
Abstract
Spontaneous hemoperitoneum is rare and is often labeled as idiopathic because the source of bleeding is never found. We report the case of a 35-year-old male who died of a splenic vein rupture. The decedent was a chronic alcoholic with a reported history of cirrhosis and medication noncompliance. Internal examination revealed pale visceral organs, marked hemoperitoneum, a fibrotic/nodular liver, esophageal varices, and a ruptured splenic vein. Pertinent microscopic findings include liver parenchyma with bridging fibrous septa, nodules of regenerating hepatocytes, and the presence of Mallory-Denk bodies. The immediate cause of death was determined to be splenic vein rupture with the underlying cause of death being chronic alcoholism. This case is reported to emphasize the importance of correlating past medical history with thorough vascular dissection in cases of spontaneous hemoperitoneum. In a patient with fatal hemoperitoneum and risk factors for splenic vein pathology (ie, cirrhosis, portal vein hypertension), a high suspicion should be kept for splenic vein rupture.
Introduction
Trauma to the abdomen can often cause hemoperitoneum if rupture of a major vessel or vascular organ occurs. Based on the location of the injury, the source of the bleeding can likely be found and treated. On the other hand, spontaneous hemoperitoneum (also known as abdominal apoplexy or idiopathic spontaneous intraperitoneal hemorrhage) can be more difficult to manage therapeutically as there are no obvious external or internal guides to the source of bleeding. Unfortunately, spontaneous hemoperitoneum is often fatal and death can come rapidly with surgical teams never finding the hemorrhaging vessel. An autopsy, sometimes the last hope for uncovering the final diagnosis, can also come up short with no clear answer as to the source of bleeding even after careful dissection (1).
Since the 1930s when the term “abdominal apoplexy” was first coined there have been several conditions found to be associated with it, including vascular disorders (ruptured visceral aneurysm, ruptured utero-ovarian vessels), gynecological disorders (ruptured gravid uterus, ectopic pregnancy), and liver cirrhosis with portal hypertension (leading to ruptured varices) to name a few (2-4). As a cause of hemoperitoneum and as a general condition, spontaneous splenic vein rupture (SVR) is rare. Major and minor trauma to the spleen is well-documented and these injuries can often lead to splenic rupture and consequently hemoperitoneum (5). In contrast, reports related to hemoperitoneum secondary to spontaneous rupture of splenic vessels—more specifically the splenic vein—are hard to come by. Forensic literature regarding SVR is sparse (2). In broader medical literature, reports on spontaneous SVR are also quite scant but when found it is often seen associated with either cirrhosis or pregnancy (6-9).
We report a case of a 35-year-old male, with a history of chronic alcoholism, who was found dead on the porch of a friend's residence. The friend found the decedent supine, unresponsive, not breathing, and with adjacent vomitus. The emergency medical team confirmed asystole on the scene. Law enforcement noted that the decedent was “cold to the touch with rigor mortis.” Upon questioning, investigators discovered that the decedent was a homeless person without shelter and would often sleep on his friend's porch. No trauma was noted and law enforcement had no suspicion of foul play. The family and friend informed investigators that the decedent was a heavy drinker and was diagnosed with cirrhosis, but he declined any treatment and was not adherent to the medications that he was prescribed. On the day of his death, there was no one who reported seeing him drinking alcohol.
Methods
Prior to performing the autopsy, the departmental case summary report was reviewed. This report included the terminal event/circumstances, medical history, social history, medications, time of death, place of death, as well as the investigator assigned to the case. Once reviewed, an external/internal examination was performed followed by evisceration using the Ghon or “en bloc” technique; this allowed for more thorough assessment of the abdominal vessels. After this, the organs were weighed, examined, and sectioned. Representative sections of the heart, lungs, and liver were taken for microscopic examination.
Results
During external examination, the body was that of a well-developed and nourished adult man. The decedent had a medium body build, weighed 179 pounds, and was 5 feet 8 inches tall (BMI was 27.2 kg/m2). The body was unremarkable with no evidence of external trauma or source of bleeding.
