
Abstract
Background:
Managing glycemia during Ramadan is challenging for individuals with type 1 diabetes (T1D) due to prolonged fasting and altered eating patterns. While many are exempt from fasting, some choose to fast, necessitating careful monitoring. The glycemia risk index (GRI) is valuable for assessing glycemic quality and interpreting continuous glucose monitoring (CGM) data to identify individuals needing closer clinical attention. This study investigates the effects of Ramadan fasting on glycemic control in T1D, focusing on GRI and its components for hypoglycemia (CHypo) and hyperglycemia (CHyper).
Method:
An ambispective study involved 186 individuals with T1D using intermittent scanning CGM (isCGM). Data were retrospectively collected for one month before Ramadan and prospectively during and one month after Ramadan. Clinical, metabolic, and glycemic data were collected, with GRI calculated alongside its components.
Results:
During Ramadan, GRI improved by 54.6% (from 56.4 to 25.6), CHypo decreased by 60% (from 6 to 2.4), and CHyper dropped by 40.5% (from 21 to 12.5). However, these benefits were temporary, as glycemic measures increased after Ramadan, reflecting a return to pre-Ramadan patterns once normal routines resumed. No participants were admitted for diabetes emergencies during Ramadan. Adolescents and patients on insulin pumps had more favorable outcomes. GRI and its components significantly correlated with other CGM metrics, with these relationships maintained during and after Ramadan.
Conclusions:
Ramadan fasting significantly improved GRI and its components in individuals with T1D. Incorporating GRI as a novel metric alongside classical CGM metrics could enhance glycemic control, highlighting the need for personalized diabetes management strategies.
Keywords
Introduction
Ramadan, a month of fasting observed by Muslims worldwide, involves abstaining from food, drink, sexual activities, and any form of ingestion from dawn until sunset each day, with fasting durations ranging from 11 to 20 hours depending on geographic location and season.1,2 This practice presents unique challenges for individuals with type 1 diabetes (T1D). 3 While Islamic law allows exemptions for those with medical conditions, many individuals with T1D opt to fast during this period, often motivated by perceived benefits such as weight loss and the cessation of unhealthy habits.4 -6 The EPIDIAR study highlights this phenomenon, revealing that 42.8% of individuals with T1D fasted for at least 15 days during Ramadan. 7 Fasting can pose significant challenges, as evidenced by a study showing that 52% of participants experienced at least one episode of hypoglycemia during Ramadan. However, with appropriate education and monitoring, many could fast safely.8,9 This underscores the need for careful management in T1D patients who fast, as fasting alters dietary and lifestyle habits for 29 to 30 days. 10
One of the primary challenges faced by T1D patients during Ramadan is glycemic variability (GV), which is strongly linked to both acute and chronic complications, independent of HbA1c levels.11,12 Ramadan fasting, categorized as diurnal intermittent fasting, necessitates substantial modifications in self-management strategies, including insulin administration and self-monitoring, to mitigate risks such as hypoglycemia, hyperglycemia, and diabetic ketoacidosis (DKA). 13 The advent of continuous glucose monitoring (CGM) has transformed T1D management by providing real-time glucose data, which is crucial for managing GV and optimizing diabetes outcomes.11,14
The glycemia risk index (GRI) is a relatively novel metric that enhances the evaluation of glycemic control by capturing both hyperglycemic and hypoglycemic risks derived from CGM data. GRI offers a nuanced understanding of glycemic control, incorporating multiple dimensions of GV that are essential for effective T1D management.15 -17 Its ability to quantify the severity and risk associated with deviations from optimal glucose ranges allows clinicians to gain insights beyond average glucose exposure, highlighting dangerous fluctuations often overlooked by traditional metrics such as HbA1c.14,17,18 Thus, incorporating GRI into diabetes management can provide a comprehensive risk assessment, enabling personalized treatment adjustments to mitigate extremes in glucose levels and prevent diabetes-related complications.8,17,19,20
Despite the critical need, it remains unclear how Ramadan fasting affects GRI and CGM-derived metrics in individuals with T1D. In regions with high incidences of T1D, such as ours, where rates reach 33.5 cases per 100 000 people,21,22 evaluating these metrics is particularly critical. This study aims to investigate the impact of Ramadan fasting on GRI and its components, along with other CGM metrics, using real-world data from individuals with T1D who fast.
We hypothesize that fasting during Ramadan will improve GRI and its components—the hypoglycemia component (CHypo) and the hyperglycemia component (CHyper)—resulting in improved GV. This improvement is expected to stem from the structured eating patterns associated with fasting, which may foster more stable glycemic control. Moreover, we anticipate that this improvement will not be associated with an increase in admissions for diabetes emergencies during Ramadan, as indicated by earlier studies.9,23,24 GRI is expected to show a more pronounced improvement due to its comprehensive capture of hypoglycemic and hyperglycemic risks. Thus, incorporating GRI as a novel metric alongside classical CGM metrics could optimize management strategies during Ramadan, providing actionable insights that can improve clinical care.
Methods
Study Design
This ambispective, one-group pre-post study was conducted at the Department of Endocrinology and Diabetes in a major tertiary hospital in Saudi Arabia. Our Research and Ethics Committee approved the study protocol (IRB approval No: E-2277). The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines in its entirety 25 and followed the 1964 Helsinki Declaration and its subsequent amendments. 26
Eligibility Criteria
The study recruited individuals diagnosed with T1D for more than one year, aged 14 years or older, who had been using the isCGM FreeStyle Libre 2 (FSL2) system (Abbott Diabetes Care, Alameda, CA) for self-monitoring for at least three months. These participants, according to the Diabetes and Ramadan (DAR) guidelines,27,28 were eligible to fast, and they participated in Ramadan fasting in 2024. All participants were required to attend regular follow-up visits at the outpatient diabetes center of our institution and demonstrate at least 70% usage of the FreeStyle Libre system.
Exclusion criteria included individuals with type 2 diabetes (T2D), those diagnosed with T1D within the last year, individuals who had changed their insulin regimen or started continuous subcutaneous insulin infusion (CSII) therapy within the past three months, and those with less than 70% system usage over a 14-day period. In addition, individuals at very high risk, according to the DAR guidelines,27,28 were excluded. Other criteria for exclusion were a history of recent DKA episodes within three months prior to Ramadan, hypoglycemia unawareness, pregnancy, chronic kidney disease stages 4 and 5 or those on chronic dialysis, and significant macrovascular complications.
Study Procedure and Data Collection
Retrospective data were collected for the month prior to Ramadan, while prospective data were gathered during and after Ramadan. Routinely, all participants engage in a structured educational program two weeks before Ramadan. This program guides adjusting insulin doses, provides instructions on when to break the fast in response to signs of hyperglycemia or hypoglycemia, and emphasizes adherence to proper diet and exercise regimens as recommended by the DAR guidelines. Individuals in any risk strata of the IDF-DAR guidelines are advised to break their fast and seek immediate medical attention if they experience any documented episode of hypoglycemia or symptomatic hyperglycemia during Ramadan.28,29 Before enrolling in the study, participants were informed of their unconditional right to withdraw or break the fast at any time without providing a reason or prior notice. Both participants and their parents or caregivers were fully briefed about their roles in the study and signed informed consent forms before enrollment.
