
Abstract
Importance:
Otitis media with effusion (OME) is common in children, often persisting for more than 3 months, which can lead to hearing loss. Effective treatments are needed to manage this condition.
Objective:
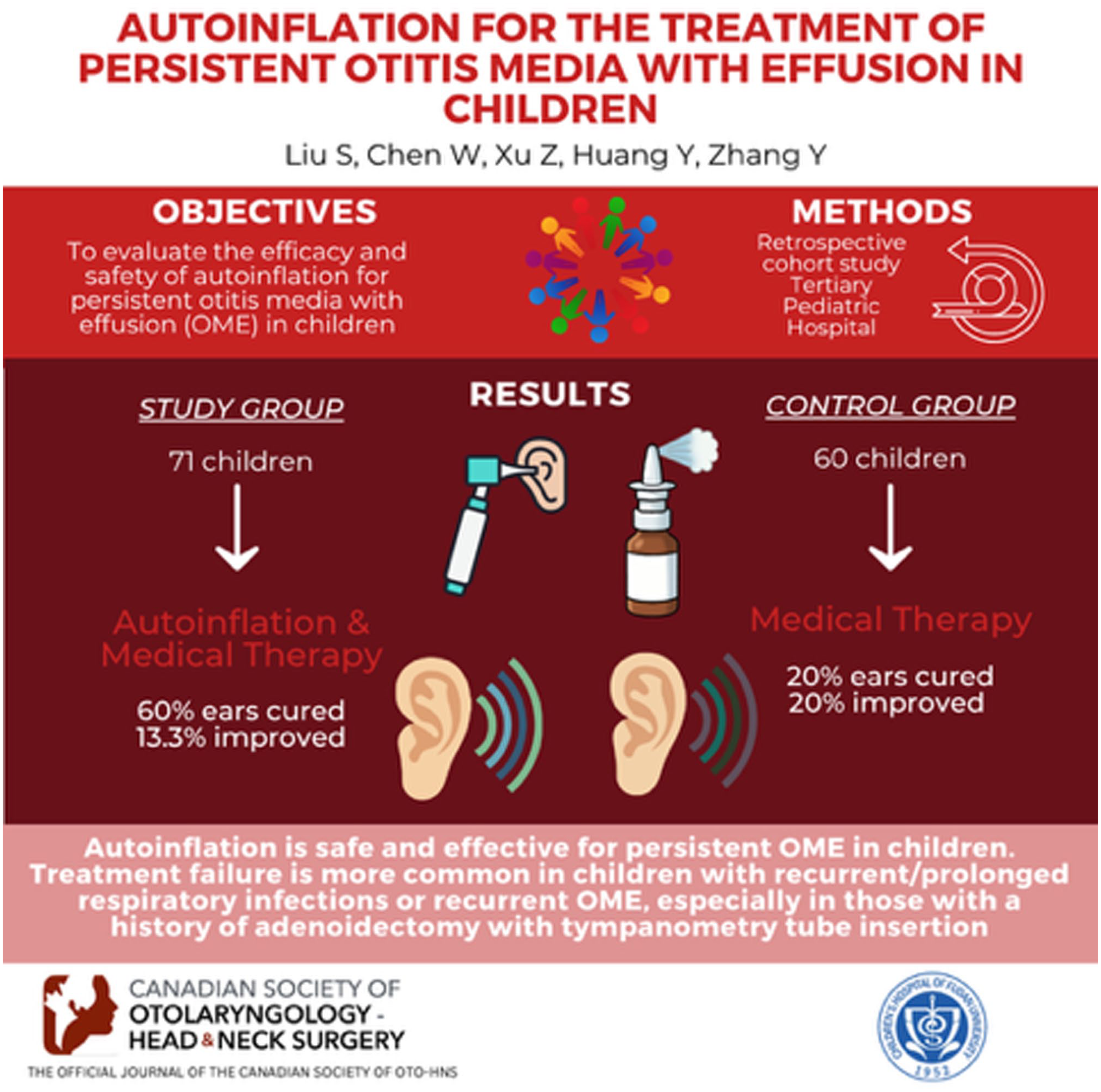
To evaluate the efficacy and safety of autoinflation for persistent OME in children.
Design:
Retrospective cohort study.
Setting:
The study was conducted at a tertiary pediatric hospital.