During internal examination, the thoracic evaluation was unremarkable. The heart weighed 320 g and coronaries had normal caliber with no atherosclerosis. The right and left lungs weighed 430 and 480 g, respectively, and had no discrete lesions or areas of consolidation. The abdominal evaluation yielded the most significant diagnostic information. The visceral organs were mildly pale. The peritoneal cavity had a measured collection of approximately 4 L of blood (
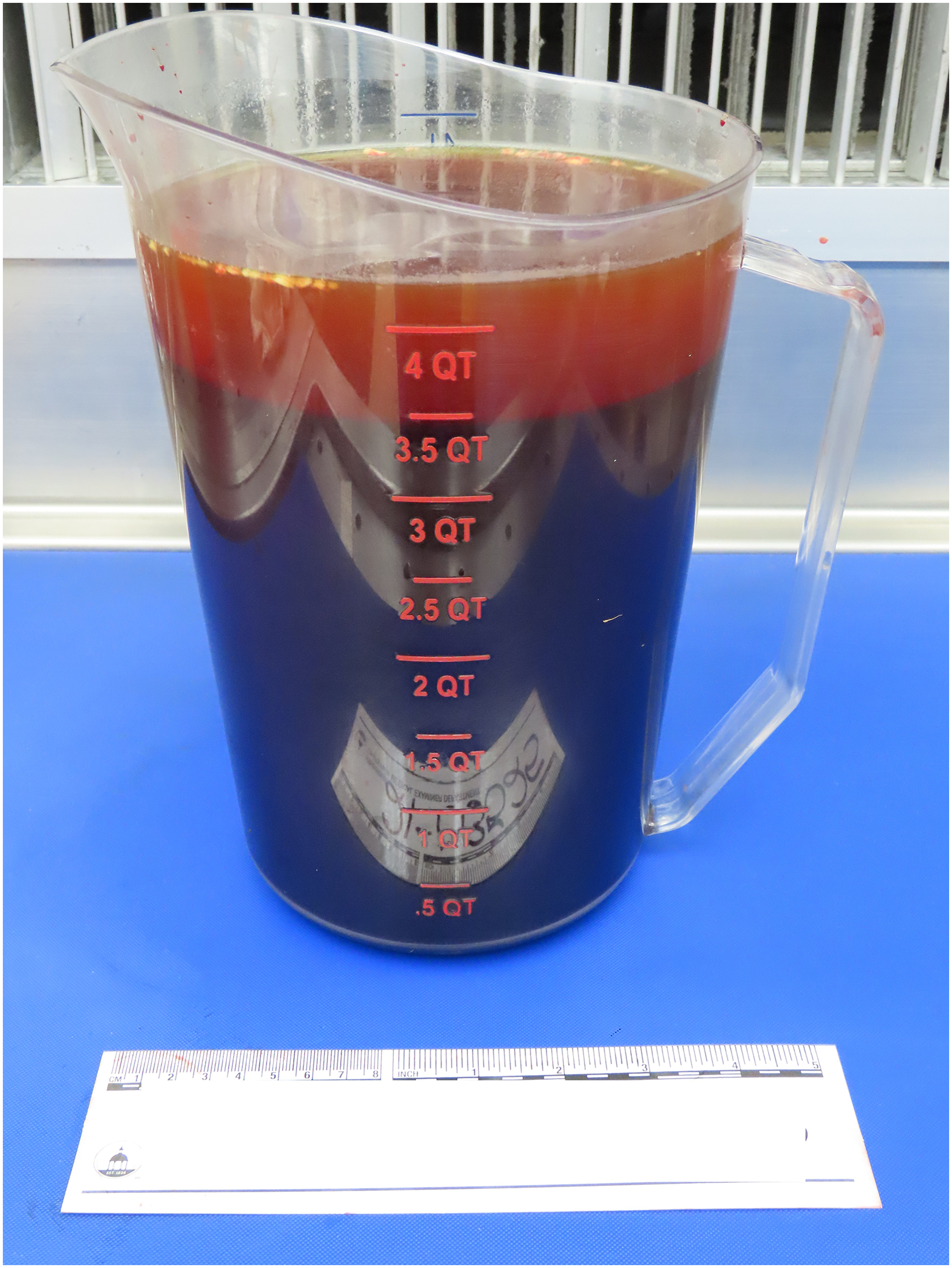
Approximately 4 L removed from the abdominal cavity.

