
Abstract
Importance:
Sensorineural hearing loss (SNHL) accompanied by vertigo is a condition with clinical heterogeneity. Understanding vascular underpinnings is crucial for management.
Objective:
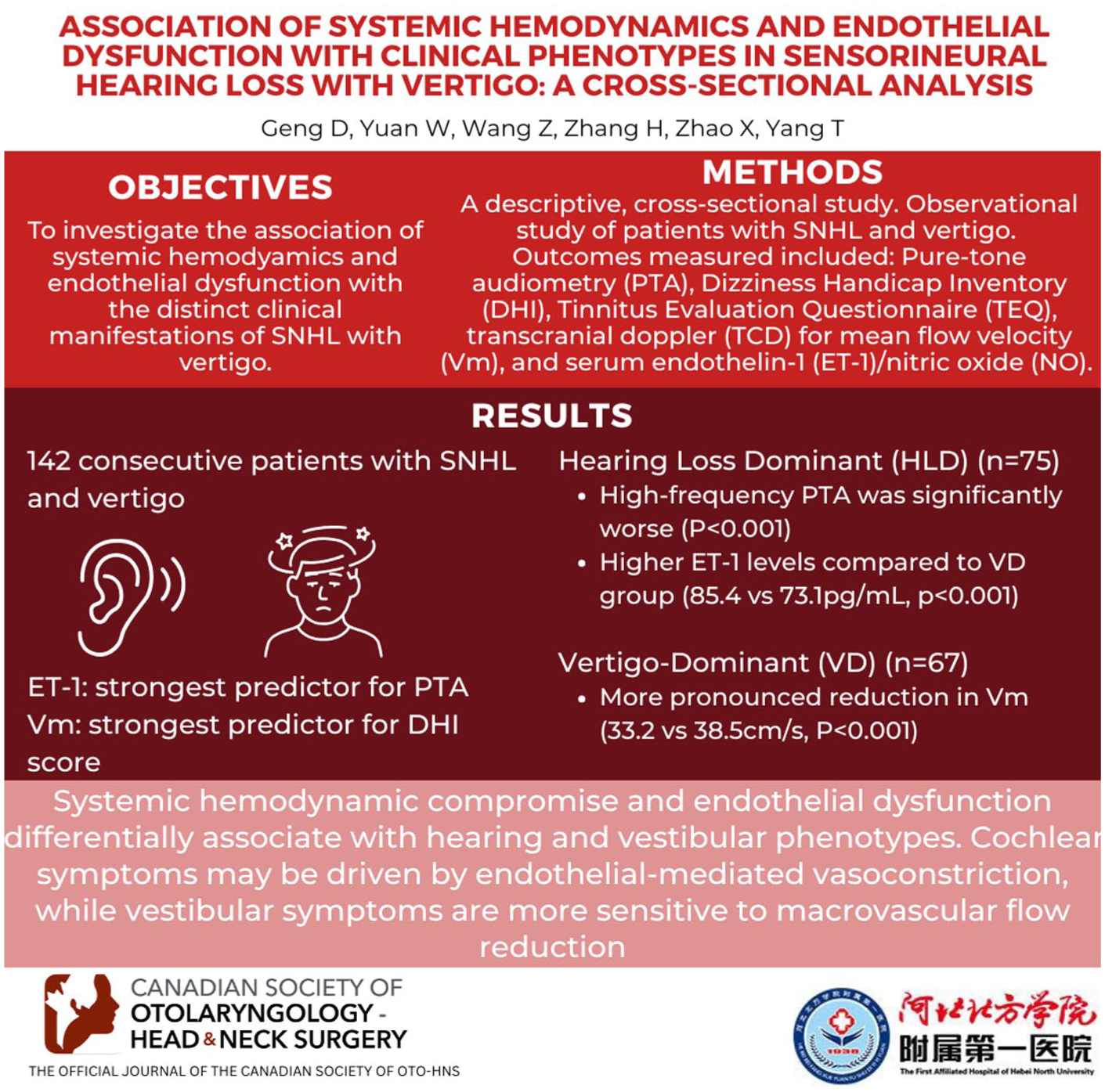
To investigate the association of systemic hemodynamics and endothelial dysfunction with the distinct clinical manifestations of SNHL with vertigo.
Design:
A descriptive, hospital-based cross-sectional study.
Setting:
Department of Otolaryngology Head and Neck Surgery at a tertiary academic hospital.
Participants:
One hundred forty-two consecutive patients with SNHL and vertigo (disease duration ≤30 days) enrolled between January 2023 and October 2025.
Intervention:
Observational study; no intervention was performed.
Main Outcome Measures:
Pure-tone audiometry (PTA) including high-frequency thresholds (6-8 kHz), Dizziness Handicap Inventory (DHI), Tinnitus Evaluation Questionnaire, transcranial Doppler for mean flow velocity (Vm), and serum endothelin-1 (ET-1)/nitric oxide (NO). Linear regression analyzed associations.
Results:
Linear regression showed PTA was significantly predicted by higher ET-1 (R2 = .37, P < .001) and lower NO. DHI was predicted by lower Vm (R2 = .40, P < .001). High-frequency PTA (6-8 kHz) was significantly worse in the Hearing Loss-Dominant (HLD) group (P < .001). The HLD group (n = 75) exhibited significantly higher ET-1 levels compared to the Vertigo-Dominant (VD) group (n = 67) (85.4 vs 73.1 pg/mL, P < .001). Conversely, the VD group showed a more pronounced reduction in Vm (33.2 vs 38.5 cm/s, P < .001). Multiple linear regression identified ET-1 as the strongest predictor for PTA and Vm for DHI score.