Participants:
A total of 131 children with persistent OME were enrolled from January 2020 to July 2025. Seventy-one children received autoinflation treatment, and 60 children were assigned to the control group.
Exposure or Intervention:
The autoinflation group received twice-daily autoinflation treatment for 1 to 3 months in addition to medical therapy. The control group received only medical therapy.
Main Outcome Measures:
Efficacy was evaluated based on cure rates assessed by tympanometry and otoacoustic emissions before and after treatment. Safety was assessed through the frequency and severity of adverse events.
Results:
In the autoinflation group after 3 months, 60.8% of ears were cured, and 13.3% showed improvement. In the control group, only 20.0% of ears were cured, and 20.0% improved. Univariate analysis indicated that recurrent OME and recurrent/prolonged respiratory tract infections were significant risk factors for autoinflation failure. Approximately half of the children experienced mild ear pain during the first week, which was generally tolerable.
Conclusion:
Autoinflation appears to be safe and effective in children with persistent OME. Treatment failure is more common in children with recurrent/prolonged respiratory infections or recurrent OME, especially in those with a history of middle ear surgery (adenoidectomy with tympanostomy tube insertion). Although autoinflation is a low-risk alternative to surgery for suitable patients, it should be avoided in children with skull base or orbital defects, craniofacial anomalies, or active infection or inflammation.
Relevance:
This retrospective cohort study supports the use of autoinflation as a treatment option for persistent OME. Identifying risk factors for treatment failure may help guide clinical decisions.
Key Message
For children with otitis media with effusion (OME) lasting ≥3 months, autoinflation is a good alternative to surgery. However, for those with recurrent OME or repeated/prolonged upper respiratory tract infections, surgery is still recommended.
Autoinflation appears to be safe, except for children with skull base or orbital defects, craniofacial anomalies, or active infection or inflammation.
Introduction
Otitis media with effusion (OME) is a common pediatric middle ear inflammation with fluid but no infection, often causing conductive hearing loss. In early life, the Eustachian tube is anatomically and functionally immature; it is relatively short, wide, and more horizontally oriented, making it vulnerable to obstruction by local factors such as adenoid hypertrophy. Epidemiological data indicate that more than 50% of infants experience at least one episode of OME within the first year of life, rising to approximately 60% by 2 years of age. 1 A screening study of 5 to 6-year-old primary school children reported unilateral or bilateral middle ear effusion in 1 out of 8 participants. 2 As the period from 1 to 6 years is critical for language acquisition, prolonged OME-related hearing loss may adversely affect speech and cognitive development. Persistent middle ear effusion can cause irreversible tympanic membrane damage and secondary complications, imposing substantial burdens on families and healthcare systems. 1
OME is typically self-limiting, with a high rate of spontaneous resolution. In children with a disease duration of less than 3 months and no risk factors, unnecessary medical or surgical interventions should be avoided. Alternatives to tympanostomy tube insertion are largely limited to surveillance, because medical therapy (antibiotics, antihistamines, decongestants, systemic steroids, and topical nasal steroids) is ineffective and not recommended. 3 Surgical indications vary slightly across countries. Clinical guidelines for pediatric otitis media usually recommend tympanostomy tube insertion when effusion persists for 3 months or longer. 4 However, for children with OME persisting beyond 3 months whose families decline surgery, there remains no clear consensus regarding the choice between continued medical therapy and autoinflation.
Autoinflation aims to restore middle ear ventilation by increasing nasopharyngeal pressure, thereby opening the Eustachian tube and equalizing pressure across the tympanic membrane. Techniques can be classified as active (eg, the Valsalva maneuver and the Politzer method) or passive. Owing to limited cooperation in young children, passive device-assisted autoinflation is more commonly employed. These approaches require dedicated devices, and multiple studies suggest that they may serve as an effective non-surgical adjunct in the comprehensive management of pediatric OME. Four principal categories of autoinflation devices have been described5-7: nasal balloons connected to tubing, Politzer balloon pressure devices, pressure systems integrated with toys or nasal masks, and electronic autoinflation devices. Device development has progressed over time. The earliest widely used system, a play-based nasal balloon device, was developed by Hunt-Williams in 1968 after 4 years of refinement. It was inexpensive and simple to administer following brief instructions. By 1999, electronically controlled pressure devices had entered clinical practice. Although all devices operate on the same principle of applying positive external pressure to drive air through the Eustachian tube into the middle ear, differences in pressure control, usability, and adherence may influence clinical effectiveness. A review of 11 studies (1036 children) suggested that autoinflation may improve OME-specific quality of life and short-term persistence, but its effect on hearing recovery and adverse events is uncertain. 8 In recent years, OME management guidelines published in many countries have recommended a three-month period of watchful waiting for children without risk factors. During this period, noninvasive autoinflation therapy may be used, which can reduce the likelihood of subsequent surgery (all are Evidence B).1,10-13
In this retrospective cohort study, we evaluated the efficacy and safety of autoinflation in 71 children with persistent OME lasting more than 3 months, aiming to inform management strategies for this patient subgroup.
