
Abstract
Interpretation of deaths in hostile environments may be informed by postmortem microscopic examination of injured tissues. In context with their macroscopic correlates, the commonly observed histologic changes seen in environmental deaths are reviewed—these include exposure (i.e., hypothermia and hyperthermia), fire, electrocution, and water. Rarely observed pathognomonic findings are highlighted. While it may not yield specific findings, microscopic examination is one of the necessary steps of a thorough postmortem examination.
Introduction
The four classical elements are the accused. Their injurious effects are seen in postmortem examination and frequently invoked to corroborate pre-autopsy information about the scene, circumstances, and history of a person’s death. Given the importance of accurate determination of cause of death (and the implications of incorrect attribution), the histopathologic changes (with macroscopic correlates) seen in environmental deaths are reviewed here.
Here, hostile environments are categorized by their nature as well as their effects. They are grouped (and herein reviewed) as deaths by: exposure, causing hyperthermia and hypothermia; fire, causing smoke inhalation and thermal injury; electricity; and water, causing drowning, dysbarism, and hypothermia. These categories do not directly implicate the only solid classical element, earth. Its effects on the body result from mechanical trauma that is well described in the archival literature; accordingly, there would be negligible benefit from an additional histopathologic description of the canonical blunt and sharp force injuries. Poisons are excluded from the present discussion because their identification is confirmed using toxicologic methods, even though they may create characteristic morphologic changes (e.g., globus pallidus necrosis in survivors of carbon monoxide poisoning).
The histopathologic features that range from pathognomonic to entirely nonspecific in each of these types of environmental death is reviewed in the following sections.
Discussion
Air: Hypothermia and Hyperthermia
Hypothermia
There are no specific diagnostic findings in death by hypothermia, despite the oft cited characteristic constellation of gross findings that include cold erythema (especially over large joints) and localized frostbite, Wischnewski spots, and pancreatic changes (1 –3); paradoxical undressing and stigmata of “hide-and-die” syndrome (abrasions of the knees and knuckles) are behavioral phenomena seen in hypothermic deaths, each with its own theoretical explanations (1). With the exception of paradoxical undressing, each of these gross features has its microscopic correlate. Changes of several other organ systems have been reported in the archival literature, including vacuolization of hepatocytes, adrenal, exocrine pancreatic, and renal cells; hypoxic cardiac changes; and fatty changes of cardiomyocytes, hepatocytes, and renal tubular cells. Cold erythema and frostbite, Wischnewski spots, pancreatitis, and fatty changes of the renal tubular cells will be described here.
In frostbite, acral tissue (such as fingers, toes, ears, and nose) freezes and becomes blue or white; blistering forms a day or so after rewarming and is replaced days later by scarring. Microscopic examination will reveal necrosis of the affected area with surrounding inflammatory infiltrate and granulation tissue formation at the boundary between viable and necrotic tissue (4). In cold erythema, cellular damage is not seen; rather, physiologic derangement is indicated by the nonspecific findings of congestive hyperemia (vascular dilation/engorgement) in the subcutaneous soft tissues (5).
Grossly, Wischnewski spots appear as black-brown discolorations of the gastric mucosa (Image 1). Using routine histology and immunohistochemistry on serial sections of Wischnewski spots in 14 cases of hypothermia, Tsokos et al. attempted to characterize the lesions and understand their underlying pathophysiology (6). Histologically, gastric erosions or ulcers were not identified, neither were inflammatory infiltrates or fibrin exudates; however, the regions reacted positively with anti-hemoglobin. The authors concluded that the spots represent peri-agonal circumscribed hemorrhages of gastric glands, with release autolytic destruction of erythrocytes causing release of hemoglobin that is then hematinized by gastric acid to create the typical black-brown spots. Given the lack of vital injury or response (e.g., erosion, ulceration, inflammation, etc.), Wischnewski spots are interpreted as peri-agonal epiphenomena in hypothermia.
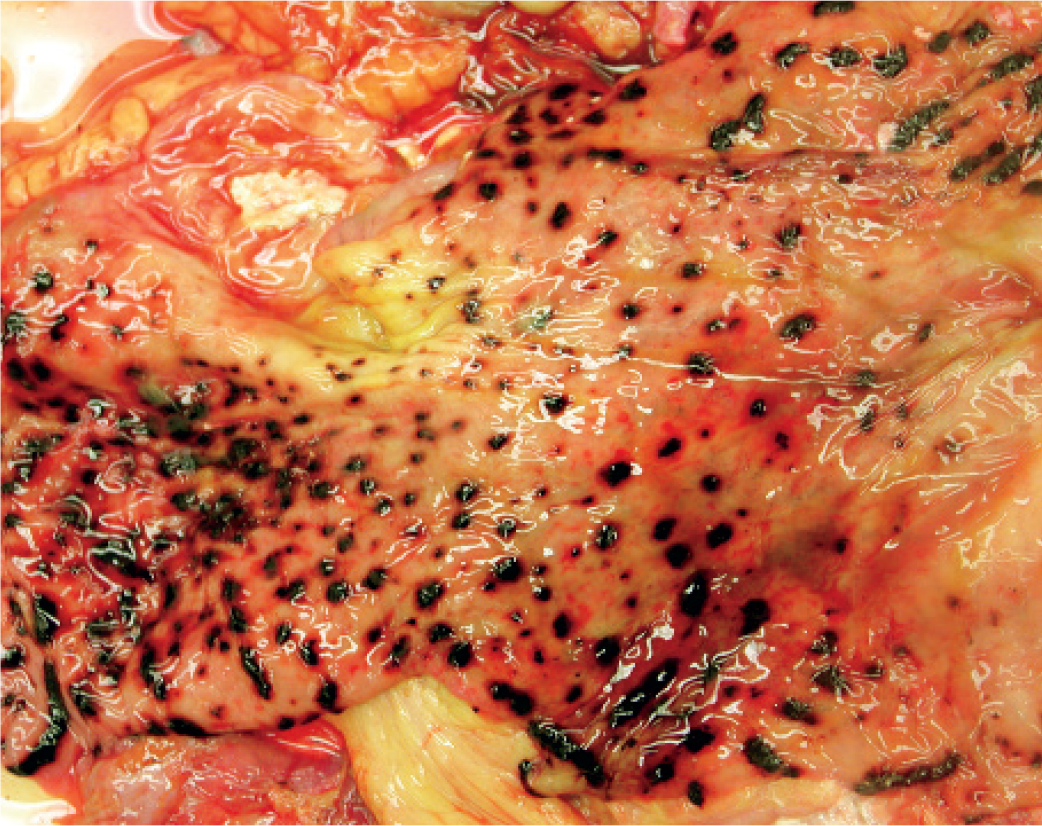
Gross view of hemorrhagic gastropathy. When seen in the context of hypothermia, these are called Wischnewski spots. These are a stress response, also seen in starvation, drowning, and ketoacidosis.
