
Abstract
Background:
Individuals with intellectual disabilities (IDs) are at risk of diabetes mellitus (DM) and diabetic peripheral neuropathy (DPN), which can lead to foot ulcers and lower-extremity amputations. However, cognitive differences and communication barriers may impede some methods for screening and prevention of DPN. Wearable and mobile technologies—such as smartphone apps and pressure-sensitive insoles—could help to offset these barriers, yet little is known about the effectiveness of these technologies among individuals with ID.
Methods:
We conducted a scoping review of the databases Embase, PubMed, and Web of Science using search terms for DM, DPN, ID, and technology to diagnose or monitor DPN. Finding a lack of research in this area, we broadened our search terms to include any literature on technology to diagnose or monitor DPN and then applied these findings within the context of ID.
Results:
We identified 88 articles; 43 of 88 (48.9%) articles were concerned with gait mechanics or foot pressures. No articles explicitly included individuals with ID as the target population, although three articles involved individuals with other cognitive impairments (two among patients with a history of stroke, one among patients with hemodialysis-related cognitive changes).
Conclusions:
Individuals with ID are not represented in studies using technology to diagnose or monitor DPN. This is a concern given the risk of DM complications among patients with ID and the potential for added benefit of such technologies to reduce barriers to screening and prevention. More studies should investigate how wearable devices can be used among patients with ID.
Keywords
Introduction
Adults with intellectual disabilities (IDs) have severe cognitive deficits compared to adults in the general population. 1 Intellectual disability can substantially limit a person’s independent activities of daily living and health-promotion practices. As a result, individuals with ID have disparately high rates of obesity, malnutrition, and physical inactivity,2-6 all of which can result in higher rates of chronic health conditions such as diabetes mellitus (DM). Some individuals with ID, such as those with Down syndrome, are at further risk of type 1 DM due to increased autoimmune dysfunction.5,7 According to the Centers for Disease Control and Prevention, 6.5 million people in the United States have ID. 8 Potentially, 520 000 people with ID also have DM. 6 However, despite the co-prevalence of ID and DM, patient-centered practices for DM care among patients with ID are scarce.9-11
One area of particular importance is the prevention of DM-related foot complications. As many as half of the patients with DM develop diabetic peripheral neuropathy (DPN), a disorder in which the nerve fibers in the lower limbs become damaged, leading to decreased blood flow, loss of sensation, and diabetic foot ulcers (DFUs). 12 Diabetic peripheral neuropathy is a leading cause of nontraumatic lower-extremity amputations in the United States, and foot complications are a leading cause of hospitalization among patients with DM. 13 Recent articles by Cuypers et al 14 and Youn et al 15 suggest that individuals with ID and DM have a 1.87 (95% confidence interval [CI]: 1.41-2.49) times higher incidence of foot complications and are 5.52 (95% CI: 3.78-8.05) times more likely to undergo avoidable, DM-related hospitalizations than the general population.
These findings highlight the importance of evidence-based, patient-centered practices to prevent DM-related foot complications and ensure prompt intervention for foot complications when these do occur. However, preventive foot care relies largely on regular monitoring of the feet and day-to-day foot care. To accomplish this, patients with DM and ID may benefit from assistive devices, such as wearable or mobile technology to prompt preventive foot care practices or alert caregivers when further attention is needed. Such devices have been shown to be efficacious in screening and monitoring patients with DM, as well as DM complications, in other contexts,16-32 but the utility of these technologies in patients with co-occurring DM and ID is unknown. To answer this question, we conducted a scoping review focused on three questions: (1) What is the current state of the technology used to diagnose and monitor DPN? (2) What has been published on the use of wearable technologies in monitoring DPN in individuals with ID? (3) What gaps persist in the current literature about the use of such technologies in individuals with ID?
Methods
Search Strategy
We conducted a literature search using the databases Embase, PubMed, and Web of Science. Our original search queries aimed to identify studies that use technology to diagnose or monitor DPN of the lower extremities in individuals with ID. These queries can be found in Table 1. These terms resulted in only five publications from Embase, none from PubMed, and none from Web of Science. As a result, we concluded that available literature specific to the topic of DPN diagnosis and monitoring in patients with DM and ID is scarce. Thus, we focused on literature describing the current state of technology use to diagnose and monitor DPN in the general population and sought to place these results in the broader context of ID care. We broadened our original search by omitting the ID search terms (highlighted in bold in Table 1). After running the remaining search terms, we cross-checked the articles found in each database for duplication and removed these duplicates.
Queries for Diabetes Mellitus, Diagnostic Procedures, Wearable Technology, Neuropathy, and Intellectual Disabilities Used in Literature Search of Embase, PubMed, and Web of Science.