Methods
Study Design and Patients
This retrospective cohort study included children diagnosed with persistent OME at the outpatient department of Northwest Women’s and Children’s Hospital and the Children’s Hospital of Fudan University Hospital from January 2020 to July 2025. The data were obtained from clinic lists, and patients were included consecutively. Children were considered to have OME if there was evidence of middle ear effusion without signs or symptoms of acute infection. Middle ear effusion was confirmed by pneumatic otoscopy, showing a retracted or opacified tympanic membrane, air fluid levels, or visible bubbles. Moreover, tympanometry (type B) or acoustic reflectometry was used to support the diagnosis. The diagnosis of OME was determined jointly by an otolaryngologist and an audiologist. Inclusion criteria were as follows: (1) Age >4 years; (2) Presence of tympanic membrane retraction or bulging on otoscopy, with visible fluid levels and/or bubbles; (3) Type B or C2 tympanogram; (4) Disease duration ≥3 months, calculated from the date of initial OME diagnosis; (5) No sinusitis or only mild sinusitis (absence of purulent nasal discharge); (6) Ability to comply with autoinflation therapy and follow-up visits. Exclusion criteria were: (1) Children with cleft palate, primary ciliary dyskinesia, immunodeficiency or immunocompromised status, autoimmune diseases, and those taking immunosuppressants; (2) Moderate to severe sinusitis (with purulent nasal discharge); (3) Children with orbital or skull base defects; (4) Inability to cooperate with autoinflation therapy or regular follow-up visits. All patients underwent lateral nasopharyngeal radiographs to assess adenoid size. Diagnosis of adenoid hypertrophy was defined as an adenoid/nasopharynx (A/N) ratio ≥0.6. Recurrent or prolonged respiratory tract infection was defined as experiencing 3 or more episodes of respiratory tract infection (including upper and lower respiratory tracts) during the course of inflation therapy, or as having a prolonged, non-resolving respiratory tract infection. Recurrent OME was defined as a new episode occurring at least 1 month after complete recovery from a previous episode of OME, whether achieved through follow-up, surgical intervention, or non-surgical management.
A total of 71 children were included in this retrospective cohort study, comprising 38 cases of initial persistent OME and 33 cases of recurrent persistent OME, all of whom received autoinflation therapy. During the same study period and from the same clinical setting, 60 children with persistent OME who did not receive autoinflation were consecutively included as the control group. The control group was selected to achieve comparable baseline characteristics with the autoinflation group in terms of age, sex, types of otoacoustic emissions, disease course, OME recurrence, and history of previous OME surgery. However, individual patient matching was not performed. All children in the control group declined autoinflation due to financial reasons. All children received pharmacological treatments prior to and during enrollment, including nasal corticosteroids (eg, mometasone), anti-allergic treatments, and antibiotics for severe sinusitis or respiratory tract infections. This retrospective cohort study was approved by the hospital’s Ethics Committee. The autoinflation group underwent autoinflation therapy (Streamsys, Beijing Zhuochi Technology Co., Ltd., China) in addition to their existing pharmacological treatments.
Audiological Examinations
Tympanometry was performed using the TympStar II middle ear analyzer (GSI, USA) with a 226 Hz probe tone. Tympanogram results were evaluated according to the diagnostic criteria of Bidarian-Moniri et al 14 : (1) A Type B curve or middle-ear pressure ≤−400 daPa indicates middle-ear effusion, consistent with OME. (2) Middle ear pressure between −399 and −200 daPa is classified as a Type C2 curve, suggesting significant negative middle ear pressure and pathology. (3) Middle ear pressure between −199 and +100 daPa, corresponding to Type C1 or Type A curves, excludes OME pathology.
