
Abstract
Background
Tension pneumothorax is a life-threatening condition in trauma patients requiring rapid recognition and treatment. Needle thoracostomy (NT) is a critical prehospital intervention to treat this condition.
Objective
To evaluate prehospital NT performance through medical examiner (ME) assessment of anatomical placement, pleural space access, and complications in prehospital nontransported traumatic cardiac arrest patients.
Methods
A prospective observational study reviewed 144 prehospital NTs performed on 77 patients after initial emergency medical service (EMS) care from 01 February, 2022 to 16 June, 2024. NTs were evaluated during autopsy for placement within recommended external anatomical landmarks, pleural space entry, and evidence of complications. EMS documentation was reviewed to correlate findings.
Results
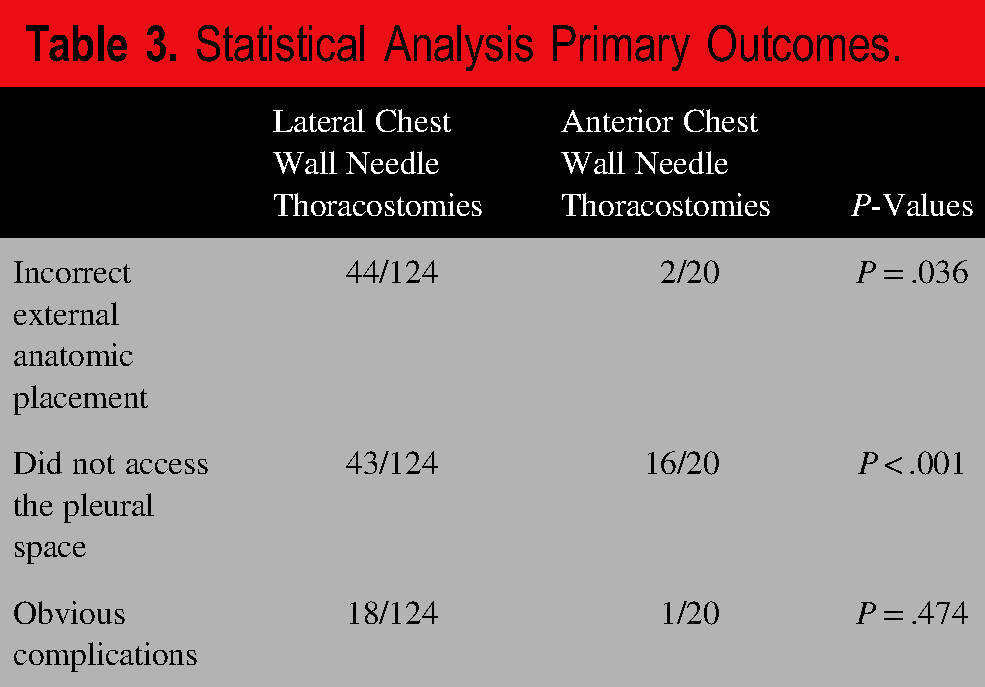
Of 124 lateral chest wall NTs, 35.5% were outside of recommended anatomic landmarks and 34.6% did not access the pleural space, with a 14.5% complication rate. Among 20 anterior chest wall NTs, 10% had incorrect external placement and 80.0% did not access the pleural space, with a 5.0% complication rate. When comparing lateral chest wall NTs to anterior chest wall NTs the difference in correct external placement (P = .036) and pleural access (P < .001) were statistically significant but the complication rates (P = .474) were not.
Conclusion
Autopsy-based review provides valuable insight into the real-world performance of prehospital NTs. Lateral chest wall NTs have high rates of incorrect external anatomic placement but more often access the pleural space as compared to anterior chest wall NTs. Complications are rare overall. This collaborative model between the ME and EMS can identify trends and challenges, inform training, guideline development and system-level improvements.
Keywords
INTRODUCTION
Tension pneumothorax (T-PTX), a treatable, potentially life-threatening condition where pressure in the pleural space leads to cardiovascular and respiratory compromise. Tension Pneumothorax has a variable incidence in literature based on the studied population but has been noted to be as high as 30% in some populations. 1 T-PTX is typically treated in the prehospital setting with needle thoracostomy (NT), whereby a needle is inserted into the pleural space to relieve pressure. This procedure has been shown to be performed in as many as 1.7% of transported prehospital patients. 2
The decision by an emergency medical service (EMS) clinician in the prehospital setting to treat a T-PTX is difficult due to the traditionally taught, but rarely detected, clinical findings (decreased breath sounds, tracheal deviation, and jugular venous distention) being over emphasized in education compared to vital sign abnormalities (tachycardia, hypoxia, and hypotension) that are more often present in T-PTX patients. 1 Even when the procedure is indicated, proper needle placement can be challenging. Historically, the anterior chest wall was utilized as the preferred external anatomical location for NT. In 2018, Advanced Trauma Life Support incorporated the lateral chest wall as an alternative location. This addition was due to documented failure of pleural space access anteriorly as well as less subcutaneous tissue in the lateral chest. 3 Either procedural approach requires careful consideration of anatomic landmarks, appropriate needle size and length, and the correct procedural steps due to an ever increasingly heterogenous population habitus within civilian EMS. Finally, once the needle penetrates the skin, iatrogenic complications from lung and vascular injury that can induced bleeding, PTX, and visceral organ damage, to include the heart may occur.4,5
Despite these barriers, prehospital placement of NT is potentially lifesaving. In the appropriate patient population, prehospital NT is associated with a lower 24-h mortality. At the same time, a large study by Muchnok et al noted that 89% of potentially eligible patients did not receive a prehospital NT of which highlights the difficulty of prehospital identification of procedural need. 6 Given the critical nature of the procedure in a large portion of prehospital trauma patients, understanding the accuracy and efficacy of the procedure by all levels of medical providers is important. To date, studies evaluating external placement and internal accuracy of NT have been largely limited to nonprehospital settings, anterior chest wall approaches, and radiographic evidence, which may present limitations. 7
This article presents a novel process of engagement between the medical examiner (ME) and a large, metropolitan fire-based EMS system in evaluating NT placements in prehospital traumatic cardiac arrest patients who did not survive to the emergency department and were thus not transported. Specifically, this study aimed to provide detailed evaluations of NT placement, outlining findings with relation to proper placement using external anatomic landmarks, pleural space entry, and iatrogenic injury.