Conclusions:
Systemic hemodynamic compromise and endothelial dysfunction differentially associate with hearing and vestibular phenotypes. Cochlear symptoms may be driven by endothelial-mediated vasoconstriction, while vestibular symptoms are more sensitive to macrovascular flow reduction.
Relevance:
Vascular profiling could inform targeted therapeutic strategies.
Keywords
Key Messages
Sensorineural hearing loss with vertigo presents with distinct “Hearing-Dominant” and “Vertigo-Dominant” clinical phenotypes associated with different vascular profiles.
Endothelial dysfunction (elevated ET-1) is the primary predictor of hearing loss severity, while hemodynamic compromise (reduced vertebral flow) drives vestibular handicap.
Vascular profiling using transcranial Doppler and serum biomarkers may guide personalized therapeutic strategies for cochleovestibular disorders.
Introduction
Sensorineural hearing loss (SNHL) co-presenting with vertigo is a debilitating condition that poses a significant diagnostic and therapeutic challenge. This clinical entity, encompassing disorders such as sudden SNHL with vestibular symptoms, significantly compromises patients’ ability to communicate and maintain balance, leading to a drastic reduction in quality of life and often triggering secondary psychological morbidities such as anxiety and depression.1,2 It is also important to note that many individuals with SNHL and vertigo also experience tinnitus, which further diminishes their quality of life and can lead to concurrent psychiatric symptoms. Specifically, the severity of tinnitus handicap has been shown to correlate strongly with depression and anxiety scores, necessitating comprehensive management. 3
While the etiology is often idiopathic, the predominant hypothesis for its pathophysiology centers on a vascular ischemic event within the labyrinthine artery territory, which provides a common blood supply to both the cochlea and the vestibular apparatus.4,5 This “cochleovestibular ischemia” theory, however, does not fully account for the vast clinical heterogeneity observed in patients. Some individuals present with profound hearing loss but only mild dizziness, while others suffer from incapacitating vertigo with relatively preserved hearing. 6
Considering the ischemic background, the correlation between vestibular and auditory symptoms can be found not only in the inner ear but also due to posterior circulation ischemia. In addition, an important pathophysiological connection between vertigo and SNHL is endolymphatic hydrops in the inner ear. Although this condition may also be linked to circulation issues, it is essential to recognize this phenomenon. 7 Understanding the pathophysiological underpinnings of these distinct clinical phenotypes is crucial for developing more precise and effective treatments.
Systemic hemodynamic status and vascular endothelial function are key determinants of microcirculatory perfusion. 8 Transcranial Doppler (TCD) ultrasonography offers a non-invasive method to assess the hemodynamics of major cerebral arteries, including the posterior circulation (vertebral-basilar system) from which the labyrinthine artery originates. Parameters such as mean flow velocity (Vm) and pulsatility index (PI) reflect blood flow volume and downstream vascular resistance, respectively, providing an indirect window into inner ear perfusion.9,10 Concurrently, the vascular endothelium plays a pivotal role in regulating local blood flow, and its dysfunction is implicated in numerous ischemic diseases. 11 Endothelin-1 (ET-1), a potent vasoconstrictor, and nitric oxide (NO), a primary vasodilator, are key biomarkers of endothelial health. An imbalance in the ET-1/NO ratio, favoring vasoconstriction, is thought to contribute significantly to microvascular compromise.12,13
While previous studies have linked vascular markers such as endothelial dysfunction and vasospasm to SNHL or vertigo as separate entities, there remains a scarcity of research that systematically investigates their relationship with the combined cochleovestibular syndrome and its phenotypic variations. For instance, a recent study demonstrated that acute SNHL is associated with elevated endothelin-1 and impaired endothelial adhesive function. 12 In contrast, vertigo severity has been linked to vestibular hypofunction, which could reflect a more general reduction in blood flow volume in the anterior vestibular artery (AVA) or PICA territories rather than focal vasospasm. 14 It remains unclear whether the severity of hearing loss and vertigo is driven by the same or different aspects of vascular pathology. Answering such questions could provide a basis for phenotyping patients not just clinically, but also pathophysiologically.
This descriptive clinical cross-sectional study was designed to bridge this knowledge gap. In accordance with the STROBE (Strengthening the Reporting of Observational studies in Epidemiology) guidelines, 15 we aimed to explore the association between systemic hemodynamic parameters, endothelial dysfunction biomarkers, and the clinical phenotypes of SNHL accompanied by vertigo in a cohort of newly diagnosed patients. We hypothesized that distinct patterns of vascular and endothelial dysfunction would be associated with the relative severity of auditory versus vestibular symptoms, thereby providing a potential pathophysiological explanation for the clinical heterogeneity of the disease.
Methods
Study Design and Participants
This was a cross-sectional study conducted at our hospital. A total of 142 consecutive patients were enrolled between January 2023 and October 2025. This study was conducted at the Department of Otolaryngology Head and Neck Surgery, The First Hospital of Zhangjiakou and approved by the Ethics Committee of The First Hospital of Zhangjiakou (Approval No. 2022-11T-025-03, Date: December 20, 2022), and written informed consent was obtained from all participants prior to data collection. The study flowchart is presented in Figure 1.
