
Abstract
While automated insulin delivery (AID) systems have multiple well-established benefits outside of pregnancy and are widely used in non-pregnant individuals with type 1 diabetes (T1D), none of the commercially available AID systems in North America are approved for use during pregnancy. Use of commercially available AID systems off-label in pregnancy is currently limited by: (1) glucose targets higher than the fasting glucose target range recommended during pregnancy and (2) algorithms which were not designed for the dynamic changes in insulin resistance which occur across gestation. However, as AID use in the general population expands, many individuals will opt to continue using these systems off-label during pregnancy, and thus, guidance for providers regarding AID use and optimization during pregnancy is of the utmost importance. A cornerstone to the effective use of AID systems is the systematic and accurate interpretation of continuous glucose monitoring (CGM) data. One obstacle to the use of both CGM and AID systems by obstetric providers is the lack of comfort with CGM interpretation. We therefore present here: (1) a systematic approach to CGM interpretation during pregnancy and (2) practical guidance regarding AID use during pregnancy for individuals who opt to use commercially available AID systems off-label during pregnancy after consideration of individualized risks and benefits.
Keywords
Introduction
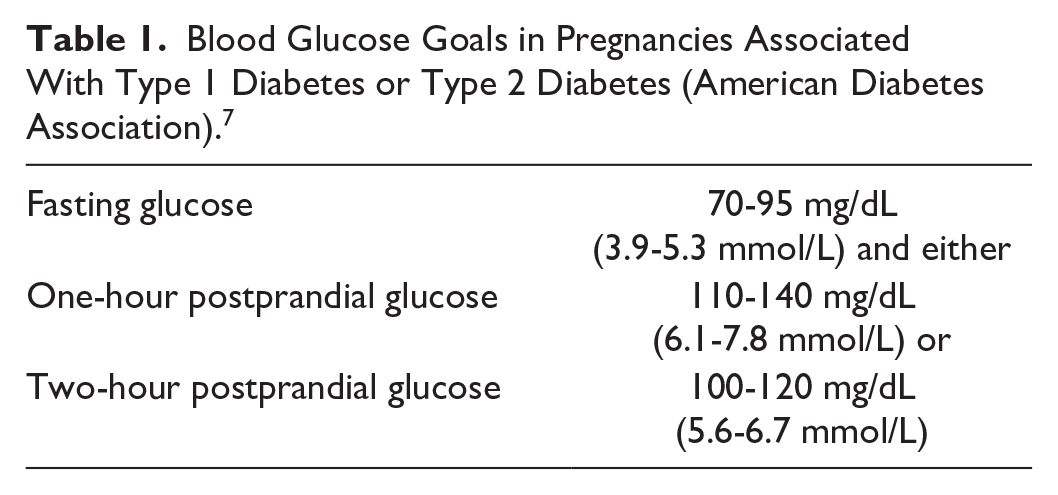
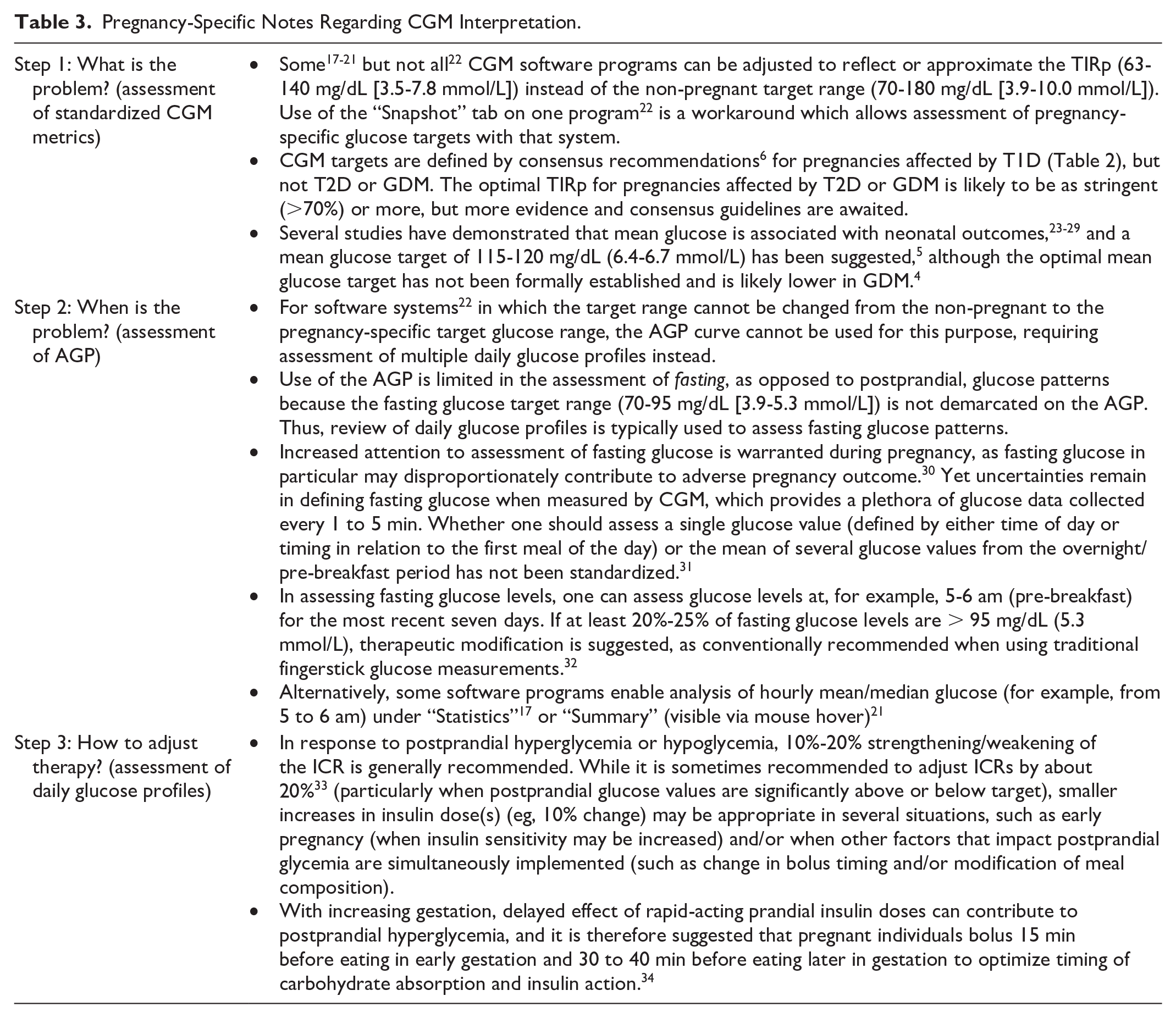
Achieving glycemic targets during pregnancy affected by diabetes is of the utmost importance, as sustained hyperglycemia during pregnancy is associated with increased risk of multiple adverse pregnancy and neonatal outcomes. 1 Fortunately, achieving optimal glycemia during pregnancy significantly decreases these risks, and lower glycemic targets are recommended during pregnancy (Table 1). The seminal CONCEPTT trial notably demonstrated significant improvements in neonatal outcomes with continuous glucose monitoring (CGM) use among pregnant women with type 1 diabetes (T1D). However, glycemic targets remain difficult to attain2-4 and are often not achieved until late in gestation. 5 Pregnancy-specific targets for percentages of time in the different CGM-derived glycemic ranges are shown in Table 2. Greater than 70% Time in Range (TIR) is similarly recommended for non-pregnant and pregnant individuals, but the target glucose range is lower during pregnancy (63-140 mg/dL [3.5-7.8 mmol/L] vs 70-180 mg/dL [3.9-10.0 mmol/L]). Note that standardized CGM metrics are established for pregnant individuals with T1D but not for individuals with gestational diabetes (GDM) or type 2 diabetes (T2D) due to insufficient data.6,7 The optimal TIR for pregnancies affected by T2D or GDM is likely to be as stringent (>70%) or more, but more evidence and consensus guidelines are awaited.
