
Abstract
Importance
To our knowledge, this represents the first adult-only, fully endoscopic, three-arm comparative cohort of autograft, allograft, and xenograft materials in type I tympanoplasty.
Objective
To compare graft-take, audiometric outcomes, operative time, and complications among perichondrium, MegaDerm, and Biodesign in adult endoscopic type I tympanoplasty.
Design:
Retrospective comparative cohort study.
Setting:
Tertiary referral center.
Participants:
Adults who underwent endoscopic type I tympanoplasty with perichondrium, MegaDerm or Biodesign between October 2021 and March 2025. Patients with revision surgery, concomitant otologic procedures, active middle-ear disease, profound sensorineural hearing loss, preoperative air-bone gap (ABG) ≥50 dB, or follow-up <3 months were excluded.
Intervention or Exposures
Endoscopic type I tympanoplasty using perichondrium (autograft), MegaDerm (allograft), or Biodesign (xenograft).
Main Outcome Measures:
Graft-take rate, hearing gain (air-conduction and ABG), operative time, and complications.
Results
Ninety-three ears were analyzed (perichondrium n = 33; MegaDerm n = 21; Biodesign n = 39). Three-month graft-take rates were similar, and final graft-take rates remained comparable across groups (3 months: 90.9%, 90.5%, 94.9%; P = .6862; final: 84.8%, 85.7%, 84.6%; P > .999). Air-conduction (AC) and ABG improved significantly within all groups. Between-group differences were not significant for AC gain (13.79 ± 9.84 vs 7.24 ± 12.46 vs 9.14 ± 10.01 dB; P = .0804) or ABG gain (9.58 ± 10.46 vs 8.82 ± 10.37 vs 7.58 ± 8.46 dB; P = .7757); the proportion achieving postoperative ABG ≤20 dB was similar (P = .475). Operative time was significantly longer for perichondrium (98.23 ± 32.35, 68.52 ± 20.84, and 74.88 ± 17.27; P < .0001). Complications were infrequent (otomycosis, n = 3; myringitis, n = 1), and no facial palsy, intractable vertigo, profound sensorineural hearing loss(SNHL), or dysgeusia occurred.
Conclusion:
In adult endoscopic type I tympanoplasty, perichondrium, MegaDerm, and Biodesign demonstrated comparable short-term graft-take and audiometric outcomes, while commercially available grafts were associated with shorter operative time.
Relevance:
These findings support patient-centered graft selection balancing donor-site considerations, operative efficiency, and cost; prospective studies with standardized follow-up and patient-reported outcomes are warranted.
This is a visual representation of the abstract.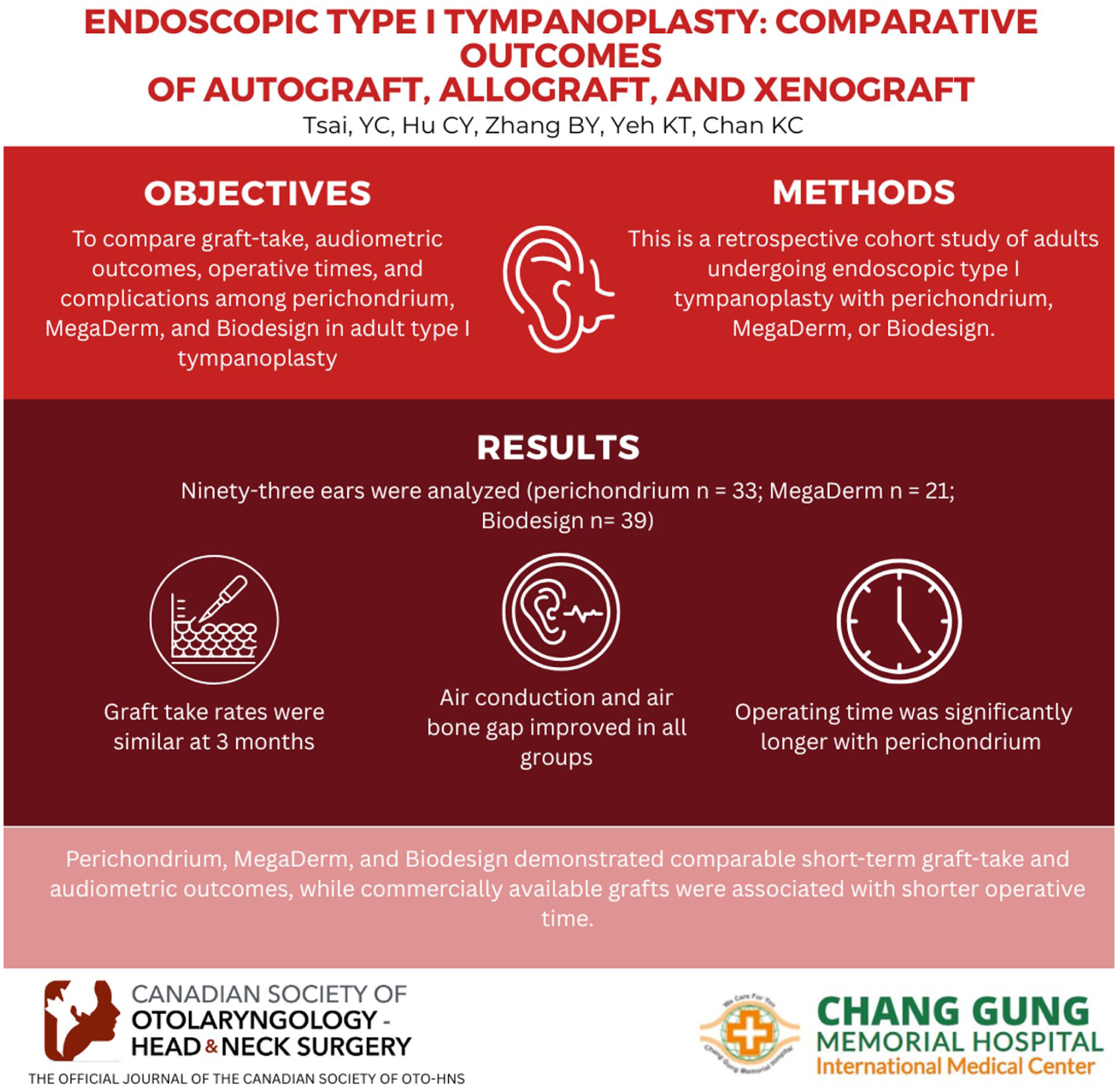
Keywords
Key Message
In an adult-only, fully endoscopic, three-arm cohort, perichondrium, MegaDerm, and Biodesign achieved comparable graft-take and hearing outcomes at short-term follow-up.