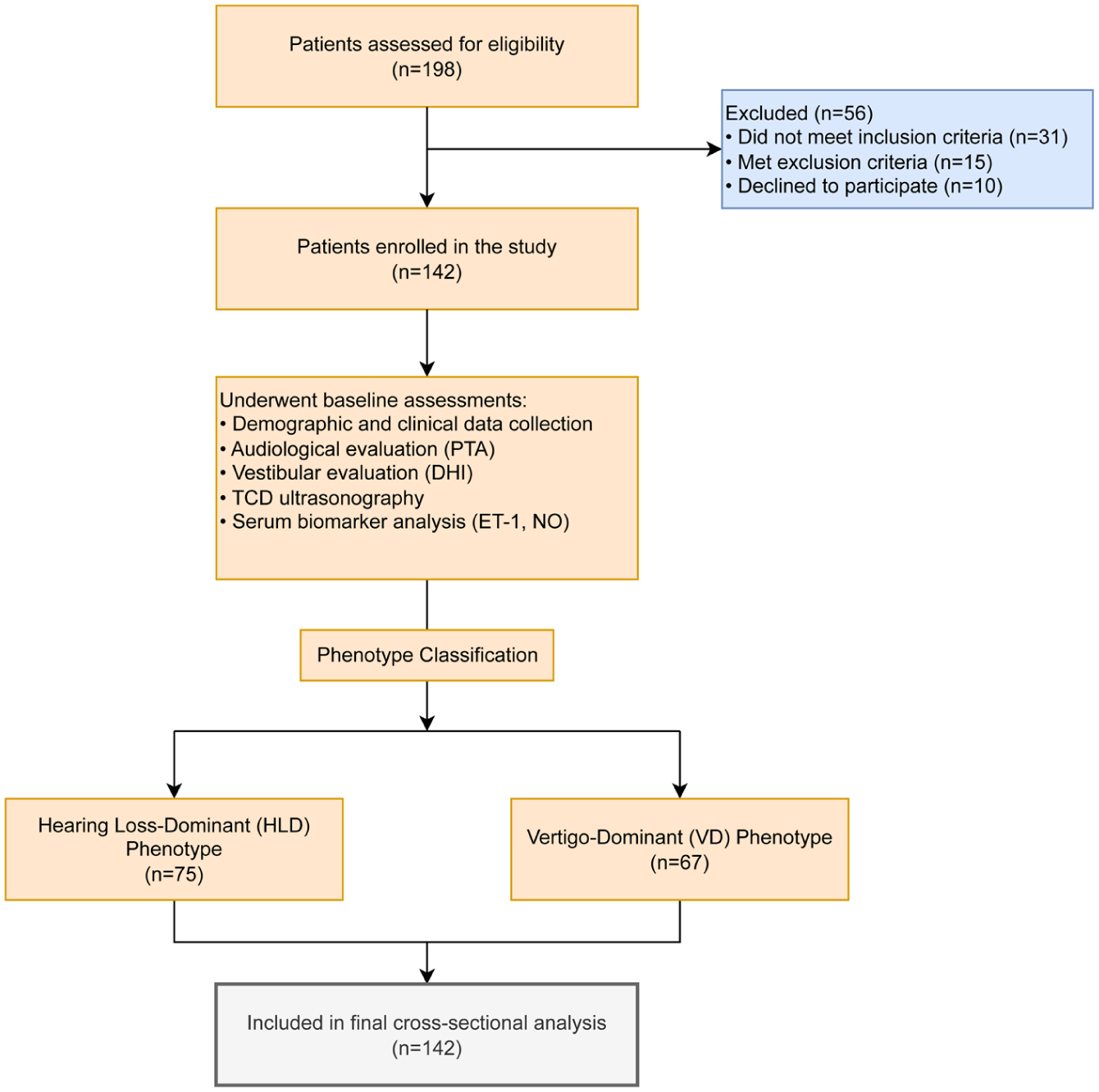
STROBE flow diagram of the study. The diagram illustrates the process of participant enrollment, assessment, and inclusion in the final analysis for this cross-sectional study. PTA, pure-tone audiometry; DHI, Dizziness Handicap Inventory; TCD, Transcranial Doppler; ET-1, endothelin-1; NO, nitric oxide.
Inclusion criteria were: (1) age between 18 and 65 years; (2) diagnosis of SNHL with concurrent vertigo or dizziness; (3) disease onset within 30 days of enrollment; (4) audiometric confirmation of SNHL, defined as a sensorineural hearing loss of ≥30 decibels (dB) in at least 3 consecutive frequencies; (5) willingness to undergo all planned examinations. Exclusion criteria included: (1) conductive or mixed hearing loss; (2) a definitive or probable diagnosis of Ménière’s disease according to the Bárány Society criteria, vestibular neuritis, or benign paroxysmal positional vertigo; (3) hearing loss attributable to trauma, ototoxic drugs, noise exposure, or tumors (eg, vestibular schwannoma); (4) history of fluctuating hearing loss; (5) severe uncontrolled systemic diseases, including cardiovascular, cerebrovascular, renal, or autoimmune disorders; (6) central vestibular disorders such as vestibular migraine or posterior circulation ischemia confirmed by MRI; (7) autoimmune inner ear disease, ruled out via clinical history and serological screening including antinuclear antibody, erythrocyte sedimentation rate, and C-reactive protein.
Data Collection and Clinical Assessments
All data were collected at the time of initial diagnosis, before the initiation of any specific treatment. A standardized case report form was used to collect demographic data, medical history, and symptom duration.
Audiological Evaluation: A comprehensive audiological assessment was performed by an experienced audiologist in a soundproof chamber using a GSI 61 Audiometer (Grason-Stadler, MN, USA). Pure tone average (PTA) was calculated as the mean of air-conduction hearing thresholds at 0.5, 1, 2, and 4 kHz for the worse-affected ear. Additionally, high-frequency thresholds were measured at 6 and 8 kHz, and High-Frequency PTA (HF-PTA) was calculated as the mean of these 2 frequencies. SNHL was staged as Mild (26-40 dB), Moderate (41-55 dB), Moderately Severe (56-70 dB), Severe (71-90 dB), and Profound (>90 dB).