METHODS
This was a prospective observational study that was approved by the Medical College of Wisconsin Institutional Review Board. ME and EMS data on identified patients from 01 February, 2022 to 16 June, 2024 were included. The Milwaukee County ME Office and the Office of Emergency Management were both involved in data collection. The County's EMS system is a large, metropolitan EMS system in the United States. The County has a population of approximately 920 000 and is served by a fire-based EMS system, with approximately 115 000 patient encounters per year. The EMS system utilized a standard 14-gauge, 3.25-inch nonfenestrated catheter over needle for all NT procedures. Inclusion criteria for data evaluation included deceased trauma patients who were not transported to the hospital, had a prehospital NT performed by Milwaukee County EMS, and were evaluated by the Milwaukee County ME office. These patients were entered into a secure database that utilized the EMS Electronic Patient Care Record to identify patient demographics, mechanism of injury to include blunt versus penetrating, and side of NT performance. The ME completed a secure online form within the same database to document NT details in real time. Collected variables including patient height and weight, side of injury, and the cause and manner of death were completed following case completion. Patients excluded from data analysis were patients with no ME evaluation completed, incomplete ME evaluation data, and patients under the age of thirteen due to the adjustment in NT procedure and equipment within the EMS system for this age group.
The ME evaluated all NT placements. The specific details of the NT gathered by the ME included the external anatomic location of the NT, if the pleural space was accessed, and visualization of obvious complications specified as either lung parenchymal injury, cardiac injury, diaphragmatic injury, major vessel injury, intra-abdominal injury, or other inadvertent NT placements. The correct anatomic location was defined as in th second intercostal space midclavicular line for anterior placement. Similarly, lateral chest wall NTs were reviewed for correct anatomical placement, which was defined as placement between the third to fifth intercostal space between the mid to anterior axillary line. The ME obtained additional information to clarify why the NT was in the wrong location for the anterior chest wall (too superior, inferior, medial, or lateral) as well as the lateral chest wall (too superior, inferior, medial, or posterior). For all NT placements, the ME obtained the exact intercostal space or whether the NT was placed within the borders of the cardiac box (which was defined as the area between the mid-clavicular lines, the sternal notch, and the xiphoid process). Importantly, visuals were provided for clarification to the reviewer within the secure online form as to the correct anatomical landmarks outlined above.
The ME collection of this data included the following processes. An external examination was performed to determine the external location on each decedent where the NT was placed through the skin. The NTs were kept in place while a “Y” shaped incision was performed over the chest and abdomen, followed by removal of the anterior ribcage. Once the thoracic cavity was accessed, further visual inspection was carried out to determine if the catheter was within the chest cavity, and if so, to identify the point of entry. Further inspection was performed to determine if any damage had occurred to adjacent structures by evaluating for puncture marks consistent with an NT or hemorrhage within surrounding tissues.
Statistical analysis included the calculation of frequencies and descriptive statistics for all data. For the lateral and anterior chest wall, NTs were compared regarding placement, access to the pleural space, and obvious complications using a Fisher's exact test. To account for patients potentially having more than one procedure performed, mixed effects logistic regression was used to test if BMI predicted incorrect placement (1 = incorrect, 0 = correct), not accessing the pleural space (1 = did not access the pleural space, 0 = accessed the pleural space), and obvious complications (1 = obvious complications, 0 = no obvious complications); odds ratios and 95% confidence intervals were calculated. The package lme4 was used with R version 4.3.1. 8 For all data statistical significance was set at P-values <.5.
RESULTS
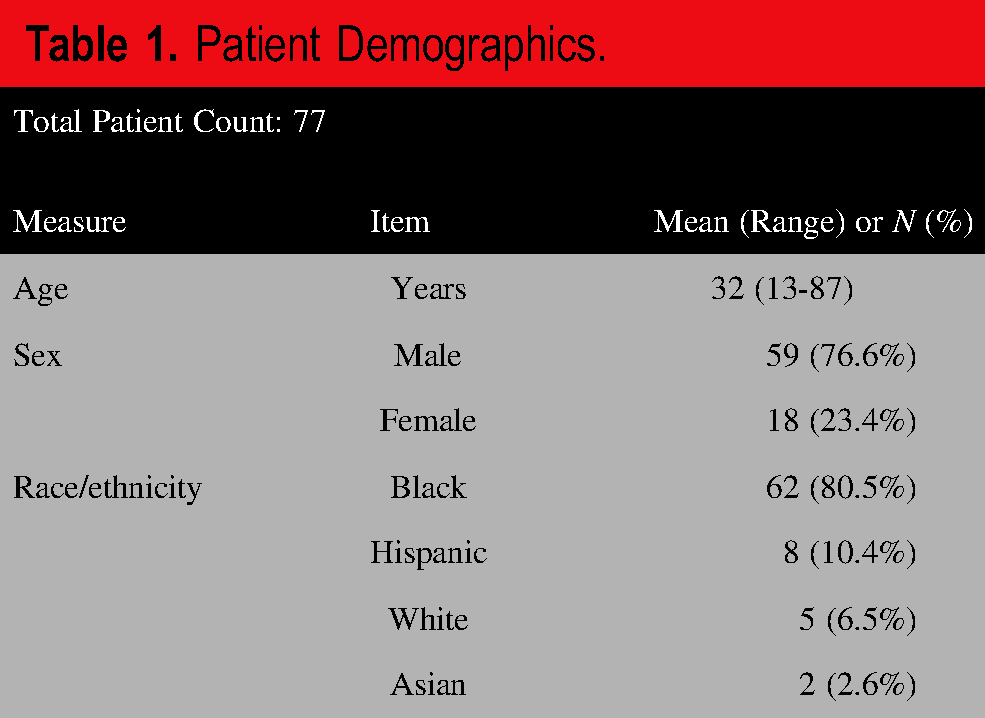
One hundred and thirty-one patients met the inclusion criteria during the study time frame. Fifty-one patients were removed because no ME data was collected, one patient under the age of 12 was removed because the EMS procedure for NT is different for pediatric patients, and two patients were removed for incomplete data, which resulted in 77 total patients for evaluation (Figure 1). The demographics of evaluated patients are outlined in Table 1.