This study primarily focused on GRI and its components—CHypo and CHyper—in conjunction with other glycometric parameters. We collected system usage and metabolic control data by downloading and analyzing information from participants’ devices via the LibreView platform.
Glycemia risk index was calculated by integrating both CHypo and CHyper components. CHypo was derived from the classifications of time spent in low glucose ranges, defined as follows: very low glycemia was identified as %TBR<54, while low glycemia was determined as %TBR54-69. The CHypo was computed using the formula: CHypo= [%TBR<54 + (0.8×%TBR54-69)]. Conversely, CHyper was calculated by categorizing time spent in elevated glucose ranges, with high glycemia categorized as %TAR181-250 and very high glycemia as %TAR>250. The CHyper was calculated as follows: CHyper= [%TAR>250 + (0.5×%TAR181-250]. GRI was then determined using the following formula: GRI=[(3.0×CHypo)+(1.6×CHyper)].17,20 A 14-day period of CGM data has recently been recognized as the optimal duration for calculating GRI. 30
In addition to GRI, we analyzed several key glycometric parameters to further characterize participants’ metabolic control. These included mean glucose levels (mg/dL), the Glucose Management Indicator (GMI%), the percentage of time in range (%TIR70-180) defined as glucose levels between 70 and 180 mg/dL, the percentage of time above range (%TAR>180) for glucose levels exceeding 180 mg/dL, and the percentage of time below range (%TBR<70) for glucose levels below 70 mg/dL. We assessed GV through the coefficient of variation (CV%).
Statistical Analysis
The analysis was conducted using SPSS version 28.0 (SPSS Inc., Chicago, IL, USA) and RStudio version R 4.3.0. The normal distribution of variables was assessed using the Kolmogorov-Smirnov test. Quantitative data with a normal distribution were presented as mean and standard deviation (SD), while nonnormally distributed data were described using the median and interquartile range (IQR, 25th-75th percentile). Categorical variables were expressed as frequencies and percentages. Various methods were utilized to evaluate the changes in glucose metrics across multiple time points and among different subgroups. A repeated measures analysis of variance (ANOVA) using the Friedman test was employed to assess changes in glycometric parameters before, during, and after Ramadan. To delve deeper into specific differences highlighted by the Friedman test, pairwise comparisons were conducted using the Durbin-Conover method, allowing for a detailed assessment between each pair of time points. In addition, subgroup analysis was performed to explore distinct responses among various participant groups within the study (age groups and treatment modality), leveraging the Wilcoxon rank-sum test for comparisons where data did not follow a normal distribution. For this study, adolescents were defined as individuals aged 19 years or younger, per the World Health Organization classification. 31 The Chi-square test was employed to analyze categorical data within the study. Spearman’s correlation coefficient (r) was used to determine the correlation between quantitative variables, with the strength of the correlation ranging from 0 to ±1. Statistical significance was set at P-values less than .05.
Results
Demographic Characteristics and Glycemic Risk Components
The study cohort consisted of 186 participants (58.1% males, 41.9% females) with a median age of 17 years (IQR: five years) and a median duration of diabetes of nine years (IQR: four years). Participants were predominantly treated using multiple daily injections (MDI), with 134 individuals (72.0%) following this regimen, while 52 participants (28.0%) were managed with insulin pump therapy (IPT). Table 1 details the baseline clinical and metabolic characteristics of the study participants. Prior to Ramadan, the Chypo and Chyper components had medians of six (IQR: 5.8) and 21 (IQR: 12.5), respectively, and the overall GRI was 56.4 (IQR: 39.1), Table 1. During Ramadan, participants fasted for a median of 29 days. Notably, no hospitalizations were recorded for emergencies such as DKA, hypoglycemia, or hyperglycemia throughout the fasting period.
Baseline Clinical and Metabolic Characteristics of Study Participants.
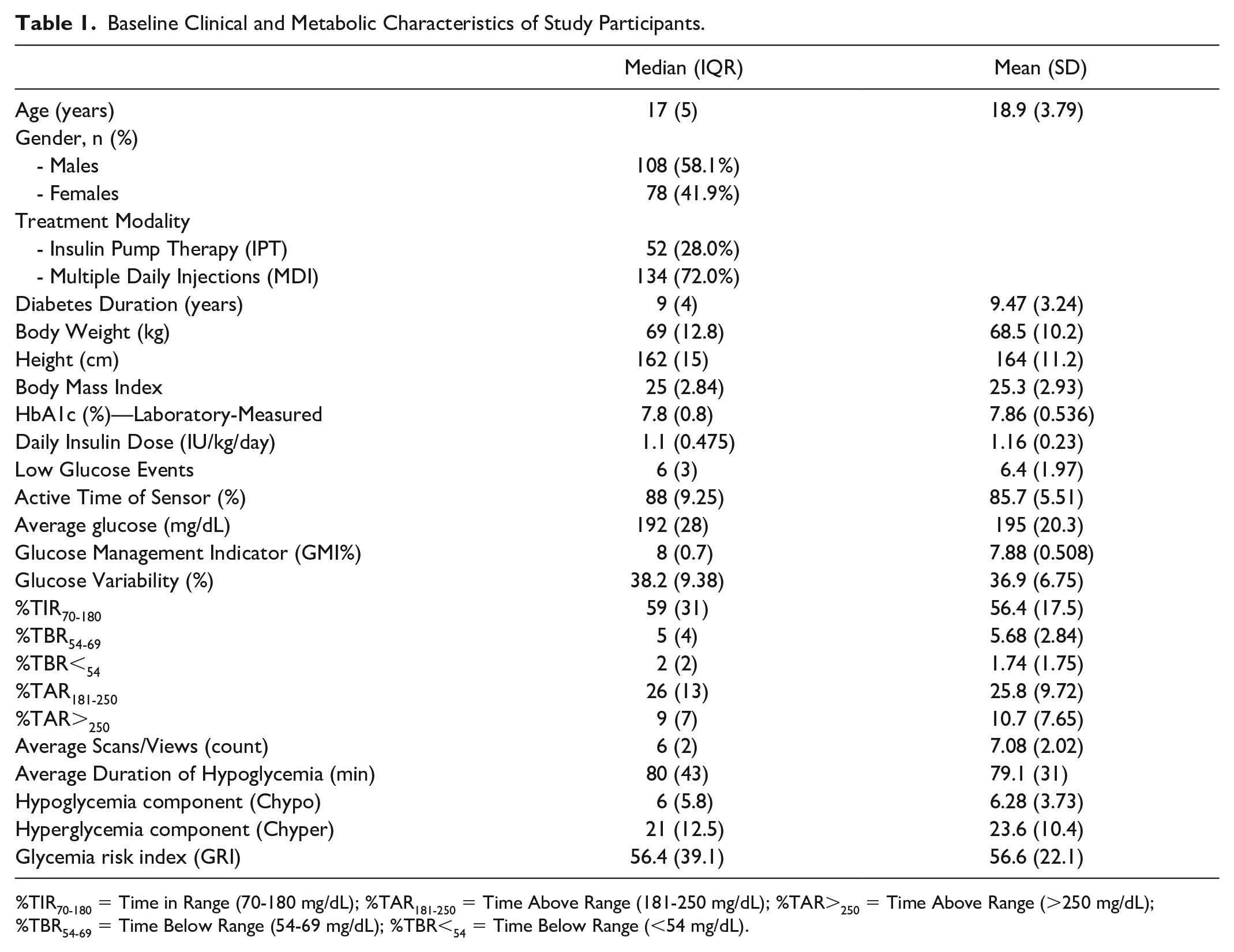
%TIR70-180 = Time in Range (70-180 mg/dL); %TAR181-250 = Time Above Range (181-250 mg/dL); %TAR>250 = Time Above Range (>250 mg/dL); %TBR54-69 = Time Below Range (54-69 mg/dL); %TBR<54 = Time Below Range (<54 mg/dL).