Distortion Product Otoacoustic Emission (DPOAE) testing was performed using the Otoread otoacoustic emission screening device. Pure-tone stimuli were delivered at L1 = 65 dB SPL and L2 = 55 dB SPL, with an f2/f1 ratio of approximately 1.20, presented 30 times per frequency. The headphone frequency response range was set between 2 and 5 kHz. A response signal with an amplitude ≥6 dB above the background noise was considered a pass. The criterion for a passing result was the presence of DPOAE responses in at least 3 out of 4 tested frequencies.
Autoinflation
All children received the same pressure, with the autoinflation device delivering a pressure of 20 kPa. During the procedure, the child holds a sip of water in their mouth. The silicone treatment tip of the device is placed against one nostril while the other nostril is occluded by pinching. After pressing the activation button, airflow is introduced into the nasal cavity for approximately 3 seconds. While the device is operating, the child swallows the water, allowing airflow to enter the middle ear. After a 5-minute rest, the process is repeated once. Treatment was performed twice daily, in the morning and evening, for 6 to 8 consecutive weeks. If an upper respiratory tract infection occurred during therapy, autoinflation was paused and resumed only after the infection had resolved. All children continued autoinflation therapy until the affected ear was cured, with a maximum treatment duration not exceeding the follow-up period of 3 months.
Follow-Up and Criteria For Evaluating Efficacy
All patients were followed up in the outpatient clinic once a month for the first, second, and third months of treatment, with relevant audiological assessments completed at each visit. The cure rate was calculated as: Cure/Total × 100%, and the improvement rate was calculated as: Improvement/Total × 100%. (1) Cure: Normalization was defined as conversion from a Type B or C2 tympanogram to a Type C1 or Type A tympanogram. (2) Improvement: Improvement (but not normalization) in tympanometric findings was defined as conversion from a Type B to a Type C2 tympanogram. (3) Ineffective: Children with no change or deterioration in tympanometric findings were defined as non-responders, while those with normalization or improvement were defined as responders.
Statistical Analysis
Data analysis was performed using SPSS 20.0 software (IMB company, USA). Continuous data were presented as median and interquartile range (IQR). Comparisons between 2 groups were performed using the Mann–Whitney U test, while comparisons among 3 groups were conducted using the Kruskal–Wallis H test. For children with persistent OME, the outcomes of autoinflation treatment were categorized into 3 groups: no improvement, improvement, and cure. Categorical data were described using frequency and percentage, and group comparisons were performed using the chi-square test or Fisher’s exact test, as appropriate. Using these 3 treatment outcomes as the dependent variable, and gender, age, presence of recurrent OME, adenoid hypertrophy, and repeated respiratory tract infections as independent variables, a multinomial logistic regression analysis was conducted to identify factors influencing the outcomes of autoinflation treatment. A P-value <.05 was considered statistically significant.
Results
Patient Characteristics
This study included 71 children with persistent OME who had not undergone surgery for various reasons, including unwillingness to undergo surgery and waiting for surgical bed availability. A total of 60 controls were included in this study. All children experienced varying degrees of ear discomfort, including stuffiness, pain, and/or hearing loss. The course of OME in all children exceeded 3 months. The general information of the 2 groups is presented in Table 1. In the autoinflation group (n = 71), 38 children were diagnosed with OME for the first time, 33 had recurrent OME, and 12 had previous surgery (adenoidectomy with tympanostomy tube insertion). In the control group (n = 60), 29 children were diagnosed with OME for the first time, 31 had recurrent OME, and 14 had previous surgery (adenoidectomy with tympanostomy tube insertion). Their general information, including age, gender, number of OME ears, types of otoacoustic emissions, disease course, OME recurrence, and history of previous OME surgery, was compared between groups, and the results showed no significant difference (P > .05).
Comparisons of General Information Between Patients and Controls.