Blood Glucose Goals in Pregnancies Associated With Type 1 Diabetes or Type 2 Diabetes (American Diabetes Association). 7
CGM Targets for Pregnant Individuals with T1D. 6
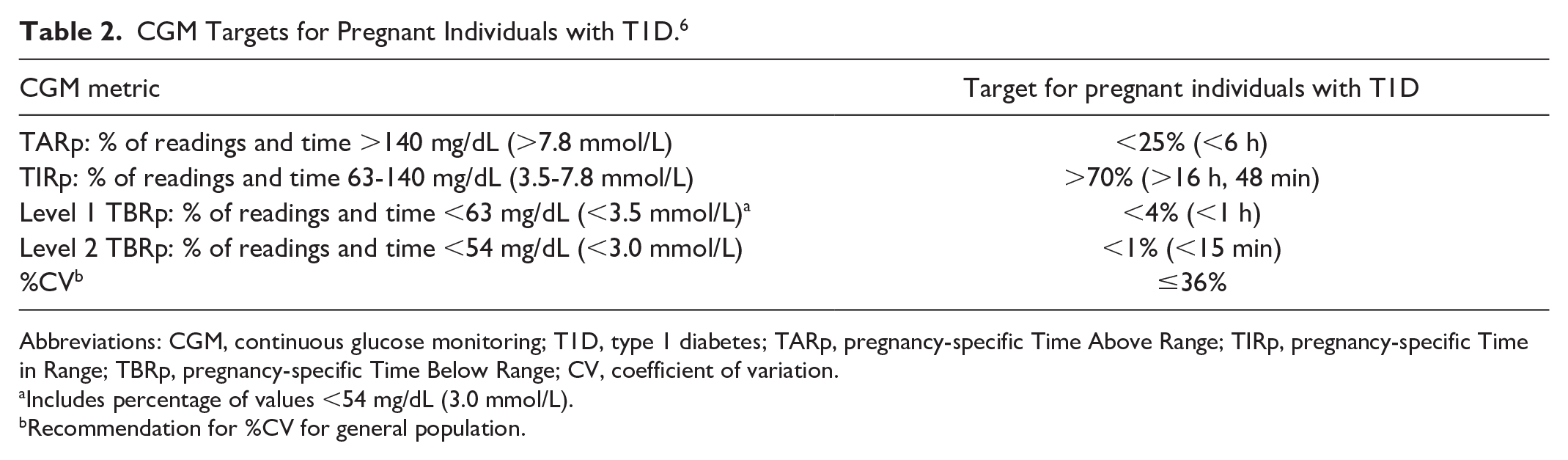
Abbreviations: CGM, continuous glucose monitoring; T1D, type 1 diabetes; TARp, pregnancy-specific Time Above Range; TIRp, pregnancy-specific Time in Range; TBRp, pregnancy-specific Time Below Range; CV, coefficient of variation.
Includes percentage of values <54 mg/dL (3.0 mmol/L).
Recommendation for %CV for general population.
Automated insulin delivery (AID) systems are considered the preferred therapy in non-pregnant adults with T1D and other forms of insulin-deficient diabetes, and they also confer glycemic benefits to non-pregnant adults with type 2 diabetes (T2D). 8 AID systems are designed to keep glucose levels at a specified target. Glucose data obtained via CGM feed into the AID algorithm, which then adjusts the basal insulin levels (sometimes augmented by automated bolus doses) to achieve the pre-determined glucose target within an allotted time. All current AID systems are “hybrid closed-loop” systems, as they still rely upon the user to estimate and input carbohydrates ingested into the algorithm or to announce meals. The algorithm will then advise the user of a suggested bolus dose—a prandial bolus per the insulin:carbohydrate ratio (ICR) before carbohydrate intake, and a correction bolus if hyperglycemia is present according to the insulin sensitivity factor (SF), glucose target, and active insulin.
In contrast to the well-established benefits of AID use outside of pregnancy, at the time of writing, none of the commercially available AID systems available in North America are approved for use during pregnancy. It is important to note that none of these AID systems were designed for use during pregnancy, none have sufficiently low glucose targets to allow glucose levels to reach the lower fasting glucose goals recommended during pregnancy, and none have algorithms intended to respond to the progressive changes in insulin resistance that occur during pregnancy.8,9 Studies evaluating off-label use of commercially available AID systems have variably reported improvement in some but not all CGM metrics, and none to date have demonstrated improved pregnancy-specific TIR (TIRp).10,11 The results of the CIRCUIT trial, evaluating the Tandem Control-IQ system in pregnancy, are eagerly awaited. 12 The only commercially available AID system with the capability to set glucose targets within the pregnancy-specific fasting glucose range (CamAPS FX) did improve TIRp 13 and is approved for use in pregnancy in Europe and Australia, but it is not yet available in North America, and the glycemic benefits demonstrated with this system cannot be extrapolated to those which lack pregnancy-specific glucose targets. A pilot study in the United States of an investigational AID algorithm customized for pregnancy showed impressive improvements in most glycemic parameters; 14 however, this system is not yet commercially available and has yet to be tested in a proper randomized trial.
Nevertheless, many individuals will already be using commercially available AID systems when they become pregnant and will want to continue AID use (off-label) during pregnancy based on informed individualized decision-making.
Selective off-label AID use during pregnancy can lead to improved overall glycemia in some individuals in cases when glycemic targets are not achieved by conventional therapy (at the expense of fasting glucose above the pregnancy-specific fasting glucose target range). Current guidance advises that “AID systems without pregnancy-specific glucose targets or a pregnancy-specific algorithm may be considered for select pregnant individuals with T1D when used with assistive techniques and working with experienced health care teams,” 7 and advises that “[i]nitiating or continuing AID systems during pregnancy needs to be assessed carefully.” 8 It is imperative that providers counsel all pregnant individuals considering off-label AID use that it is currently unknown if glycemic benefits are offset by the inability to achieve pregnancy-specific fasting glucose targets and that the impact of off-label AID use on pregnancy outcomes is not well understood at this time. Factors to be considered in determining whether or not to use commercially available AID systems off-label during pregnancy have been described elsewhere.7,8,15
A cornerstone of effective AID use is CGM interpretation. With the increasing adoption of these technologies and obstacles to specialist access, obstetric providers are increasingly being called upon to interpret CGM data and manage AID use. Accordingly, we present here: (1) a stepwise and systematic approach to CGM interpretation during pregnancy and (2) practical guidance aimed at obstetric providers intended to assist in customizing AID systems as much as possible to optimize glycemia for individuals who opt to use commercially available AID systems off-label during pregnancy based on consideration of individualized risks and benefits.
Stepwise Approach to Continuous Glucose Monitoring Interpretation for the Obstetric Provider
A systematic approach to CGM interpretation is central to the identification of the clinically relevant glycemic patterns that warrant therapeutic modification. The below approach is modified for use in pregnancy from an approach previously published 16 for use outside of pregnancy.