The median body mass index was 25 kg/m² (IQR: 2.84 kg/m²), with a median HbA1c of 7.8% (IQR: 0.8%). Participants experienced a median of six low glucose events (IQR: 3), with an average duration of hypoglycemia per event of 80 minutes (IQR: 43). Sensor active time was high, with a median of 88% (IQR: 9.25%). The average glucose level was 192 mg/dL (IQR: 28 mg/dL), with a GMI of eight (IQR: 0.7) and GV of 38.2% (IQR: 9.38%) (Table 1).
Supplemental Table S1 highlights significant clinical and metabolic differences between adolescents and adults. Median values for Chypo and GRI were significantly higher in adults (7.6 and 58.0, respectively) compared with adolescents (5.0 and 54.2), with P < .01 for both. In contrast, Chyper values were similar between the two groups, with a median of 21 for both (P = .15). Moreover, both GRI components were lower in IPT users, with Chypo at 4.0 and Chyper at 16.5, compared with MDI users, who had Chypo at 6.0 and Chyper at 26.0 (P < .01 for both). In addition, GRI was significantly lower in IPT users (43.0) than in MDI users (62.0), P < .01 (Supplemental Table S2).
Adults exhibited a higher average glucose level (195.0 mg/dL) and greater GV (39.2%) compared with adolescents (188.0 mg/dL and 35.8%, respectively), while adolescents showing a higher %TIR70-180 (P < .01), Supplemental Table S1. Average glucose was also lower in IPT users (186 mg/dL) versus MDI users (196 mg/dL), with less GV (IPT: 35.1%, MDI: 38.9%, P < .01). IPT users required a lower daily insulin dose (0.9 IU/kg for IPT vs 1.3 IU/kg for MDI) and had a higher %TIR70-180 (IPT: 66%, MDI: 50%, P < .01), Supplemental Table S2.
Comparative Analysis of Glycemic Parameters During and After Ramadan
Chypo scores significantly dropped during Ramadan, from a median of 6 before to 2.4 during fasting, then rose to eight post-Ramadan (P < .001). Chyper scores also showed significant changes, decreasing from 21 before Ramadan to 12.5 during, and rising to 18.5 afterward, remaining below baseline yet reflecting only partial retention of Ramadan benefits (P < .001). Both GRI and GV improved during Ramadan, with GRI reducing from 56.4 to 25.6 and returning to 53 after one month (P < .001). GV decreased from 38.2% to 30.1%, indicating more stable glucose levels, before returning close to pre-Ramadan values (Figure 1 and Table 2).
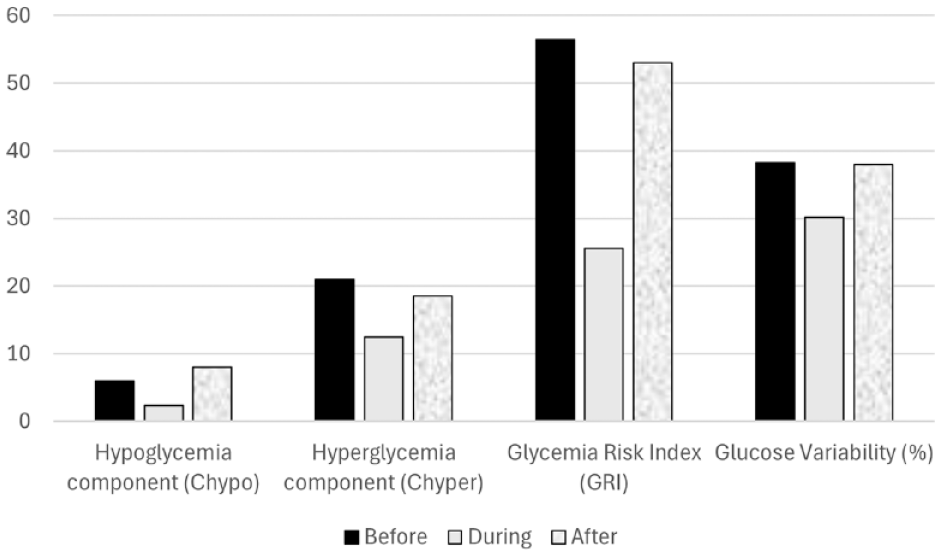
Variations in hypoglycemia, hyperglycemia, glycemia risk index, and glucose variability metrics before, during, and after Ramadan.
Comparative Analysis of Metabolic and Glycemic Parameters Before, During, and After Ramadan.