Cirrhotic liver with fibrotic and nodular capsule.
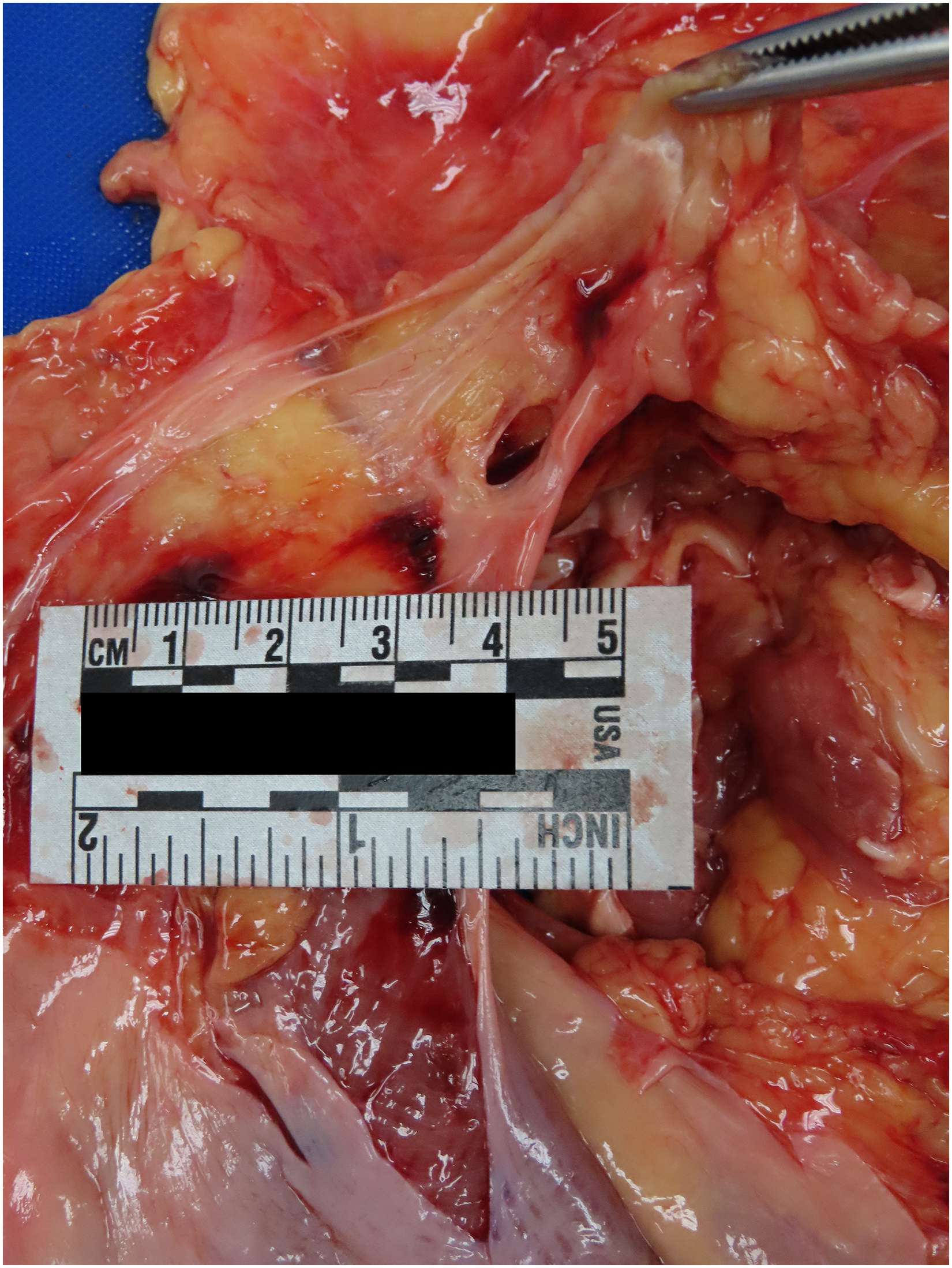
Splenic vein rupture.