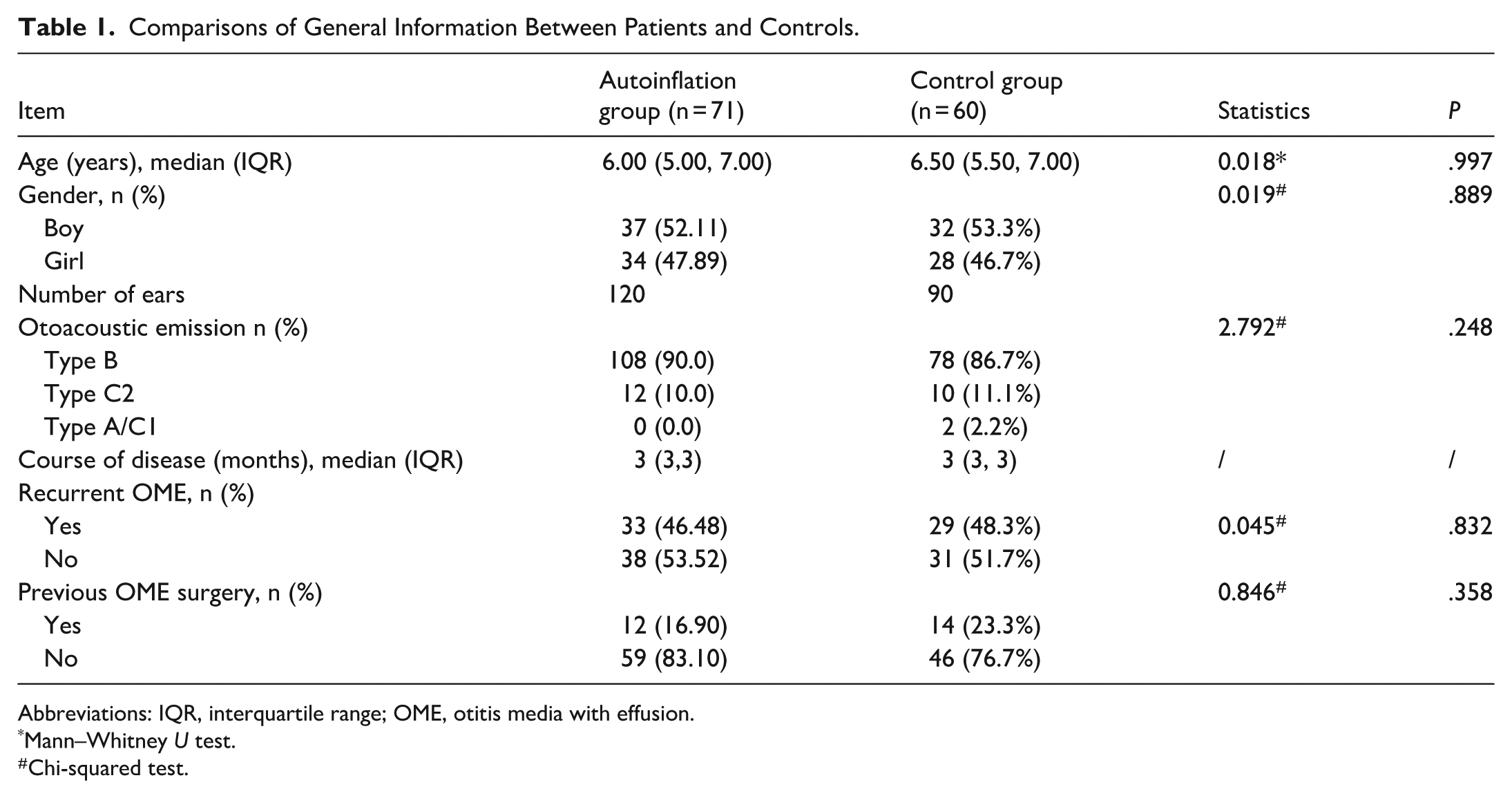
Abbreviations: IQR, interquartile range; OME, otitis media with effusion.
Mann–Whitney U test.
Chi-squared test.
Efficacy of Autoinflation Treatment in Children With Persistent OME
Before autoinflation, 108 ears were classified as Type B and 12 ears as Type C2, and all DPOAE results were recorded as refer. Before autoinflation, 108 ears were Type B and 12 ears were Type C2, and all of DPOAE showed refer results. After 1 month of autoinflation, 21.7% and 25.0% of ears were cured and improved, respectively. After 2 months of autoinflation, 48.3% and 20.0% of ears were cured and improved, respectively. After 3 months of autoinflation, 60.8% and 13.3% of ears were cured and improved, respectively. However, in the control group, after 3 months of medical treatment, only 20.0% and 20.0% of ears were cured and improved, respectively (Tables 2 and 3).
The Effective Rate and Audiological Examinations Pre- and Post-Autoinflation (1, 2, and 3 Months) of the Autoinflation Group.