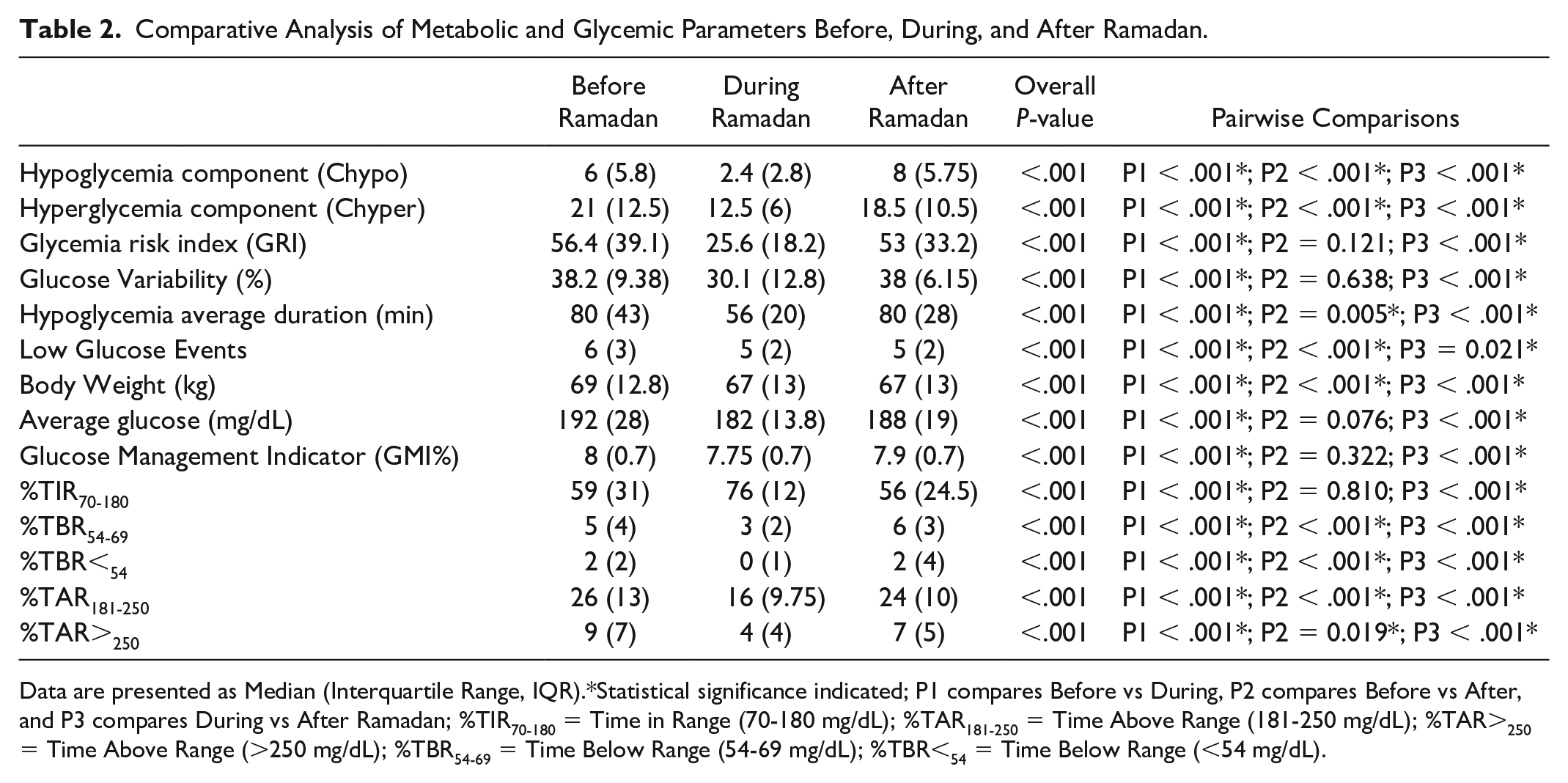
Data are presented as Median (Interquartile Range, IQR).*Statistical significance indicated; P1 compares Before vs During, P2 compares Before vs After, and P3 compares During vs After Ramadan; %TIR70-180 = Time in Range (70-180 mg/dL); %TAR181-250 = Time Above Range (181-250 mg/dL); %TAR>250 = Time Above Range (>250 mg/dL); %TBR54-69 = Time Below Range (54-69 mg/dL); %TBR<54 = Time Below Range (<54 mg/dL).
Average glucose levels and GMI improved during Ramadan, decreasing from 192 mg/dL before to 182 mg/dL during, then rising slightly to 188 mg/dL one month later. Glucose management indicator also improved from eight to 7.75 during Ramadan, then slightly increased to 7.9 afterward, with significant changes noted (P < .001). Low glucose events decreased from six to five during and after Ramadan, achieving statistical significance (P < .05). As shown in Figure 2 and Table 2, %TIR70-180 increased significantly from 59% to 76% during Ramadan (P < .001) but dropped to 56% after, returning near baseline levels (P = 0.81). %TBR and %TAR improved during Ramadan with less time in hypo- and hyperglycemic states (P < .001). Body weight significantly decreased from a median of 69 kg before fasting to 67 kg during and remained lower after Ramadan (Table 2).
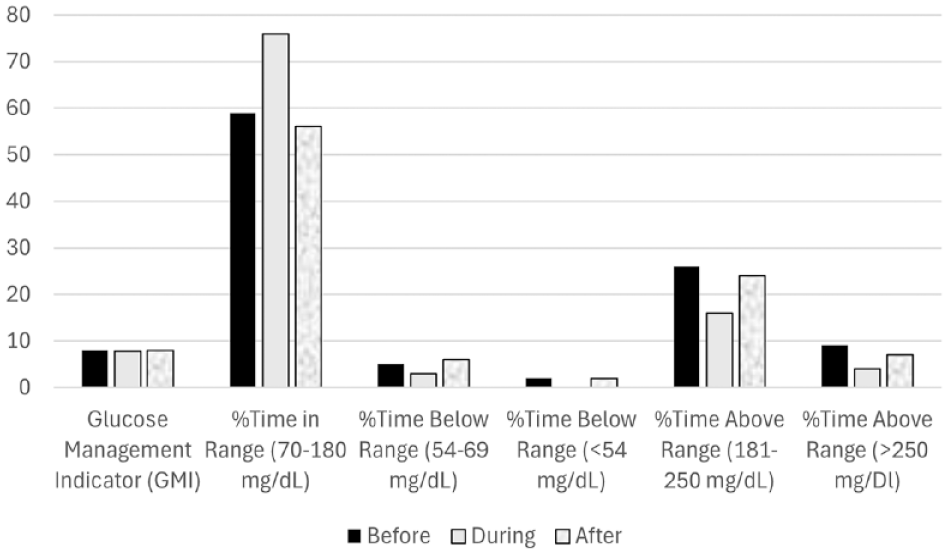
Changes in time spent within various glucose ranges before, during, and after Ramadan.
Comparative Analysis of Glycemic Metrics by Age Groups
Supplemental Table S3 presents a detailed evaluation of various metabolic and glycemic parameters across three periods—before, during, and after Ramadan—differentiated by age group. Chypo and Chyper scores significantly improved during Ramadan (Supplemental Figure S1), with adolescents decreasing from 5.0 to 2.4 (Chypo) and from 21 to 11 (Chyper), while adults decreased from 7.6 to 3.2 (Chypo) and from 21 to 15 (Chyper). Glycemia risk index also showed significant improvement, dropping from medians of 54.2 to 23.6 in adolescents and 58.0 to 35.9 in adults. However, slight regressions were observed one month later, indicating that the adjustments in diabetes management during fasting were temporary. Glycemic variability decreased for both groups during Ramadan, with no significant differences observed between the groups during this period (P = .16) and one month later (P = .06).