Unruptured esophageal varices at distal esophagus.
Microscopic examination of heart revealed early autolysis and rare nuclear features of myocyte hypertrophy but no inflammation or infarction. The lung examination revealed anthracotic pigment deposits, patchy atelectasis, and few bronchi/bronchioles containing inspissated mucus. Microscopic examination of the liver revealed bridging fibrous septa with scant lymphocytic infiltrate and roundish parenchymal nodules of regenerating hepatocytes (
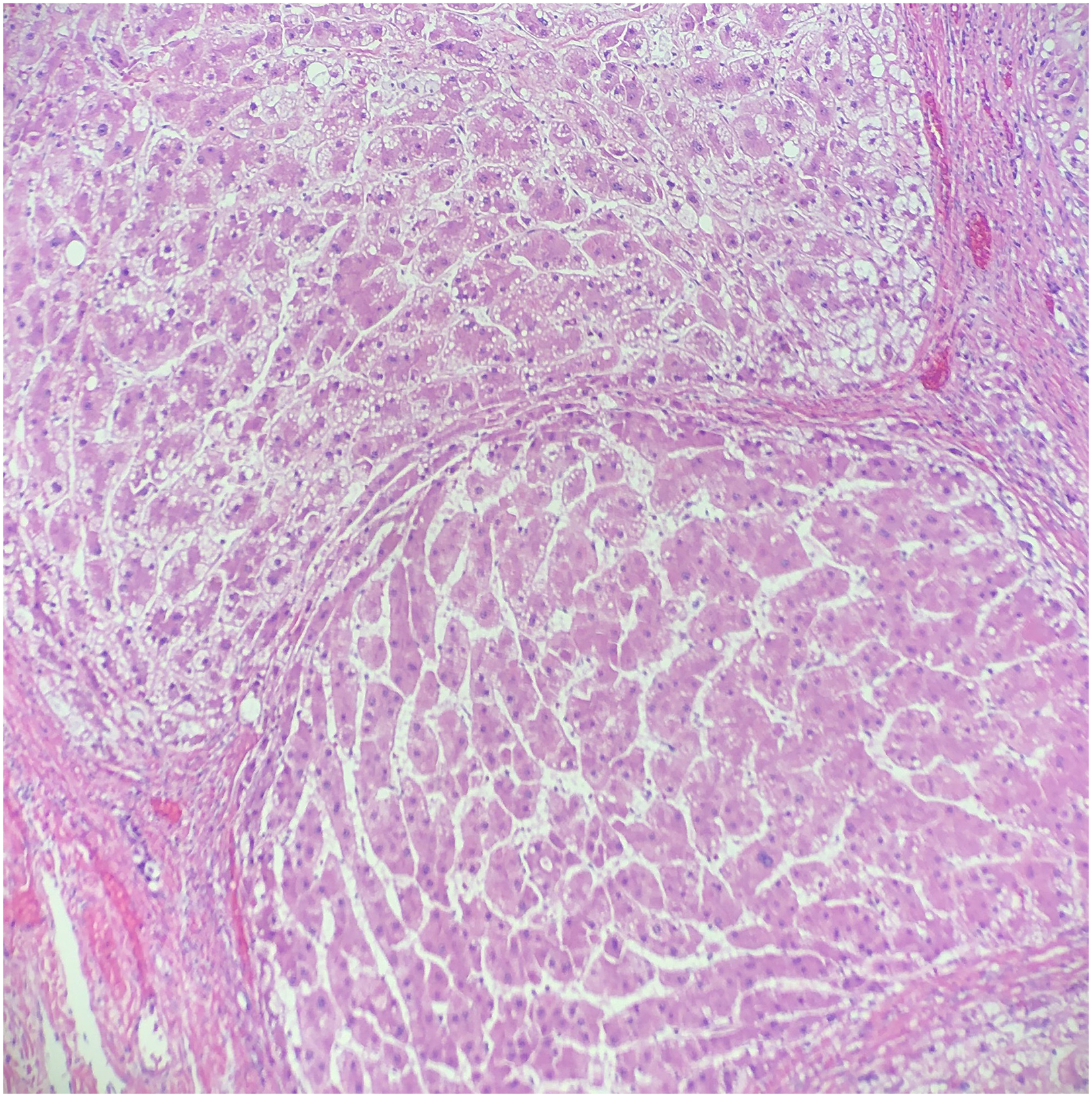
Microscopic examination of the liver (H&E, 100×). Bridging fibrous septa with scant lymphocytic infiltrate and roundish parenchymal nodules of regenerating hepatocytes.
