
Abstract

People with type 1 diabetes (T1D) receiving hemodialysis (HD) are prone to glycemic variability and hemoglobin abnormalities, limiting the utility of traditional capillary point-of-care (POC) blood glucose (BG) monitoring and hemoglobin A1c (HbA1c), respectively. Continuous glucose monitoring (CGM) may overcome such limitations. 1 However, according to manufacturer instructions, use of some devices (including Dexcom G5/G6/G7, FreeStyle Libre1/Libre2/Libre3) is not recommended with HD, due to insufficient accuracy evaluations.
With diabetes prevalence in hospital increasing, 2 and CGM uptake in people with T1D increasing, there is both opportunity and need for CGM accuracy assessment amongst inpatients with T1D receiving HD.
We conducted a multicenter retrospective study, across three health services (ethics approvals: QA23-105-102749; QA2023122; SSA/103943/PH-2023), of adult inpatients with T1D receiving chronic HD, who required multiday acute hospital admissions between July 2020 and December 2023. Patients using their own FreeStyle Libre2 (Abbott Diabetes Care Inc, VIC, Australia) or Dexcom G6 (DexCom Inc, CA, USA) in hospital (linked to hospital Libreview and Clarity accounts, respectively) were included.
Point-of-care testing was via Accu-Chek Guide (Roche Diabetes Care, Rotkreuz, Switzerland), Nova StatStrip (Nova Biomedical, MA, USA), or FreeStyle Optium Neo H (Abbott Diabetes Care, CA, USA); blood gas (GAS) testing was via GEM5000 (Werfen, Barcelona, Spain), or ABL90/ABL800 FLEX (Radiometer, Copenhagen, Denmark), according to study site.
In total, 290 time-matched (±5 minutes) CGM and reference glucose pairs (mean BG 203 mg/dL, SD 102 mg/dL) were obtained in 22 admissions (G6 used in 13; Libre2 in nine), from 10 patients (five male; five female). Median (IQR) age was 44 years (37-53), Charlson comorbidity index six (5-6), and admission duration six days (3-12). Mean HbA1c was 67 mmol/mol (8.3%).
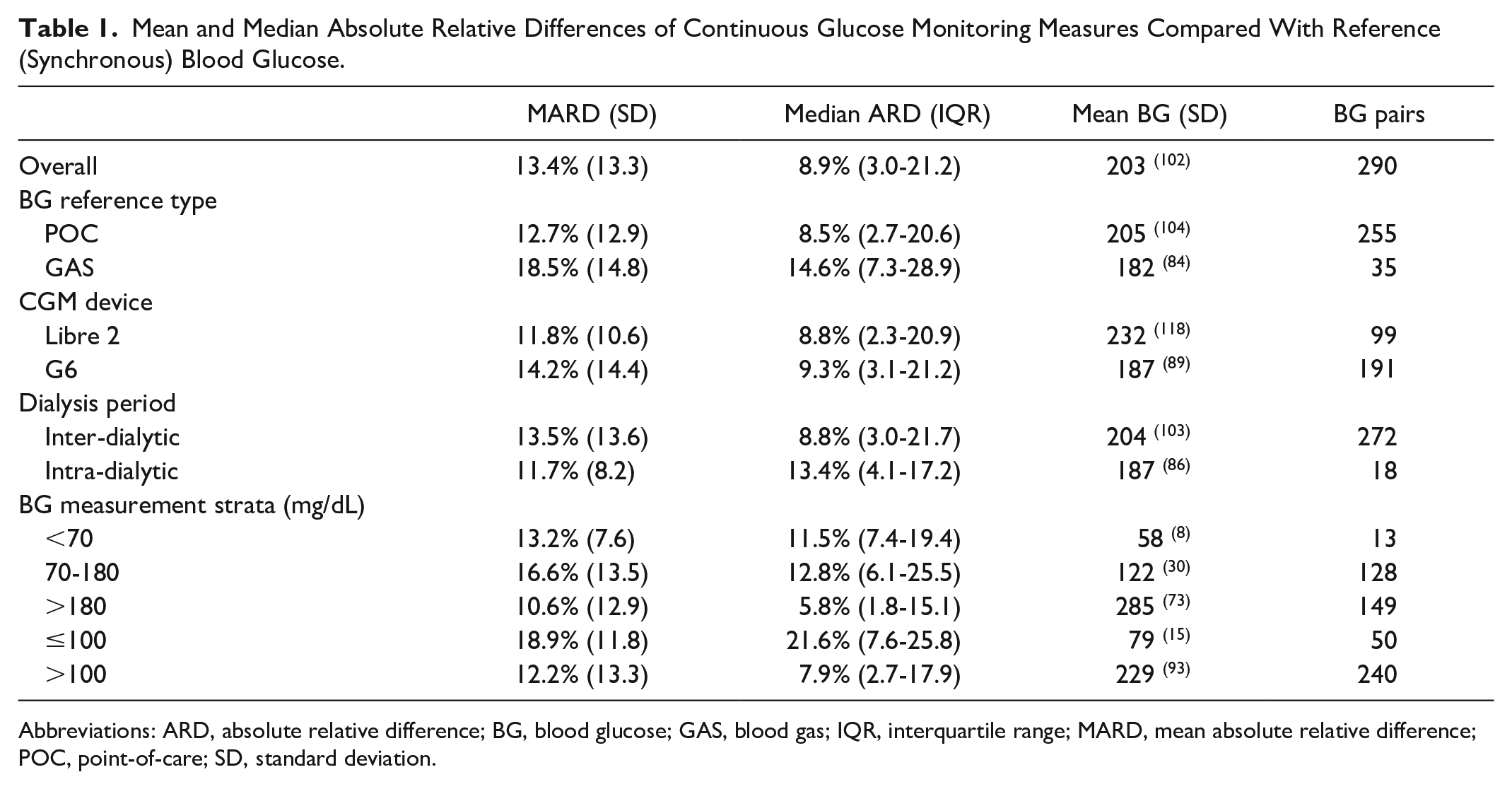
Overall population mean (SD) and median (IQR) absolute relative difference (ARD) were 13.4% (13.3) and 8.9% (3.0–21.2), respectively (Table 1). Amongst 255 CGM-POC pairs, mean (SD) and median (IQR) ARD were 12.7% (12.9) and 8.5% (2.7-20.6). GAS measures were likely performed when patients were more unwell; amongst 35 CGM-GAS pairs, mean (SD) and median (IQR) ARD were 18.5% (14.8) and 14.6% (7.3–28.9). Overall %15/15, %20/20, and %30/30 agreement rates were 67%, 76%, and 90%, respectively. In consensus error grid (CEG) analysis, 99.3% of pooled glucose pairs were in zones A/B (99.2% CGM-POC pairs; 100% CGM-GAS pairs). In Bland-Altman analysis, bias (95% CI) was +7.8mg/dL (+2.6, +13.0) for G6 and -18.1mg/dL (-23.1, -13.2) for Libre2, compared with pooled reference BG.
Mean and Median Absolute Relative Differences of Continuous Glucose Monitoring Measures Compared With Reference (Synchronous) Blood Glucose.
Abbreviations: ARD, absolute relative difference; BG, blood glucose; GAS, blood gas; IQR, interquartile range; MARD, mean absolute relative difference; POC, point-of-care; SD, standard deviation.