Both groups experienced a significant difference in low glucose events before Ramadan (adolescents at 6.0 and adults at 8.0); these differences did not persist during or after Ramadan (P = .23 and P = .54). Average glucose levels decreased during Ramadan, with adolescents dropping from 188.0 to 181.5 mg/dL and adults from 195.0 to 183.0 mg/dL. Post-Ramadan levels rose slightly but remained significantly lower than pre-Ramadan levels. Glucose management indicator improved significantly during Ramadan but slightly increased one month later. Both adolescents and adults spent more time in the glucose range of 70-180 mg/dL during Ramadan (adolescents from 63.0% to 76.0% and adults from 45.0% to 70.0%). However, this improvement did not persist one month later, and no significant differences were observed between the groups (P = .21). Body weight significantly decreased during Ramadan, with adolescents showing a median reduction from 64.0 to 63.0 kg and adults from 80.0 to 78.5 kg. These changes persisted one month later, with significant differences between groups across all periods. Similar rates of diabetes-related fasting interruptions in both age groups during Ramadan were observed (P = .552), Supplemental Table S3.
Comparative Analysis of Glycemic Metrics by Treatment Modality
A comparative analysis of metabolic and glycemic parameters across the three distinct periods categorized by treatment modality is shown in Supplemental Table S4. During Ramadan, Chypo values decreased in both treatment groups (Supplemental Figure S1). For IPT users, the median Chypo dropped from 4.0 to 2.4, while MDI users experienced a similar decrease from 6.0 to 2.4. After Ramadan, Chypo values increased, reverting to pre-Ramadan levels, with medians rising to 6.8 for IPT users and 8.4 for MDI users, with no significant difference between both groups (P = .36). Chyper values also improved, with IPT users decreasing from 16.5 to 12.0 and MDI users from 26.0 to 12.5 during Ramadan. Afterward, median Chyper values rose to 18.0 for IPT users and 19.7 for MDI users, with no significant difference between both groups (P = .84). Glycemia risk index improved significantly for both groups during Ramadan, with IPT users’ median GRI decreasing from 43.0 to 23.6 and MDI users from 62.0 to 27.2. However, this improvement was not sustained one month later, with medians rising to 52.8 for IPT and 53.0 for MDI users. GV decreased significantly during Ramadan, with IPT users reducing from 35.1% to 24.1% and MDI users from 38.9% to 30.2%. One month later, GV slightly increased but did not return to pre-Ramadan levels, with significant differences between groups (P = .04).
Significant differences were observed in low glucose events between treatment modalities. Insulin pump therapy users experienced fewer events, decreasing from 5.0 before Ramadan to 4.5 during, and then stabilizing at 5.0 after one month. Multiple daily injections users had higher events before Ramadan at 7.0, decreasing to 5.0 during, but returning to 5.0 post-Ramadan. Both groups’ changes during Ramadan were statistically significant (P = .01), while post-Ramadan figures showed no significant differences (P = .79). Both IPT and MDI users exhibited significant improvements in average glucose levels and GMI during Ramadan; however, post-Ramadan levels showed a slight rebound toward pre-Ramadan values. In addition, both groups demonstrated notable enhancements in %%TIR70-180, with IPT users increasing from 66% to 79% and MDI users from 50% to 71%. Nevertheless, these gains were not fully maintained one month later, as IPT users decreased to 65% and MDI users to 56%. Similarly, %TAR>250 improved during Ramadan but regressed one month later. The analysis of diabetes-related broken fasting days showed no significant differences between IPT and MDI users (P = .259), Supplemental Table S4.
Correlation Analysis of Glycemic Indices and Their Interrelationships
Before Ramadan, Chypo and Chyper positively correlated with average glucose (r = .38 and r = .63), GMI (r = .44 and r = .62), GV (r = .49 and r = .63), %TBR54-69 (r = .96 and r = .25), %TBR<54 (r = .898 and r = .48), %TAR181-250 (r = .595 and r = .83), and %TAR>250 (r = .34 and r = .85). Glycemia risk index showed positive correlations with average glucose (r = .62), GMI (r = .59), GV (r = .6), %TBR54-69 (r = .57), %TBR<54 (r = .76), %TAR181-250 (r = .8), and %TAR>250 (r = .81). Chypo, Chyper, and GRI were negatively correlated with %TIR70-180 (r = -.56, r = -.74, and r = -.76). The correlations between the glycemic parameters and components such as Chypo, Chyper, and GRI were maintained during and after Ramadan (Figures 3-5).
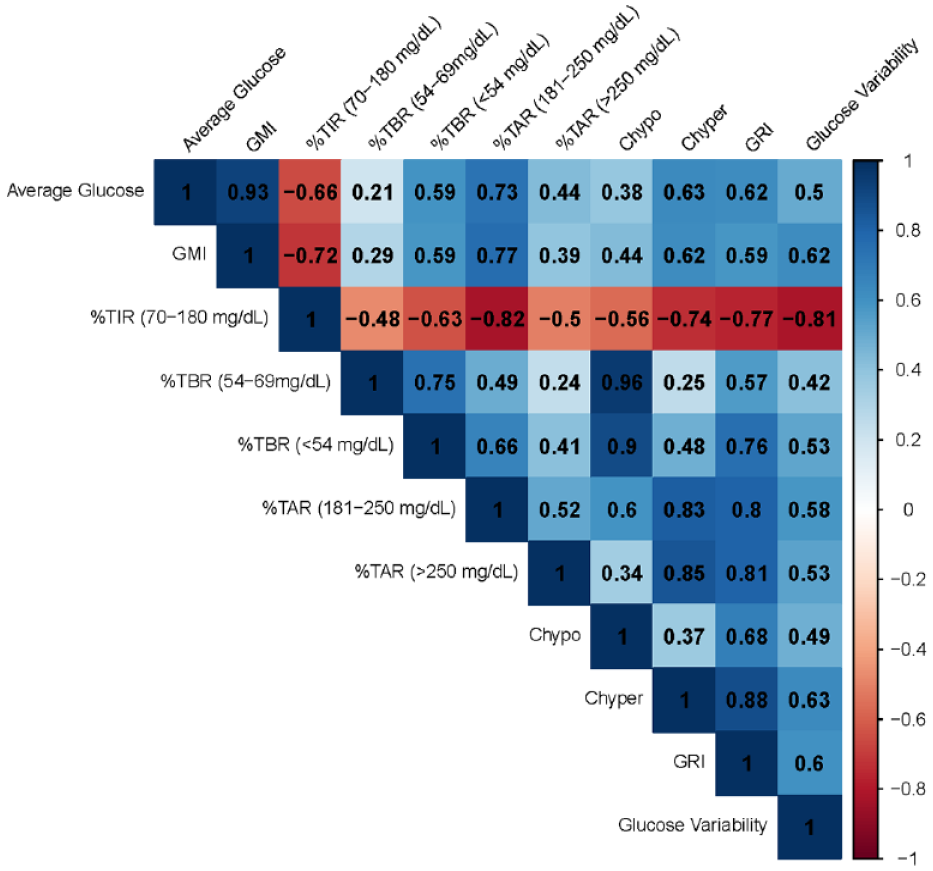
Correlation plot visually represents the relationships between various glycemic-related metrics before Ramadan.