Discussion
To better understand the cause of SVR, and those at risk for it, general knowledge of splenic vein pathology (and their respective risk factors) is imperative. Uy et al lays out five main vascular diseases of the splenic vasculature: splenic vein thrombosis (SVT), splenic vein aneurysm (SVA), splenic artery aneurysm, splenic arteriovenous fistula, and spontaneous splenorenal shunt (10). Splenic vein thrombosis is often complicated by gastric varices and upper GI bleeding; in catastrophic cases it can even lead to splenomegaly and splenic rupture. Splenic vein aneurysm, a rare entity, is often complicated by SVR (along with other sequelae—thrombosis, obstructive jaundice). Splenic vein aneurysm is considered to be most commonly caused by portal hypertension. Elevated portal pressures lead to vessel wall changes that ultimately result in fibrosis and aneurysm formation (7). Although there are cases of SVA that do not involve portal hypertension, when the etiology is unclear it likely suggests weakness in the vessel wall of some sort—whether acquired or congenital (6). Splenic vein aneurysm is an easy diagnosis to place on one's differential for SVR but there are several articles of vein rupture that show no evidence of SVA. Pregnant women who fall victim to spontaneous hemoperitoneum may provide further clues behind other causes of SVR. There are several cases in medical literature of pregnant women, typically in their third trimester (9), dying from SVR as well as rupture of utero-ovarian vessels. Several theories have been proposed for what may predispose pregnant women to vessel rupture and they include (1) physiological increase in blood flow combined with sudden increase in intravenous and intra-abdominal pressure (3) and (2) progesterone-induced vasodilation and vessel wall weakness (7).
In this case, the decedent was a male who had no known prior history of splenic vein pathology (ie, SVT or SVA) and no SVT or SVA was reported on autopsy. There were no signs of splenic rupture. The spleen was 160 g and had a smooth intact capsule with normal underlying parenchyma. The only vascular findings were portal vein dilation and SVR with adjacent hemorrhage. It is noted that in some cases of hemoperitoneum, particularly in that of chronic hemorrhaging prior to the acute exsanguination, an area of hematoma can be found nearby the source of bleeding (2,4,6,9,11). In this case, no discrete or obvious area of hematoma was noted. Other than the SVR, the decedent's history of chronic alcoholism/cirrhosis and the gross finding of a cirrhotic liver and portal vein dilation were the only potential clues that could lead the examiner toward higher suspicion of the splenic vein as the cause of bleeding. Cirrhosis and portal vein dilation (suggestive of portal vein hypertension) would contribute toward the hemodynamic and the structural venous wall changes that could lead to a weakened splenic vein. Of note, in several cases of spontaneous hemoperitoneum where the bleeding source is not found there is often a cirrhotic liver present (1).