Before Starting: Assessment of Data Sufficiency
First, one must assess if adequate data are available in the selected analysis period to inform meaningful assessment. By convention, the percentage of time CGM is active must be at least 70% of data from 14 days. 6 In pregnancy, we also consider the most recent seven days, given the rapid fluctuations in glycemia during pregnancy.
Step 1: What is the Problem?
The first step is to determine whether there is excessive (1) hyperglycemia, (2) hypoglycemia, or (3) both by assessing standardized CGM metrics (Table 2) for the specified analysis period. TIRp <70% indicates insufficient time in the target range, which could be due to excessive hyperglycemia, hypoglycemia, or both. If pregnancy-specific Time Above Range (TARp) is >25%, there is too much hyperglycemia, and if pregnancy-specific Time Below Range (TBRp) is >4% (or if time below 54 mg/dL [3 mmol/L] is >1%), there is too much hypoglycemia. Table 3 shows pregnancy-specific considerations.
Pregnancy-Specific Notes Regarding CGM Interpretation.
Step 2: When is the Problem?
Once one has determined what the problem is (too much hyperglycemia, hypoglycemia, or both) in Step 1, the next step is to determine when (at what time(s) of day) is the problem occurring. The ambulatory glucose profile (AGP) 35 visually displays combined glucose profiles from the selected analysis period over the 24-hour day (Figure 1). The dark-shaded band (interquartile range [IQR]) represents 50% of the glucose values and thus reflects the most common glucose patterns (Figure 1b, blue arrows). The light-shaded bands above and below the dark band represent the more extreme glucose patterns (Figure 1b, yellow arrows); for example, 5% of glucose values fall above the 95th percentile (top) line, and 5% of glucose values fall below the 5th percentile (bottom) line. In order to identify hypoglycemia patterns, find times of day when the light-shaded band (extreme percentile curve) crosses below the lower limit of the target range (Figure 2). Since goal TBRp is <4%, therapeutic adjustments are warranted even when a small percentage of glucose values cross below the target range. In contrast, in identifying postprandial hyperglycemia patterns, find times of day when the dark-shaded band (most common glucose patterns, instead of extreme percentile curves) crosses above the upper end of the target range (Figure 2). In general, therapeutic modification is not warranted when only the more extreme curves cross above the target range, as they may represent atypical deviations from the norm, and the general goal is to achieve TARp <25%. Use of the integrated AGP view enables one to efficiently distill common postprandial hyperglycemia patterns from the often overwhelming amount of CGM data generated, but it is less helpful for assessment of fasting glucose patterns (see Table 3 for pregnancy-specific considerations).
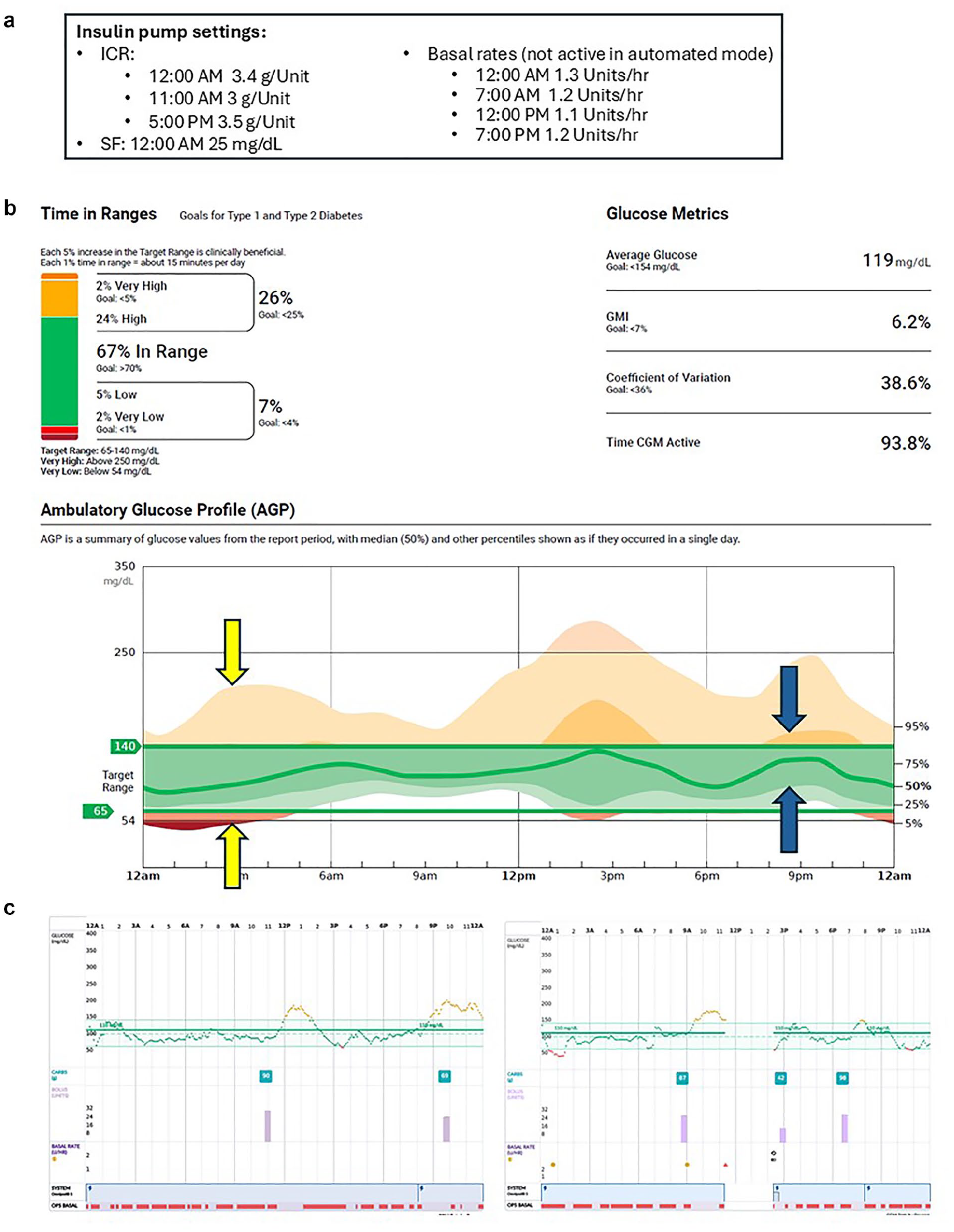
Case example of a 27-year-old woman with T1D at 32 weeks gestation using AID. (a) Insulin pump settings. Note that basal rates are not active when in automated mode for this AID system. (b) Standardized CGM metrics and AGP. The middle (green bolded) line represents the median glucose. The interquartile range (IQR; 25th-75th percentiles) is represented by the dark-shaded ribbon surrounding the median line and is indicated by the blue arrows. The light-shaded outer ribbons (bounded by the 95th and 5th percentiles) are indicated by the yellow arrows. To convert mg/dL to mmol/L, divide by 18. (c) Example of daily glucose profile is displayed. Pregnancy-specific glucose target range defined as 65 to 140 mg/dL (the lower limit of the target range is set to 65 mg/dL instead of 63 mg/dL when 5 mg/dL is the minimum increment available on the software program).