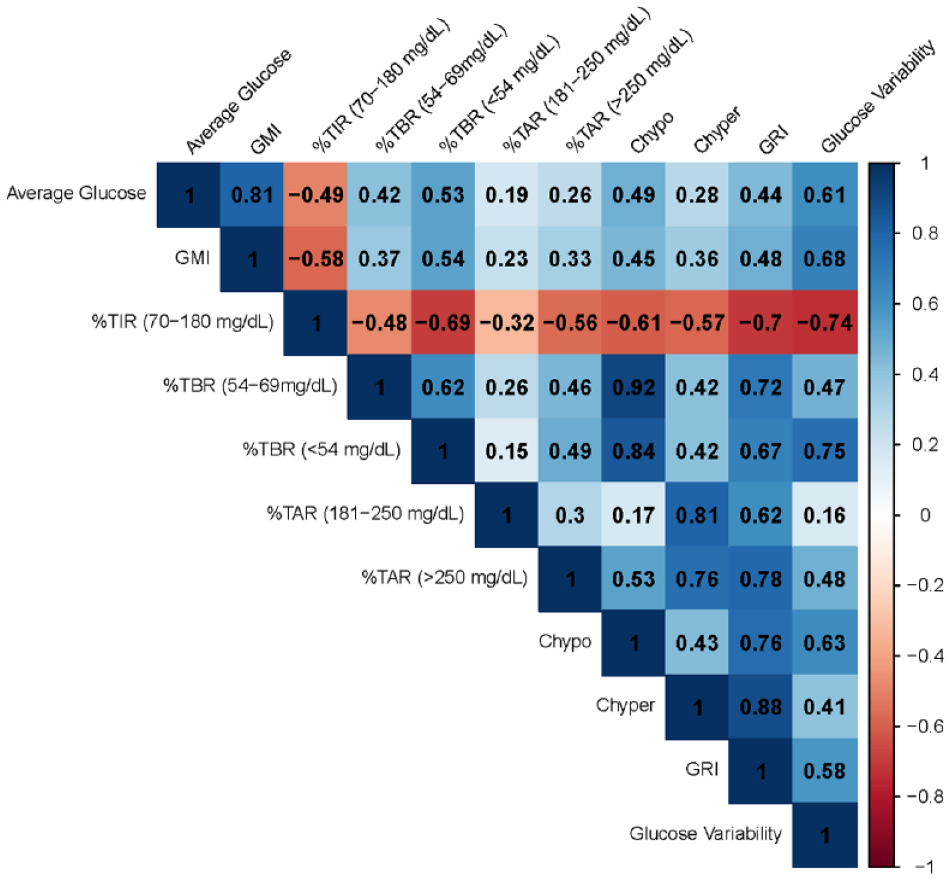
Correlation plot visually represents the relationships between various glycemic-related metrics during Ramadan.
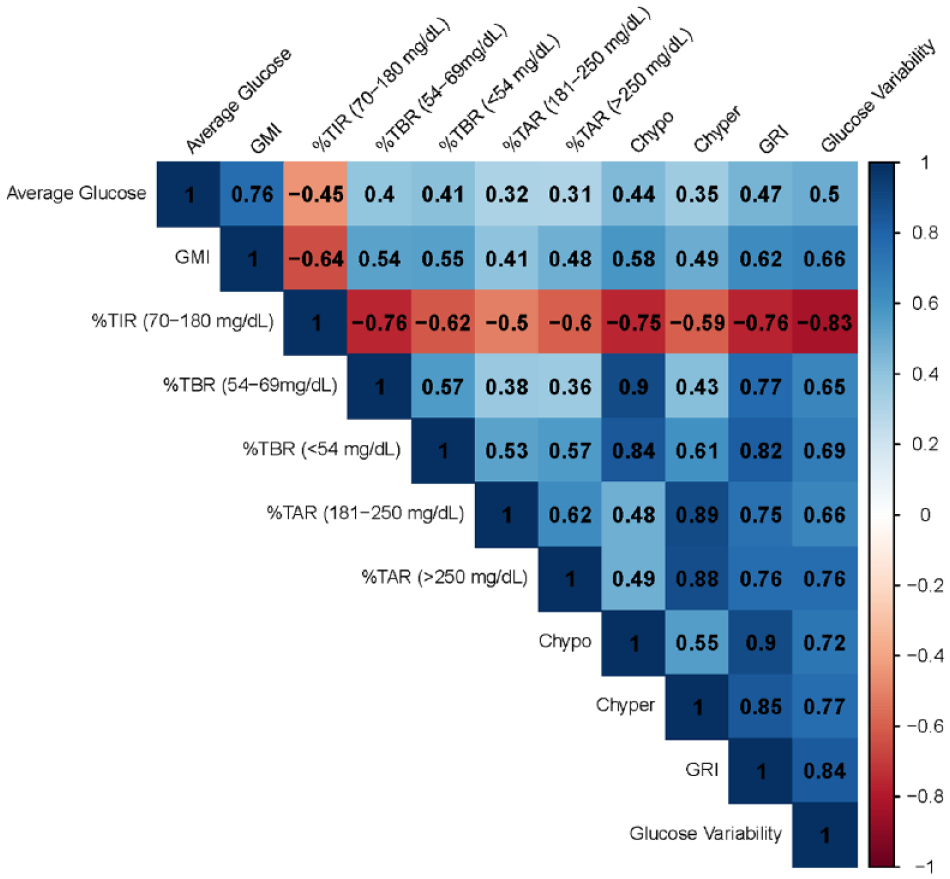
Correlation plot visually represents the relationships between various glycemic-related metrics after Ramadan.