Pancreatic changes, including hemorrhage, acute pancreatitis, and vacuolization of the pancreatic adenoid cells have been observed in deaths due to hypothermia (5, 7). Acute pancreatitis is, possibly, the most commonly cited change. Grossly, acute pancreatitis appears with hemorrhage of the pancreas and surrounding tissue and fat necrosis; microscopic examination will show acute inflammatory infiltrate and, possibly, necrosis of the pancreatic tissue (Image 2).
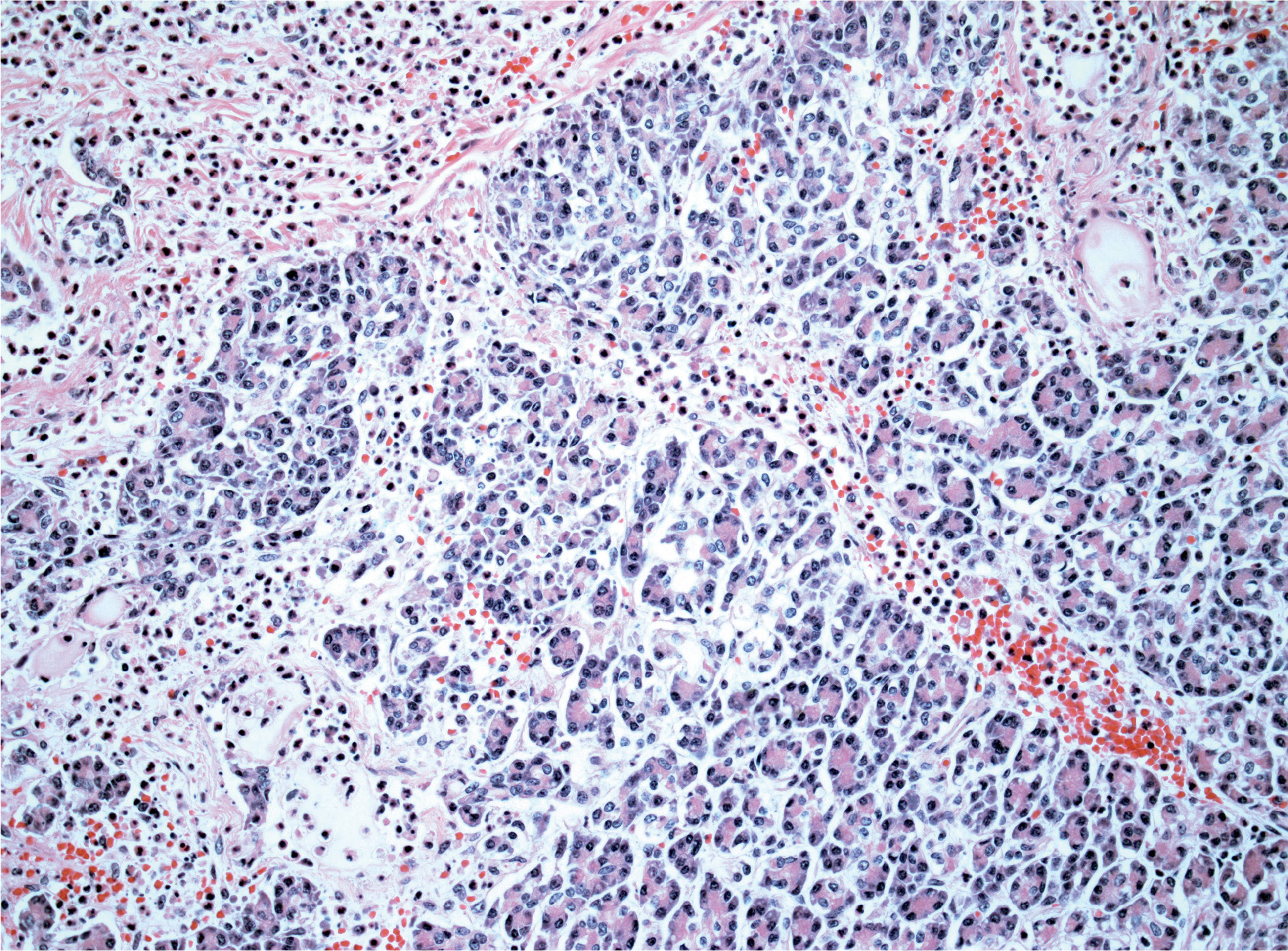
High power view of acute pancreatitis with heavy neutrophilic infiltrate that nearly obscures normal pancreatic parenchyma in one-half of the field of view (H&E, x200).