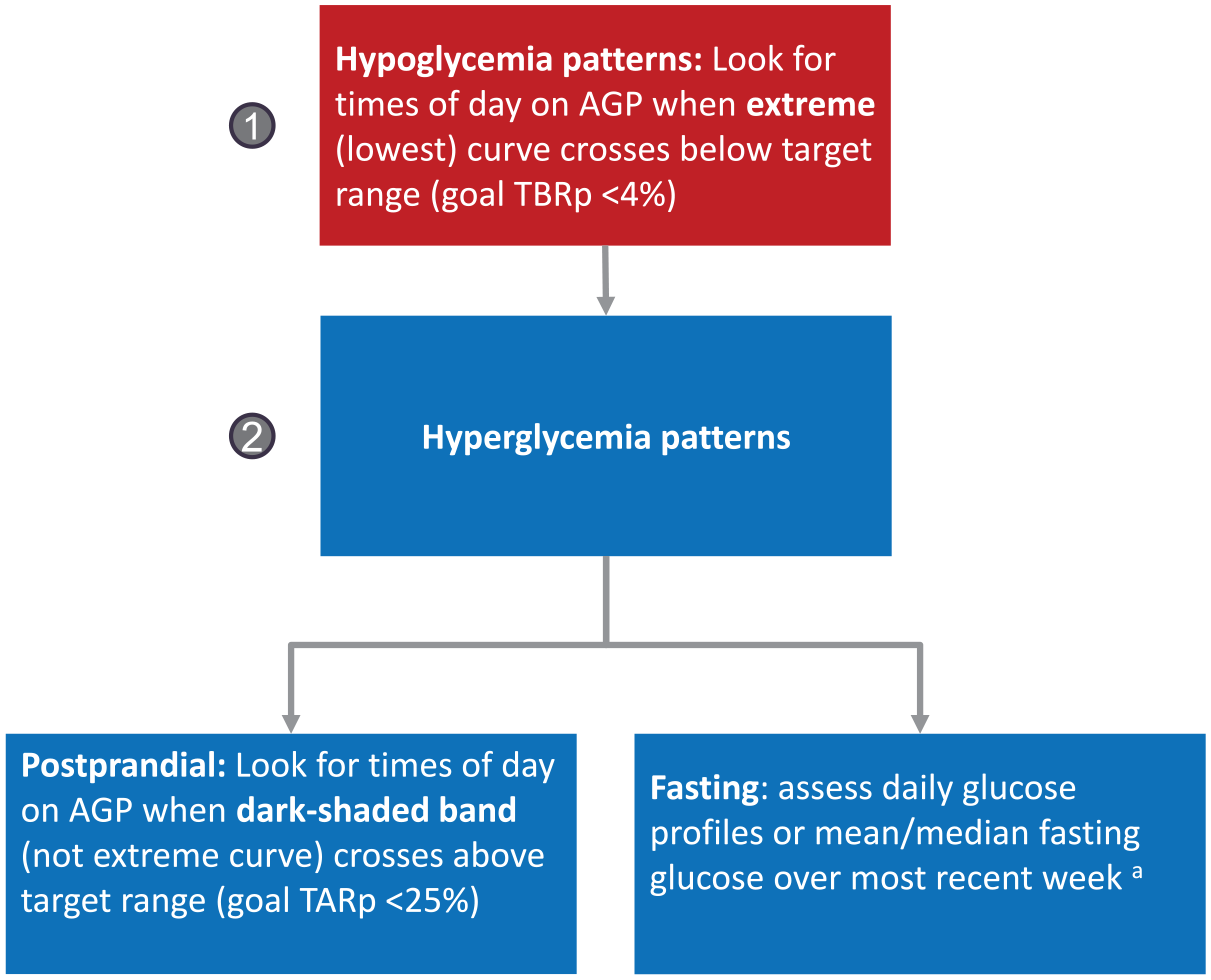
Approach to assessment of hypoglycemia and hyperglycemia patterns with continuous glucose monitoring.
Step 3: How to Adjust Therapy?
Review of the daily glucose profiles provides detailed information about glucose trends over the day, meal patterns, and timing of insulin administration, and thus informs decisions regarding specific therapeutic adjustments. A key principle is that hypoglycemia must be addressed first (Figures 2 and 3) because (1) even infrequent severe hypoglycemia can carry risk for the mother and (2) “hypoglycemia begets hyperglycemia” due to reflexive counter-regulatory responses and the need for ingestion of uncovered carbohydrate to mitigate hypoglycemia.

Therapeutic modifications based on CGM patterns.
Next, hyperglycemia trends must be assessed. When postprandial hyperglycemia is present, consider treatment strategies shown in Figure 3. In determining treatment of fasting hyperglycemia, one must evaluate the overnight trend in glucose. If fasting hyperglycemia follows an episode of nocturnal hypoglycemia (sometimes called the “Somogyi effect,”37,38 or “rebound hyperglycemia”), then basal and/or rapid-acting insulin dose(s) must be decreased where appropriate (as above, always address hypoglycemia first). Even in the absence of overt hypoglycemia, if glucose decreases significantly overnight 36 (Figure 3), this typically indicates that the basal insulin dose is adequate or even excessive, and fasting hyperglycemia results instead from lingering postprandial hyperglycemia on the night preceding (not from inadequate basal insulin). In this situation, evening postprandial hyperglycemia must be treated, which in turn leads to improved fasting glucose the next morning. If basal insulin were increased in this situation, overnight hypoglycemia could occur on days when evening postprandial glucose is optimal (a large overnight glucose decrease will result in hypoglycemia when the starting point is already in the target range). On the contrary, if fasting hyperglycemia occurs in the absence of preceding evening postprandial hyperglycemia, or if fasting glucose increases overnight (including “dawn phenomenon,” when glucose increases early morning in concert with morning increases in counter-regulatory hormones),37,38 this requires an increase in basal insulin delivery at the time period(s) needed (see Table 3 for pregnancy-specific considerations, and see sections below regarding common strategies for AID system adjustments).
Basic Principles of Automated Insulin Delivery System Use and Adjustments
Commercially available AID systems vary by glucose targets available, ability to change certain settings, and additional features (Table 4). Therefore, individualized approaches are needed according to the system used. 15 Pump settings must be repeatedly reassessed and adjusted as insulin resistance and glycemic patterns change progressively across gestation.
AID Systems and their Features.