Discussion
This study explored how Ramadan fasting influences GRI and its components, along with various CGM-derived metrics. The objective is to generate practical insights that will improve clinical management and optimize diabetes care throughout the Ramadan period. Overall, the study revealed notable improvements in glycemic outcomes during Ramadan, but these benefits were not entirely sustained one month after, highlighting the temporary nature of fasting-related improvements. Recommendations suggest that individuals with T1D who are considering fasting consult with their physician to thoroughly assess potential risks. A comprehensive pre-Ramadan health evaluation is essential for those opting to fast. In addition, patients should receive guidance on physical activity, meal planning, glucose monitoring, and appropriate medication adjustments.32,33 An individualized management plan, along with regular follow-up care, is critical to minimizing risks and preventing complications. 32
Glycemia risk index is a composite measure that assesses both hyperglycemic and hypoglycemic risks, offering a more detailed view of glucose control than traditional metrics. It emphasizes glycemic extremes, making it crucial for predicting complications.16,17,34 Regarding GRI, we observed a significant reduction during Ramadan, decreasing from 56.4 to 25.6. This indicates that structured fasting profoundly impacts stabilizing blood glucose levels in individuals with T1D. Such findings align with prior research, demonstrating that well-organized fasting periods can significantly reduce the glycemic burden in individuals with diabetes. 35 However, a key challenge arises in maintaining these improvements after Ramadan, as individuals return to regular eating patterns and less structured insulin management. This pattern has been similarly documented in studies involving individuals with T1D, highlighting the need for long-term strategies to preserve fasting-associated benefits. 36
The reduction in GRI during Ramadan carries critical clinical implications, particularly in terms of reducing its components, Chypo and Chyper. In this study, Chypo significantly decreased from 6 to 2.4, demonstrating that structured insulin management and meal planning effectively minimized the risk of hypoglycemia. 37 Likewise, Chyper reduced from 21 to 12.5, indicating improved hyperglycemia control, often linked to overeating during Iftar (the meal that breaks the fast) and improper insulin dosing. These improvements support the importance of structured insulin and meal schedules during Ramadan, as documented in prior studies. 38
Despite these positive outcomes during Ramadan, the partial reversion of GRI, Chypo, and Chyper post-Ramadan emphasizes the difficulty of sustaining glycemic control in the absence of structured management. Similar trends have been observed in other studies, suggesting that maintaining these benefits requires continuous structured care beyond the fasting period. 39 Insulin adjustments during Ramadan, particularly reductions in basal insulin and timing of doses to coincide with meal timings, have contributed to the reduced risk of hypoglycemia. However, basal insulin reduction alone may not always prevent symptomatic hypoglycemia, underscoring the need for individualized insulin regimens. 40
The role of CGM in managing T1D during Ramadan cannot be overstated. Continuous glucose monitoring supports real-time glucose tracking, enabling timely insulin adjustments and significantly lowering the risks of both hypoglycemia and hyperglycemia. Studies have shown that CGM use during Ramadan enhances glycemic outcomes by offering valuable insights into glucose fluctuations and optimizing insulin timing.41 -43 Post-Ramadan, the reversion of risk parameters highlights the need for continued CGM use and a gradual shift back to nonfasting insulin regimens to sustain the glycemic improvements achieved during Ramadan. 44
Building on the substantial improvements observed in key risk parameters like GRI, Chypo, and Chyper, our study also demonstrated significant enhancements in overall glycemic control and other glycometric measures during Ramadan fasting. These findings highlight the broader metabolic benefits of structured fasting beyond just risk reduction.
Fasting during Ramadan notably improved glycemic control in individuals with T1D, as average glucose levels dropped from 192 mg/dL to 182 mg/dL, while the GMI improved from 8.0% to 7.75%. These gains were further underscored by a marked increase in the %TIR70-180, rising from 59% to 76% during fasting. In addition, GV, measured by the CV%, also decreased from 38.2% to 30.1%. These findings are clinically relevant, as elevated GV has been associated with a higher risk of diabetes-related complications.11,12,45
Despite these improvements during fasting, there was a partial reversion post-Ramadan, with average glucose levels rising to 188 mg/dL and %TIR70-180 decreasing to 56%. This highlights the importance of structured post-Ramadan interventions, such as ongoing diabetes education and regular follow-ups, to sustain these glycemic improvements and minimize GV.9,37 Our study found no increase in low glucose events during or after Ramadan, with the median number of events stable at six before, five during, and five after one month. The average duration of hypoglycemia decreased from 80 minutes pre-Ramadan to 56 minutes during fasting but returned to 80 minutes post-Ramadan. This aligns with previous studies showing either similar hypoglycemia rates to nonfasting T2D patients or no significant changes in glucose fluctuations.46,47
When examining subgroup differences by age, consistent patterns emerged regarding the impact of Ramadan fasting on risk parameters. Adolescents demonstrated better control, as indicated by higher %TIR70-180 and lower GRI scores, with their %TIR70-180 increasing from an average of 63% pre-Ramadan to 76% during fasting. In contrast, adults started with a lower %TIR70-180 (45%), and although they showed improvements during Ramadan, their overall glycemic control remained less favorable. Factors contributing to adolescents’ improved control include greater insulin sensitivity, shorter diabetes duration, consistent meal timing, and more frequent CGM use. 20 Both age groups exhibited partial reversion of glycemic improvements post-Ramadan; however, adolescents maintained better levels than their prefasting values, while adults experienced a higher GRI. This suggests that fasting can lead to temporary improvements across all age groups, but adults may require more frequent monitoring and personalized adjustments after Ramadan.
The study also explored the impact of insulin delivery methods on glycemic control during Ramadan, comparing IPT with MDI. Results indicated that IPT users experienced better glycemic control during fasting. GV decreased more substantially in IPT users, from 35.1% pre-Ramadan to 24.1% during fasting, compared with MDI users, whose GV decreased from 38.9% to 30.2%. Supporting literature has shown that IPT can improve GV, although no significant differences were found in hypoglycemia or hyperglycemia rates.48,49 In addition, IPT’s ability to provide tailored insulin dosing is particularly beneficial during fasting, where insulin requirements fluctuate. This flexibility, along with reduced injection frequency, facilitates better management of unexpected glucose fluctuations during fasting. Post-Ramadan, IPT users maintained better glycemic control, whereas MDI users experienced more substantial increases in GRI.
Participants in this study experienced a significant reduction in body weight during Ramadan, decreasing from a median of 69 to 67 kg, with this weight loss sustained one month post-Ramadan. This aligns with findings in T2D studies, where weight loss during Ramadan has been reported.50,51 Sustained weight loss may enhance glycemic control by improving insulin sensitivity and reducing GV, ultimately benefiting overall health outcomes.52 -54
Our study found that no hospitalizations for diabetic emergencies occurred throughout the fasting period. This observation aligns with previous research, suggesting that the incidence of diabetes-related emergencies during Ramadan fasting may not be as significant as often perceived. For instance, a study by Akram et al 23 reported no increase in emergency room visits for patients with diabetes during Ramadan compared with other lunar months. Moreover, a cross-sectional prospective study by Tong et al, 24 conducted in 18 public hospitals, found that admissions were highest pre-Ramadan. The authors concluded that fasting during Ramadan does not increase admissions for diabetes emergencies. This similarity in findings underscores the effectiveness of diabetes management strategies among individuals who fast, highlighting a shared understanding of how to navigate dietary changes during Ramadan. Understanding the relationship between fasting, diabetes management, and emergency health care needs is crucial for optimizing outcomes for patients with diabetes during this period.