Assessment of Dizziness and Quality of Life: The severity of vertigo-related handicap was quantified using the validated Chinese version of the DHI. 16 The DHI consists of 25 items divided into 3 subscales: physical, functional, and emotional. The total score ranges from 0 to 100, categorized as mild (0-30), moderate (31-60), and severe (61-100) handicap. Tinnitus severity was assessed using the Tinnitus Evaluation Questionnaire (TEQ), which comprises 6 items evaluating tinnitus duration, intermittency, timber, loudness, sleep disturbance, and annoyance, graded on a total severity scale. 17
Transcranial Doppler (TCD) Ultrasonography: TCD examinations were performed using a Multi-Dop X digital system (DWL Elektronische Systeme GmbH, Germany). Patients rested in a supine position for at least 15 minutes before the measurement. A 2-MHz probe was placed at the suboccipital window to insonate the vertebral-basilar artery. The mean flow velocity (Vm) and PI were recorded. Measurements were repeated 3 times, and the average value was used for analysis. The PI was calculated as (peak systolic velocity − end-diastolic velocity)/Vm. All measurements were conducted by a single certified neurosonographer blinded to the patients’ clinical details. 18
Biochemical Analysis: Venous blood samples were drawn from each patient in the morning after an overnight fast into serum separator tubes. Samples were centrifuged at 3000 rpm for 15 minutes, and the serum was stored at -80°C until analysis. Serum levels of ET-1 and NO were measured using commercially available enzyme-linked immunosorbent assay kits (R&D Systems, Minneapolis, MN, USA) according to the manufacturer’s instructions. 19 All samples were analyzed in duplicate by a laboratory technician blinded to the patient data.
Phenotype Classification
To compare subgroups with different clinical presentations, patients were classified into 2 phenotypes: “Hearing Loss-Dominant” (HLD) and “Vertigo-Dominant” (VD). As PTA and DHI have different scales, scores were first normalized into Z-scores using the mean and standard deviation of the entire cohort. A dominance score was calculated for each patient as Z-score (DHI) − Z-score(PTA). Patients with a negative dominance score were classified as HLD, while those with a positive or zero score were classified as VD. 19
Statistical Analysis
Statistical analyses were performed using SPSS for Windows, version 26.0 (IBM Corp., Armonk, NY, USA). Continuous data were presented as mean ± standard deviation (SD), and categorical data as frequency (percentage). The normality of data distribution was assessed using the Shapiro-Wilk test. Linear regression analyses were performed to evaluate the relationships between clinical scores (PTA, DHI) and vascular markers (ET-1, Vm), providing regression equations and R2 values. Independent samples t-tests were used to compare means of continuous variables between the HLD and VD phenotype groups. Multiple linear regression analysis, using a stepwise method, was performed to identify independent predictors of PTA and DHI scores. Variables included in the regression model were age, sex, disease duration, Vm, PI, ET-1, and NO. A two-sided P value <.05 was considered statistically significant for all analyses.
Results
Participant Characteristics
A total of 142 patients (70 males, 72 females) with SNHL and vertigo were included in the final analysis. The mean age of the cohort was 48.7 ± 12.5 years, and the mean duration of symptoms prior to presentation was 9.8 ± 6.3 days. The non-statistically significant differences in age (P = .481) and sex (P = .755) ensured the comparability of the groups (Table 1). The mean PTA for the worse ear was 62.4 ± 15.8 dB HL, and the mean DHI score was 64.1 ± 18.2. Based on the phenotype classification algorithm, 75 patients (52.8%) were categorized into the HLD group, and 67 patients (47.2%) were categorized into the VD group. The baseline demographic and clinical characteristics of the total cohort and the 2 phenotype groups are summarized in Table 1.
Baseline Demographic and Clinical Characteristics of the Study Participants.
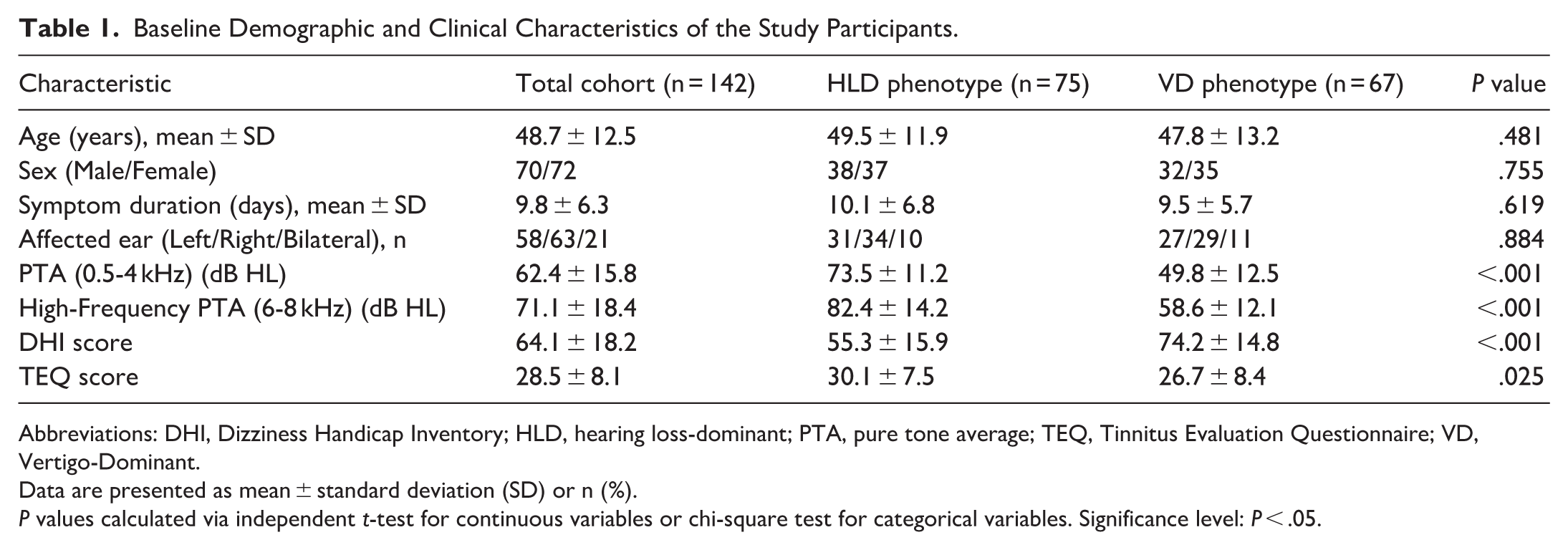
Abbreviations: DHI, Dizziness Handicap Inventory; HLD, hearing loss-dominant; PTA, pure tone average; TEQ, Tinnitus Evaluation Questionnaire; VD, Vertigo-Dominant.