None of the pancreatic changes, however, is a specific finding; it is common knowledge that hemorrhage and acute pancreatitis have a number of causes. Among a series of studies on hypothermic deaths, Preuss et al. reviewed the pancreatic changes in autopsies due to hypothermia. They found that vacuolization of the adenoid cells of the pancreas could be an additional sign of death due to or associated with hypothermia (7). Vacuolization could therefore be used to support a diagnosis of hypothermia; it cannot be used alone to confirm or to make a diagnosis of hypothermia.
Fatty degeneration of renal tubular epithelium is easily seen on hematoxylin and eosin stained slides as subnuclear (basal) vacuoles of tubular epithelial cells (Image 3); the vacuoles can be highlighted with the periodic acid-Schiff (PAS) staining method. Special significance has been attributed to this finding (8); however, its true value is uncertain. The control group in the study by Preuss et al. included cases with a history of diabetes mellitus, but none where death was attributed to ketoacidosis (which can be caused by diabetes mellitus, alcoholism, and malnourishment) (8). Considering that subnuclear vacuolization is also seen in these conditions, questions around the specificity and causality of this change are raised. It could be that fatty degeneration of the renal tubular epithelium arises in any ketotic state, regardless of whether it is brought on by hypothermia, alcoholism, diabetes mellitus, or malnourishment, or it could be a general but complex pathophysiologic pathway involving stress and leading to death (9, 10). The issue is furthermore complicated because alcoholism, homelessness (malnourishment), and chronic disease are among the risk factors for death due to hypothermia (11).
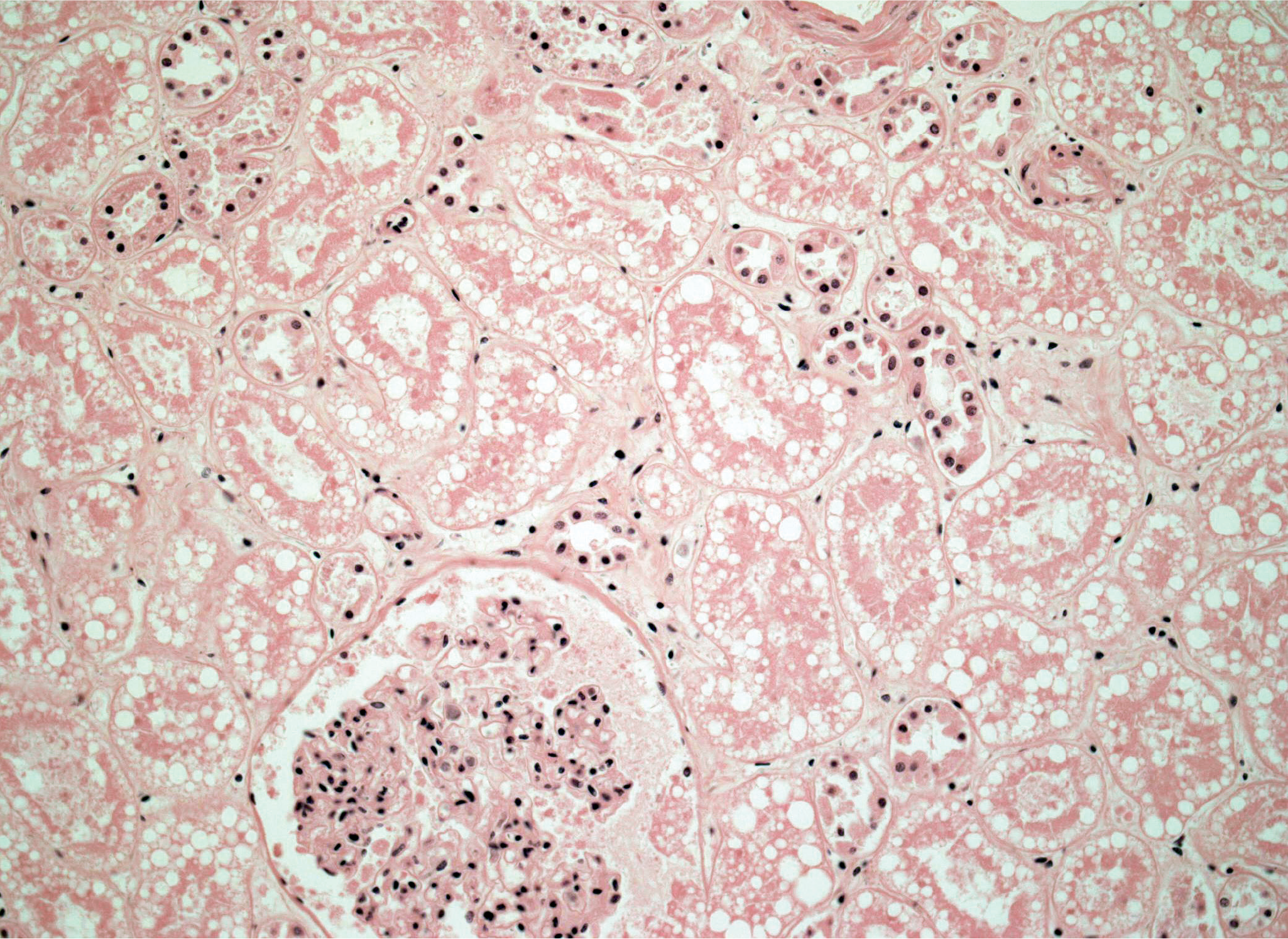
High power view of prominent sub-nuclear vacuoles in the renal tubules; nuclear detail in the tubules has been lost due to autolysis (H&E, x200).
The underlying mechanism of vacuolization seen in other tissues is unclear. To the authors’ knowledge, a justifiable unifying explanation of these findings has not been presented.