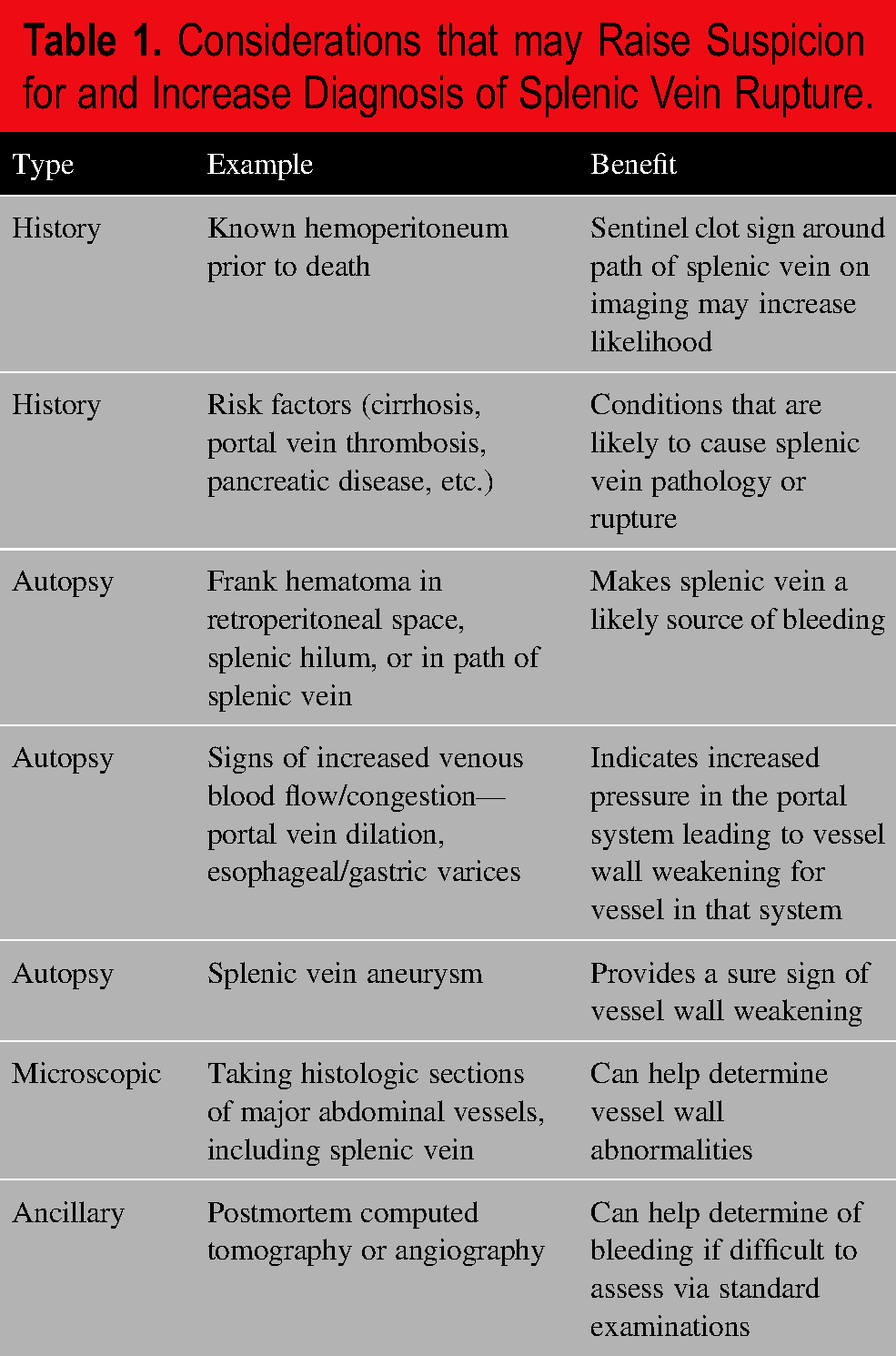
In cases of hemoperitoneum, a SVR should be considered if there is history of cirrhosis. Although it is possible that many cases of spontaneous hemoperitoneum are idiopathic, it may also be possible that in populations of decedents with cirrhosis a discrete SVR is being missed when there is not high enough suspicion. We recommend several considerations (
Considerations that may Raise Suspicion for and Increase Diagnosis of Splenic Vein Rupture.
Conclusion
In this case, the decedent had historical, macroscopic, and microscopic findings that contributed to the determination of the immediate and underlying cause of death. Fortunately, the rupture of the splenic vein was readily found with careful standard examination. Forensic literature has shown that the source of spontaneous hemoperitoneum is not always readily found. Yet, in several reported cases the decedents are found to have a history of cirrhosis. In the case of decedents with history of chronic alcoholism and/or cirrhosis, careful considerations before, during, and after autopsy may lead to fewer idiopathic diagnoses and more discoveries of spontaneous SVR leading to fatal hemoperitoneum.
Footnotes
DECLARATION OF CONFLICTING INTERESTS
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
FUNDING
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors