wider range of settings to underline the variability in awareness of HNC risk factors across different demographic groups. The subjects from the two university outpatient clinics were personally recruited with the help of a questionnaire, which can lead to bias in the answers, as bias can occur in sensitive questions. This bias (“social desirability bias”) results from the tendency to respond to questions not in terms of personal attitudes but according to social norms that the subject deems desirable. Especially questions about sexual behavior are still taboo among older people and thus may not be answered truthfully. In addition, people with a lower level of education may feel intimidated by questions they do not understand; therefore, they either refuse to participate directly or select “don’t know” for many questions with a high tendency. Furthermore, the group of subjects may differ significantly from the general population. For example, 91.5% of participants identified as heterosexual, leaving limited representation of homosexual, bisexual, and nonbinary individuals. Given the relevance of HPV-associated cancers in specific populations, particularly those disproportionately affected by HPV, this imbalance limits our ability to assess knowledge disparities across sexual orientations. To perform more complex statistical analyses, a larger sample size is required. Moreover, the three study groups (HNC patients, suspected HNC patients, control group) were not comparable in size and age. In particular, the group of suspected HNC patients was relatively small. Patients in the noncancer group were younger. Furthermore, we did not use a standardized survey.
Conclusion
We demonstrated for the first time the lack of knowledge in patients with a confirmed or suspected HNC diagnosis concerning risk factors of HNC, HPV-driven cancer entities, and HPV vaccination. The general awareness of HNC was 70.3%. However, the awareness of the risk factors of alcohol consumption (39.5%) and HPV (17.8%) was significantly lower than the awareness of smoking cigarettes (63.3%) as a risk factor, which could explain the low primary and tertiary prevention success of HNC. Furthermore, the knowledge of cancer entities driven by HPV was comparably low. In light of the rising incidence of HPV-driven cancer entities and ongoing consumption of alcohol and cigarettes, our study provides many crucial arguments for further studies, educational training, and campaigns aiming to improve the knowledge of affected, possibly affected HNC patients, as well as of the general population.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216261436005 – Supplemental material for Awareness of Head and Neck Cancer, its Risk Factors, and of Human Papillomavirus—A Survey Study
Supplemental material, sj-docx-1-ohn-10.1177_19160216261436005 for Awareness of Head and Neck Cancer, its Risk Factors, and of Human Papillomavirus—A Survey Study by Theresa Obermueller, Sarah Volpe, Denitze Lara Escobar, Annett Pudszuhn, Nicole Rotter, Veit Maria Hofmann and Benedikt Kramer in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author upon reasonable request.*
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Approval and Informed Consent Statements
According to the Helsinki Declaration, the study was approved by the respective local institutional ethical review boards (EA 4/054/20 and 2020-595N). Informed consent was obtained from all individuals involved in the study. Participants were provided with detailed information about the study’s purpose, procedures, potential risks, and benefits, and were given the opportunity to ask questions before consenting. All participants voluntarily agreed to participate and were informed of their right to withdraw from the study at any time without consequence.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.