In summary, none of the characteristic histopathology findings in hypothermia are unique; each is seen in other conditions that cause death. For example, it is nearly axiomatic that skin erythema is seen in hypothermia, cyanide poisoning, carbon monoxide poisoning, and refrigeration. Rather, a collection of findings (both microscopic and gross) can be used in concert with scene, circumstances, and history to support a diagnosis of hypothermia as the cause of death—as is often the case in forensic pathology.
Hyperthermia
Paradoxically, it is generally accepted that there are no specific autopsy findings for hyperthermia (12, 13). The reason that academia accepts this in hyperthermia and not hypothermia are not known; perhaps it is a quirk of human nature. It is more likely that the postmortem findings in deaths due to hyperthermia are comparatively ordinary: congestion and edema of the skin and organs, right ventricular dilation, subendocardial hemorrhage, and venous distension in the cerebrum (14). The rapid onset and progression of postmortem decomposition may be the best grossly observable clue to hyperthermia—or sepsis (15).
The body of literature on deaths in hyperthermia is largely populated by articles on malignant hyperthermia (including those cited here). In this condition, a rapid rise in body temperature is due to increased metabolism and production of energy in skeletal muscle that can be recognized histologically. Muscle fibers of the heart appear fragmented and skeletal muscle fibers show sarcolysis with lumpy breakdown, phagocytosis of myoglobin, fatty infiltration, and longitudinal striation from clumped myofibrils (16, 17). These changes should not be expected in environmental hyperthermia.
Fire: Smoke Inhalation and Thermal Injury
Deaths due to fire occur acutely/subacutely due to smoke inhalation and/or due to thermal injury, and later due to complications that may arise during treatment and recovery. Regardless of survival time, there is a spectrum of external and internal injuries that can be observed in fire deaths.
The external appearance will depend on whether it is due to moist thermal damage (scalds) or due to burns from dry heat. Scalds usually do not have carbonization; they are characteristically well demarcated and uniform over the entire burn area. Dry burns have variable appearance, ranging from reddening to carbonization to complete destruction of surface skin. The additional characteristic features of severe dry burns include skin splitting, fracture contractions, and the pugilistic stance.
Internal gross evidence includes heat epidural hematoma, heat fixation of tissues, and deposition of soot in the airways. Bright “cherry red” coloration of the blood and tissues may be seen if there was sufficient inhalation of carbon monoxide gas prior to death. When this is seen, measurement of blood carboxyhemoglobin level can used to determine whether a person was dead or alive at the time of the fire, which is critical to accurately certify the death. Forensic pathologists might also resort to histologic examination of tissues in order assist determination of cause of death and vitality of thermal injuries.
Smoke Inhalation
Injuries of the respiratory tract by inhaled hot gases indicate vitality—that the person was alive at the time of the fire. Deposition of soot in the airways may be seen with the naked eye; photographic methods using alternative light sources may also be used to highlight nonorganic materials in the airways (18, 19). Deaths attributed to smoke inhalation result from the effects of toxic gases produced by the fire (such as carbon monoxide, cyanide, nitrogen species, etc.); thermal injury of the respiratory tract may also result.
Histologic examination of mucosal and submucosal tissues may also reveal unique signs of heat and smoke inhalation. Soot may be found up to the secondand third-order bronchi (Image 4) (20). Additional features are easily identified in the trachea, vocal cords, and large to medium sized airways of the lungs; these will have the similar features to those commonly recognized as cautery/heat artifacts seen in surgical pathology specimens. These early findings of heat inhalation trauma include loss of the ciliated border, basal vacuolization of the respiratory epithelium, elongated and palisading cell nuclei, swelling and coagulative necrosis of epithelial cells, submucosal congestion and edema, and protrusion of submucosal glands (21).
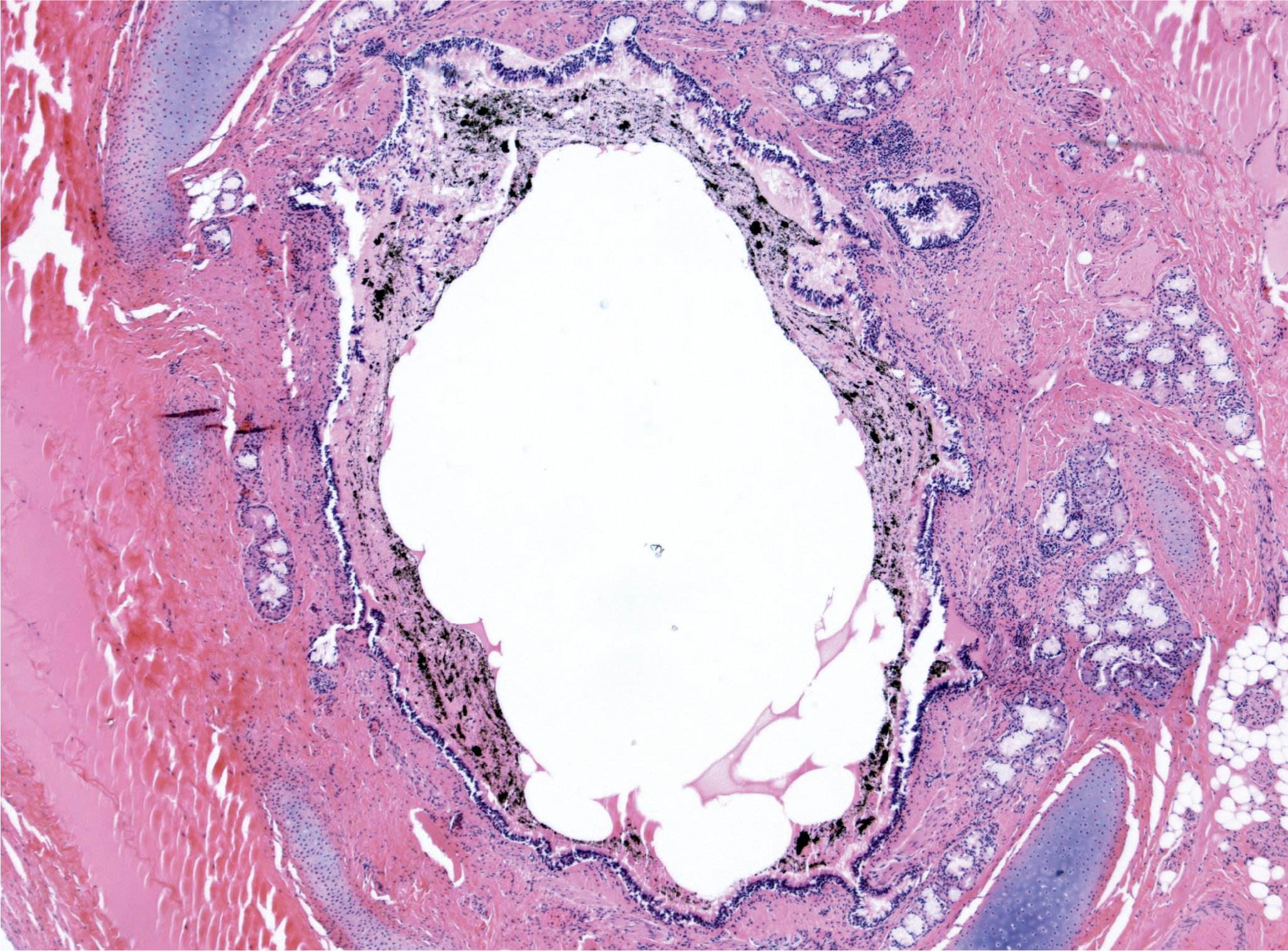
