
Abstract

Worldwide, the number of individuals developing type 1 diabetes (T1D) is projected to increase. 1 The economic cost of T1D is also substantial, as patients with T1D, even though markedly fewer in number, have significantly higher total medical costs per year compared with others with type 2 diabetes (T2D). 2 At the time of diagnosis of T1D, a major concern is the delay in the recognition of new onset of T1D, increasing the risk of diabetic ketoacidosis (DKA) requiring hospital admission. 3 Recent research has suggested that the number of individuals developing DKA has increased in the past decade with a significant number being identified as a late diagnosis of T1D. 4 Therefore, identifying T1D at an early stage where evidence-based therapies can be given to delay the onset would potentially have important health and economic benefits.
Type 1 diabetes is an autoimmune disease characterized by immune-mediated destruction of insulin-producing pancreatic β-cells. The loss of endogenous β-cell function necessitates an absolute requirement for life-long exogenous insulin for survival. β-cell destruction is marked by the production of autoantibodies against pancreatic islet cells that can be detectable many years before the development of symptomatic hyperglycemia. 5 In particular, the presence of two or more T1D-associated islet autoantibodies (IAbs) is highly predictive of the eventual development of clinical disease. This pattern now serves as the basis for defining the earliest of three stages of T1D. These stages are presented in Table 1.
T1D Develops in Most Cases Following a Phase of Evolving Risk Characterized by Increased Genetic Risk, Immune Activation, and an Immune Response.
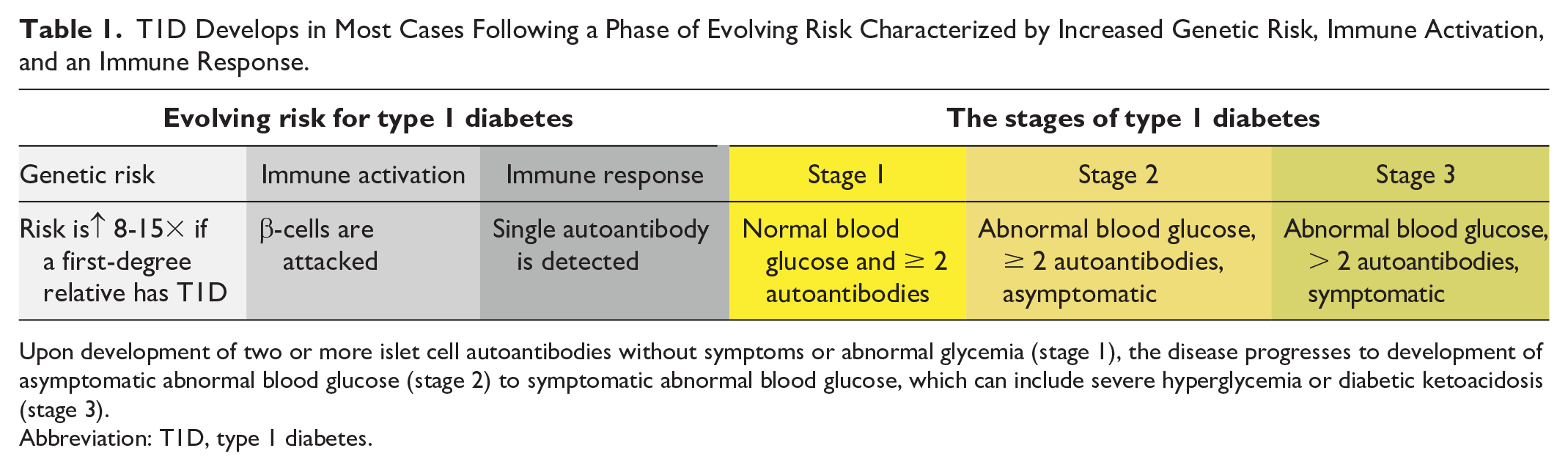

Upon development of two or more islet cell autoantibodies without symptoms or abnormal glycemia (stage 1), the disease progresses to development of asymptomatic abnormal blood glucose (stage 2) to symptomatic abnormal blood glucose, which can include severe hyperglycemia or diabetic ketoacidosis (stage 3).
Abbreviation: T1D, type 1 diabetes.
At present, stage 2 T1D, where at least two antibodies and asymptomatic dysglycemia are present, provides an opportunity to offer intervention with a US Food and Drug Administration (FDA)-approved immune-modulating therapy to delay the progression to stage 3. In addition, early identification of at-risk individuals would also allow an opportunity to establish timely and appropriate surveillance to reduce the risk of unrecognized progression to stage 3 and the potential development of unexpected DKA.