Commercially available allograft/xenograft materials were associated with shorter operative time compared with autologous perichondrium.
These data inform shared decision-making by quantifying trade-offs among donor-site morbidity, operative efficiency, and cost, while highlighting the need for longer-term follow-up and patient-reported outcomes.
Introduction
Chronic otitis media (COM) with persistent tympanic membrane (TM) perforation is a clinical condition that often requires surgical repair. Tympanoplasty aims to restore TM integrity and improve hearing. Autologous grafts—such as cartilage, perichondrium, and temporalis fascia—are commonly used materials offering high graft-take rates with favorable hearing outcomes. 1 Previous cohort studies and meta-analyses have explored outcomes among various autologous graft types.2-7
In recent years, biologic scaffold materials—including allogeneic and xenogeneic extracellular matrix materials—have gained attention as practical alternatives. These materials undergo decellularization to remove cellular components while preserving matrix structures (eg, preserving collagen, elastin, and bioactive constituents). Further antigen removal and sterilization are performed to ensure biocompatibility and safety.8-14
Commercially available options, such as MegaDerm (L&C Bio Co., Seongnam-si, Republic of Korea)—a sterile, acellular human dermal matrix—and Biodesign (Cook Medical, Bloomington, IN, USA)—derived from porcine small intestinal submucosa (SIS)—offer ready-to-use materials that avoid donor-site morbidity. Both have demonstrated graft-take rates and hearing outcomes comparable to autologous materials in multiple clinical cohorts and meta-analyses.9,11-19
However, most studies remain limited to 2-arm comparisons and often mix endoscopic and microscopic approaches and/or include heterogeneous populations (eg, pediatric or revision cases). Only a few studies include 3 arms, yet none has simultaneously evaluated autograft, allograft, and xenograft under a standardized endoscopic protocol. For example, Vos et al 12 compared AlloDerm (LifeCell Corp., Branchburg, NJ, USA), cartilage-with-fascia, and fascia alone, reporting comparable graft-take rate and air-bone gap (ABG) closure. A direct head-to-head comparison of all 3 graft categories under uniform surgical conditions remains lacking.
Accordingly, we evaluated whether graft material (autologous-perichondrium, allogeneic-MegaDerm, and xenogeneic-Biodesign) affects graft-take and hearing outcomes in adults undergoing endoscopic type I tympanoplasty and compared operative time across materials. Given evidence that a fully endoscopic approach yields outcomes comparable to microscopic surgery while reducing postoperative discomfort and facilitating recovery,20-23 all surgeries in our cohort were performed endoscopically under a standardized protocol. We hypothesized similar graft-take and hearing outcomes, shorter operative time with commercially available grafts, and infrequent complications.
Material and Methods
Ethical Considerations
This retrospective comparative cohort study was approved by the Chang Gung Medical Foundation Institutional Review Board (IRB No. 202501369B0), which waived the requirement for informed consent.
Patient Selection
This retrospective cohort included adults (≥18 years) who underwent endoscopic type I tympanoplasty at Chang Gung Memorial Hospital, Linkou, Taiwan, between October 2021 and March 2025. All procedures were performed by 2 experienced otologists. Demographic and baseline clinical characteristics were retrieved from medical records. Postoperative complications were also reviewed. Eligible patients were adults (≥18 years) with COM and a TM perforation persisting for at least 3 months with a dry ear for a minimum of 1 month prior to surgery. Exclusion criteria included inadequate follow-up (<3 months), concurrent otologic procedures, revision tympanoplasty, active middle-ear disease, profound SNHL, and a preoperative ABG ≥50 dB.
Graft Selection and Graft Materials
At the outpatient visit, surgeons introduced all available graft options. Counseling covered expected graft-take, donor-site harvest and morbidity, anticipated difference in operative time, material-specific considerations, and cost. Patients could seek further consultation and finalize their decision any time before surgery. No protocol-driven preference was applied. Patients enrolled received 1 of the 3 materials for type I tympanoplasty: (1) autograft-ipsilateral tragal perichondrium (33 ears); (2) allograft-MegaDerm (21 ears); or (3) xenograft-Biodesign (39 ears).
Surgical Technique
All surgeries were performed under general anesthesia. Following irrigation of the external auditory canal (EAC) with povidone-iodine and saline, the TM and ossicular chain were inspected endoscopically to exclude middle-ear disease. In the autologous group, tragal perichondrium was harvested first. The perforation edges were carefully de-epithelialized as needed. A circumferential canal incision was then made, allowing elevation of the tympanomeatal flap along with annulus to access the middle ear. Gelfoam pledgets were placed in the mesotympanum. The graft was positioned medial to the residual drum remnant and lateral to malleus manubrium. The tympanomeatal flap was subsequently repositioned over the graft and adjusted to ensure optimal placement. Additional Gelfoam was placed around the graft margin, and the EAC was loosely packed. Operative time was defined as the interval from initial canal preparation to final packing of the EAC.
Audiometric Assessment
Audiometric analyses followed the 1995 American Academy of Otolaryngology–Head and Neck Surgery (AAO-HNS) Committee on Hearing and Equilibrium consensus guidelines. 24 Pre- and postoperative air-conduction (AC) and bone-conduction (BC) thresholds at 0.5, 1, 2, and 4 kHz were extracted, and the corresponding ABGs were calculated. In addition, high-frequency BC threshold averages (1, 2, and 4 kHz) were calculated at both time points to screen for potential iatrogenic postoperative SNHL. Audiometric evaluations were obtained by audiologists blinded to graft type.