Deposition of soot in a medium sized airway is seen as anthracotic pigment on the mucosal lining (H&E, x40).
In an interesting comparison study, morphologic changes in the lungs of people who died in fire and who died by suffocation were compared (22). Bronchiolar dilatation, ductal and alveolar insufflation, and alveolar hemorrhage were seen in fire deaths but not suffocations; it is not certain that these changes are unique to fire deaths, however. Unfortunately, these heat-induced changes are not always seen (23, 24).
This presence of soot in the airways is a strong indicator that a person was alive at the time of the fire, however it is not definitive; corroborating evidence, as described above, should be sought. Additional corroborating evidence could also include external signs of thermal injury.
Thermal Injury
When the cause of death is attributed to thermal injury, death may have occurred acutely or subacutely due to physiologic disturbances that result from the injuries, or remotely due to complications that may arise during recovery. The sequelae of thermal injuries depend upon depth and extent (body surface area) of burns, degree and nature of inhalation injuries, and post-injury care. Burns are classified as superficial (confined to the epidermis, formerly known as 1st degree), partial thickness (injury extends to the dermis, formerly known as 2nd degree), and full thickness (extends to sub-cutaneous tissue, formerly 3 rd and 4th degree) (25). Microscopic examination of burns can be used in order to observe and assess the degree of damage; erythema, blistering, necrosis, and charring (in dry burns, not scalds) are the key histologic features that can aid in determining vitality, the degree of damage, and/or the age of the injury.
In tissues (including skin), evidence of vitality can be seen by the presence of an inflammatory reaction in a blister chamber, in the papillary stratum and superficial cornium, by the presence of fibrin in the blister chamber, and by reactive hyperemia and edema; furthermore, the presence of massive intravascular concentration of Sudan III-positive fats can also be regarded as a vital sign (23). See Dettmeyer’s Heat, Fire, Electricity, Lightning, Radiation, and Gases in Forensic Histopathology for a summary of histopathological findings (21).
Histologic findings of burn shock may also be seen, particularly if there is a survival interval. Such findings correspond, more or less depending on etiology, to the histopathologic findings in other types of shock. Changes can be seen in the lungs, heart, brain, pancreas, gastrointestinal tract, kidneys, adrenal glands, and liver (23).
Late changes in deaths due to thermal injury will depend on the immediate cause of death: sepsis, respiratory insufficiency, systemic inflammatory response syndrome, organ system failure, and so on.
Electricity: Lightning and Electrocution
Whether by lightning or electricity, the possible mechanisms of death from electrocution are the same: cardiac dysrhythmia due to passage of current through the heart, respiratory paralysis due to spasm of intercostal muscles and diaphragm from passage of current through the chest and abdomen, or paralysis of cardiac and/or respiratory centers in the brainstem from passage of current through the head (16). Regardless of the mechanism, the forensic pathologist seeks evidence that death occurred due to electrocution rather than some other cause. Histological evidence of electrocution is usually present, is straightforward to identify, and can be striking to behold (pardon the pun).
Depending on the nature of the source of electricity (e.g., voltage, amperage, current type) and the characteristics of the entry and exit points on the skin (e.g., surface area, wet or dry, etc.), there may be tell-tale gross and histologic signs of electrocution on the skin. The macroscopic features of electrical burns of the skin are well described in forensic textbooks and in the archival literature.
Sampling of electrical burns should include both the injured lesion and the surrounding unchanged skin and subcutaneous soft tissue; at the very least, comparison of normal and injured skin will assist interpretation. The typical histologic features of electrical burns are easily recognized by classically trained surgical pathologists as cautery artifact, introduced in surgical procedures, is commonly seen in surgical specimens (Images 5 and 6). This should not be surprising as heat generated for surgical cautery is, in modern day medicine, electrically generated.