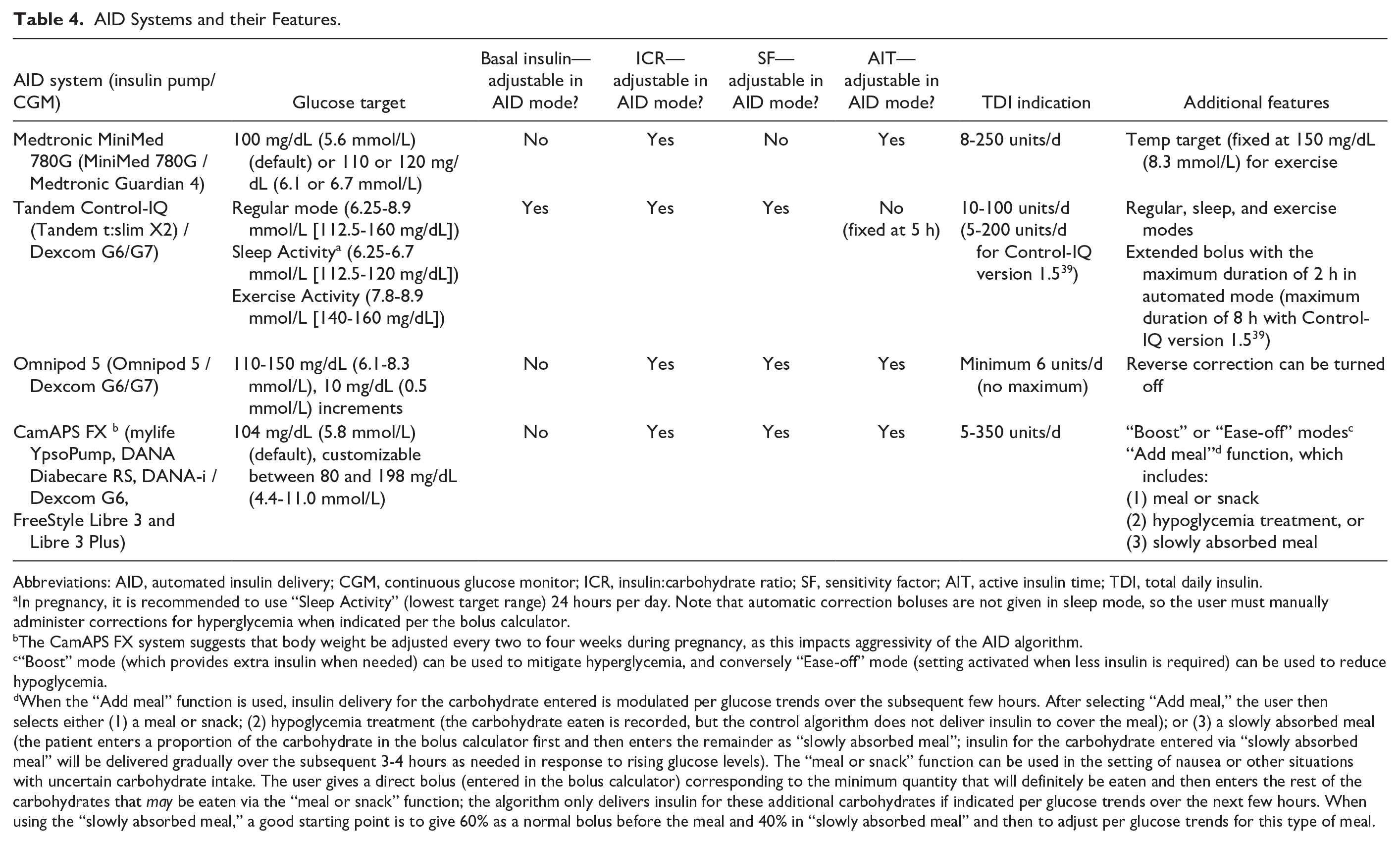
Abbreviations: AID, automated insulin delivery; CGM, continuous glucose monitor; ICR, insulin:carbohydrate ratio; SF, sensitivity factor; AIT, active insulin time; TDI, total daily insulin.
In pregnancy, it is recommended to use “Sleep Activity” (lowest target range) 24 hours per day. Note that automatic correction boluses are not given in sleep mode, so the user must manually administer corrections for hyperglycemia when indicated per the bolus calculator.
The CamAPS FX system suggests that body weight be adjusted every two to four weeks during pregnancy, as this impacts aggressivity of the AID algorithm.
“Boost” mode (which provides extra insulin when needed) can be used to mitigate hyperglycemia, and conversely “Ease-off” mode (setting activated when less insulin is required) can be used to reduce hypoglycemia.
When the “Add meal” function is used, insulin delivery for the carbohydrate entered is modulated per glucose trends over the subsequent few hours. After selecting “Add meal,” the user then selects either (1) a meal or snack; (2) hypoglycemia treatment (the carbohydrate eaten is recorded, but the control algorithm does not deliver insulin to cover the meal); or (3) a slowly absorbed meal (the patient enters a proportion of the carbohydrate in the bolus calculator first and then enters the remainder as “slowly absorbed meal”; insulin for the carbohydrate entered via “slowly absorbed meal” will be delivered gradually over the subsequent 3-4 hours as needed in response to rising glucose levels). The “meal or snack” function can be used in the setting of nausea or other situations with uncertain carbohydrate intake. The user gives a direct bolus (entered in the bolus calculator) corresponding to the minimum quantity that will definitely be eaten and then enters the rest of the carbohydrates that may be eaten via the “meal or snack” function; the algorithm only delivers insulin for these additional carbohydrates if indicated per glucose trends over the next few hours. When using the “slowly absorbed meal,” a good starting point is to give 60% as a normal bolus before the meal and 40% in “slowly absorbed meal” and then to adjust per glucose trends for this type of meal.
Glucose Targets
The lowest glucose target/range available for each system is chosen in pregnancy. For Medtronic 780G and Omnipod 5 (OP5), 100 mg/dL (5.6 mmol/L) and 110 mg/dL (6.1 mmol/L) are chosen, respectively. For Tandem Control-IQ, it is suggested to use sleep mode 24 hours per day, 40 which allows one to use the lowest glucose target range available on this system at all times (112.5-120 mg/dL [6.3-6.7 mmol/L] compared to the standard Control-IQ target range of 112.5-160 mg/dL [6.3-8.9 mmol/L]). For CamAPS FX, 100 mg/dL (5.5 mmol/L) in the first trimester is suggested, while 81 mg/dL (4.5 mmol/L) overnight and 90 mg/dL (5.0 mmol/L) during daytime is suggested in the second and third trimesters. In all systems, an individualized approach must be taken, considering each patient’s preferences, glucose trends, and risk of hypoglycemia.
Basal Insulin Delivery
Tandem Control-IQ is the only system in which manually inputted basal insulin rates are utilized in the AID algorithm. Thus, it is important to change these rates frequently in pregnancy, as one would do for non-automated pump settings. In general, the total programmed basal insulin should be higher (eg, 20%-25%) than the total basal insulin that is being delivered for optimal results during pregnancy. 40 Note that Control-IQ technology will decrease/temporarily suspend basal insulin if the 30-minute predicted glucose is below 112.5 mg/dL (6.3 mmol/L) or 70 mg/dL (3.9 mmol/L), respectively. Thus, there is limited yield to large basal rate increases since basal insulin suspension can lead to rebound hyperglycemia and is thus counterproductive.
The other systems (Medtronic, OP5, CamAPS FX) do not utilize the programmed basal insulin settings for automation, and changing basal rates in these systems has no impact in automated mode. However, manual mode basal rates need to be updated regularly across gestation to ensure that they approximate the average amount of basal insulin delivered in automated mode, in the event that automated mode cannot be utilized (eg, sensor failure).
Individuals may also choose to toggle between manual mode overnight (with adjustment of basal rates to achieve pregnancy-specific fasting glucose targets) and automated mode during the day (which can mitigate glucose variability, postprandial glucose excursions, and hypoglycemia). 15 Some systems (Medtronic) have partial closed-loop modes, which temporarily suspend basal insulin delivery when hypoglycemia occurs or is predicted, and this can be utilized in lieu of full manual mode overnight.
Prandial Boluses
ICR: ICR is the number of grams of carbohydrate that 1 unit of rapid-acting insulin will cover. A lower number indicates a stronger ICR (for a 50-gram meal, 10 units are taken if ICR is 1:5, while only 5 units are taken if ICR is 1:10). During pregnancy, insulin sensitivity increases early in pregnancy, but insulin resistance rises dramatically after 20 weeks’ gestation. Thus, weakening of the ICR may be needed early in pregnancy, while serial strengthening of the ICR is typically needed in the second and third trimesters. In general, 10%-20% strengthening/weakening of the ICR is recommended in response to postprandial glycemic trends (Table 3).