Postoperative Graft Evaluations
EAC packing was removed at 2 weeks postoperatively. Graft status was assessed endoscopically at follow-up visits; graft-take was defined as a fully epithelialized TM without perforation or lateralization. Only patients with ≥3 months of postoperative follow-up time were collected.
Statistical Analysis
Statistical analyses were conducted using GraphPad Prism, version 10.6.1 (GraphPad Software, San Diego, CA, USA). Continuous variables are reported as mean ± standard deviation (SD). Normality of distribution was assessed using the Shapiro–Wilk test. Between-group comparisons used one-way ANOVA or the non-parametric Kruskal–Wallis test as appropriate. Categorical variables were compared using Pearson’s chi-square test (if all expected counts ≥5) or Fisher’s exact test. Pre- versus postoperative audiometric thresholds were compared using paired t-tests or Wilcoxon signed-rank tests. All tests were two-tailed with P < .05 considered significant.
Because postoperative interval audiometry test was not regularly performed for all patients, paired audiometric analyses were restricted to ears with both pre- and postoperative audiograms; potential ascertainment bias was assessed by graft-take rates in ears with versus without postoperative audiometry within each group using Fisher’s exact test. A multivariable logistic regression was performed to evaluate whether graft type was independently associated with graft-take after adjustment for relevant covariates. Besides, to account for intra-patient correlation in bilateral cases, a 1-ear-per-patient sensitivity analysis was performed using a prespecified outcome-independent selection rule (left ear for odd medical record numbers; right ear for even).
Results
Baseline Characteristics
Baseline clinical characteristics are summarized in Table 1. We analyzed 93 adult ears (perichondrium, n = 33; MegaDerm, n = 21; Biodesign, n = 39). Median age ranged from 56.0 to 60.9 years across groups. The male-to-female distribution was 12/21, 6/15, and 15/24, respectively. Smoking was more common in the perichondrium group (18.2%), while hypertension and diabetes mellitus (DM) were infrequent across cohorts. Laterality was 12 right/21 left (perichondrium), 12 right/9 left (MegaDerm), and 19 right/20 left (Biodesign). Perforation size, categorized as small (≤25%) + medium (25%-50%) versus large (≥50%), was 26/7, 13/8, and 28/11, respectively. No statistically significant between-group differences were observed in age, sex, perforation size, laterality, smoking status, DM, hypertension (all P > .05).
Demographic and baseline audiometric characteristics of patients.
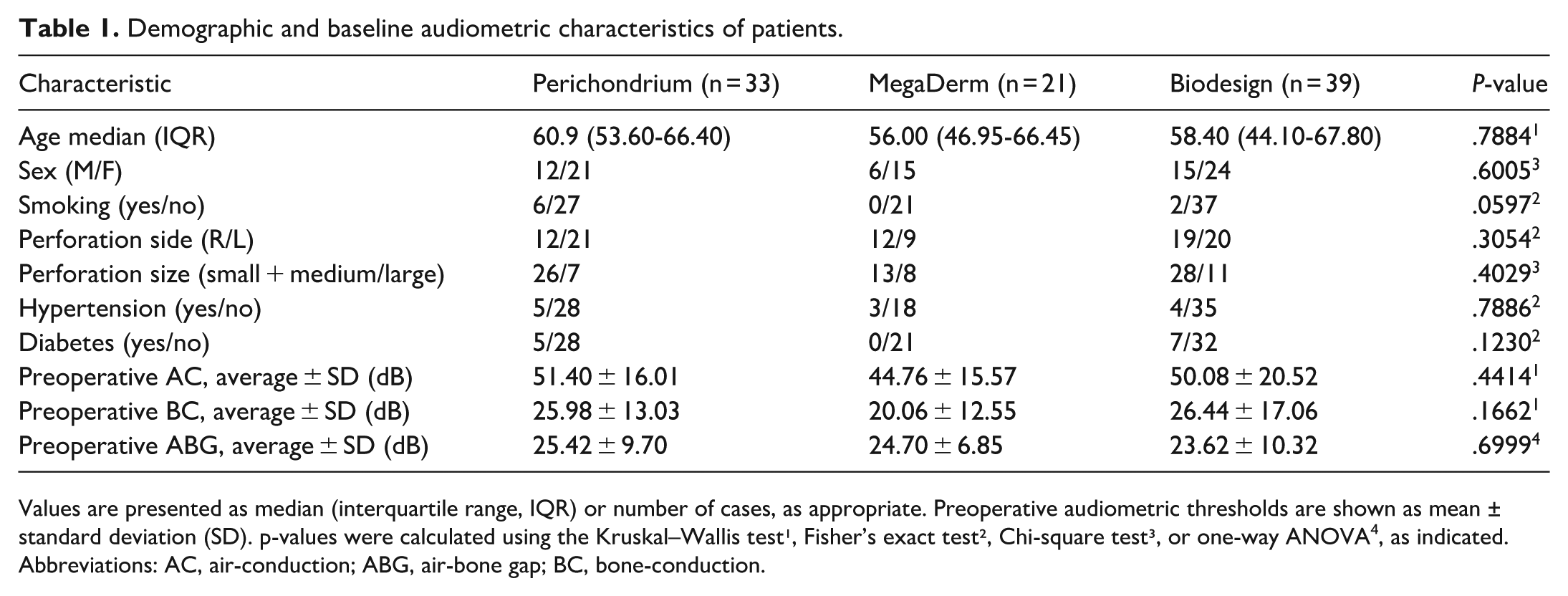
Values are presented as median (interquartile range, IQR) or number of cases, as appropriate. Preoperative audiometric thresholds are shown as mean ± standard deviation (SD). p-values were calculated using the Kruskal–Wallis test¹, Fisher’s exact test², Chi-square test³, or one-way ANOVA⁴, as indicated. Abbreviations: AC, air-conduction; ABG, air-bone gap; BC, bone-conduction.