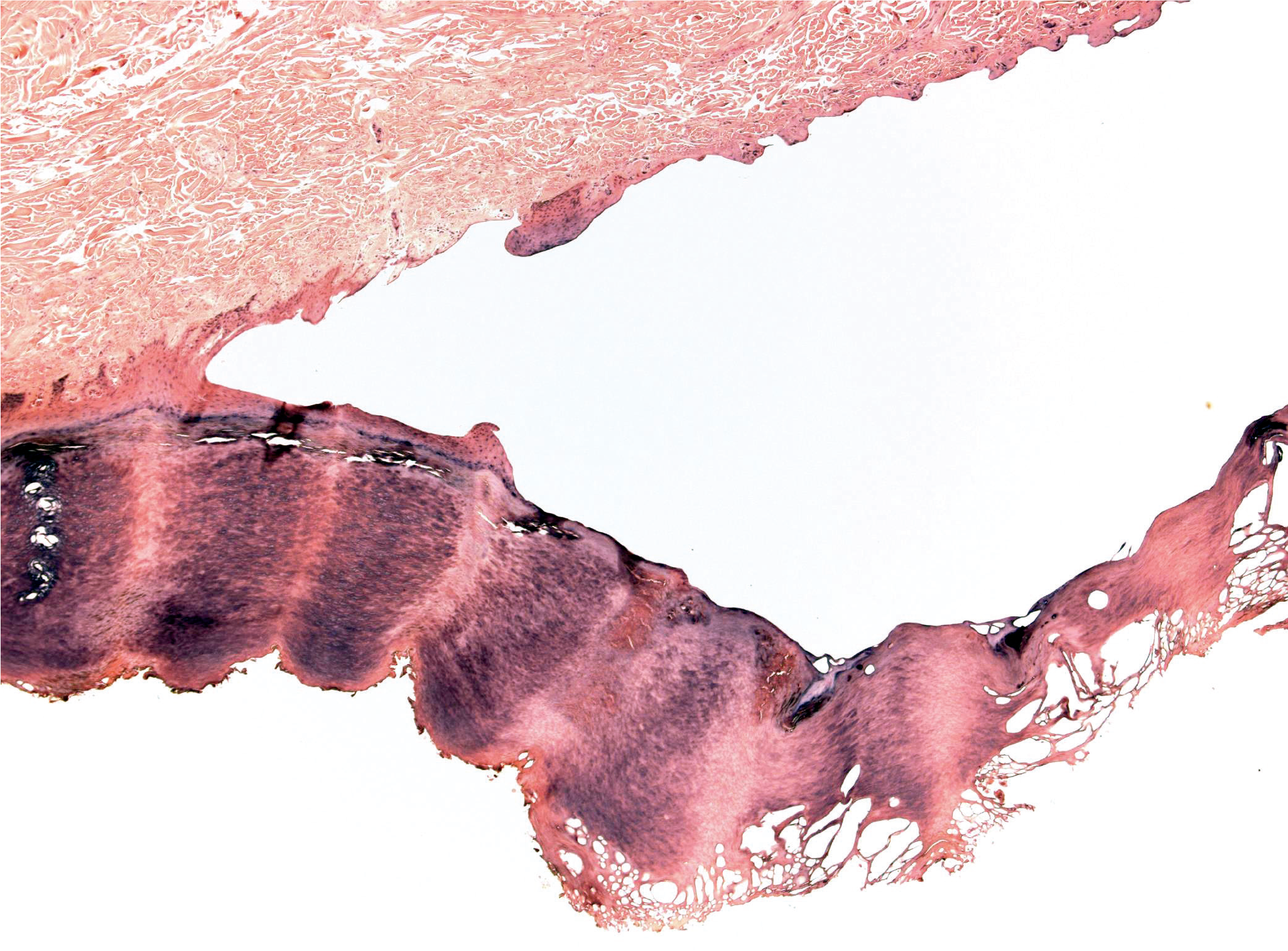
Low power view of an electrical burn of the skin of the sole of the foot; an intraepidermal blister, obliteration of the epidermis and basket-weave-like changes of the keratin layer are seen (H&E, x40).