Approximately, 80% of cases of T1D occur sporadically without a family history of a first or second degree relative with T1D, 6 and early identification of those at risk is important since those with multiple IAbs have a lifetime risk of more than 85% of developing T1D. 7 The five-year risk of eventual development of T1D at the first stage is at least 44%, and by the second stage, when dysglycemia appears, the five-year risk increases to 75%. A clinical advantage of screening children for IAbs and identifying risk and early stages of T1D includes a five-fold reduction in DKA rates at stage 3 of the disease. In addition, there is a window of opportunity for administering prevention therapy if T1D is identified between the first and third stages.
Teplizumab, a monoclonal antibody targeting T-cell-mediated β-cell destruction, has shown efficacy in reducing abnormal glucose tolerance in individuals at high risk of developing T1D when administered as a 14-day infusion. It was approved by the US FDA in November 2022 as the first treatment indicated to delay the onset of stage 3 T1D in adult and pediatric patients aged eight years and older with stage 2 T1D. 8 This medication teplizumab appears to be able to delay the need for exogenous insulin therapy for an average of nearly three years. 9
International consensus guidance has been developed for ongoing metabolic monitoring for disease progression in individuals at stage 1 T1D. The recommended monitoring includes regular assessments for dysglycemia with various blood tests requiring that the patient (who is usually a child) have phlebotomy to check fasting glucose, two-hour glucose from an oral glucose tolerance test (OGTT), random glucose, or hemoglobin A1c (HbA1c). 10 An alternative would be the use of continuous glucose monitor (CGM) data, as it is likely that many people at risk, especially children, may prefer using a CGM, which is potentially less invasive, less painful, and less burdensome than phlebotomy, if CGM data were established to provide useful treatment recommendations. 11
If the metabolic monitoring process for progression to stage 2 T1D is too frequent and/or burdensome, then individuals at risk may become frustrated and refuse further testing. If monitoring for dysglycemia is infrequent or not done, then there is a potential missed opportunity for treatment with stage 2 therapies, such as teplizumab, and/or a risk of progression to DKA, which is dangerous and not amenable to prevention therapy. Currently, no consensus guidelines exist for how to use CGM data to identify stage 2 T1D, during which approved prevention therapy can be successfully prescribed.
Continuous glucose monitoring has been used off label to monitor glucose concentrations for a variety of metabolic conditions characterized by either hyperglycemia or hypoglycemia, including as a tool to detect dysglycemia in patients with stage 2 T1D. Use of continuous glucose montioring provides several metrics in a standardized report called the ambulatory glucose profile. 12 These metrics can be applied individually or in combination to identify dysglycemia, leading to a recommendation for a confirmatory glucose or HbA1c test for diagnosis.