Timing of prandial bolus: Although commonly used prandial insulins are called “rapid-acting” insulins, their absorption is often slower than that of the carbohydrates ingested. This phenomenon is exaggerated in pregnancy, where absorption of insulin takes longer with increasing gestation. 34 It is very important to match the timing of carbohydrate absorption with insulin action. If mismatched, carbohydrates are absorbed more quickly while insulin takes effect later, causing initial postprandial hyperglycemia, followed by subsequent hypoglycemia. In AID users, this late postprandial hypoglycemia can be potentiated if an automated basal insulin increase (that was triggered by recent postprandial hyperglycemia) overlaps with the delayed prandial bolus peak. One way to optimize matching of carbohydrate absorption with insulin action is to pre-bolus before eating, so the insulin action aligns optimally with carbohydrate absorption. Accordingly, it is suggested that pregnant individuals bolus 15 minutes before eating in early gestation, increasing to 30-40 minutes before eating in late pregnancy. 34 This may be most needed at breakfast, a time when insulin resistance and resulting postprandial hyperglycemia are often the greatest. 33 If the optimal pre-bolus timing is not known, one can bolus and watch for glucose levels to start to decrease (even just 0.1 mmol/L or 2 mg/dL) on CGM before eating (A. Dunlop, personal communication, October 25, 2023). If the pattern of early postprandial spike followed by late postprandial hypoglycemia persists, one can progressively increase the pre-bolus time and/or strengthen the ICR, and (for systems that allow basal rate adjustment) lower the basal rates in the postprandial period. If late postprandial hypoglycemia continues once pre-bolusing improves postprandial glycemia, the ICR can then be weakened.
Sensitivity Factor
SF setting: The SF is how much one unit of rapid-acting insulin is expected to lower blood glucose. If the SF is decreased, the correction dose administered becomes stronger; conversely, if the SF is increased, the correction dose administered becomes weaker. For example, if glucose is 50 mg/dL (2.8 mmol/L) higher than the glucose target, a 1-unit correction dose will be administered by a person using a SF of 1:50 mg/dL (1:2.8 mmol/L) and a 2-unit correction dose will be administered by a person using a SF of 1:25 mg/dL (1:1.4 mmol/L). Thus, the SF influences the strength of a correction bolus dose and should be assessed at each visit. The SF can also indirectly influence basal modulation, because a stronger SF will lead to larger correction doses and thus increased TDI, a major determinant of the aggressivity of basal modulation. Throughout pregnancy, one can assess the appropriateness of the SF (when adjustable) using the calculation of 1700/TDI (90/TDI for mmol/L) as a reference point to assess for consistency with the patient’s TDI. 40 If target glucose is either not reached or exceeded 3 to 4 hours later, the SF should be strengthened or weakened, respectively.
When SF cannot be adjusted: In pregnancy, correction boluses are encouraged to treat hyperglycemia. For the Medtronic system (SF cannot be adjusted), entering small amounts of “phantom carbs” (carbohydrates that are not actually consumed) has been suggested in those instances where the system does not allow for a correction bolus. 11 If used, start with small amounts (eg, 5 g) and increase as needed.
Active Insulin Time
AIT is an estimate of how many hours an insulin bolus is active and is used by the system to weaken correction boluses given shortly after another to reduce insulin “stacking.” Generally speaking, setting a shorter AIT allows administration of larger correction boluses when given in close proximity. In Tandem Control-IQ, AIT is fixed at 5 hours in automated mode, whereas it can be adjusted in the other systems (Table 4).
For those meals that are higher in protein and/or fat content, adjustments should be made to insulin distribution on a meal-to-meal basis. In those systems that offer an extended bolus in automated mode (Tandem Control-IQ), this should be used. Otherwise, a portion of the bolus can be given upfront, while the remainder can be given approximately 1 to 2 hours later. In the CamAPS FX system, the “slowly absorbed meal” function is used (Table 4).
Intrapartum and Postpartum Considerations
Labor and Delivery
Tight intrapartum glycemic control is associated with lower rates of neonatal hypoglycemia, 41 and glucose targets during labor and delivery vary by professional society, with the majority ranging between 70 and 126 mg/dL (3.9-7.0 mmol/L).1,42,43 Intrapartum continuous subcutaneous insulin infusion (CSII) via insulin pump is now considered an alternative to intravenous insulin delivery. CSII achieved lower glucose levels during delivery than those switched to intravenous insulin infusion 44 and enhances autonomy in diabetes self-management. The option to continue CSII use for labor and delivery is therefore offered to pregnant individuals via shared decision-making in advance of delivery (Table 5). Limited data on the use of AID systems during labor were positive.40,45 Certain clinical factors may preclude AID use in labor such as critical illness, altered level of consciousness, lack of pump supplies, and lack of health care providers facile in AID management. In these cases, intravenous insulin delivery is recommended with infusion rates based on institutional guidelines for intravenous insulin infusion with pregnancy-specific targets.
Suggested Patient Instructions for Continuing AID Systems During Labor and Delivery.
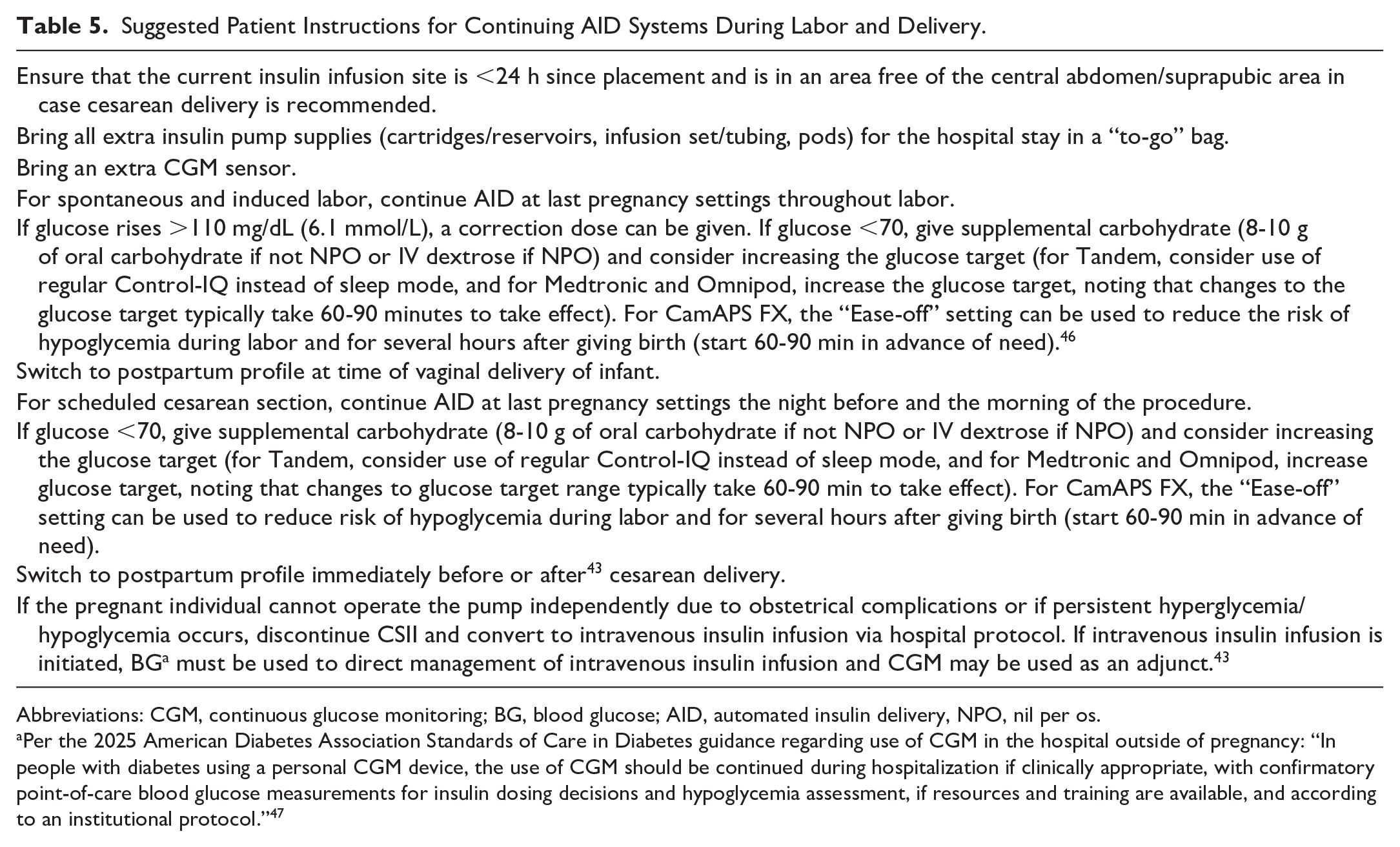
Abbreviations: CGM, continuous glucose monitoring; BG, blood glucose; AID, automated insulin delivery, NPO, nil per os.