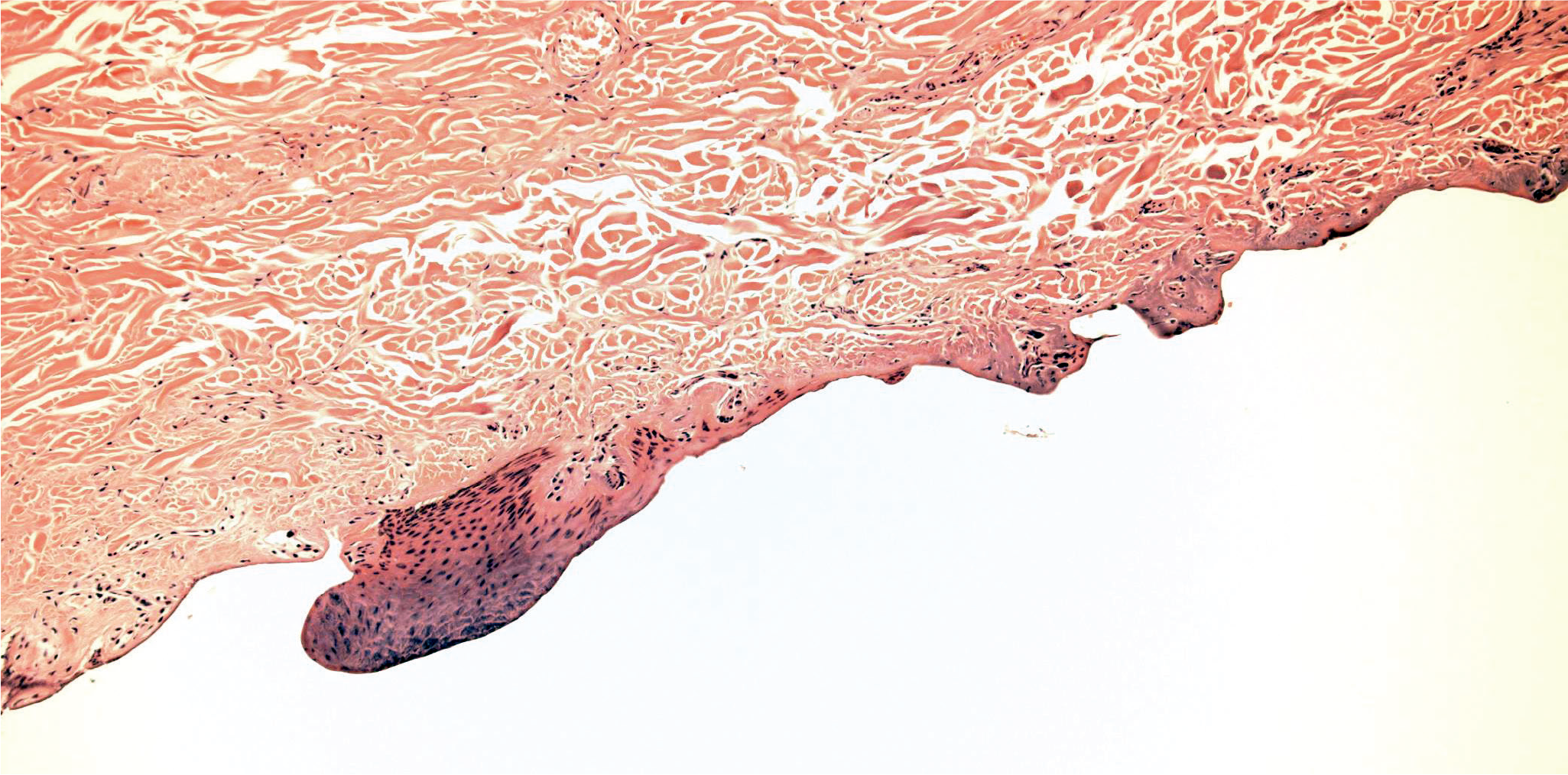
High power view of the same region shown in
In a comparison of electrical burns and flame burns (and abrasions), the features of intraepidermal separation, subepidermal separation, coagulation necrosis, epidermal nuclear elongation, dark nuclear staining, and depth of intraepidermal separation were compared in 30 samples of electrical burns and 30 samples of flame burns in an attempt to determine specific identifying features. Some trends were identified, but pathognomonic changes were not (26). Electrical metalization, deposition of black particles from the electrical conductor, may also be seen. The heat-related changes in the collagen due to electrical burns, such as thickening of the supepidermal collagen bundles, may be highlighted using Masson trichrome stained slides where the heated collagen will also stain red, in distinction from unaffected collagen that will remain blue-green (Image 7).
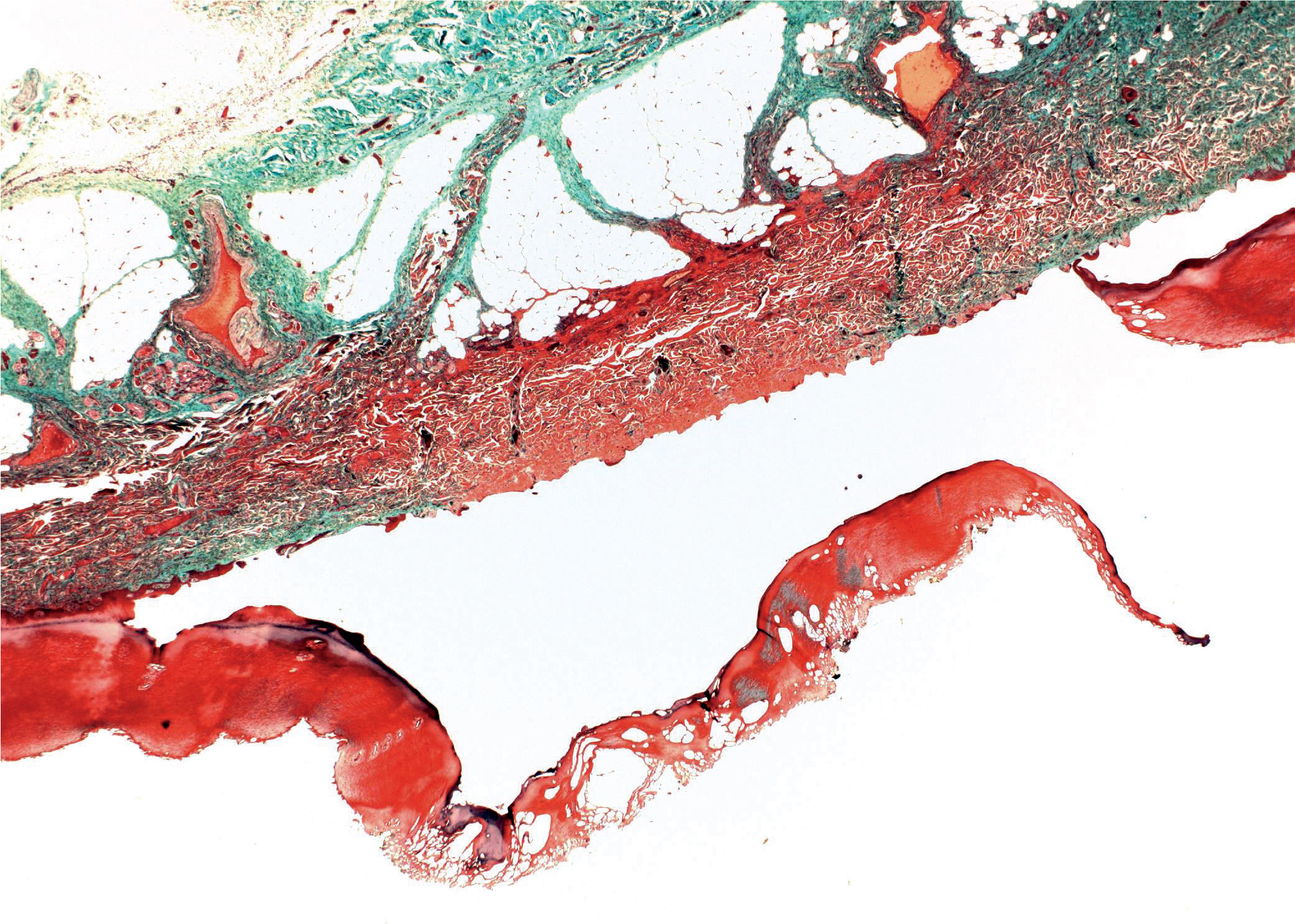
Special stained low power view of an electrical burn; red coloration of subepidermal collagen highlights the regions where heat changes were greatest as well as the depth of heat effects (in this case, to the subcutaneous fat) (Masson trichrome, x20).