Abbreviation: DPOAE, Distortion Product Otoacoustic Emission.
The Effective Rate and Audiological Examinations Pre- and Post-Treatment (1, 2, and 3 Months) of the Control Group.
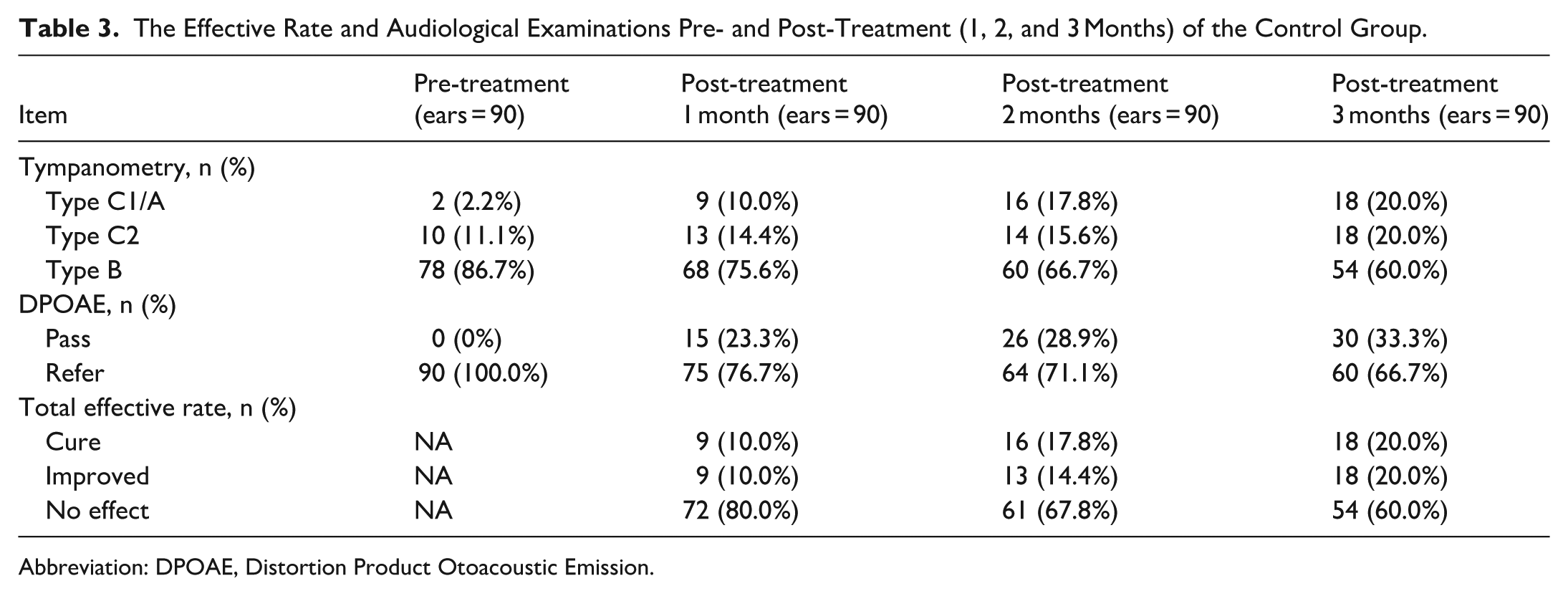
Abbreviation: DPOAE, Distortion Product Otoacoustic Emission.
Univariate and Multinomial Logistic Regression Analysis of Failed Autoinflation in Children With Persistent OME
The possible causes of autoinflation treatment failure were explored in these cases. As shown in Table 4, univariate analysis indicated that recurrent OME and repeated respiratory tract infections were significant risk factors for treatment outcomes (P < .05). Based on clinical considerations, all variables included in the univariate analysis were entered into the multinomial logistic regression model to identify factors influencing treatment outcomes of autoinflation in children with persistent OME. As shown in Table 5, the analysis revealed that recurrent OME (OR [95% CI]: 10.285 [2.649-39.924], P = .001) and repeated respiratory tract infections (OR [95% CI]: 18.510 [5.006-68.436], P < .001) were independent risk factors for unfavorable outcomes. Specifically, children with recurrent OME were 10.285 times more likely to experience poor treatment outcomes compared with those without recurrent OME, whereas those with repeated respiratory tract infections were 18.510 times more likely to have an unfavorable response to autoinflation.