Mean preoperative AC thresholds were 51.40 ± 16.01, 44.76 ± 15.57, and 50.08 ± 20.52 dB for perichondrium, MegaDerm, and Biodesign, respectively. Corresponding BC thresholds were 25.98 ± 13.03, 20.06 ± 12.55, and 26.44 ± 17.06 dB, yielding ABGs of 25.42 ± 9.70, 24.70 ± 6.85, and 23.62 ± 10.32 dB; these measures were comparable among groups (all P > .05).
Surgical Outcomes
Graft-take rates at 3 months were similar across groups: 90.90% (30/33) for perichondrium, 90.48% (19/21) for MegaDerm, and 94.87% (37/39) for Biodesign (P = .6862). Additional failures occurring between postoperative 3 to 6 months reducing final graft-take rate to be 84.8% (28/33), 85.7% (18/21), and 84.6% (33/39), respectively (P > .999). All 14 failures occurred within 6-month postoperatively. The earliest failure was detected at postoperative week 2 in the Biodesign group; additional failures were detected at 1 month (2 cases in perichondrium group) and 2 months (n = 1 perichondrium, n = 2 MegaDerm, n = 1 Biodesign), with the remaining cases occurring between 3 and 6 months after surgery. Among failure cases, 5 were managed with observation according to patients’ preference, whereas 9 ears underwent revision tympanoplasty. Revision achieved successful closure in all but 1 ear, which experienced re-perforation after cartilage graft following an initial perichondrium repair.
Operation time differed significantly (one-way ANOVA, P < .0001): 98.23 ± 32.35 minutes (perichondrium), 68.52 ± 20.84 minutes (MegaDerm), and 74.88 ± 17.27 minutes (Biodesign), as shown in Table 2. Post hoc Tukey’s test revealed longer operative time with perichondrium than MegaDerm (MD: 29.72 minutes; 95% CI, 13.50-45.93; P < .0001) and Biodesign (MD: 23.35 minutes; 95% CI, 9.607-37.09; P = .0003). No significant difference was found between the MegaDerm and Biodesign groups (MD: −6.37 minutes; 95% CI, −22.09 to 9.359; P = .6009).
Graft-take rate and operative time by graft type.
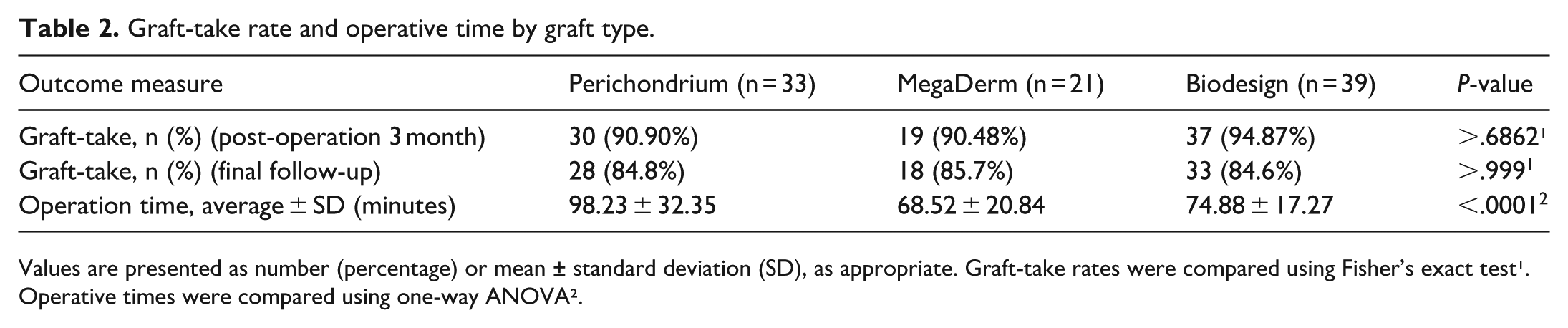
Values are presented as number (percentage) or mean ± standard deviation (SD), as appropriate. Graft-take rates were compared using Fisher’s exact test¹. Operative times were compared using one-way ANOVA².
Follow-Up Duration
Postoperative follow-up duration was variable. All patients were followed at least for 3 months postoperatively. The proportions of ears with ≥6 months follow-up were 16/33 (48.5%), 12/21 (57.1%), and 18/39 (46.2%) for perichondrium, MegaDerm, and Biodesign, respectively. The corresponding proportions with ≥12 months follow-up were 8/33 (24.2%), 6/21 (28.6%), and 9/39 (23.1%).
Adjusted Analysis of Surgical Outcomes
Multivariable logistic regression included graft type (with perichondrium as the reference), perforation laterality, perforation size, and preoperative ABG. DM, hypertension, and smoking were evaluated descriptively but excluded from the adjusted model due to low prevalence and sparse event counts, which could increase the risk of sparse-data bias.
After adjustment, no statistically significant association was observed. Compared with perichondrium, MegaDerm (adjusted odds ratio [OR] 1.92, 95% confidence interval [CI] 0.36-12.33) and Biodesign (adjusted OR 1.35, 95% CI 0.32-5.67) demonstrated no significant differences in graft-take rate. Perforation size and preoperative ABG were not independently associated with graft-take (small + medium vs large perforation: adjusted OR 1.87, 95% CI 0.43-8.09; preoperative ABG: adjusted OR 1.04 per 1-dB increase, 95% CI 0.97-1.12).
Sensitivity Analysis Accounting for Intra-Patient Correlation
Fourteen patients contributed bilateral ears (perichondrium 7; MegaDerm 5; Biodesign 2); therefore, a 1-ear-per-patient sensitivity analysis was performed to account for intra-patient correlation. After selecting 1 ear per patient using the prespecified outcome-independent rule described above, graft type remained not independently associated with graft-take (MegaDerm vs perichondrium: adjusted OR 1.78, 95% CI 0.32-12.05; Biodesign vs perichondrium: adjusted OR 1.55, 95% CI 0.36-6.76).