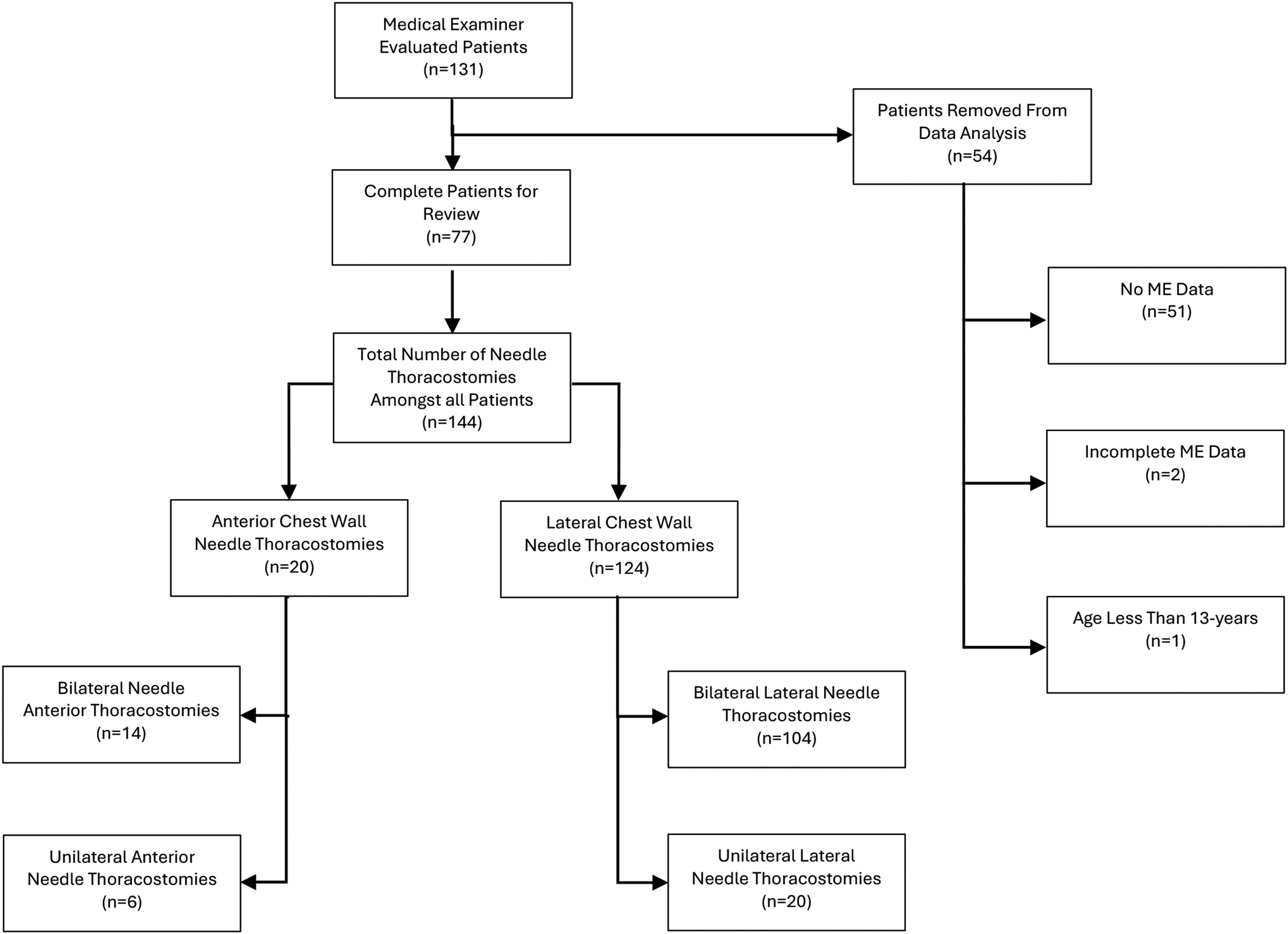
Inclusion/exclusion and origin of all needle thoracostomies.
Patient Demographics.
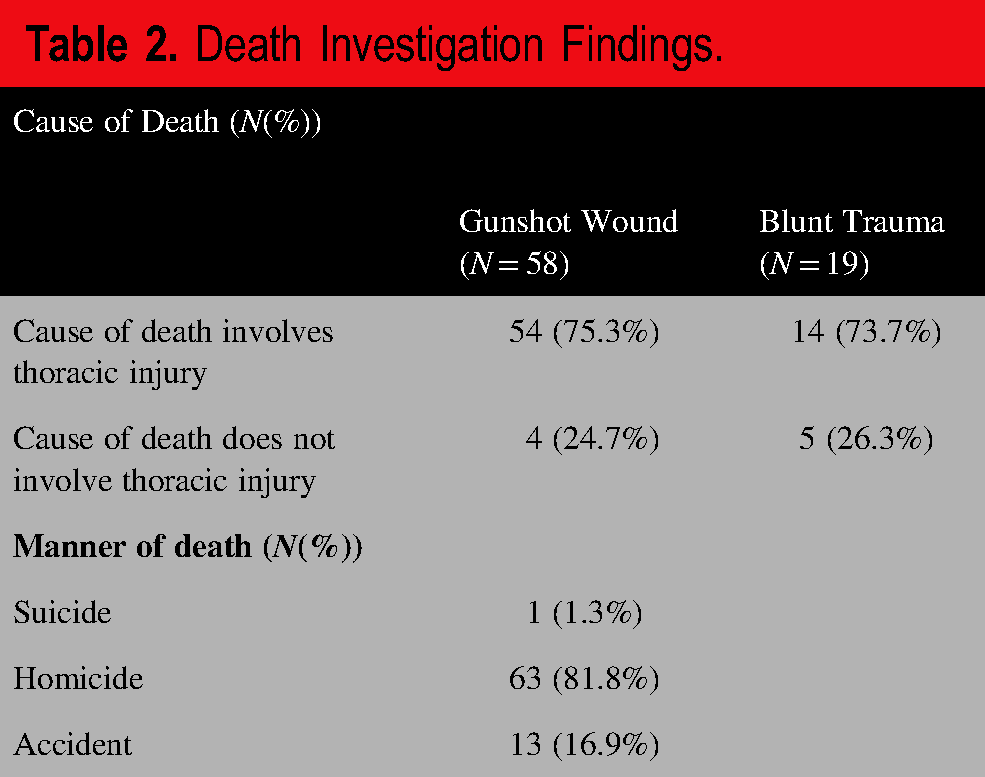
The death investigation findings are outlined in Table 2. Specifically, the manner of death for all patients was most commonly homicide, accounting for 63/77 (81.8%) cases. The most frequent cause of death was gunshot wound, which occurred in 58/77 (75.3%) cases. In 9/77 (11.7%) cases, the cause of death did not involve thoracic injuries (Table 2).
Death Investigation Findings.
Among 77 patients, there were a total of 144 separate NT procedures evaluated due to most patients having multiple NT procedures performed. This included 124 lateral chest wall NTs and 20 anterior chest wall NTs. Within the lateral chest wall group, 20 patients had unilateral procedures, and 52 patients had bilateral procedures. In the anterior chest wall group, 6 pateints had unilateral procedures, and 14 patients had bilateral procedures (Figure 1).