Univariate Analysis of Treatment Outcomes of Autoinflation For Children With Persistent OME.

Abbreviation: OME, otitis media with effusion.
Kruskal–Wallis H.
Chi-squared test.
Multinomial Logistic Regression Analysis For the Factors Influencing the Outcomes of Autoinflation For Children With Persistent OME.

Abbreviation: OME, otitis media with effusion.
P < .05.
Safety
Half of the children experienced ear pain within the first week of treatment, but it was tolerable, and no other discomfort was reported. Twenty children experienced worsening sinusitis with increased purulent nasal discharge during autoinflation. Autoinflation was paused in these cases and resumed once the nasal discharge had decreased.
Discussion
Autoinflation is a noninvasive treatment that can significantly improve symptoms of OME, especially in patients with a short disease duration and mild symptoms. This study aims to explore whether an electronic autoinflation device is effective in children with persistent OME (>3 months). In 1999, Silman et al 15 developed the first electronic autoinflation device, which is compact, handheld, and suitable for home use. It works by applying continuous positive pressure to the nasal cavity and nasopharynx to open the Eustachian tube. In 2000, his team used this device to treat 20 children with OME twice weekly for 6 weeks. The results showed that 70% of the treatment group achieved normalization of the air-bone gap, compared with only 20% in the control group. 16 In 2005, Arick et al conducted a randomized controlled trial using this device for OME. 17 Children aged 4 to 11 years underwent a 7-week treatment. For children under 7 years old, the initial pressure was set at 2.5 psi for the first week and increased to 5.2 psi once they adapted. For children aged 7 years and older, the pressure was set at 5.2 psi from the start. At the end of the trial, the treatment group showed greater improvements in air-bone gap, tympanic peak pressure, and tympanic membrane mobility (observed via otoscopy) compared with the control group. 18 In 2009, another electronic device, EarPopper™, was introduced. Its design, size, working principle, and usage are similar to those of the previous device. A 2015 trial (n = 29, aged 4-11) found that 7 weeks of EarPopper™ use significantly improved air-conduction thresholds (10.9 vs 3.6 dBHL) and reduced tympanostomy tube insertion (53.3% vs 78.6%) over a mean 47.7-month follow-up. 19 However, the treatment frequency in these studies was relatively conservative, with only 1 to 2 sessions per week; increasing the frequency of use may enhance therapeutic efficacy.
OME has a high spontaneous resolution rate at 3 months. 20 Many national OME guidelines recommend a 3-month observation period for children without high-risk factors. For first-time OME cases, treatment is generally not difficult. The real challenge lies in managing OME lasting more than 3 months and recurrent OME. When both conditions are present, especially in the presence of additional high-risk factors, such as young age, recurrent/prolonged respiratory tract infections, and adenoid hypertrophy, treatment becomes much more complicated. This is the issue our study aims to explore.
In this study, we first analyzed children with persistent OME. A total of 71 children aged 4 to 13 years were included in the autoinflation group. While treating high-risk factors (such as rhinitis, sinusitis, and adenoid hypertrophy), an electronic autoinflation device was added to the treatment regimen. The device was used twice daily for 1 to 3 months. After a 3-month follow-up, 60.8% and 13.3% of ears were cured and improved, respectively. Children who were not fully cured were recommended for surgery. This cure rate is consistent with previous studies.6,21 Our study demonstrated a markedly higher cure rate in the autoinflation group (60.8%) than in the control group (20.0%). This finding is consistent with a previous study, 14 which showed that 52% of children with persistent OME in the autoinflation group achieved normal middle ear pressure, compared with 15% in the control group, with a statistically significant difference (P < .001). Based on our findings and previous studies, we believe that approximately half of children with persistent OME may avoid surgery in the short term by using an electronic autoinflation device. However, its long-term effectiveness remains unclear and requires further investigation. Moreover, it should be acknowledged that children with persistent OME required a longer duration of autoinflation therapy than those without persistent disease, likely because middle ear effusion gradually develops into glue ear over time, which is more difficult to resolve.