Audiometric Outcomes
Within-group analyses demonstrated significant postoperative improvements in AC thresholds (perichondrium: P < .0001; MegaDerm: P = .0296; Biodesign: P = .0006; Table 3) and ABG (perichondrium: P < .0001; MegaDerm: P = .0016; Biodesign: P = .0010; Table 3) for all graft types. Between-group comparisons showed no difference in AC gain (13.79 ± 9.84, 7.24 ± 12.46, 9.14 ± 10.01 dB (P = .0804)) or ABG gain (9.58 ± 10.46, 8.82 ± 10.37, 7.58 ± 8.46 (P = .7757)), as shown in Table 4 and Figure 1. The proportion of ears achieving postoperative ABG ≤20 dB did not differ among groups (P = .475; Table 4). Individual changes are visualized in Glasgow plots (Figure 2).
Within-group comparison of pre- and postoperative audiometric thresholds by graft type.
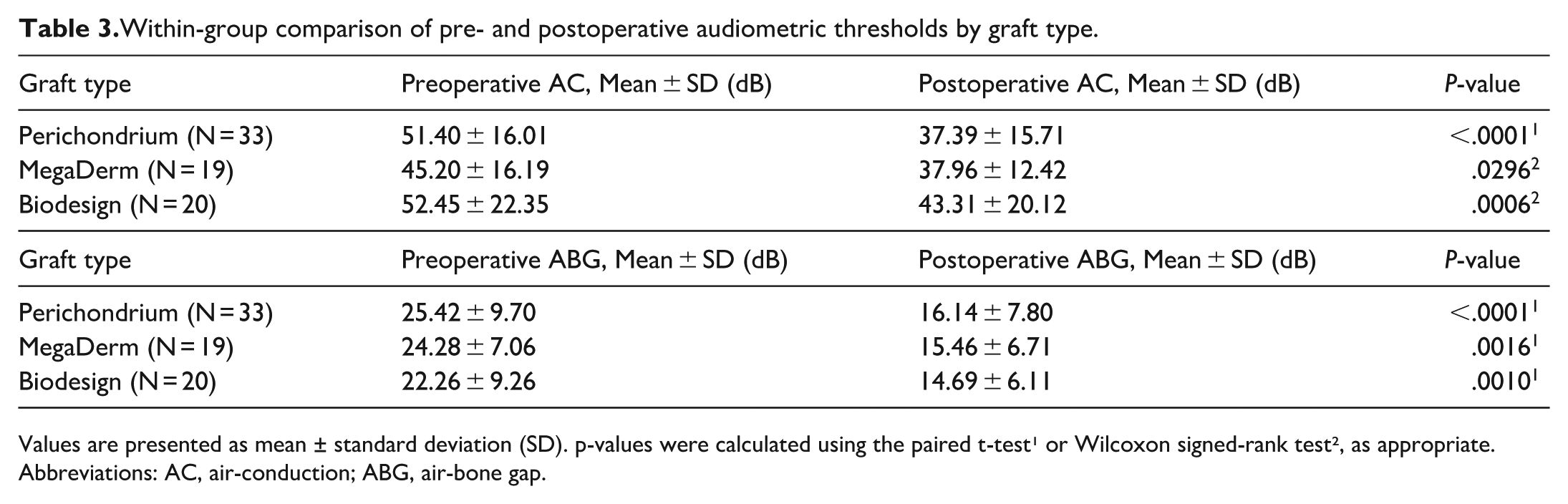
Values are presented as mean ± standard deviation (SD). p-values were calculated using the paired t-test¹ or Wilcoxon signed-rank test², as appropriate. Abbreviations: AC, air-conduction; ABG, air-bone gap.
Between-group comparison of postoperative hearing improvement across graft materials.
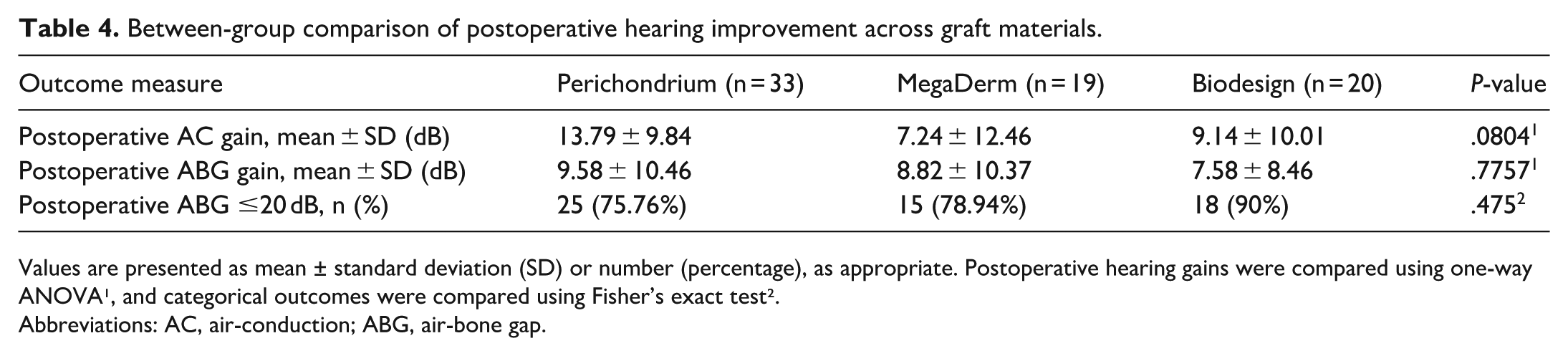
Values are presented as mean ± standard deviation (SD) or number (percentage), as appropriate. Postoperative hearing gains were compared using one-way ANOVA¹, and categorical outcomes were compared using Fisher’s exact test².
Abbreviations: AC, air-conduction; ABG, air-bone gap.