Specific histologic evidence of cardiac dysrhythmia due to electrical shock will not be found; it is uncertain whether histopathologic changes of the myocardium could be solely attributed to electrical injury. Likewise, features of rhabdomyolysis, purportedly due to electrically induced muscular spasm might not be definitively attributed to electrocution.
Finally, it is possible that electrocution causing death may not create any gross or microscopically identifiable lesion even after careful examination of the body.
Water: Drowning, Dysbarism, and Hypothermia
Drowning
Histopathologic diagnosis of drowning is the most precarious of the environmental deaths; there are no pathognomonic gross or microscopic features of drowning. Diagnosis of drowning is made based upon history, absence of competing causes of death, and presence of supporting evidence at autopsy such as wet clothes, sodden appearing hands and feet, heavy and hyperinflated lungs, frothy fluid in the airways, stomach with hemorrhagic gastropathy and watery contents, and water in the sinuses of the skull. A sure conclusion was drawn by Bernard Knight when he wrote: Much has been written about both light and electron microscopy of the lungs in immersion deaths…The accounts are confusing, however, and sometimes contradictory, the consensus of opinion being that such changes are inconsistent and unreliable (27).
This conclusion can be extended to microscopy of every organ system in drowning.
Dysbarism
Dysbarism, defined as disease that results from changes in ambient pressure, includes decompression sickness and pulmonary barotrauma related to a too-rapid ascent from a dive underwater; effects related to high-altitude and aerospace endeavors are also included in the term. However, deaths due to pressure effects in high altitude activities are vanishingly rare; it is more common that deaths are due to descent from height.
In decompression sickness, a reduction in ambient pressure during ascent following a dive allows release of dissolved gases (primarily nitrogen) into the blood and tissues; the gases then form bubbles that cause disease by disrupting cell function, activating the coagulation cascade, and interrupting blood circulation (28). While decompression sickness is a common cause of morbidity among divers, it is a rare cause of death except in its most severe form of arterial gas embolism. When death does occur, rapid body recovery and transport for autopsy is necessary to permit observation of the formed bubbles. Furthermore, postmortem decompression (or off-gassing), resuscitation, and decomposition are common additional sources of artifactual gas at autopsy. Therefore, gross or microscopic identification of gases observed at autopsy cannot be unquestionably confirmed as being due to decompression sickness. Decompression sickness is categorized by the severity of its symptoms: type 1 (mild), type 2 (serious), and arterial gas embolism. The final of these is also called pulmonary barotrauma (29, 30).
In pulmonary barotrauma, reduced ambient pressure allows expansion of gases in the lungs that, if not exhaled, traumatically escapes from the bronchiolar and alveolar tree into the pulmonary circulatory system; arterial gas embolism can affect any system in the body including, critically, the coronary arteries and the cerebral arteries. Unfortunately, as mentioned before, gross or microscopic findings may not be definitively attributed to gas formation related to the environment. Furthermore, there is often also evidence of drowning as an agonal event, despite the commonly given history of a diver who ascends/surfaces rapidly and then loses consciousness within minutes (31).
Hypothermia
For bodies recovered from water, the cause of death may be hypothermia. The findings in hypothermia, described above, may be found in addition to signs of immersion (or signs of drowning). Given that the gross and microscopic findings of both entities are nonspecific, it can be difficult to determine a precise cause of death; histologic sections may be noncontributory. Scene, history, and circumstances should inform interpretation of autopsy findings.
Conclusion
Deaths in a hostile environment may present quandaries to the autopsy pathologist; some cases declare themselves while others may have no tell-tale evidence. Histologic evidence may be sought and found; it might even form additional evidence that supports a cause of death that arises from scene, circumstances, and history. That being said, many cases of deaths in a hostile environment do not generate any distinctive or pathognomonic histologic findings.
Footnotes
Ethical Approval
As per Journal Policies, ethical approval was not required for this manuscript
Statement of Human and Animal Rights
This article does not contain any studies conducted with animals or on living human subjects
Statement of Informed Consent
No identifiable personal data were presented in this manuscript
Disclosures & Declaration of Conflicts of Interest
The authors, reviewers, editors, and publication staff do not report any relevant conflicts of interest
Financial Disclosure
The authors have indicated that they do not have financial relationships to disclose that are relevant to this manuscript