Given the relatively small sample size, we selected only 5 risk factors for univariate analysis. The results indicated that recurrent OME and recurrent respiratory tract infections were high-risk factors for autoinflation treatment failure. First, among the 33 cases of recurrent OME included in this study, 10 children had previously undergone OME surgery, including one child who had received tympanostomy tube insertion 3 times. Recurrent OME is often associated with multiple high-risk factors, such as younger age, recurrent respiratory tract infections, adenoid hypertrophy, rhinitis, and poor mastoid pneumatization.22,23 Particularly in children with recurrence after tympanostomy tube insertion, multiple high-risk factors often coexist. These factors interact and collectively influence the effectiveness of autoinflation therapy. Second, possible reasons why recurrent or prolonged respiratory tract infections reduce the efficacy of autoinflation may include: (1) when nasal secretions are abundant, improper operation may push these secretions into the middle ear cavity, aggravating the condition; and (2) when purulent nasal secretions are present, parents are advised to temporarily suspend autoinflation. In this study, many of the enrolled children were younger and had weaker immunity, leading to repeated respiratory tract infections, which may explain their poorer response to autoinflation therapy. Third, our study found that adenoid size did not affect the efficacy of autoinflation therapy; as long as purulent nasal secretions were absent and the child was cooperative, autoinflation could be performed. In addition, treatment efficacy was not associated with age or sex. In summary, for children with recurrent persistent OME, especially those with a history of surgical treatment and those with recurrent respiratory tract infections, autoinflation is not recommended, and surgical intervention should be considered instead. However, given the small sample size, these findings should be interpreted with caution.
Autoinflation is generally considered safe; however, rare complications have been reported. For example, epidural emphysema has been described following a forceful Valsalva maneuver. Other reported complications include orbital swelling and intracranial air. Importantly, these cases typically involved patients with predisposing conditions, such as a history of mastoidectomy, orbital tumors, or craniotomy.24,25 In our study, approximately half of the patients experienced ear pain at the initiation of treatment, but the discomfort was mild and tolerable. For children with significant nasal discharge, it is recommended to first treat sinusitis and reassess the middle ear condition. If OME persists, autoinflation can then be initiated. Children over 4 years of age generally demonstrate good cooperation and compliance with the procedure. However, the relatively high cost of the electronic autoinflation device remains a limitation, particularly in low-income and underdeveloped regions, restricting its widespread clinical application.
This study has some limitations: (1) As a retrospective study, it may have selection bias and unmeasured confounding. Treatment was not randomized. Notably, most children in the control group declined autoinflation due to financial reasons, which introduces a specific source of selection bias that should be acknowledged. Additionally, group differences in socioeconomic status or health behaviors may have overestimated efficacy. (2) Although the sample size of this study met the basic requirements for multivariate analysis, the relatively limited sample size may still constrain the power to detect other potential risk factors (such as adenoid hypertrophy, P = .211). Future studies with larger sample sizes are warranted to validate our findings. Furthermore, the subgroup and regression analyses presented in this study should be considered exploratory and interpreted with caution due to the limited sample size. (3) Outcome assessment relied on tympanometry and DPOAE without systematic pure-tone audiometry, as some children could not complete behavioral testing, so hearing threshold improvement could not be evaluated. (4) Follow-up was only 3 months, so long-term recurrence was not assessed. This is a significant limitation because recurrence is common in OME and even after tube extrusion. Whether recurrence rates differ between autoinflation and surgery remains unknown. (5) Mastoid pneumatization patterns (pneumatized, diploic, or sclerotic types) may affect middle ear ventilation; however, due to the lack of routine temporal bone CT imaging and substantial missing data, this variable could not be analyzed. (6) The study population consisted of children older than 4 years from tertiary pediatric centers, and all received the same electronic autoinflation device. Therefore, the generalizability of these findings to younger children, primary care settings, or regions with limited access to electronic devices may be restricted. Taken together, these limitations suggest that while our findings support autoinflation as a promising non-surgical option for selected children with persistent OME, the results should be interpreted cautiously.
Conclusion
Autoinflation provides a safe and effective treatment option for more than half of children with persistent OME. However, treatment failure is more likely in children with recurrent or prolonged upper and lower respiratory tract infections, as well as in those with recurrent OME, particularly with a history of middle ear surgery (adenoidectomy with tympanostomy tube insertion). While autoinflation represents a low-risk alternative to surgery in appropriately selected patients, it should be avoided in specific populations, including children with skull base or orbital defects, craniofacial anomalies, or active infection or inflammation.
Footnotes
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the 2021 Shanghai Science and Technology Innovation Action Plan–Medical Innovation Research Special Project (21Y31900500).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The data are available from the corresponding author* on reasonable request.