Per the 2025 American Diabetes Association Standards of Care in Diabetes guidance regarding use of CGM in the hospital outside of pregnancy: “In people with diabetes using a personal CGM device, the use of CGM should be continued during hospitalization if clinically appropriate, with confirmatory point-of-care blood glucose measurements for insulin dosing decisions and hypoglycemia assessment, if resources and training are available, and according to an institutional protocol.” 47
Postpartum
The postpartum period can be challenging, due to newborn care needs, erratic sleep-wake cycles, sleep deprivation, and decreased time and energy available for diabetes self-care. Insulin requirements decrease markedly once the placenta is delivered, typically to levels lower than prepregnancy, 48 with a return to prepregnancy insulin requirements in the weeks following delivery. 7 Insulin pump settings must be adjusted accordingly per glucose trends. For those who provide breastmilk for their infants, increased insulin sensitivity and caloric expenditure contribute to increased hypoglycemia risk. AID use among individuals with T1D decreased hypoglycemia in the postpartum period. 49
There are limited data on AID use during the postpartum period, with most guidance emanating from small studies, expert opinion, and guidance from AID system manufacturers. Postpartum management using AID systems should be tailored to the specific needs of the postpartum individual using shared decision-making. Postpartum profiles should be created and reviewed by the clinician with the pregnant individual in the third trimester. Suggested postpartum practices for individuals using commercially available AID systems off-label during pregnancy are outlined in Table 6.
Suggested Postpartum Practices for Pregnant Individuals Using Commercially Available AID Systems Off-Label.
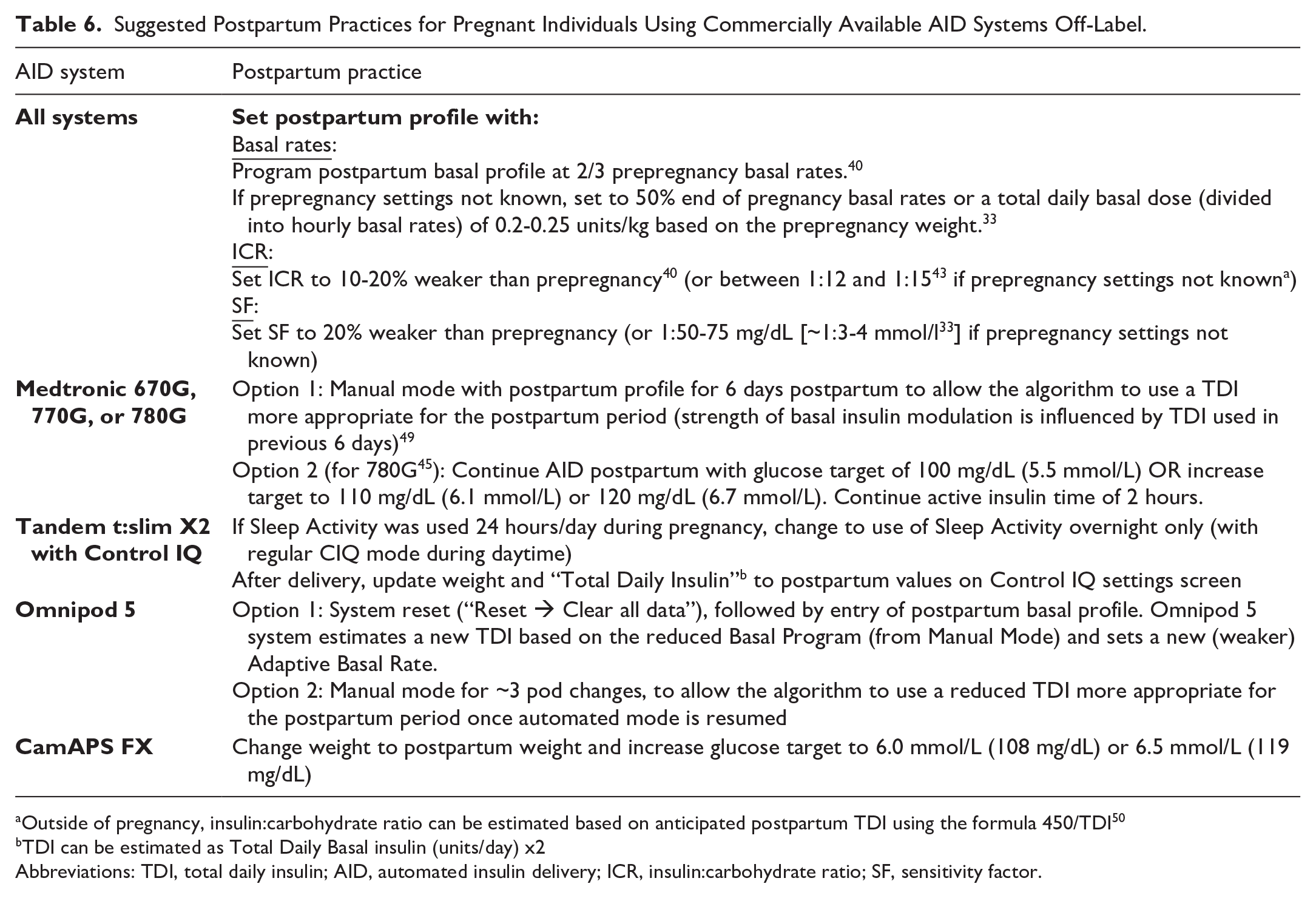
Outside of pregnancy, insulin:carbohydrate ratio can be estimated based on anticipated postpartum TDI using the formula 450/TDI 50
TDI can be estimated as Total Daily Basal insulin (units/day) x2
Abbreviations: TDI, total daily insulin; AID, automated insulin delivery; ICR, insulin:carbohydrate ratio; SF, sensitivity factor.
Postpartum, the TIR target should be adjusted to the non-pregnant glucose target range of 70 to 180 mg/dL (3.9-10 mmol/L). It is prudent to review glucoses at three to seven day intervals in the immediate postpartum period so that further adjustments can be made as needed based on glucose trends.