Before Ramadan, we observed strong positive correlations between glycemic parameters—such as average glucose, GMI, and GV—and GRI, as well as its components, Chypo and Chyper. These correlations suggest that higher average glucose levels and greater GV contribute to an increased risk of both hypo- and hyperglycemia. This aligns with findings from prior studies indicating that higher glycemic fluctuations are associated with greater glycemic risk and poor diabetes outcomes.20,55 -57 Another key finding was the strong negative correlation between %TIR70-180 and both GRI, Chypo, and Chyper. The more time patients spend within the target glucose range (70-180 mg/dL), the lower their risk for both hypoglycemia and hyperglycemia. This underscores the importance of increasing %TIR70-180 as a primary strategy for reducing overall glycemic risk. Studies have consistently shown that a higher %TIR70-180 is associated with better long-term diabetes outcomes, including lower risks of microvascular and macrovascular complications and improved overall quality of life.58 -62 Interestingly, these correlations were maintained during and after Ramadan. Despite the overall reduction in GRI, Chypo, and Chyper during fasting, the association between higher glucose levels and increased glycemic risk remained consistent. This highlights the predictive value of these metrics for assessing overall glycemic risk across different periods. The persistence of these correlations suggests that, regardless of fasting status, average glucose and GV remain key determinants of glycemic risk.
Recent studies highlight that dietary patterns focused on macronutrient balance, rather than simply caloric intake, are crucial for managing GV in T1D.63 -66 Zhou et al 63 demonstrated that the distribution of carbohydrates, fats, and proteins is key to reducing hypoglycemia risks, while Lin et al 67 found that a daily carbohydrate intake below 50% combined with moderate protein effectively reduced glycemic fluctuations, especially overnight. Further evidence showed that a modified DASH diet low in carbs improved GV and reduced hypoglycemia in adolescents, 68 while another research emphasized the benefits of meal consistency and macronutrient balance with preprandial insulin. 69 More recently, Cristello et al 65 further validated that “Structured Eating”—with consistent timing and macronutrient balance—enhanced CGM metrics, supporting stable blood glucose levels, especially during fasting periods like Ramadan.
Linking these findings to the GRI during Ramadan, a macronutrient-focused, structured eating approach appears promising for minimizing GV and reducing hypoglycemic risk. By prioritizing balanced carbohydrate intake and consistent meal timing, as observed in “Structured Eating” strategies, T1D patients may achieve more stable glucose levels, which should positively reflect on GRI scores by limiting hypoglycemic events. Based on our results, we expect that implementing a controlled dietary structure during Ramadan fasting can help limit GV and is likely to reduce the GRI, particularly by decreasing hypoglycemic fluctuations during extended fasting periods.
Strengths and Limitations
This study presents the first data on GRI during Ramadan in our region, representing a significant advancement in understanding glycemic T1D during Ramadan fasting. Using real-world data provides relevant insights for clinical practice by incorporating a range of glycemic metrics beyond traditional markers. This approach aims to enhance our understanding of glucose stability and associated risks during Ramadan fasting. Despite its strengths, the study has several limitations. The follow-up period was relatively short, encompassing one month prior to Ramadan, Ramadan month, and one month following Ramadan. This timeframe primarily focused on outcomes during fasting, yielding limited data on how glucose control is managed postfasting. Consequently, the sustainability of any glycemic improvements observed during Ramadan and subsequent management of glucose levels remain uncertain. In addition, the specific geographic population studied may limit the generalizability of the findings to broader T1D populations in different regions and health care settings. The observational nature of the study may introduce potential biases, particularly reporting bias in self-reported data regarding hypoglycemia episodes and adherence to insulin regimens. Furthermore, these findings may not be generalizable to individuals with hypoglycemia unawareness, pregnant individuals, those with chronic kidney disease stages 4 and 5, those undergoing chronic dialysis, or those with significant macrovascular complications. While real-world data provide valuable insights, such biases may affect the accuracy and reliability of the reported outcomes.
Clinical Implications and Recommendations
The findings from this study provide insights that can inform the clinical management of T1D during and after Ramadan. The observed improvements in glycemic control highlight the importance of personalized insulin management plans. Clinicians should tailor both basal and bolus insulin dosing to accommodate fasting periods and meal timings, such as Iftar and Suhoor. Structured education programs prior to Ramadan are crucial for preparing patients. Comprehensive guidance on adjusting insulin doses, regular glucose monitoring, and understanding fasting-related risks, including hypoglycemia and DKA, is essential. Evidence suggests that such educational interventions can enhance glycemic outcomes during Ramadan and promote safer fasting practices.37,70 -72 Looking ahead, future research could focus on exploring the long-term effects of Ramadan fasting on glycemic control. Understanding how fasting influences GRI, GV, insulin requirements, and long-term diabetes complications may provide insights for developing sustained interventions.
Conclusion
This study demonstrates that Ramadan fasting improves short-term glycemic control in T1D patients, evidenced by significant reductions in GRI and its components (Chypo and Chyper), along with decreased GV and increased %TIR70-180. Our study findings highlight the incorporation of GRI as a novel metric alongside classical CGM metrics. This dual approach enhances our understanding of glucose stability and facilitates tailored management strategies to address the unique challenges faced by T1D patients during Ramadan fasting. Using both metrics, clinicians can make more informed decisions regarding insulin management and patient education, ultimately optimizing glycemic control throughout fasting periods.
Supplemental Material
sj-docx-1-dst-10.1177_19322968241301750 – Supplemental material for Improvement of Glycemia Risk Index and Continuous Glucose Monitoring Metrics During Ramadan Fasting in Type 1 Diabetes: A Real-World Observational Study
Supplemental material, sj-docx-1-dst-10.1177_19322968241301750 for Improvement of Glycemia Risk Index and Continuous Glucose Monitoring Metrics During Ramadan Fasting in Type 1 Diabetes: A Real-World Observational Study by Ayman Al Hayek and Mohamed A. Al Dawish in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
Editorial assistance was provided by Dr Mahmoud A. Ebada, MD. The article processing charges were funded by Roche Diagnostics KSA.
Abbreviations
CGM, continuous glucose monitoring; CHyper, hyperglycemia component; CHypo, hypoglycemia component; CSII, continuous subcutaneous insulin infusion; CV, coefficient of variation; DKA, diabetic ketoacidosis; FSL2, FreeStyle Libre 2; GMI, glucose management indicator; GRI, glycemia risk index; GV, glycemic variability; HbA1c, glycated hemoglobin; IPT, insulin pump therapy; IQR, interquartile range; MDI, multiple daily injection (therapy); SPSS, statistical package for the social sciences; STROBE, strengthening the reporting of observational studies in epidemiology; T1D, type 1 diabetes; T2D, type 2 diabetes; %TAR, time above range; %TBR, time below range; %TIR, time in range.
Author Contributions
AA contributed to the study’s conception and design. Material preparation, data collection, and analysis were performed by AA and MAA. All authors contributed to the writing of the first draft of the manuscript. AA revised the manuscript critically for important intellectual content. All authors approved the final version of the manuscript.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
This study was performed in line with the principles of the Declaration of Helsinki. Approval was granted by our Ethics Committee (No: E-2277)
Consent to Participate
All participants provided informed consent to partake in the study. Before enrollment, they were thoroughly briefed on the study’s aims, potential risks, and benefits. Participants were informed of their right to withdraw from the study at any point without penalty or loss of benefits to which they are otherwise entitled. For participants under the age of 18, informed consent was obtained from a parent or legal guardian.
Consent to Publish
Not applicable.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.