Data are presented as mean ± standard deviation (SD) or n (%).
P values calculated via independent t-test for continuous variables or chi-square test for categorical variables. Significance level: P < .05.
Regression Analysis of Vascular Markers and Clinical Severity
Linear regression analysis demonstrated a statistically significant positive relationship between PTA and ET-1 [F(1, 140) = 83.2, P < .001, R2 = 0.37]. The regression equation was: PTA (dB) = 0.82 × ET-1 (pg/mL) − 3.4. Similarly, a strong negative linear relationship was observed between DHI scores and Mean Flow Velocity (Vm) [F(1, 140) = 94.5, P < .001, R2 = 0.40], with the equation: DHI = −2.1 × Vm (cm/s) + 138.5. These results are illustrated in Figure 2 and Table 2. This indicates that poorer hearing is associated with increased vasoconstriction, higher distal resistance, and lower blood flow velocity. Similarly, higher DHI scores (worsening vertigo) were also significantly correlated with all vascular markers.
Pearson Correlation Coefficients (r) Between Vascular Markers and Clinical Severity Scores.
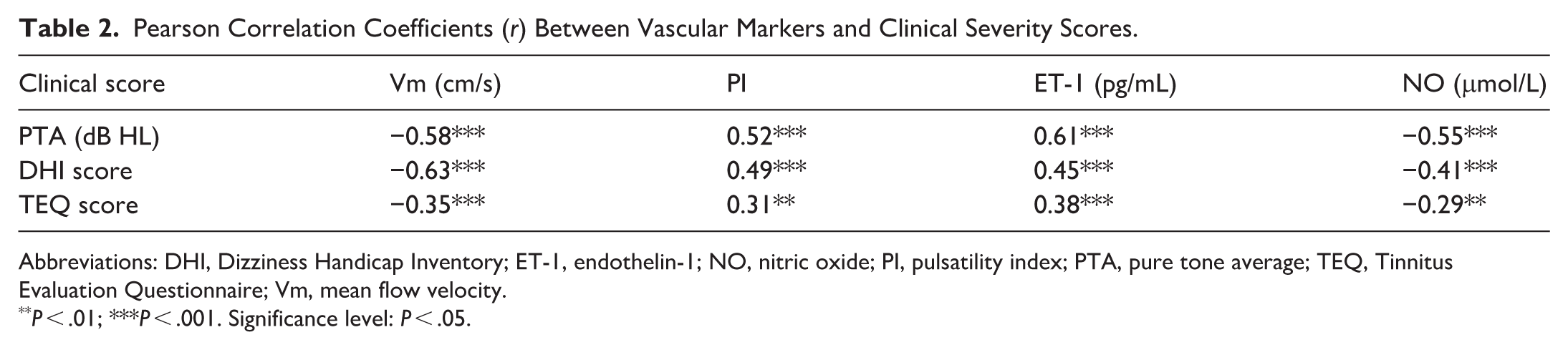
Abbreviations: DHI, Dizziness Handicap Inventory; ET-1, endothelin-1; NO, nitric oxide; PI, pulsatility index; PTA, pure tone average; TEQ, Tinnitus Evaluation Questionnaire; Vm, mean flow velocity.
P < .01; ***P < .001. Significance level: P < .05.
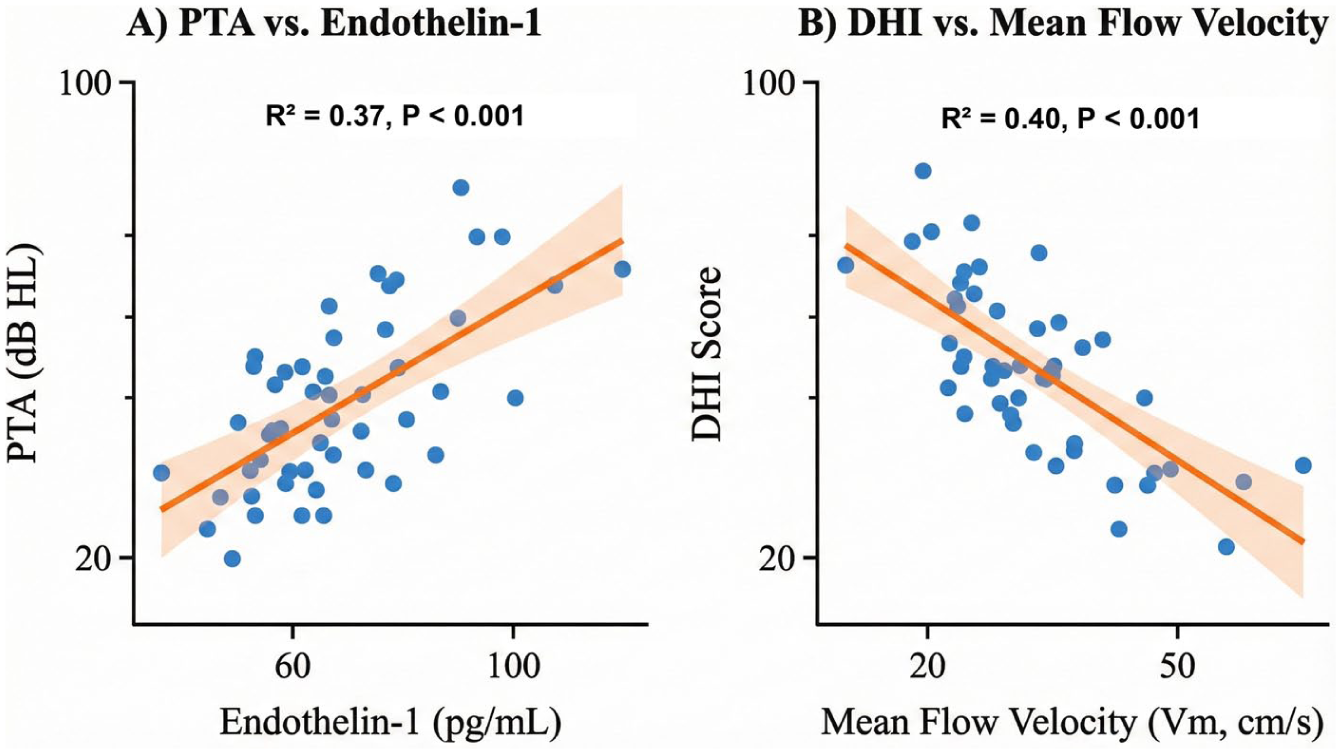
Linear regression analysis of vascular markers and clinical severity. (A) Regression plot showing the significant positive linear relationship between pure tone average (PTA) and serum Endothelin-1 (ET-1) levels (R2 = 0.37, P < .001) (Linear regression equation: PTA = 0.82 × ET-1 − 3.4). (B) Regression plot showing the significant negative linear relationship between Dizziness Handicap Inventory (DHI) scores and Mean Flow Velocity (Vm) (R2 = 0.40, P < .001) (Linear regression equation: DHI = −2.1 × Vm + 138.5). The solid line represents the linear regression fit, and the shaded area indicates the 95% confidence interval.
Comparison of Vascular Markers between Clinical Phenotypes
When comparing the 2 predefined clinical phenotypes, significant differences in vascular markers emerged (Figure 3). The HLD group, characterized by more severe hearing loss relative to vertigo, had significantly higher serum ET-1 levels (85.4 ± 10.1 pg/mL) compared to the VD group (73.1 ± 9.5 pg/mL, P < .001). The HLD group also had higher PI values (1.15 ± 0.18 vs 1.08 ± 0.15, P = .012). Conversely, the VD group, characterized by more severe vertigo, demonstrated significantly lower Vm in the vertebral-basilar artery (33.2 ± 6.1 cm/s) compared to the HLD group (38.5 ± 7.3 cm/s, P < .001). Serum NO levels were lower in the HLD group, consistent with greater endothelial dysfunction, and although less pronounced, the difference remained statistically significant (45.7 ± 8.9 μmol/L vs 49.8 ± 9.7 μmol/L, P = .009). The distribution of these data is presented in boxplots in Figure 3.
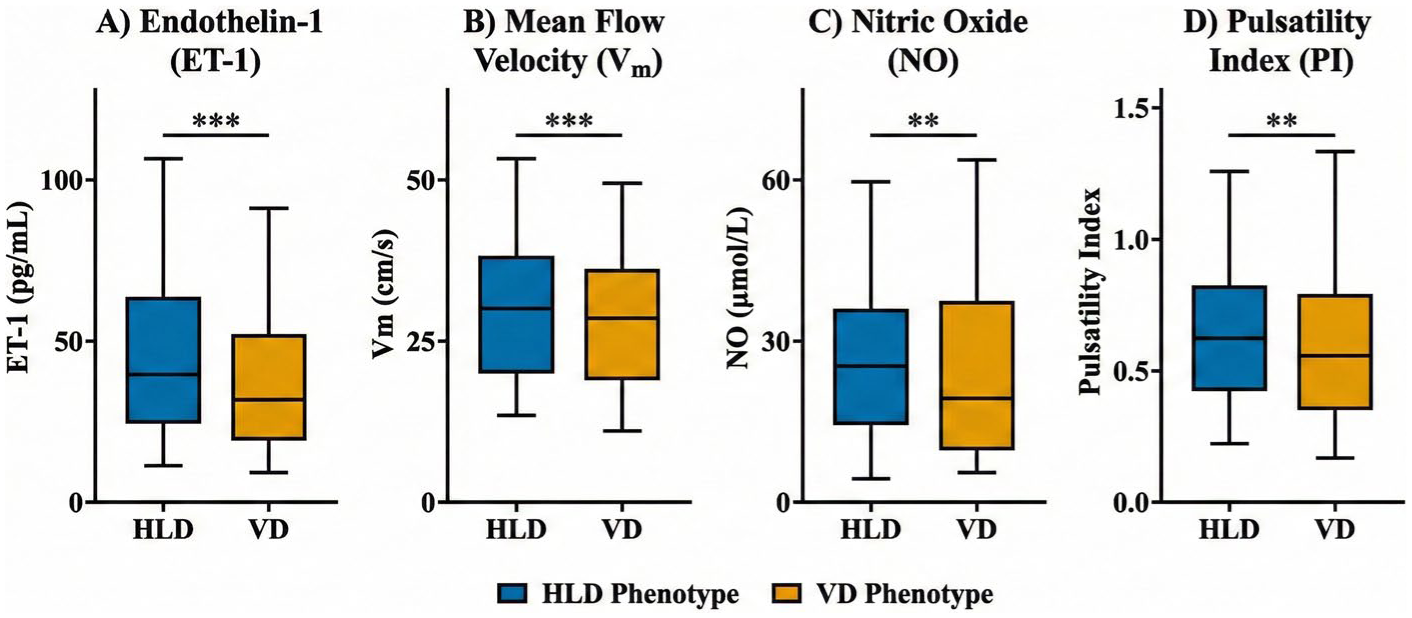
Comparison of vascular markers between clinical phenotypes represented as Boxplots. The boxplots display the distribution of (A) Endothelin-1 (ET-1), (B) Mean Flow Velocity (Vm), (C) Nitric Oxide (NO), and (D) Pulsatility Index (PI) between the Hearing Loss-Dominant (HLD) and Vertigo-Dominant (VD) groups. The central horizontal line represents the median, the box limits indicate the 25th and 75th percentiles (interquartile range), and the whiskers extend to the minimum and maximum values excluding outliers. **P < .01, ***P < .001 (Independent samples t-test).
Independent Predictors of Clinical Severity
To identify the most influential factors for hearing loss and vertigo severity, 2 separate multiple linear regression models were constructed (Table 3). In the model predicting PTA, after adjusting for age, sex, and disease duration, serum ET-1 level emerged as the strongest independent predictor (β = 0.53, P < .001), followed by Vm (β = −0.31, P < .001). These 2 variables together explained 48% of the variance in PTA (Adjusted R2 = 0.48). In the model predicting the DHI score, Vm was the strongest independent predictor (β = −0.47, P < .001), followed by PI (β = 0.25, P = .002). This model explained 45% of the variance in DHI scores (Adjusted R2 = 0.45). These results suggest that while both circulatory aspects are involved, endothelial dysfunction (represented by ET-1) is a more dominant predictor for the degree of hearing loss, whereas compromised blood flow (represented by Vm) is a more dominant predictor for the severity of vertigo.
Stepwise Multiple Linear Regression Analysis For Predictors of PTA and DHI Scores.
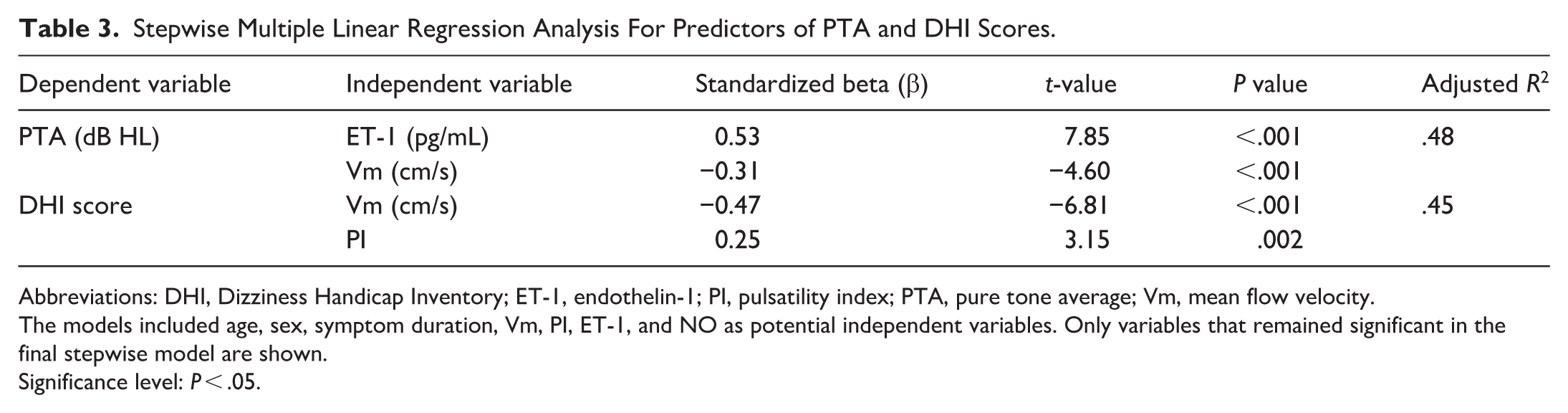
Abbreviations: DHI, Dizziness Handicap Inventory; ET-1, endothelin-1; PI, pulsatility index; PTA, pure tone average; Vm, mean flow velocity.
The models included age, sex, symptom duration, Vm, PI, ET-1, and NO as potential independent variables. Only variables that remained significant in the final stepwise model are shown.
Significance level: P < .05.
Discussion
This cross-sectional study provides evidence of significant associations between specific patterns of systemic hemodynamic and endothelial dysfunction and the heterogeneous clinical presentation of SNHL with vertigo. Our main findings are threefold: first, the overall severity of cochleovestibular symptoms is strongly correlated with markers of impaired microcirculation, including reduced blood flow velocity, increased vascular resistance, and an endothelial imbalance favoring vasoconstriction. Second, we identified distinct vascular profiles for different clinical phenotypes: patients with HLD symptoms exhibited more significant endothelial dysfunction (higher ET-1), whereas those with VD symptoms showed more pronounced brain blood flow velocity reduction. Third, multivariable regression analyses confirmed that ET-1 and Vm are independent and dominant predictors for the severity of hearing loss and vertigo, respectively.
Our results align with recent literature highlighting the vascular etiology in otologic disorders. For instance, a recent study utilizing carotid and vertebral ultrasonography found that vascular changes such as intima-media thickening were significantly associated with elevated PTA values in tinnitus patients, supporting the link between macrovascular health and cochlear function. 14 The strong correlations observed between vascular markers and clinical severity reaffirm the central role of the vascular ischemic hypothesis in the pathogenesis of this condition.20,21 The labyrinthine artery is a small-caliber end-artery, making the inner ear exquisitely sensitive to any reduction in perfusion pressure or increase in vascular resistance. 20 Our data quantitatively support this, showing that patients with worse hearing and more severe vertigo have measurable deficits in their posterior circulation hemodynamics and endothelial function.22,23 This finding aligns with previous reports that have independently linked TCD abnormalities or endothelial dysfunction with either sudden hearing loss or vestibular disorders.24,25
The most novel contribution of our study is the elucidation of a potential pathophysiological basis for the observed clinical heterogeneity. Our phenotype analysis suggests that the type of vascular insult may dictate the primary clinical manifestation. The strong association between elevated ET-1 levels and the HLD phenotype points toward a mechanism driven by intense vasoconstriction or vasospasm. ET-1 is one of the most potent endogenous vasoconstrictors, and its overproduction can lead to severe and prolonged reduction in microvascular blood flow. 26 While direct oxidative stress markers were not measured, the observed endothelial dysfunction may suggest oxidative stress mechanisms consistent with recent findings. 27 The cochlea, with its high metabolic rate, is particularly vulnerable to such ischemic events, which could explain why severe endothelial dysfunction preferentially manifests as profound hearing loss. This is consistent with animal models where ET-1 administration induces cochlear ischemia and hearing threshold shifts. 27
Conversely, the finding that reduced Vm is the strongest predictor for vertigo severity and is significantly lower in the VD phenotype suggests a different primary mechanism for vestibular dysfunction. Vestibular symptoms might be more sensitive to a general state of low perfusion or hypovolemia in the posterior circulation, rather than acute vasospasm. The vestibular system may be more resilient to transient ischemia than the cochlea but more susceptible to sustained, lower-grade hypoperfusion, which would be reflected as a chronically reduced Vm. 28 This could explain why some patients experience severe vertigo even with moderate hearing loss. The hemodynamic compromise (low Vm) might not cause extensive cochlear necrosis but could sufficiently disrupt the vestibular nuclei and pathways. 29 The lack of objective vestibular testing limits our ability to pinpoint the exact site of lesion, but the correlation with Vm supports a macrovascular etiology.
These findings have significant clinical implications. By identifying the dominant underlying vascular pathology, it may be possible to tailor treatments more effectively. For instance, patients identified with an HLD phenotype and high ET-1 levels might benefit more from therapies targeting endothelial dysfunction, such as ET-1 receptor antagonists or agents that enhance NO production.30,31 In contrast, patients with a VD phenotype and low Vm might be candidates for treatments aimed at improving systemic hemodynamics, such as volume expansion or agents that augment cerebral blood flow. This moves beyond a “one-size-fits-all” approach and toward a more personalized, pathophysiology-guided therapeutic strategy.
This study has several strengths, including a well-characterized cohort of patients, the use of standardized and objective measurement techniques, and a novel approach to clinical phenotyping. However, limitations must be acknowledged. First, the cross-sectional design precludes any inference of causality; we can only report associations. Longitudinal studies are needed to determine if these baseline vascular markers can predict treatment outcomes. Second, TCD measures hemodynamics in larger, upstream vessels, which is an indirect surrogate for the microcirculation of the inner ear itself. Direct imaging of inner ear perfusion remains a major technical challenge. Third, although we excluded patients with known severe systemic diseases, subclinical comorbidities could still have influenced the vascular markers. Fourth, while we used the DHI for subjective assessment, the absence of objective vestibular testing (eg, caloric testing, VEMP, and vHIT) significantly limits the generalizability regarding specific semicircular canal involvement. Similarly, PTA is a subjective measure, and future studies should include objective audiometry such as ABR and OAE. Finally, our phenotype classification was based on a data-driven approach, which requires further validation in independent cohorts. Furthermore, our study focused exclusively on patients with combined cochleovestibular symptoms to deconvolute this specific phenotype. The lack of a non-vertigo SSNHL control group is a limitation, and future comparative studies are required to validate whether these vascular profiles are unique to the combined syndrome.
Conclusion
In conclusion, our findings demonstrate a significant association between systemic vascular dysfunction and the clinical severity of SNHL with vertigo. We provide novel evidence that the heterogeneity of this condition may be explained by different underlying vascular pathologies: severe endothelial dysfunction, particularly elevated ET-1, is a key predictor for the severity of hearing loss, while compromised cerebral blood flow velocity is the dominant predictor for vertigo handicap. These insights not only enhance our understanding of the disease’s pathophysiology but also pave the way for a more stratified and personalized approach to the management of patients with cochleovestibular disorders.
Footnotes
Acknowledgements
We extend our sincere gratitude to all the patients who participated in this study and to the staff of the audiology and neurosonology departments at The First Hospital of Zhangjiakou for their invaluable technical support.
Ethical Considerations
This study was conducted at The First Hospital of Zhangjiakou. This study was approved by the Ethics Committee of The First Hospital of Zhangjiakou (Approval No. 2022-11T-025-03, Date: December 20, 2022).
Consent to Participate
Written informed consent was obtained from all participants prior to their enrollment in the study.
Author Contributions
DG and WY conceived and designed the study, performed the analysis, and drafted the manuscript. HZ and XZ participated in data collection and statistical analysis. TY provided clinical insights and reviewed the data. ZW supervised the entire project, provided critical revision, and approved the final version. All authors read and approved the final manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Scientific Research Plan Project of Hebei Administration of Traditional Chinese Medicine (Project No. 2026411).
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.