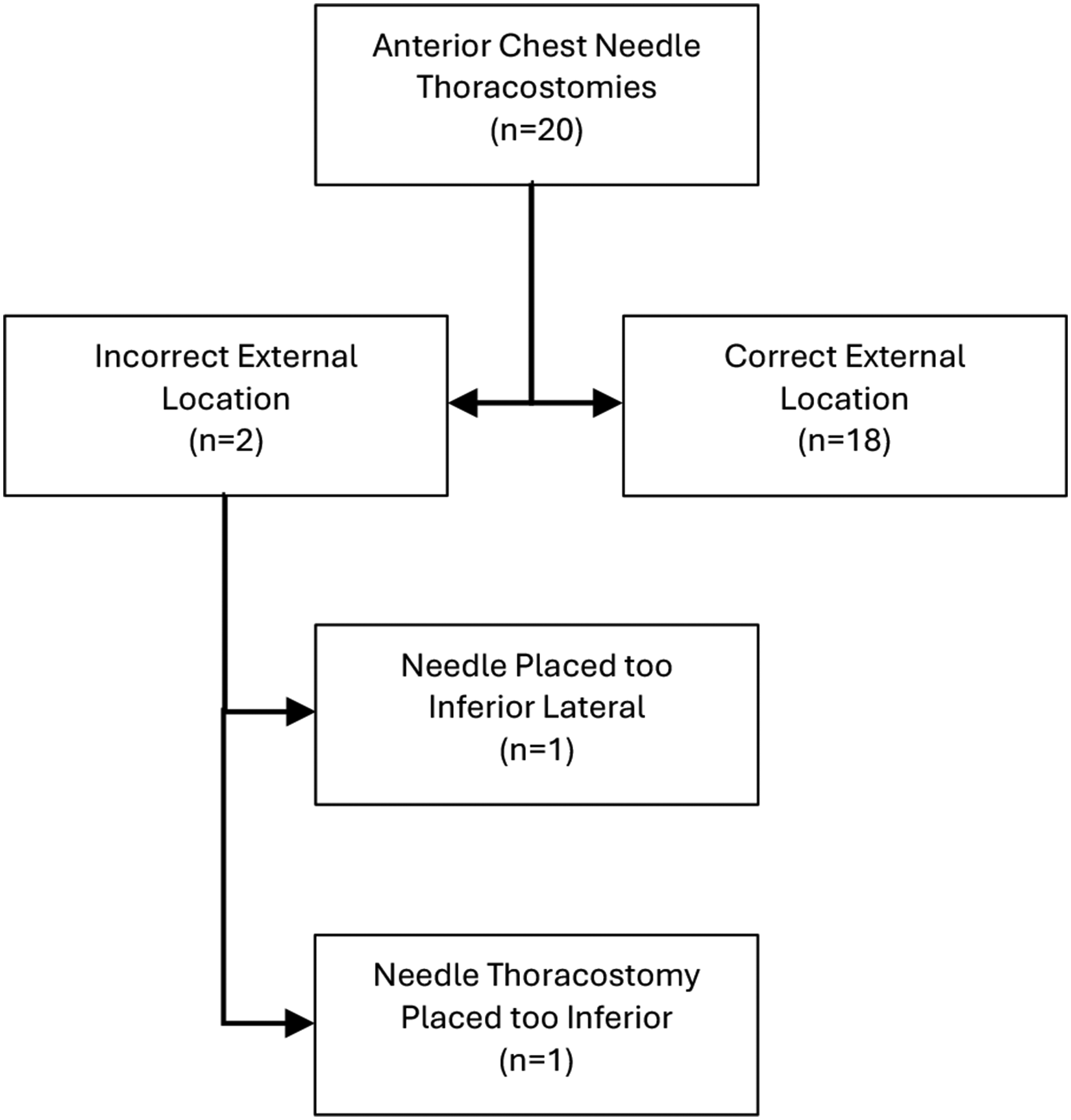
Across all NTs, 46/144 (31.9%) cases had incorrect external anatomic placement. As outlined in Figure 2 denoting the combined external anatomical placement of lateral chest wall NTs, 44/124 (35.5%) of cases had incorrect external anatomic placement in either or both of the evaluated dimension (Figure 2). Among incorrectly placed lateral chest wall NTs, 22/44 (50%) were isolated to the incorrect superior-inferior location, 11/44 (25%) were isolated to the incorrect anterior-posterior location, and 11/44 (25%) were in both the incorrect superior-inferior and anterior-posterior location (Figure 2). As outlined in Figure 3, of the procedures that were too inferior, 7/30 (23.3%) were below the seventh intercostal space. Among those placed too posterior, 4/22 (18.2%) were posterior to the posterior axillary line (Figure 3). By contrast, as outlined in Figure 4 describing the anatomical placement of anterior NTs cohort, 2/20 (10%) were placed in the incorrect external anatomic location (Figure 4). As seen in Figure 5 outlinning access to the pleural space, 59/144 (41.0%) of all NTs did not access the pleural space. Specifically, lateral chest wall NTs did not access the pleural space in 43/124 (34.7%) of cases versus 16/20 (80%) of anterior chest wall NTs (Figure 5). Last, among all NT placements, 19/144 (13.2%) demonstrated obvious complications noted in Figure 6. Including lateral chest wall NTs, 18/124 (14.5%) cases had obvious complications, compared to 1/20 cases (5%) in the anterior chest wall group (Figure 6).