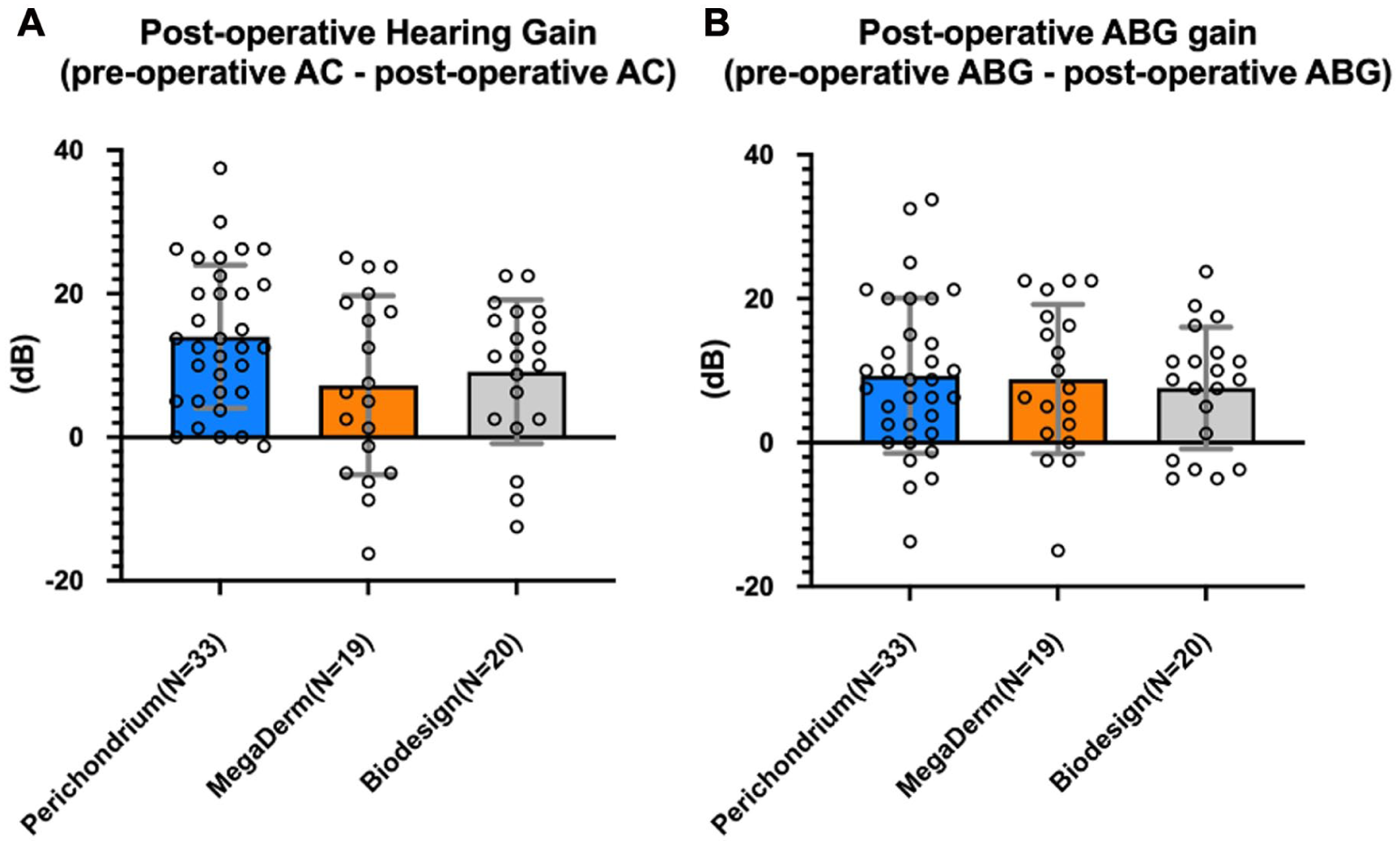
Postoperative hearing outcomes by graft type. (A) Air-conduction (AC) hearing gain calculated as preoperative minus postoperative AC pure-tone averages at 0.5, 1, 2, and 4 kHz. (B) Air-bone gap (ABG) gain calculated as preoperative minus postoperative ABG at the same frequencies. Bars represent mean ± standard deviation; overlaid points indicate individual ears. Positive values reflect improved hearing and ABG closure.

Glasgow plots comparing preoperative and postoperative air-conduction thresholds among graft groups. (A) Perichondrium group (n = 33), (B) MegaDerm group (n = 19), (C) Biodesign group (n = 20). Scatter of preoperative versus postoperative AC pure-tone average at 0.5, 1, 2, and 4 kHz. The red dashed line denotes the line of identity (y = x); points below the line indicate postoperative improvement (postoperative AC < preoperative AC). AC, air-conduction.
High-frequency BC (1, 2, and 4 kHz) changes are summarized in Table 5. The perichondrium group showed a small but significant improvement (27.73 ± 15.25 → 23.69 ± 15.76 dB; P = .0001). Changes in the MegaDerm (P = .4447) and Biodesign (P = .8501) groups were not significant.
Comparison of pre- and postoperative high-frequency bone conduction thresholds (1, 2, and 4kHz) for iatrogenic sensorineural hearing loss assessment.