Breastfeeding Considerations
Both hyper- and hypoglycemia can affect breast milk production. 51 Production of breastmilk requires significant caloric expenditure of approximately 450 kcal/d. 52 Fear of hypoglycemia has been associated with breastfeeding and in some studies has been a contributing factor to cessation of breastfeeding. 53 Initial postpartum profiles, including basal rates (when adjustable), ICR, SF, and glucose targets should follow usual postpartum guidance, but they may need to be adjusted per glucose trends shortly after delivery when full breastmilk production occurs (usually day 3-4 postpartum). The use of AID systems aids in lessening the reduction in glucose levels following nighttime breastfeeding compared with sensor-augmented pumps. 54 Some individuals may experience hypoglycemia with breastfeeding and a small carbohydrate snack during breastfeeding can be eaten if needed to prevent hypoglycemia, but this may not be necessary for individuals using AID.
Case Example of Practical Application
Practical application of stepwise CGM interpretation to adjustment of AID therapy in a pregnant individual is shown in Table 7, based on the glucose data and pump settings shown in Figure 1. Implementation of the above therapeutic modifications led to improvement in TIRp (78%), with improvements in both hyperglycemia (TARp 19%) and hypoglycemia (TBRp 3%) two weeks later. Of note, increasing the pre-bolus time immediately improved postprandial hyperglycemia, which allowed subsequent weakening of the ICR.
Example of Stepwise Approach to CGM Interpretation and Adjustment of Therapeutic Regimen in Pregnant Individual with T1D Using AID
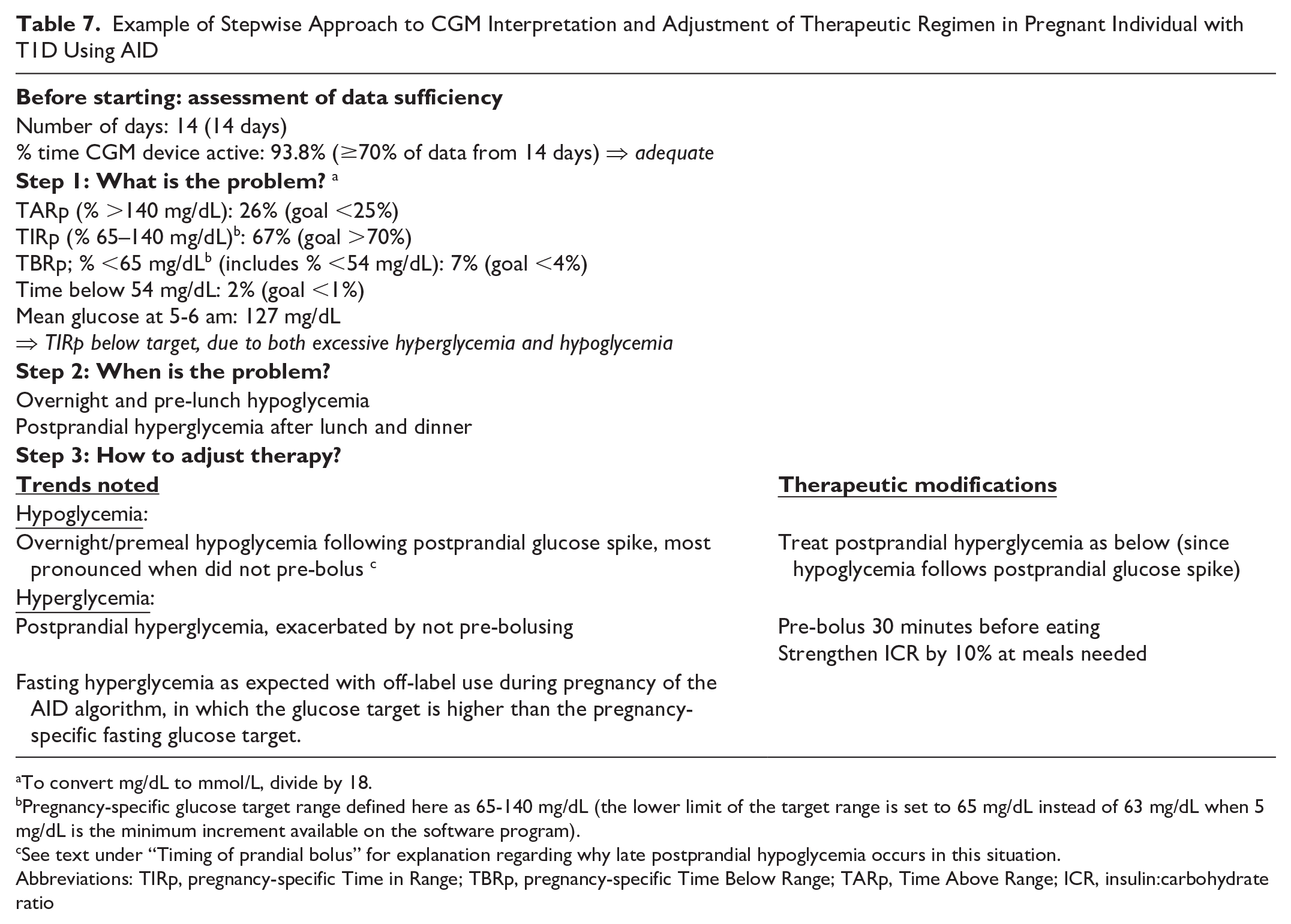
To convert mg/dL to mmol/L, divide by 18.
Pregnancy-specific glucose target range defined here as 65-140 mg/dL (the lower limit of the target range is set to 65 mg/dL instead of 63 mg/dL when 5 mg/dL is the minimum increment available on the software program).
See text under “Timing of prandial bolus” for explanation regarding why late postprandial hypoglycemia occurs in this situation.
Abbreviations: TIRp, pregnancy-specific Time in Range; TBRp, pregnancy-specific Time Below Range; TARp, Time Above Range; ICR, insulin:carbohydrate ratio
Conclusion
While AID algorithms customized for pregnancy are not currently commercially available in North America and the impact of off-label AID use on glycemic, maternal, and infant outcomes is still being elucidated, the reality in clinical practice is that many individuals will choose to use commercially available AID systems during pregnancy. Thus, familiarity among providers with best practices to optimize off-label AID use during pregnancy is essential. We present here practical guidance regarding off-label AID use in pregnancy, guided by stepwise CGM interpretation and an understanding of the unifying and distinguishing features of the different AID systems that are currently available.
Footnotes
Abbreviations
AGP, ambulatory glucose profile; AID, automated insulin delivery; AIT, active insulin time; CGM, continuous glucose monitoring; CSII, subcutaneous insulin infusion; CV, coefficient of variation; GDM, gestational diabetes; ICR, insulin: carbohydrate ratio; IQR, interquartile range; MFM, maternal fetal medicine; NPO, nil per os; SF, sensitivity factor; T1D, type 1 diabetes; TARp, Time Above Range; TBRp, pregnancy-specific Time Below Range; TDI, total daily insulin; TIRp, pregnancy-specific Time in Range.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: DSF reports grants from the Canadian Institute of Health Research and an investigator-initiated grant from Dexcom, in-kind donations from Dexcom and Tandem, and speaker honoraria from Novo-Nordisk. CD has received financial support from Dexcom for an advisory role for patient education and development of educational materials, receives royalties from UpToDate for topics on GDM, and has received funding from United Health Group and Helmsley Charitable Trust. EDS reports honoraria from the American Diabetes Association (ADA) when serving on the ADA Scientific Sessions Planning Committee 2023 and 2024.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.