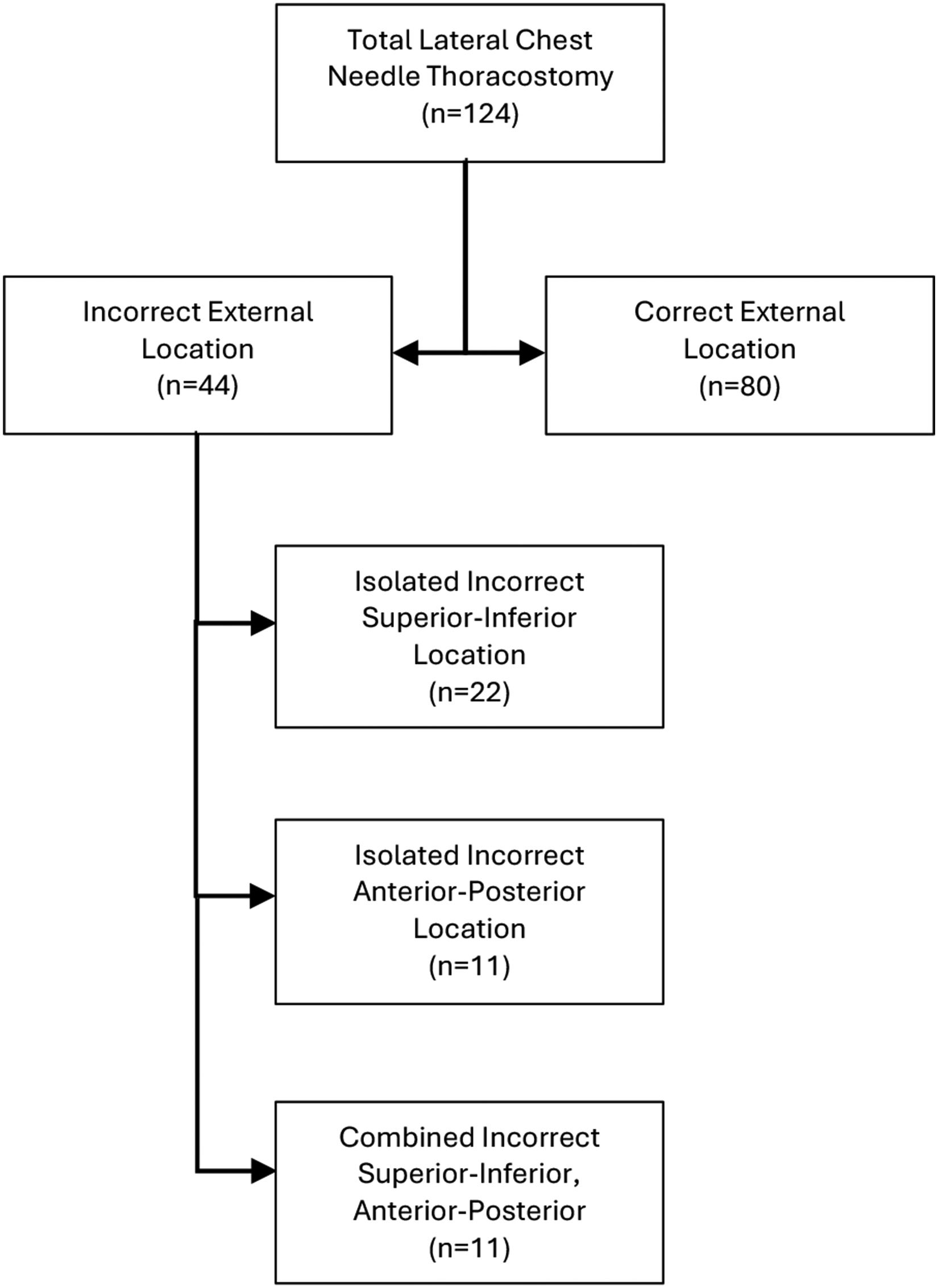
Lateral chest wall needle thoracostomies combined external anatomic placement location.
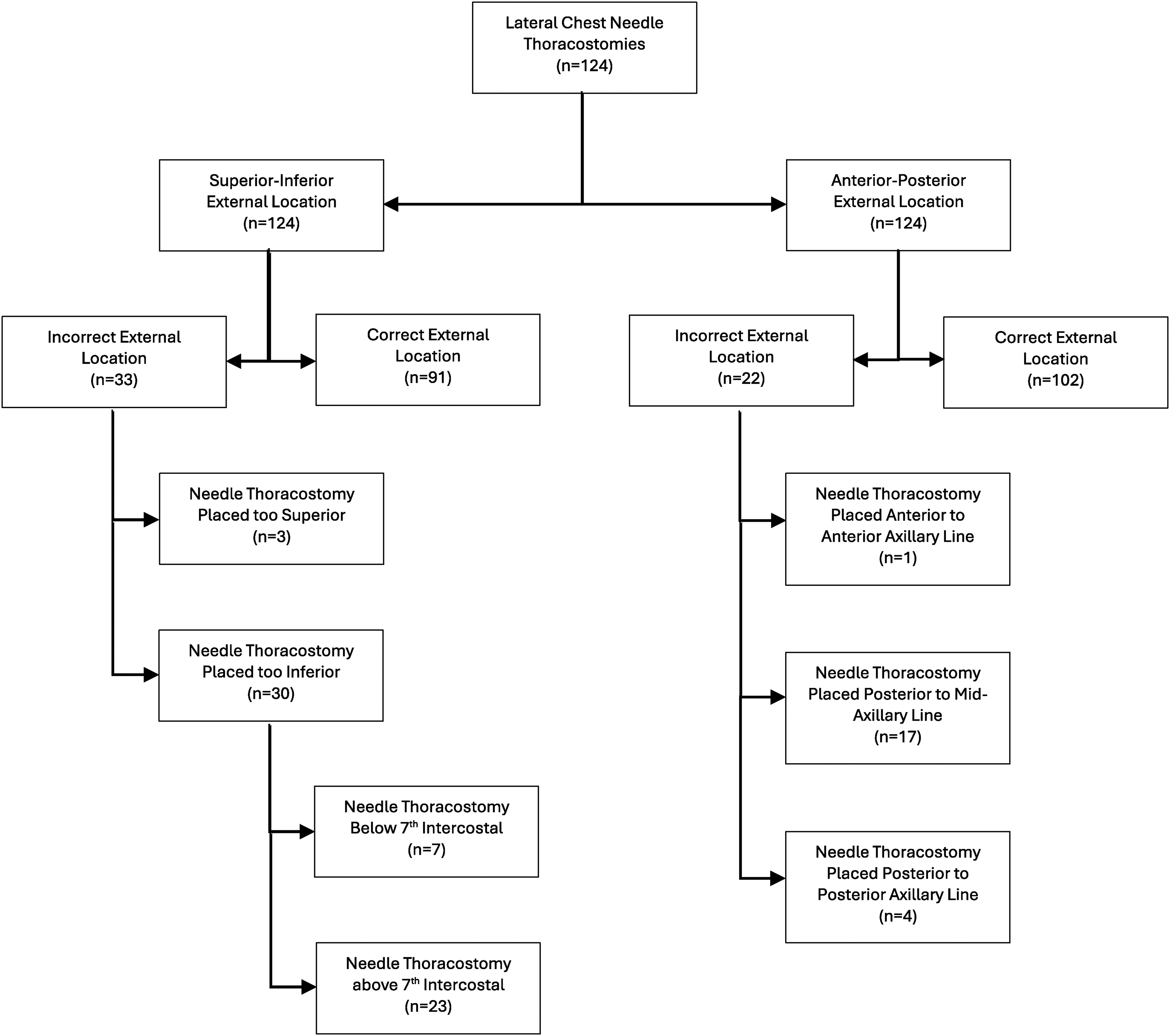
Lateral chest wall needle thoracostomies anatomic placement.