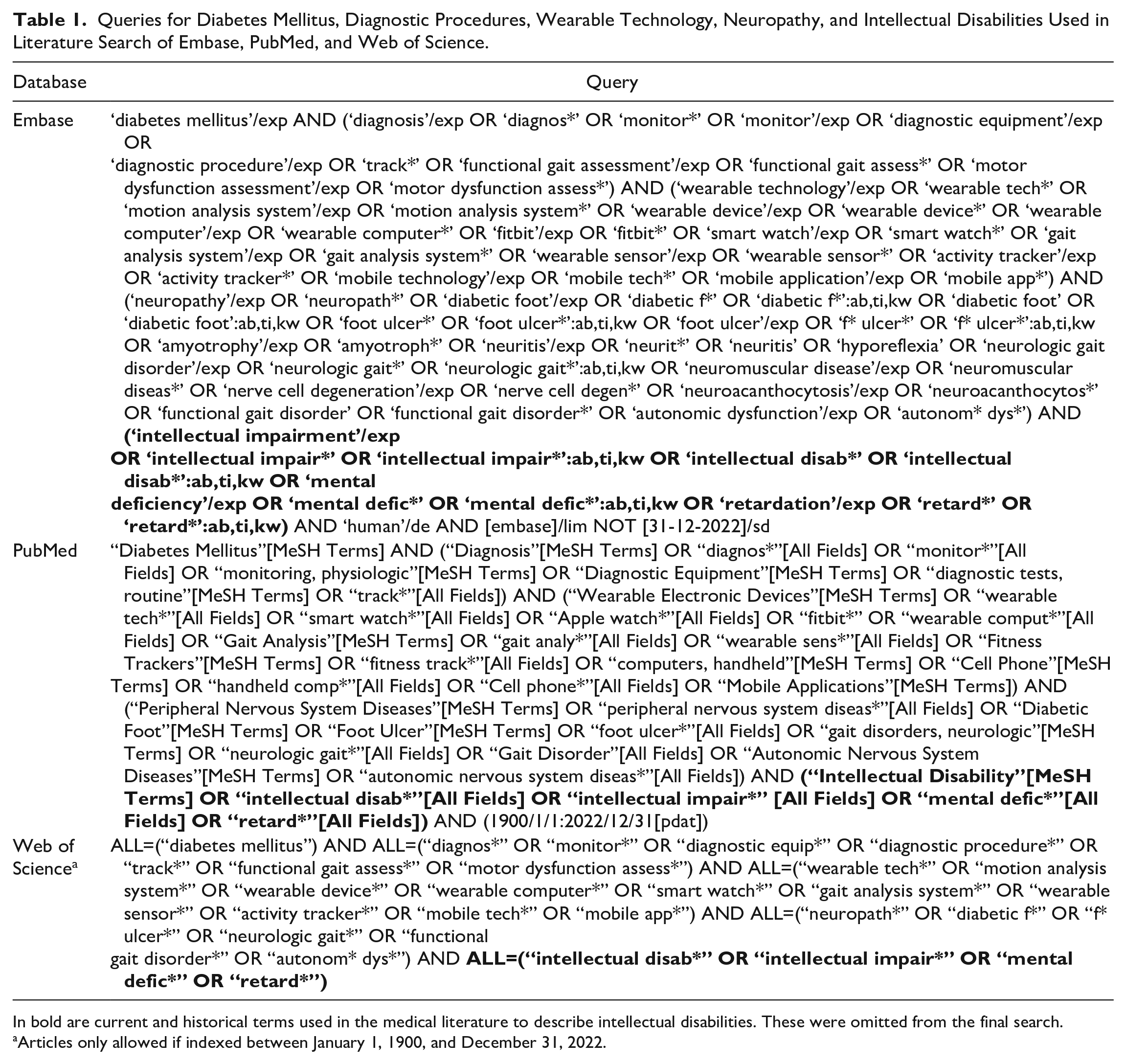
In bold are current and historical terms used in the medical literature to describe intellectual disabilities. These were omitted from the final search.
Articles only allowed if indexed between January 1, 1900, and December 31, 2022.
Abstract Review
Queries to identify abstracts for this review were run in December 2023. Two reviewers (E.B. and M.C.) independently reviewed each abstract with respect to the following inclusion criteria:
Study must include diabetes-related neuropathy or nerve-related disorder.
Study must use a technological device to diagnose, track, or evaluate patients for a clinical purpose.
Study’s subject population must be human.
Study must have been peer reviewed or an abstract submitted to a conference.
Study must have been posted online by December 31, 2022.
Study must have been completed at the time of the scoping review.
Where the reviewers disagreed, further discussion was held until consensus was achieved.
Full-Text Review
Two reviewers (E.B. and B.G.) read each article independently and voted on inclusion based on the aforementioned inclusion criteria and three exclusion criteria added in this phase to increase the responsiveness of the scoping review to the original question about DPN monitoring for patients with ID:
Study device could not be used solely for photographic purposes.
Study device could not be used purely for diabetic retinopathy.
Study could not exclusively use a force plate, pressure platform, or walkway.
Where the reviewers disagreed, ties were broken by a third reviewer (M.C.).
The Joanna Briggs Institute (JBI) checklists for systematic reviews were used as a template for determining the quality of studies.33,34 Data extraction was performed using a form built in the survey design software Qualtrics. Summary statistic calculations and other data analyses were performed using RStudio version 4.2.2.
Results
Summary of Articles Removed and Retained
A modified version of the Preferred Reporting Items for Systematic Reviews (PRISMA) 35 workflow for the scoping review is shown in Figure 1.
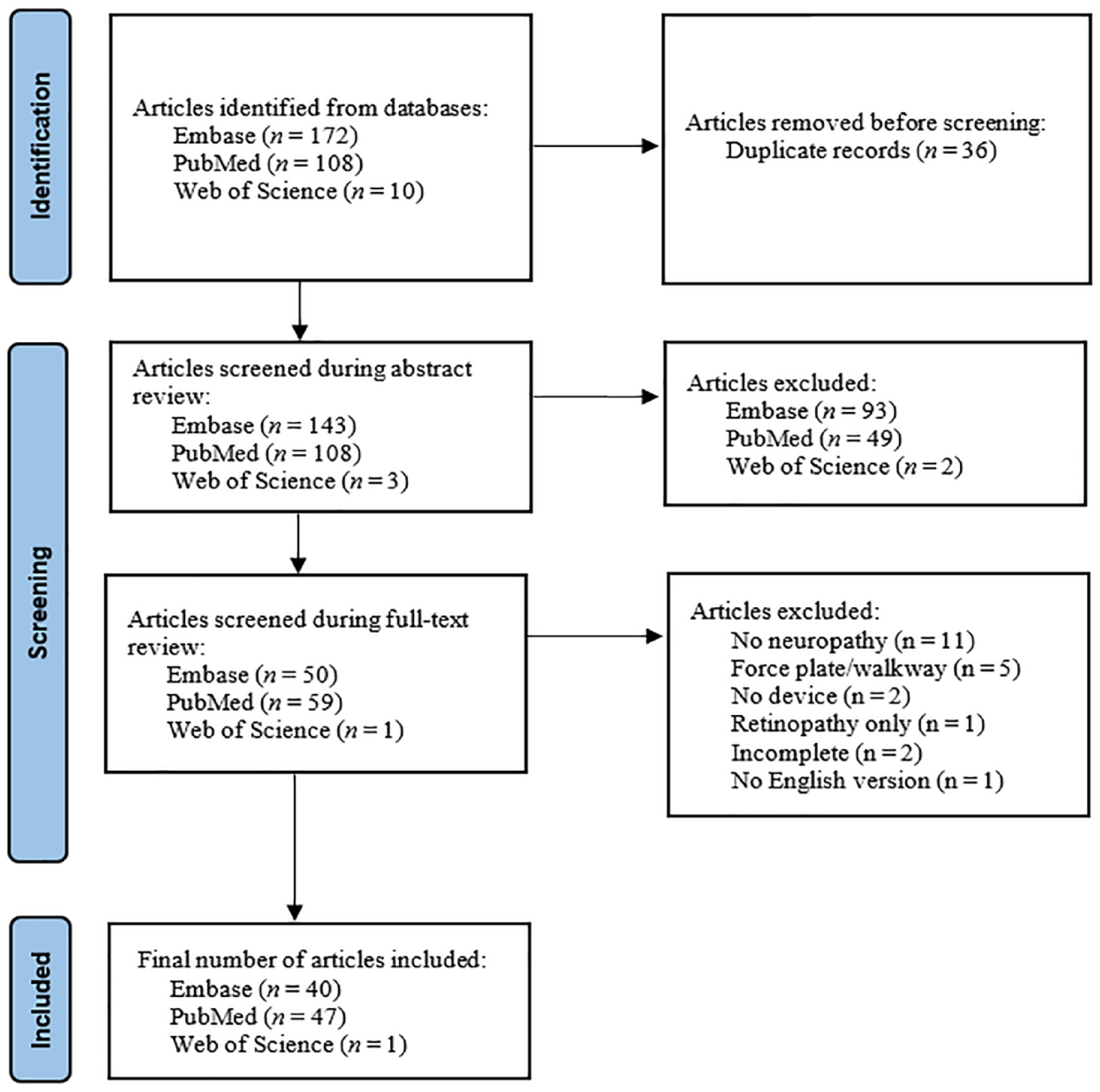
Modified Preferred Reporting Items for Systematic Reviews diagram displaying the workflow used during article evaluation for the scoping review.
Prior to removal of duplicates, there were 290 results across Embase, PubMed, and Web of Science. After removal of duplicates, we found 143 results in Embase, 108 results in PubMed, and three results in Web of Science. At the abstract review phase, 93 articles were removed from Embase as not matching the inclusion criteria, 49 were removed from PubMed, and two were removed from Web of Science. Some reasons for removal were (1) study used non-human subjects, (2) study was a literature review, and (3) device used in study was not for measurement or diagnostic purposes.
Another 22 articles were removed during the full-text review. Reasons for removal were lack of diabetes-related neuropathy (11 articles); exclusive use of a force plate or walkway (five articles); lack of a technological device to diagnose, track, or evaluate patients (two articles); study incomplete at time of review (two articles); study of retinopathy only (one article); and lack of an English version of the article (one article). After full-text review, 88 articles met the requirements to be included in the scoping review.16-32,36-106 Of these, 40 were from Embase, 47 were from PubMed, and one was from Web of Science.
Table 2 contains summary statistical findings from the review. Of the 88 articles reviewed, 46.6% were cross-sectional, 15.9% were diagnostic accuracy studies, and 9.1% were randomized controlled trials. Of the studies, 30.7% included only subjects with type 2 diabetes, 22.7% included subjects with either type 1 or type 2, and 46.6% did not specify a type of DM. In total, 70.4% of all studies had at least two comparison groups, while one article had as many as eight. More than half of the studies used a single type of technological device to diagnose, monitor, or track DPN. Non-wearable technologies, such as force plates/pressure platforms and 3-D gait analysis technologies, were the most often used devices (Figure 2). These were often used in combination to analyze gait and foot pressure distributions.
Summary Statistics of the Studies Included in This Scoping Review.
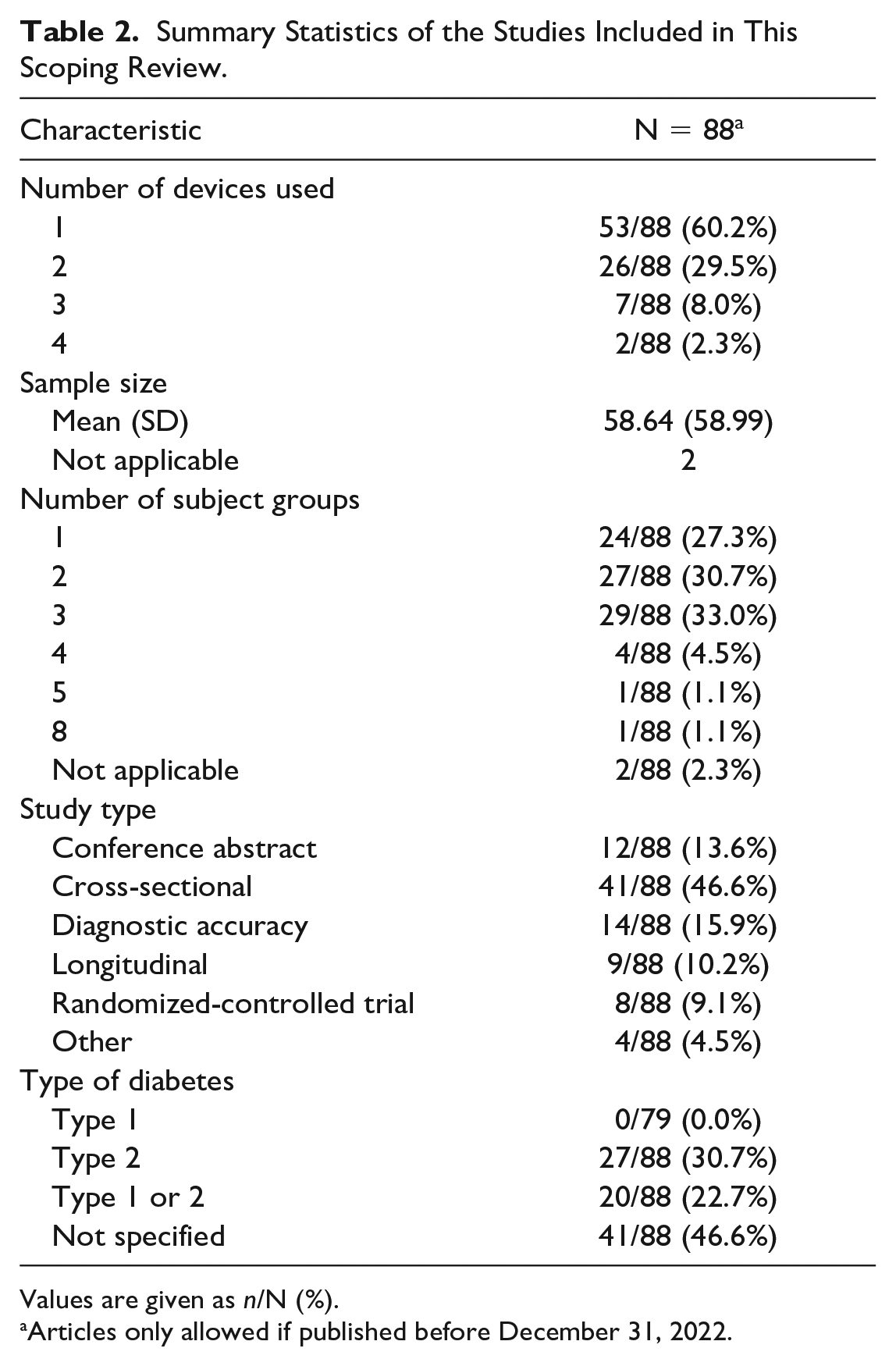
Values are given as n/N (%).
Articles only allowed if published before December 31, 2022.
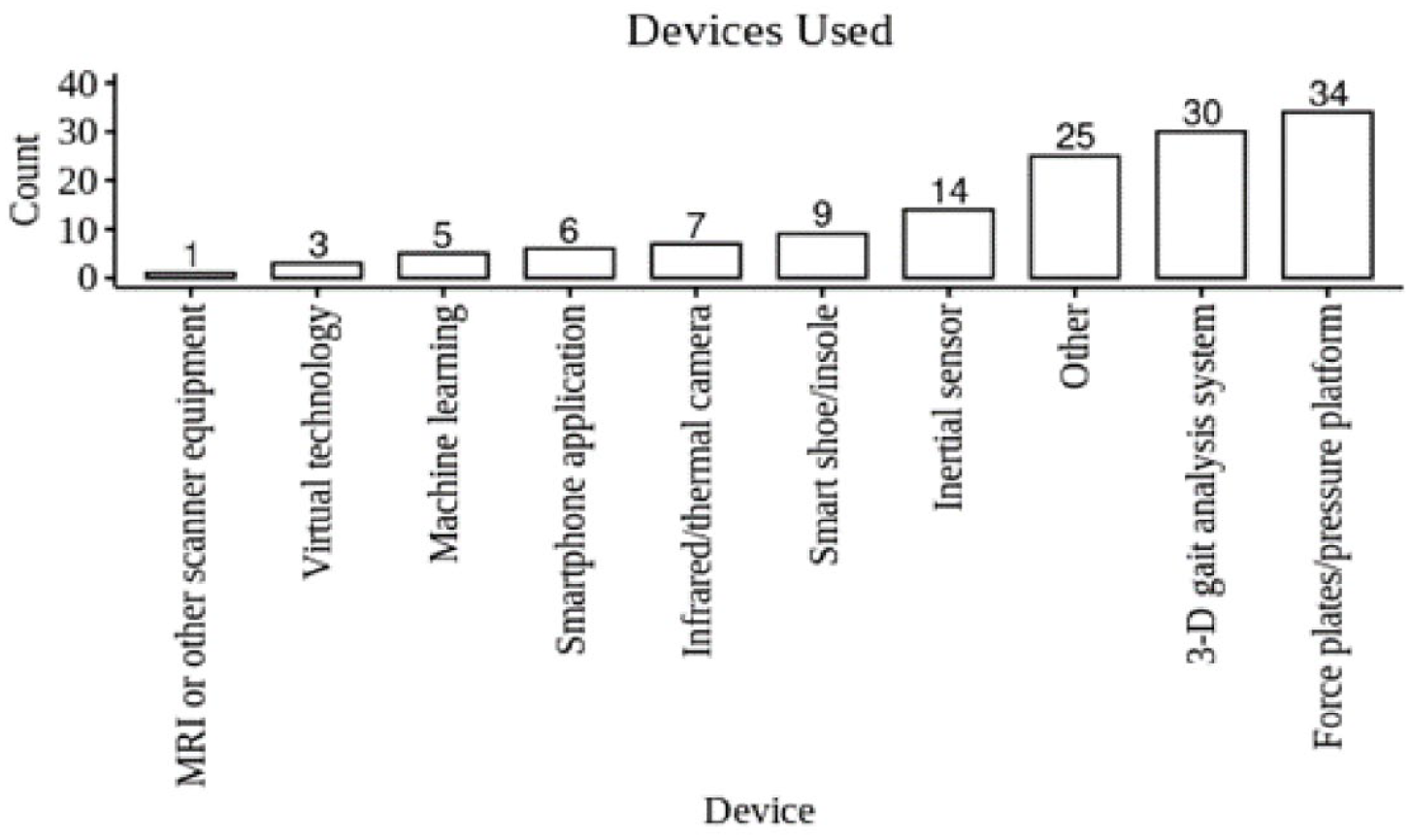
Bar plot of the most-commonly-used types of devices included in the scoping review. The category “Other” contains devices that did not fit into any of the other nine categories.
The earliest published article was from 1994 (Figure 3). 37 The years with the most published articles were 2017 and 2021, when 13 were published. The trend in publication frequency has increased over the last few decades, although year-to-year variance is high.
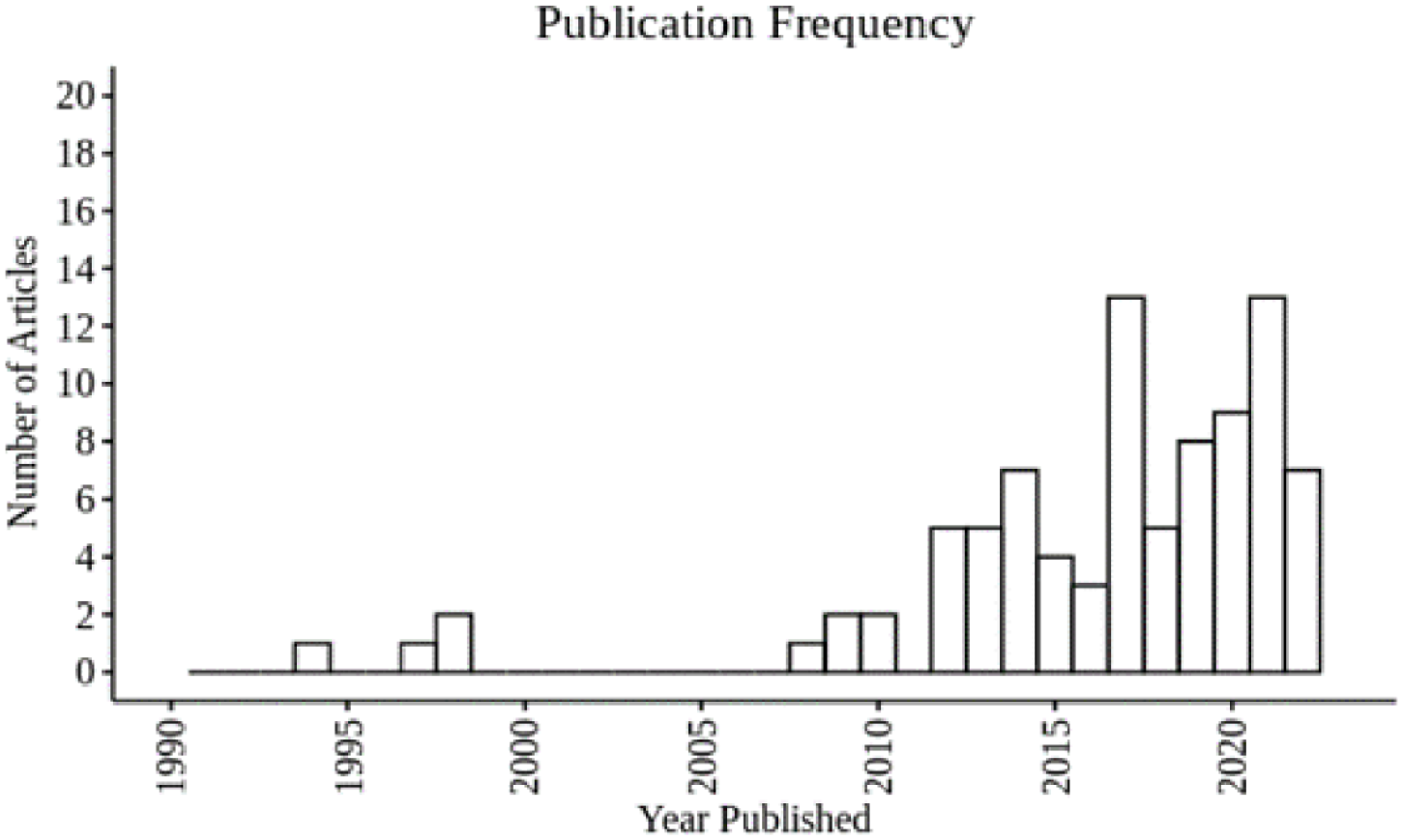
Histogram of publication years for studies included in the scoping review.
Four major themes identified during the review are shown in Figure 4. The largest portion of studies concerned gait mechanics in individuals with DPN, followed by DPN/DFU screening and wound healing/monitoring.
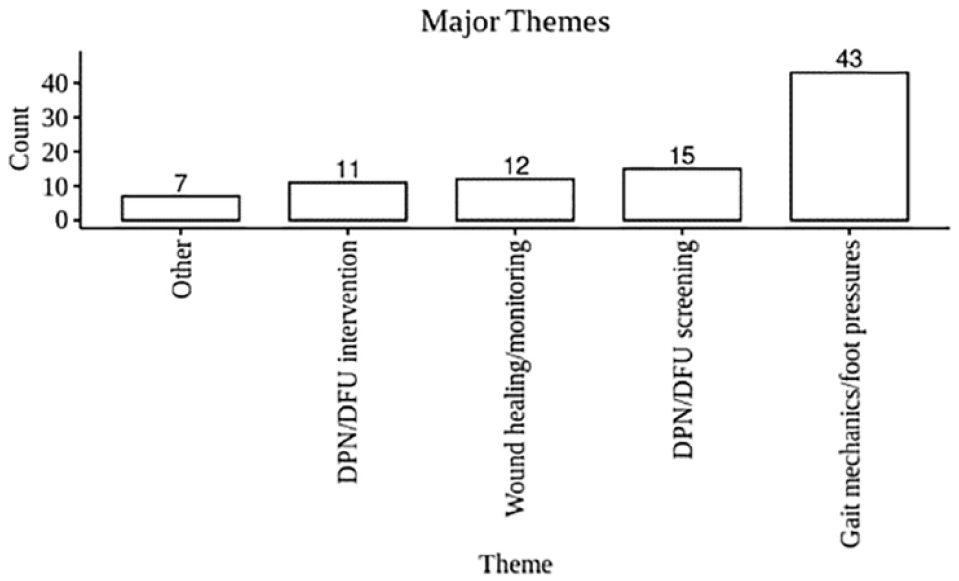
Four major themes from the studies included in the scoping review. Any themes that did not fit into the four categories are counted as “Other.”
Representation of People With ID
No articles explicitly included individuals with ID, and several explicitly excluded individuals with cognitive deficits, impairments, or dysfunction that would preclude them from full participation in the study.23,30,32,69,80 Three studies used a population of individuals with neurological conditions caused by stroke or cognitive impairment (Table 3).29,54,55 One study by Zhou et al 29 used the Mini Mental State Examination (MMSE) to quantify cognitive impairments in a group of hemodialysis patients. Individuals with greater cognitive impairment, as measured by the MMSE, were significantly less active and had longer transition times from standing to sitting than individuals without cognitive impairment. 29 Tajuddin et al 54 conducted a study in which the gait parameters of stroke survivors with DPN were compared against those of stroke survivors without DPN. Mustapa et al 55 conducted a study in which the gait parameters of stroke survivors with DPN were compared against stroke survivors without DPN and a healthy control group. Both studies showed significant changes in the gait parameters of stroke survivors.
Studies That Included Individuals With Cognitive Complications.
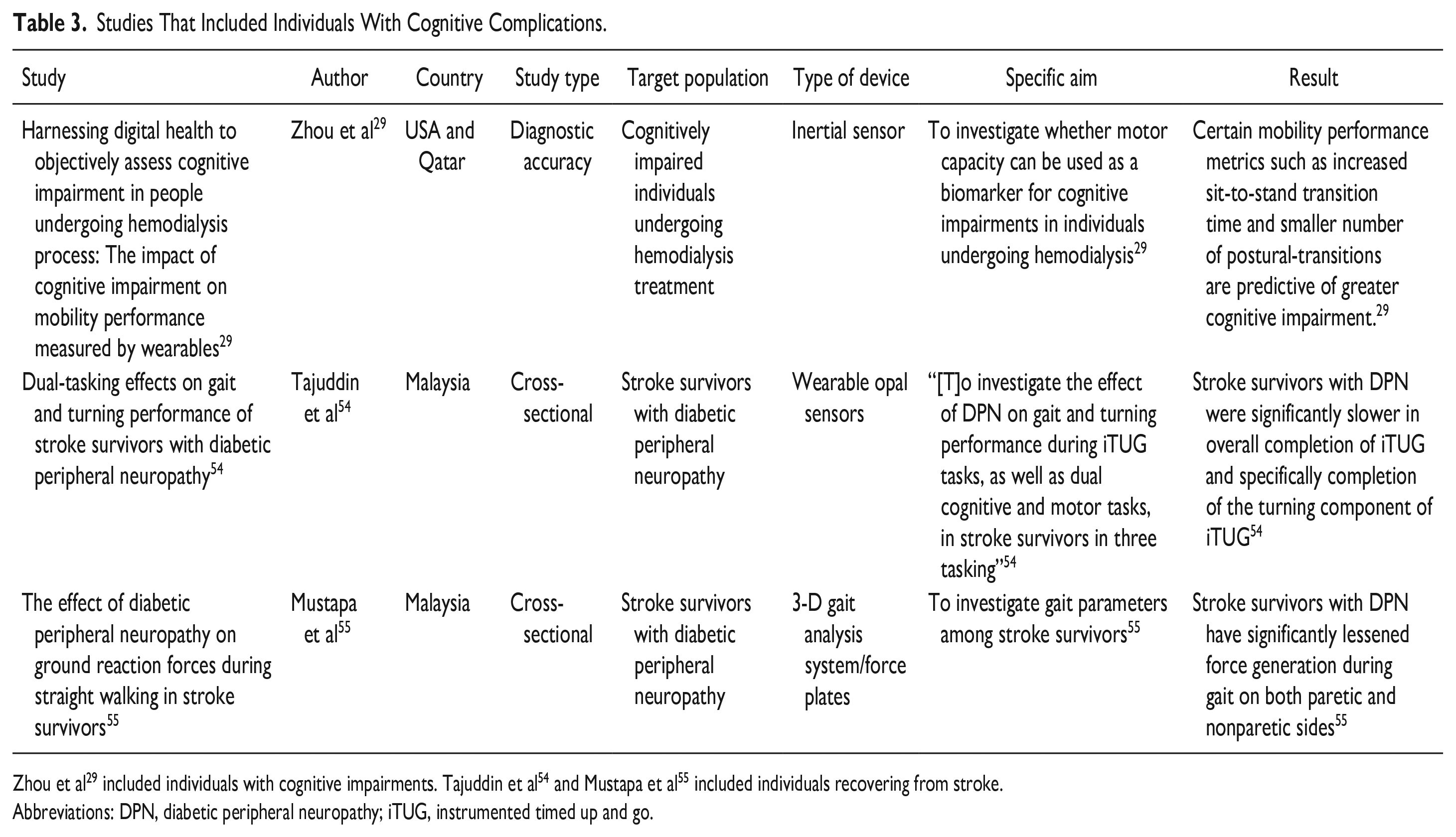
Zhou et al 29 included individuals with cognitive impairments. Tajuddin et al 54 and Mustapa et al 55 included individuals recovering from stroke.
Abbreviations: DPN, diabetic peripheral neuropathy; iTUG, instrumented timed up and go.
Eight randomized control trials have been published (Table 4). None of these studies specifically targeted individuals with ID. However, their results may be transferrable to such a population. An article by Abbott et al 30 describes a pilot study in which individuals with a history of DFUs were assigned to either a control group or an intervention group. The intervention was the SurroSense Rx smart insole (Orpyx Medical Technologies, Canada). This device is capable of sensing peak plantar pressures and warning an individual of increased risk of DFU, which occurs at higher foot pressures. The study found a significant decline in foot ulcer incidence rate in the intervention group. 30 However, the study sample explicitly excluded individuals with psychological impairment.
Eight Randomized-Controlled Trials Found During Our Literature Review.
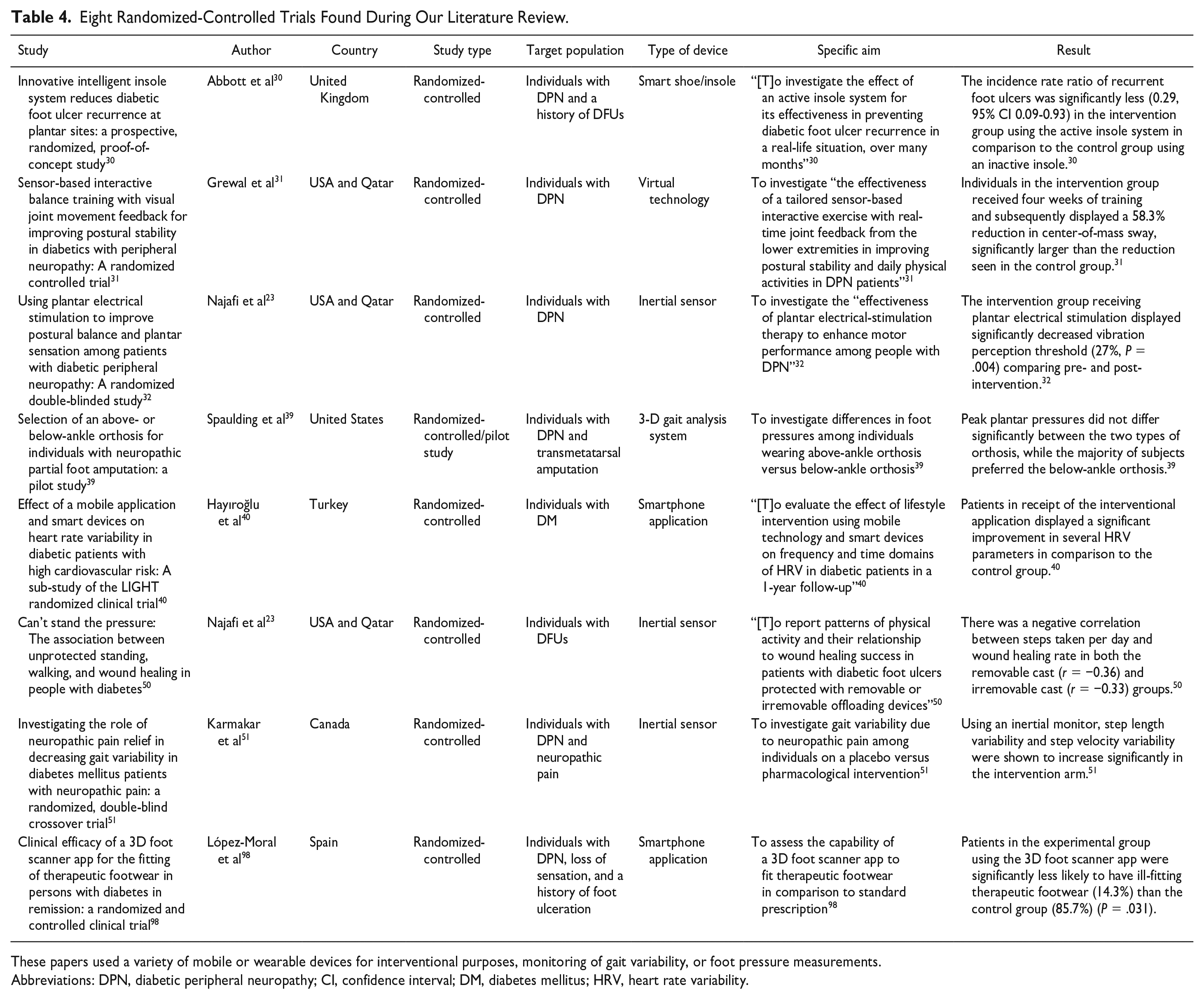
These papers used a variety of mobile or wearable devices for interventional purposes, monitoring of gait variability, or foot pressure measurements.
Abbreviations: DPN, diabetic peripheral neuropathy; CI, confidence interval; DM, diabetes mellitus; HRV, heart rate variability.
A study by Grewal et al 31 used sensors to create an interactive virtual obstacle-crossing task, where study participants with DPN could perform exercises mimicking movements to step over different obstacles displayed on a screen as a means of balance training. This type of exercise could be a simple and safe way for individuals with ID and DPN to work on their balance and postural stability, as well as encourage them to remain active physically, while also not exposing them to the dangers of real-life obstacle-crossing activities; however, as in the study by Abbott et al, 30 individuals with cognitive dysfunction were excluded from the study population.
Although review articles were not eligible for full-text analysis as individual studies in this scoping review, we examined the references in other review articles returned by our search query to assess for research that may have been inadvertently excluded by our search criteria. This revealed 29 additional studies that might have been eligible for the study if they had been captured by our original search. In general, these studies emphasized specific devices (e.g., thermometers, insoles) that may not have been picked up by our more general search criteria.107-116 Importantly, however, as with all other studies captured by our main search criteria, none of these other studies were conducted among individuals with ID.
Discussion
To the best of our knowledge, this is the first scoping review of the literature on wearable technologies and DPN, with a focus on individuals with ID. Using a broad range of queries, we searched the databases Embase, PubMed, and Web of Science for studies relating to the topic. We were unable to find sufficient evidence specific to patients with co-occurring DM and ID. Using broadened search criteria, we reviewed 88 articles and found none that used individuals with ID as the target population. In addition, many studies we found did not use technology suitable for application outside of a traditional clinical setting. These technologies, such as 3-D gait analysis systems and force plates, although useful for measuring gait parameters and foot pressures, are not compatible with day-to-day, wearable use.
We did find multiple studies that show the promise of wearable technology in DPN diagnosis and management, in general. Najafi et al 23 and Abbott et al 30 demonstrated the efficacy of the SurroSense Rx device in monitoring foot pressures in individuals at risk of recurrent DFUs during their daily lives. Torreblanca Gonzalez et al 28 investigated the use of temperature-monitoring socks to provide surveillance for DFUs in individuals with diabetes. Najafi et al 32 investigated an interventional device, the SENSUS® transcutaneous electrical nerve stimulator (NeuroMetrix, Inc., USA), which sends electrical stimuli to the soles of the feet to improve motor performance in individuals with DPN. Najafi et al 50 demonstrated the efficacy of a wearable inertial sensor in monitoring physical activity among individuals with current DFUs. Motivational apps, such as the one described in the study by Hayıroğlu et al, 40 that help individuals with DPN to make healthy choices about their diabetes may be of use in modified forms for individuals with ID, who are at risk of poor diets and sedentary lifestyles regardless of their diabetes status.2-6 These and similar devices could be of use in individuals with ID, and future studies that deliberately include populations with ID are warranted.
Indeed, research into the use of wearable devices in individuals with ID in other areas is growing rapidly. Using the query terms for ID and wearable technologies in Table 1 without including DM terms gives hundreds of results across Embase, PubMed, and Web of Science. Although these are not specific to DM or DPN, some provide a glimpse into how technology is being used to help individuals with ID and how future studies about wearable devices for DPN might be approached.117-143 Research areas include monitoring physical activity among individuals with ID using wearable devices such as inertial sensors117-123; educating and intervening on social and physiological aspects of patients’ lives using mobile technology such as smartphone applications124-130; gait analysis and its relationship to neurological variables131-140; and the general feasibility of using wearable technology in individuals with ID.141-143 The quantification of physical activity, the analysis of gait, and the general support of health promotion in this growing body of literature may translate well to future studies focused on DM care.
Notably, these studies also describe some methodological challenges for studying the use of wearable technologies among individuals with ID. First, studies should deliberately ensure that devices are acceptable to individuals and minimally disruptive to other health routines. The presence of a new device may substantively alter individuals’ physical environments and daily routines and, thus, may influence individuals’ responsiveness, receptiveness, or reaction to the device. 118 Second, studies should establish and adhere to rigorous measurement and reporting standards. Leung et al 117 conducted a systematic review of accelerometer use to measure physical activity in individuals with ID and found inconsistent measurement protocols in the current literature.
Our scoping review emphasizes an important and understudied area of device research in DM and ID, yet our approach has several weaknesses. First, we only searched three databases; others, such as PsycINFO and CINAHL, could have resulted in more studies for inclusion in our review. Second, we did not conduct a review of bibliographies from accepted articles, which could also have resulted in the inclusion of other studies. Third, our review extended through 2022 and did not include articles thereafter, although relevant technologies may continue to evolve rapidly over time. Fourth, although we tailored our search terms for technologies to diagnose or track DPN and captured studies about a broad range of devices, we inevitably omitted some specific terms that may have resulted in more studies being found and reviewed. In future studies, it may be beneficial to add terms such as “thermometer,” “insole,” or “footwear,” to widen the search even further. Finally, we did not conduct a systematic search of gray or unpublished literature. Although we did search for clinical trials topically related to wearable devices and DPN, of the two trials found, one was terminated prematurely due to COVID-19, 144 and the other does not begin until 2024. 145 Despite these weaknesses in the expansiveness of our review, it is unlikely that these substantially change the global findings of the review. Our review demonstrates that emerging evidence about the utility of wearable technologies for foot care in patients with DM is robust and ever-growing. However, people with ID who may benefit from these technologies by offsetting other, ID-related barriers to preventive care have largely been excluded from this important area of research.
Conclusion
The existing body of literature regarding technology and DPN does not adequately investigate the use of wearable technology in individuals with ID. Although dozens of articles have been published describing devices to track, monitor, and diagnose DPN or DFUs, there are currently no papers looking at how such devices can be applied to individuals with ID. In addition, most devices assessed in the studies we reviewed are not wearable or usable outside a clinical setting, although several devices show promise as real-world interventions for DFUs and as early alert systems for DPN. These include pressure-sensitive smart insoles such as the SurroSense Rx23,30 and socks capable of detecting temperature changes to parts of the foot, such as the heel, midfoot, and metatarsals. 28 Outside the hospital, these could be invaluable to individuals who experience barriers to communication with healthcare providers. Future research in this area should deliberately consider the needs, preferences, and challenges of people with co-occurring DM and ID.
Footnotes
Acknowledgements
The authors would like to thank Emily Roberts, PhD, from the University of Iowa Department of Biostatistics for thoughtful input about this manuscript.
Abbreviations
B.G., Bailey Goodman; DFUs, diabetic foot ulcers; DM, diabetes mellitus; DPN, diabetic peripheral neuropathy; E.B., Ercole Barsotti; ID, intellectual disabilities; JBI, Joanna Briggs Institute; M.C., Martha Carvour; MMSE, Mini Mental State Examination; PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analyses.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: M.C. has provided consultative support for the Suga Project/Suga Project Foundation but has not received financial compensation for this consultative work.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Graduate College Recruitment Fellowship from the University of Iowa (to E.B.) and the National Institutes of Health (KL2 TR002536, K12 TR004403, both to M.C.).