We conducted a search on PubMed for all English language reports that use original CGM data to predict the progression of patients to clinical T1D. The search string was “(“Type 1 Diabetes” OR “T1D”) AND (“continuous glucose monitor” OR CGM) AND (“autoantibod*” OR “autoimmunity”) AND (Human).” This search initially yielded 25 studies, but after completing abstract screening for relevance, and full-text screening using inclusion/exclusion criteria, we narrowed down the number of studies to eight for data extraction. Our inclusion criteria included exploration of progression to clinical T1D, the use and analysis of CGM metrics, and original experimental data. Figure 1 shows the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA) diagram summarizing this search process.
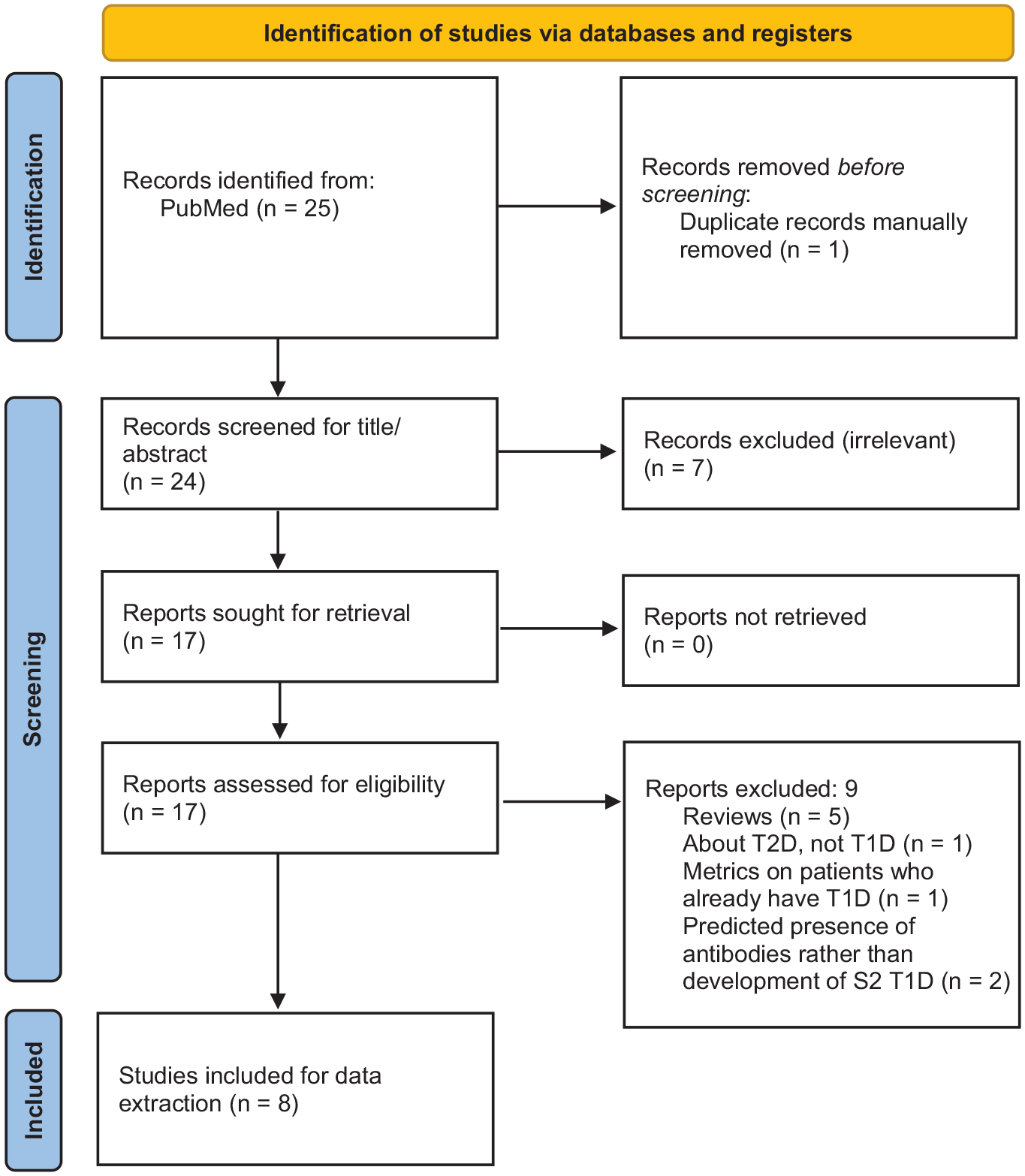
PRISMA diagram summarizing the search process to identify studies that use CGM metrics to predict the development of symptomatic T1D. Adapted from Page et al 13 under the CC-By 4.0 license (https://creativecommons.org/licenses/by/4.0/).
These eight individual reports have concluded various CGM metrics to be consistent with dysglycemia, as presented in Table 2.
Results From Studies Using CGMs to Monitor Progression of T1D to Stage 2 T1D.

Use of continuous glucose monitoring to identify asymptomatic dysglycemia in the assessment of stage 1 T1D to determine whether the disease has progressed to stage 2 T1D.
Abbreviations: AUC, area under the curve; CGM, continuous glucose monitoring; CV, coefficient of variation; GV, glucose variation; HbA1c, hemoglobin A1c; IAb+, positive islet autoantibodies; IAb–, negative islet autoantibodies; M120–150 minutes, glucose disposal rate; milligram/deciliter (mg/dL); OGTT, oral glucose tolerance test; SD, standard deviation; SMBG, self-monitored blood glucose; S2, stage 2; S3, stage 3; T1D, type 1 diabetes mellitus; TIR, time in range.
Seven7,14-19 of these eight studies concluded that certain CGM metrics may be helpful in detecting progression to S3 T1D, and five14,16-19 of these seven studies found that time spent with blood glucose (BG) ≥ 140 milligram/deciliter (mg/dL) is a statistically significant predictor of progression to stage 3 T1D. For instance, Steck et al 18 found that progressors spent 21% of time ≥ 140 mg/dL compared with 3% for nonprogressors (P < .0001) and concluded that > 10% of time with BG > 140 mg/dL is associated with a high risk of progression to stage 3 diabetes within one year for autoantibody positive children. On the other hand, Ylescupidez et al 20 found that although certain CGM metrics may indicate the eventual development of T1D, measurements derived from OGTTs had higher statistical significance in predicting the development of T1D, and they therefore did not recommend using CGMs over OGTTs to predict progression to clinical T1D. Other CGM metrics that differed between progressors and nonprogressors in at least one of the eight studies included maximum daytime glucose, daytime area under the curve (AUC), mean glucose, variation in BG (range, standard deviation, mean amplitude of glucose excursions, coefficient of variation, and mean of daily differences), and time in range. However, no standardized or consensus recommendations exist on using CGM data to diagnosis dysglycemia in stage 2 T1D.
Continuous glucose monitoring is therefore a potentially useful tool for diagnosing dysglycemia in a population of children and adults who are at high risk for developing symptomatic T1D. After a patient and/or family is trained on use of a CGM, periodic CGM testing to evaluate glycemic metrics may be more convenient if the sensor can be placed in the home without a trip to a physician’s office or a laboratory. For many individuals, going to a laboratory for blood tests is so unappealing that for them to receive training for proper use of a CGM and placement of their initial CGM sensor will be less of a burden than phlebotomy.
The granularity of CGM data, compared with a few data points with self-monitoring of BG by glucose meter, or measurement of HbA1c that includes little information about glycemic variability, might potentially provide an accurate prediction of the onset of the third stage of T1D. A single CGM metric, such as the percentage of time spent with a specific range of BG concentrations may correlate closely with current widely recognized BG or HbA1c metrics for diagnosing stage 2 T1D. Alternatively, CGM data might be used to create a composite metric with the assistance of artificial intelligence (AI) that correlates with currently accepted BG or HbA1c concentrations diagnostic of stage 2 T1D. Artificial intelligence could be used to test millions of combinations of CGM metrics from ambulatory glucose profiles retrospectively with various weightings to identify a combination algorithm, compared with established BG and HbA1c concentrations diagnostic of stage 2 TID, with the maximum sensitivity and specificity. A prospective test of the algorithm could then be organized to test its accuracy. We anticipate that continuous glucose monitoring will become established in the assessment of early stages of T1D to identify the optimal time to offer prevention therapy during the progression from preclinical to symptomatic disease.
The following questions need to be addressed on the topic of the benefits of using continuous glucose monitoring to diagnose type 1 diabetes:
What is the optimal frequency of CGM testing to balance avoidance of excessive frequency to the point of resistance and inadequate frequency to the point of missed diagnoses?
Which individual or combined CGM metric(s) provides the best sensitivity and specificity for identifying stage 2 T1D, and what is the reference for this metric?
Does CGM testing reveal dysglycemia earlier or later on the continuum of stages than BG or HbA1c?
How does the human leukocyte antigen (HLA) type or family history affect CGM readings?
For people identified to have early dysglycemia by CGM testing that is not yet detected by other metabolic metrics, would an earlier start of preventative therapy change progression to stage 3 T1D and clinical outcomes?
Is a normal CGM report adequate to delay BG or HbA1c testing?
What level of accuracy for prediction is required for CGM to become a diagnostic test for stage 2 T1D, rather than adjunctive?
What type of modeling data can predict abnormal blood testing?
Which psychosocial factors should be taken into account regarding screening using CGMs?
Footnotes
Acknowledgements
The authors thank Annamarie Sucher-Jones for her expert editorial assistance.
Abbreviations
AI, artificial intelligence; AUC, area under the curve; CGM, continuous glucose monitor; CV, coefficient of variation; DKA, diabetic ketoacidosis; FDA, Food and Drug Administration; GV, glucose variation; HbA1c, hemoglobin A1c; HBGI, high blood glucose index; HLA, human leukocyte antigen; IAb, Islet autoantibody; IAb+, positive islet autoantibodies; IAb–, negative islet autoantibodies; M120-150 minutes, glucose disposal rate; milligram/deciliter (mg/dL); OGTT, oral glucose tolerance test; PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; SD, standard deviation; SMBG, self-monitored blood glucose; S2, stage 2; S3, stage 3; TIR, time in range; T1D, type 1 diabetes; T2D, type 2 diabetes.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: A.T.A. is a consultant for Liom.
C.N.H. is a consultant for Liom.
J.C.W. has nothing to disclose.
D.K. has received research funding from Abbott Diabetes Care.
J.K.M. is a member in the advisory boards of Abbott Diabetes Care, Becton-Dickinson/Embecta, Biomea, Eli Lilly, Medtronic, Novo Nordisk, Pharmasens, Roche Diabetes Care, Sanofi and Viatris, received speaker honoraria from Abbott Diabetes Care, A. Menarini Diagnostics, Becton-Dickinson/Embecta, Boehringer-Ingelheim, Eli Lilly, MedTrust, Novo Nordisk, Roche Diabetes Care, Sanofi, Servier and Ypsomed and is shareholder of decide Clinical Software GmbH and elyte Diagnostics.
DC.K. is a consultant for Afon, Atropos Health, embecta, Glucotrack, Lifecare, Novo, Samsung, Synchneuro, and Thirdwayv.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.