Anterior chest wall needle thoracostomies anatomic placement.
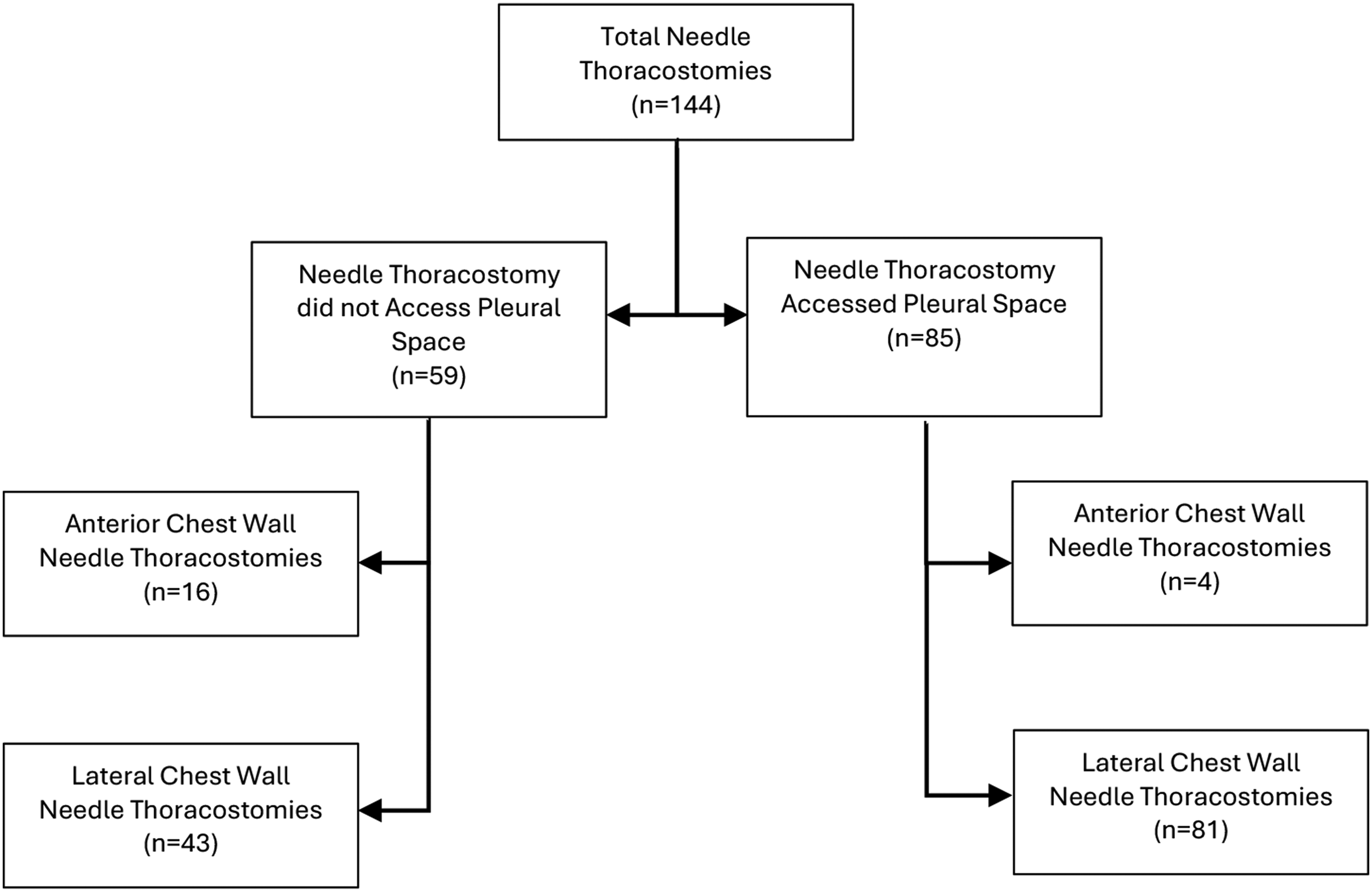
Pleural space access.
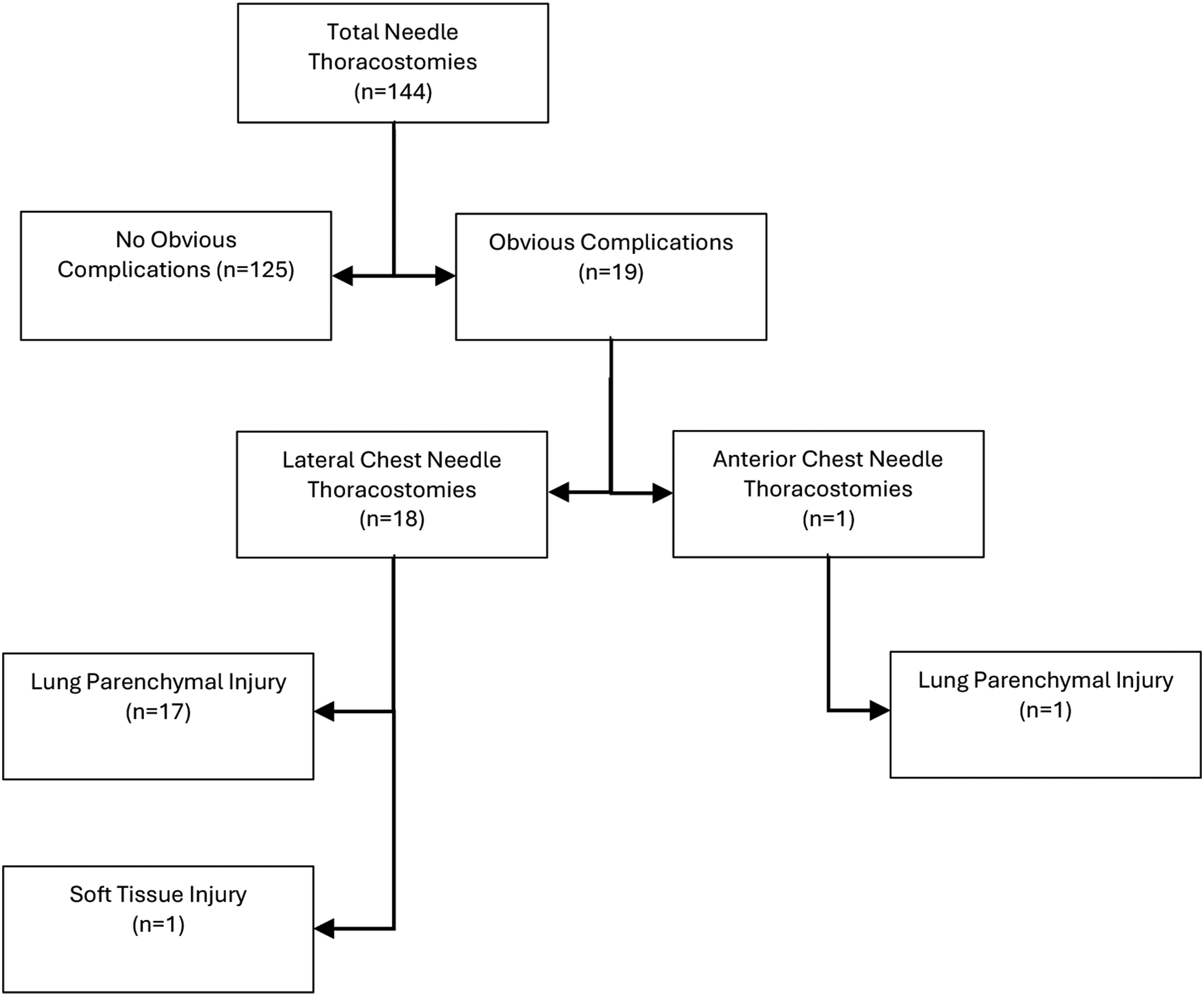
Obvious complications.