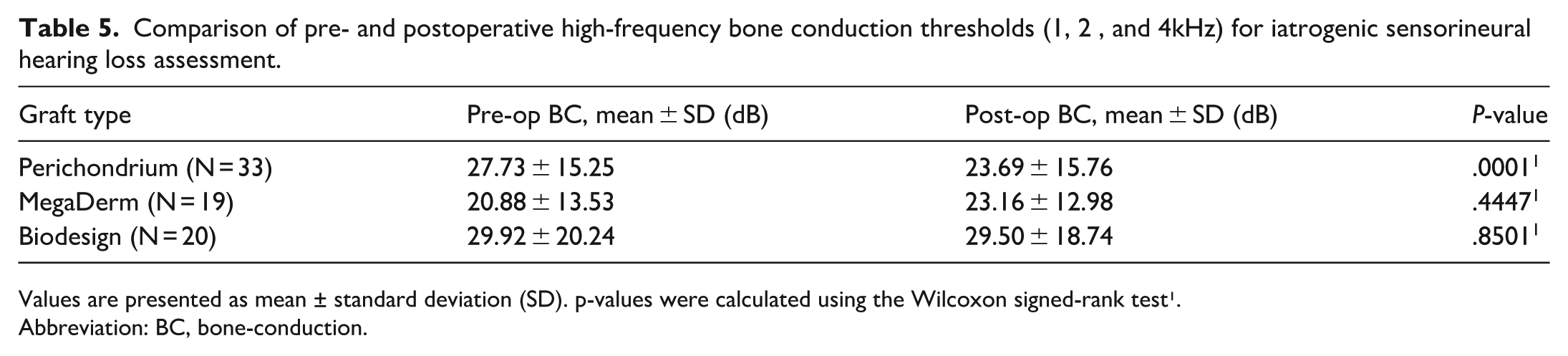
Values are presented as mean ± standard deviation (SD). p-values were calculated using the Wilcoxon signed-rank test¹.
Abbreviation: BC, bone-conduction.
Sensitivity Analysis for Audiometry Availability
All perichondrium graft cases had postoperative audiometry (33/33). Sensitivity test demonstrated no significant differences in graft-take rate between patients with and without postoperative audiometry. In the MegaDerm cohort, graft-take was 84.2% (16/19) with audiometry versus 100% (2/2) without (P > .99). In the Biodesign cohort, rate was 85.0% (17/20) with audiometry versus 84.2% (16/19) without (P > .99). When pooling allograft and xenograft cohorts, results remained similar (84.6%, [33/39] vs 85.7%, [18/21]; P > .99), suggesting that missing audiometric data did not materially bias graft-take outcomes.
Complications
Otomycosis occurred in 3 ears (perichondrium, n = 1; Biodesign, n = 2), and 1 Biodesign ear developed myringitis with otorrhea. No facial palsy, intractable vertigo, profound SNHL, or dysgeusia occurred during follow-up.
In the perichondrium group, otomycosis developed 4 weeks postoperatively and resolved within 2 weeks with topical antifungal therapy and aural toilet, without recurrence or subsequent perforation at 9.5 months of follow-up. In the Biodesign group, both otomycosis cases were managed conservatively as well. One ear had a residual perforation detected at postoperative week 2 and later underwent revision tympanoplasty with Biodesign after eradication of otomycosis 3 months later, achieving successful closure. The other developed otomycosis at 5 months postoperatively; infection resolved with local treatment, but a small, anterior perforation with an adhesive drum persisted, and the patient opted for observation.
One case of myringitis with otorrhea occurred in the Biodesign group at 5 months postoperatively. The patient, who had underlying DM and end-stage renal disease, had EAC flap swelling and discharge noted since postoperative month 2. The inflammation resolved with topical therapy; however, a persistent perforation remained and was later successfully repaired with cartilage tympanoplasty.
Discussion
This retrospective comparative cohort study evaluated perichondrium, MegaDerm, and Biodesign grafts in endoscopic type I tympanoplasty. Graft-take rates and hearing improvements were comparable across materials, whereas operative time was longer with perichondrium. Complications were uncommon and largely self-limited, with no cases of profound SNHL, intractable vertigo, facial palsy, or dysgeusia. To our knowledge, this represents the first adult-only, fully endoscopic three-arm comparative cohort with adjusted analysis.
To reduce selection-related bias, we restricted the cohort to adults with chronic, dry perforations and excluded active middle-ear disease, revision tympanoplasty, concurrent otologic procedures, profound SNHL, and severe preoperative hearing loss. Baseline characteristics and preoperative audiometry were similar across groups, and graft type remained unassociated with graft-take after multivariable adjustment and a 1-ear-per-patient sensitivity analysis, suggesting that measured covariates did not explain the comparable outcomes.
Although postoperative BC thresholds are not expected to improve after tympanoplasty, we observed no evidence of iatrogenic cochlear injury across graft types. Small BC changes reported after middle-ear surgery in prior studies25,26 may reflect improved middle-ear sound transmission rather than true cochlear recovery. TM repair can re-establish both the inertial-ossicular and external canal–osseotympanic components of BC transmission. The inertial-ossicular component, driven by the relative motion between the ossicular chain and skull, contributes most prominently around 1.5 to 2 kHz—the resonant frequency of the ossicles.26,27 When TM perforation or ossicular discontinuity is present, this pathway is compromised, leading to an apparent elevation of BC thresholds known as the Carhart effect. The external canal–osseotympanic component, meanwhile, relies on vibration-induced sound pressure within the ear canal that partially stimulates the TM and ossicular chain, particularly at lower frequencies below 1 kHz.26,27 Consistent with our findings, a retrospective study comparing dermal allograft and fat graft in endoscopic type I tympanoplasty reported significant postoperative BC improvement. 28 Another study using temporalis fascia demonstrated significant ABG improvement at low frequencies (0.25-1 kHz) but not at 4 kHz. 29 Similarly, in a cohort of 98 consecutive tympanoplasty patients, BC improvement occurred mainly at frequencies ≤2 kHz, with only one case showing improvement at 4 kHz. 30 Collectively, these results indicate that BC gains after tympanoplasty occur primarily at mid-to-low frequencies; however, frequency-specific analysis was beyond the scope of our study. The absence of statistically significant BC changes in the other 2 graft groups may reflect limited statistical power, as smaller subgroup sizes reduce the sensitivity to detect subtle effects. Taken together, these findings support the short-term safety and biocompatibility of all 3 materials.