Previous studies of CGM accuracy in HD assessed stable outpatients, predominantly with type 2 diabetes, and reported mean absolute relative difference (MARD) 11.3% to 22.7%.3-5 Our study is unique in its evaluation of acutely unwell inpatients with T1D, who experience greater glucose variability. Our accuracy results of in-hospital Libre2 and G6 use have potential implications for future automated insulin delivery use in this high-risk population. 6
The limitations of this study include small sample sizes, few plasma glucose measures, and limited intradialytic period assessments.
Amongst adults with T1D receiving chronic HD admitted to hospital for acute illness, real-world inpatient use of CGM exhibits satisfactory accuracy. Future studies using real-time CGM in the management of inpatients with T1D requiring HD are warranted.
Footnotes
Acknowledgements
The authors thank each hospital’s diabetes educators for their efforts linking patient CGM devices with hospital CGM software accounts, as well as the Business Intelligence team at The Royal Melbourne Hospital, the Data Analytics and Insights service at Eastern health, and the Data Analytics and Reporting team at Peninsula Health for their support.
Abbreviations
ARD, absolute relative difference; BG, blood glucose; CEG, Consensus error grid; CGM, Continuous glucose monitoring; GAS, blood gas; HbA1c, hemoglobin A1c; HD, hemodialysis; IQR, interquartile range; POC, point-of-care; SD, standard deviation; T1D, type 1 diabetes.
Author Contributions
RW, MK, and SF were involved in conception and design of the study. MK, AC, CC, and SF supported methodological decisions. RW, and BK performed the data acquisition. RW performed the statistical analysis and wrote the first draft of the manuscript. MK, KD, and SF provided critical revisions to the manuscript. All authors made a significant contribution to finalizing the manuscript and approved the final version of the manuscript. SF provided overall study supervision and is the guarantor of this work and, as such, had full access to all the data in the study and takes responsibility for the integrity of the data and the accuracy of the data analysis.
Authors’ Note
Parts of this study were presented in abstract form at the 60th Annual Meeting of the European Association for the Study of Diabetes, Madrid, Spain, 10-13 September 2024.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: S.F. contributes to the advisory panel for Viatris Inc. and Pfizer Inc.; has received honoraria for speaker fees for AstraZeneca, Boehringer-Ingelheim, Lilly, Novo Nordisk; and received honoraria for advisory fees for Medtronic, Mylan, Pfizer, and Sanofi. M.K. has received honoraria for speaker fees for AstraZeneca.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: R.W. is the recipient of an Australian Commonwealth Government RTP Scholarship, ACADI PhD Grant, Fred Knight Research Scholarship, Rowden White Scholarship, and Gordon P Castles Scholarship.