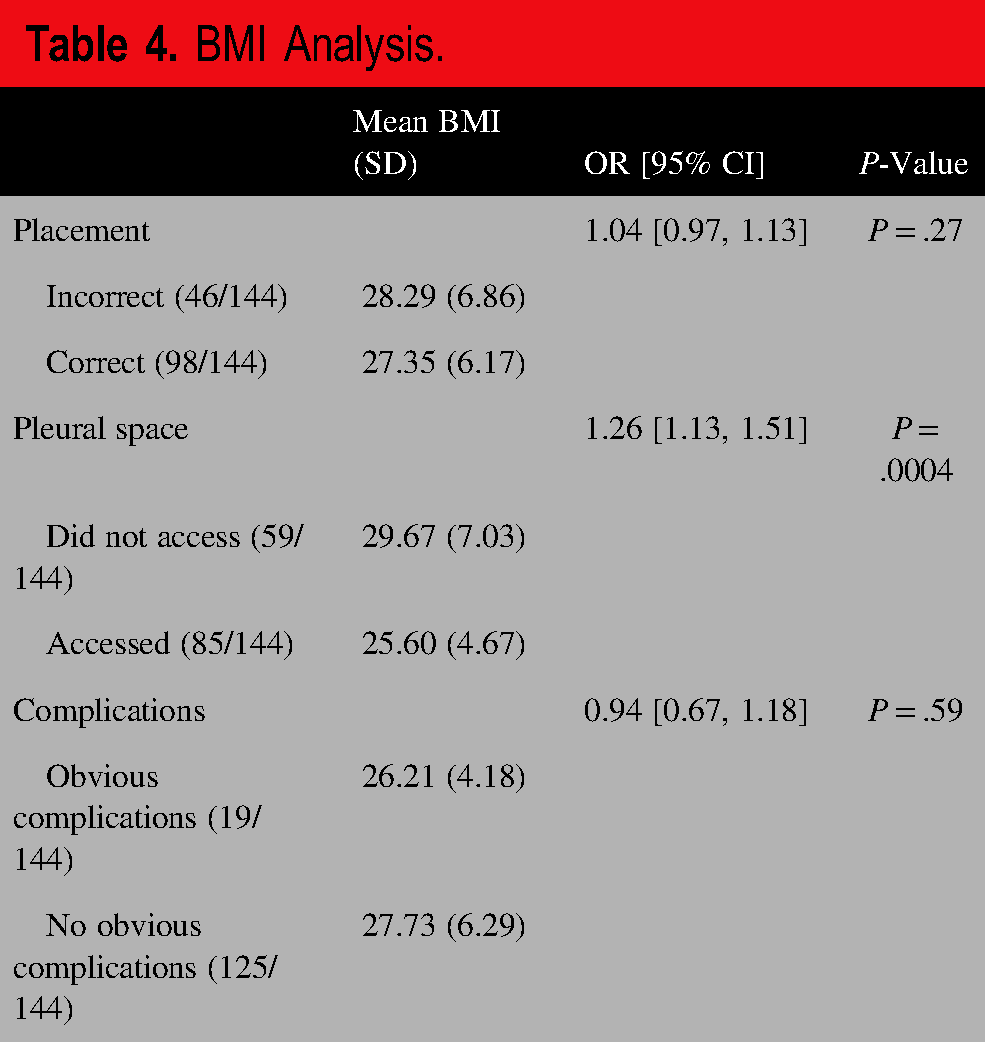
A greater percentage of lateral chest wall NTs had incorrect external anatomic placement and access to the pleural space compared to anterior chest wall NTs (P = .036 and P < .001, respectively). There was no statistically significant difference in the percentage of obvious complications in NT approaches (P = 0.474) (Table 3). There was no association between NTs placed in the correct external anatomic location and whether they accessed the pleural space access or demonstrated obvious complication rates compared to NTs not placed in the correct external anatomic location. A further subanalysis utilizing BMI was conducted and demonstrated the mean BMI was 27.57 (SD = 6.09). BMI was a statistically significant predictor of accessing the pleural space, where higher BMI was associated with greater odds of not accessing the pleural space. However, BMI was not a statistically significant predictor of correct placement or no obvious complications (Table 4).
Statistical Analysis Primary Outcomes.
BMI Analysis.
DISCUSSION
This study demonstrates three important findings in prehospital NTs performed in deceased trauma patients evaluated by a ME. Over one-third of all NTs were incorrectly positioned with lateral chest wall NTs comprising the majority of NTs incorrectly positioned, a statistically significant difference when compared to anterior NTs. Next, less than two-thirds of all NTs successfully accessed the pleural space with anterior chest wall NTs accessing the pleural space 20% of the time, which was significantly lower than lateral NTs. Overall, obvious complications were low but more common in lateral chest wall NTs than anterior chest wall NTs but this was not statistically significant.
The review of prehospital NTs by ME during autopsy to assess anatomic location, efficacy, and complications has not been documented in the literature. A review of prior literature on NTs has focused on procedural performance under different conditions such as in a healthcare setting or helicopter EMS, evaluation of only the anterior chest wall approach, shorter needle lengths, or outcome data identified by radiographic imaging. 8 Moreover, most data assessing the efficacy and accuracy of prehospital NT has been done with the assistance of radiographic evaluation in computed tomography (CT). 9 Even less studies were found to have specifically used postmortem CT. 10 While forensic pathologists commonly document medical device placement such as NTs within autopsy reports, succinct and specific data collection for such appears much less common. This specific data allows for significant novel evaluation by the ME for a multitude of reasons. Partial removal of the NT prior to CT imaging may limit procedural efficacy to a single point in time. Postmortem examination by the ME allows for manipulation of the body and more precise identification of the intercostal space and pleural cavity access. In addition, the ME is able to directly evaluate the procedural location without the presence of hemorrhage or soft tissue air acting as a surrogate marker for procedural success, which are often relied upon during CT imaging. Furthermore, many CT-based evaluations of NT placement have been limited to patients transported to the hospital alive. Autopsy evaluation, therefore, provides an opportunity to collect important procedural data that may otherwise be lost in these cases.
Historically, the traditional technique for performing an NT to treat a T-PTX was to utilize the anterior chest wall at the mid-clavicular line, second intercostal space with a 14-16 gauge catheter. Some studies have shown that, using traditional approach, failure to penetrate the pleural space can occur in as many as 76%-94% of attempted procedures. 11 These findings led to adjustment in recommended by the American College of Surgeons Advanced Trauma Life Support to catheter size from 5 cm (1.97 in) to 8 cm (3.25 in).12,13 It has been documented that the lateral chest wall thickness might be thinner in most patient populations allowing for the lower procedural failure rates in cadaveric models.14,15 Of note, there is conflicting data about the potential benefits of selecting a lateral approach compared to the anterior. Multiple studies have demonstrated poor clinician anatomical identification of anterior site and even lower rates of appropriate site selection of the lateral site.16,17 Additionally, the lateral approach is thought to increase the risk of catheter kinking during supine prolonged transport times. 18 Further, newer international ultrasound data suggests the anterior chest wall is thinner than the lateral in standard patients. 19 Our data indicates that the lateral chest wall NTs were more likely to access the pleural space; however, they were more often incorrectly placed by anatomic evaluation. The BMI of the patient appears to have a role in access to the pleural space overall, but it is unclear in our data whether that is specific to the location of the NT.
Both lateral and anterior anatomic locations for the NT procedure hold the potential for iatrogenic injury. Specifically, the risks of neurovascular injury and subsequent bleeding from costal vasculature, lung parenchyma and cardiac injury, induced pneumothorax, as well as pain to the patient are possible. 4 While the anterior approach holds the potential for injury to the mediastinal and subclavian structures, the rates of these complications are rare and often only described in case reports.20,21 However, the lateral chest wall potentially increases the rates of diaphragmatic and intra-abdominal solid organ injury if the needle is placed too low on the chest wall, which has been described to occur as often as 57%-83% of the time. 22 In recent radiographically evaluated studies for lateral chest wall NTs, this demonstrated intra-abdominal solid organ injury in 4.8% and diaphragmatic injury in 5% of cases.23,24 Reviewing this NT data, there were relatively few complications and no diaphragmatic or intra-abdominal organ injuries. The few diaphragmatic or intra-abdominal complications noted may be due to the limited sample size and rarity of these types of complications. It may also suggest improvements in guidelines and education for placement of NTs, subsequently reducing the number of these complications. In living patients, these may go unreported, particularly when they did not meaningfully impact patient outcomes or were significantly overshadowed by more life-threatening conditions.
Our data suggests that correct external anatomic positioning did not correspond to increased likelihood of accessing the pleural space or reducing complications. While this may initially appear surprising, other factors aside from external placement may play a role in procedural success. For example, the two most commonly cited reasons for procedural failure include: inadequate evacuation of the T-PTX and ineffective catheter placement. 7 Specifically, inadequate evacuation of the T-PTX might be attributed to several factors including insufficient catheter length, improper technique, clotting of the catheter, or kinking of the catheter, while ineffective catheter placement is likely multifactorial. 25 Other factors may include inadequate needle length, inaccurate needle trajectory, variations in chest wall thickness secondary to body habitus, and environmental conditions such as patient movement, limited visibility, and other complicating traumatic injuries. Finally, the operator skill, experience, and education certain plays a role in procedural success. Each of these factors is independently or collectively deserving of further study.
This study has several limitations that present opportunities for further study. The studied population is limited to prehospital, subsequently deceased trauma patients who were not transported to the hospital. The broader external validity of findings may be limited, but are likely reflective of other prehospital patient populations who receive an NT. Second, the studied EMS system promotes the usage of the lateral chest wall NT procedure as its primary location in treatment of T-PTX, influencing the training of clinicians performing this procedure. Finally, there was no real-time feedback mechanism in place between the ME and the EMS system which limited the ability of the EMS clinician to reflect on the procedure success and consider future procedural adjustments.
CONCLUSION
A collaborative model between EMS and the ME can allow for valuable autopsy-based insights into the real-world performance of prehospital NTs on deceased trauma patients who are not transported to the hospital. While anterior chest wall NTs were less likely to be placed in the incorrect external anatomical location, they often do not access the pleural space, as compared to lateral chest wall NTs. Overall, complications viewed by the ME were rare for both procedures. This collaborative model between EMS and ME helps to identify possible trends and challenges, inform training, guideline development, and system-level improvements. Such reviews are a potentially powerful quality assurance tool that can enhance patient care in high-risk, time-sensitive prehospital trauma scenarios.
Footnotes
ACKNOWLEDGMENTS
The authors would like to thank the residents and visitors of Milwaukee County for their continued trust in our fire, EMS system, and medical examiner organizations. Further, we would like to recognize the ever-challenging work that is performed without tire, day in, and day out by the EMS clinicians and the medical examiner staff.
DATA AVAILABILITY
There is no data set available for this manuscript.
DECLARATION OF CONFLICTING INTERESTS
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ETHICAL APPROVAL
This work was granted a waiver of HIPPA authorization requirements by the Medical College of Wisconsin IRB.
The authors received no financial support for the research, authorship, and/or publication of this article.
CONSENT TO PARTICIPATE STATEMENT
Not applicable.
CONSENT FOR PUBLICATION STATEMENT
Not applicable.
GENERATIVE AI DECLARATION STATEMENT
The authors did not use a generative artificial intelligence (AI) tool or service to assist with preparation or editing of this work. The authors take full responsibility for the content of this publication.
AUTHORS