Each graft type possesses distinct considerations. Auto-logous perichondrium provides excellent biocompatibility but requires donor-site harvest, which prolongs operative time and introduces potential wound-related morbidity. Human-derived allografts provide consistent, readily available material without donor-site morbidity and have shown histologically mild to absent inflammatory reactions comparable to autologous fascia. 31 Similarly, a systematic review and meta-analysis found no significant difference in complication rates between human-derived acellular dermal matrix (ADM) and autologous grafts, reporting only 2 cases of myringitis among 225 ADM tympanoplasty cases. 9 Xenogeneic grafts (eg, Biodesign) offer similar convenience; however, rare foreign-body or granulomatous reactions have been reported: MAUDE database review described histologically confirmed 5 cases of foreign-body and granulomatous reactions following the use of porcine SIS, occasionally accompanied by facial paralysis, profound SNHL, graft failure, or intractable vertigo requiring revision surgery. 32 These findings underscore the biologic plausibility that incomplete decellularization may provoke immune responses in susceptible individuals, leading to excessive inflammation, fibrosis, or graft failure. 8 Although such reactions are rare, the transient myringitis observed in our series highlights potential inter-individual variability in inflammatory response. Furthermore, the porcine origin xenografts may also be unacceptable to some patients for ethical, cultural, or religious reasons.
Graft-take rates exceeded 90% at 3 months across all graft types and remained comparable at final follow-up, with success rates of 84.8%, 85.7%, and 84.6% for perichondrium, MegaDerm, and Biodesign, respectively. Prior investigations comparing allografts with autografts9,11,12,15, as well as studies comparing xenografts with autografts14,18,19 reported no significant difference in graft-take or ABG closure. A systematic review reported an odds ratio of 0.71 (95% CI, 0.39-1.29; P = .26) when comparing ADM to autologous grafts, reinforcing clinical comparability. 9 However, much of the existing literature is limited by methodological heterogeneity-mixing endoscopic and microscopic techniques 12 and including revision cases 12 or pediatric patients,12,15 which may introduce confounding related to visualization differences, 33 instrumentation, and age-related Eustachian tube physiology. Pediatric patients are particularly prone to delayed failures due to adenoid and tonsillar hypertrophy.34,35 In contrast, concomitant adenoidectomy or tonsillectomy did not significantly affect graft-take rates or ABG improvements in adult cohorts. 36 Likewise, a recent study reported that concurrent Eustachian tuboplasty in patients aged ≥16 years did not alter long-term graft-take or audiologic outcomes. 37 These findings emphasize the importance of distinguishing pediatric patients from adult populations.
Beyond graft material and patient selection, the timing and mechanisms of graft failure are important when interpreting tympanoplasty outcomes. Early and late failures likely reflect different mechanisms. In our cohort, all failures occurred within 6 months, including events arising after an initially intact graft at 3 months. Early failure is typically related to related to infection38,39 or impaired graft vascularization, leading to necrosis or displacement before complete epithelialization. 40 Fungal infection may compromise graft viability through vascular thrombosis and avascular necrosis. 41 In contrast, late perforation—often defined as reperforation occurring beyond 3 to 12 months after confirmed graft take40,42,43—develops after a stable neotympanum has formed and is often associated with progressive graft atrophy,40,44 persistent Eustachian tube dysfunction with negative middle-ear pressure, or recurrent otitis media.43,45 In such settings, reperforation may reflect ongoing middle-ear or Eustachian tube disease rather than intrinsic graft failure. However, follow-up in our cohort was short and variable, and Eustachian tube function was not systematically assessed; therefore, durability beyond 6 months and the contribution of Eustachian tube-related mechanisms to delayed reperforation could not be determined.
Operative time varied by surgical approach, graft type, and procedural complexity. A meta-analysis 20 demonstrated significantly shorter operative times for endoscopic versus microscopic tympanoplasty, supporting the efficiency of the endoscopic approach (mean difference, 24.7 minutes; 95% CI, 38.6-10.9; P = .0005). In our study, perichondrium grafts required longer operative times than MegaDerm or Biodesign, reflecting the additional steps needed for graft harvesting and preparation. In contrast, allograft or xenograft procedures benefited from the convenience of ready-to-use graft materials with uniform thickness, which facilitated faster placement and reduced intraoperative handling. Prior reports similarly describe longer operative times with autografts than allografts (92.3 ± 16.5 vs 65.3 ± 20.5 minutes 10 ; 124 vs 82 minutes 12 ), and further time reductions have been reported when tympanomeatal flap elevation is avoided in selected technique (87.3 ± 5.1 minutes vs 48.6 ± 6.2 minutes, P < .05). 6 Thus, both graft selection and refinement of surgical technique contribute to reduced operative duration without compromising outcomes.
This study has limitations. The retrospective design, modest sample size, and limited failure events reduce precision. Follow-up was short and variable, potentially under detecting delayed reperforation, late complications, or durability differences among grafts. Graft selection was not randomized, and residual confounding from unmeasured factors (eg, middle-ear mucosal status, or Eustachian tube function) cannot be excluded despite adjustment. Given the observed event rate, the study may have been underpowered to detect small but clinically meaningful differences between graft materials. Patient-reported outcomes and formal cost-effectiveness analyses were not assessed. Larger prospective studies with standardized follow-up and comprehensive outcome measures are needed to confirm long-term outcomes.
Conclusion
In adult endoscopic type I tympanoplasty, perichondrium, MegaDerm, and Biodesign grafts demonstrated comparable graft-take and audiometric outcomes with low complication rates. Autologous perichondrium is cost-effective but carries potential donor-site morbidity, whereas allografts and xenografts may improve operative efficiency at higher material cost. Although retrospective design and limited follow-up warrant cautious interpretation, the absence of significant differences in surgical or hearing outcomes support patient-centered graft selection that balances donor-site considerations, operative efficiency, and financial factors to facilitate shared decision-making.
Footnotes
Acknowledgements
This work received no external funding. All authors take full responsibility for the integrity of the data and the accuracy of the analyses.
Ethical Considerations
This study was approved by Chang Gung Medical Foundation Institutional Review Board (IRB No. 202501369B0), which waived the requirement for patient’s informed consent.
Author Contributions
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets generated and/or analyzed during the current study are not publicly available due to institutional policy but are available from the corresponding author upon reasonable request.