
Abstract

Recent estimates show that 27% or more of hospitalized adults are living with type 1 or type 2 diabetes mellitus (DM). 1 The blood glucose (BG) target for nonacute care ward patients is: United Kingdom: 6.0 to 10.0 mmol/L 2 ; United States: 5.6 to 10.0 mmol/L 3 ; Canada: 5.0 to 10.0 mmol/L. 4 Hypoglycemia is a very uncomfortable experience for patients, 2 requires more nursing time for treatment, and is associated with longer hospital stays, and higher patient morbidity and mortality 5,6.
A frequent preventable cause of in-hospital hypoglycemia is inadequate adjustment of DM medications when there is a “looming hypoglycemia”, defined as BG 4.0 to 6.0 mmol/L. 2 An audit of four months of inpatient hypoglycemia events at our tertiary care hospital revealed an inadequate adjustment of DM medications in 64.3% of cases when there was already a BG below 5 mmol/L within the prior day.
The objective of this study was to develop and test an automatable algorithm to determine the most responsible hypoglycemic medication and recommend a decrease in its dose. This automatable algorithm could incite a new era of inpatient diabetes care technology development using artificial intelligence programming to integrate real-time hypoglycemic medication dose reductions into electronic health records. This algorithm could be written into software coding for integration into electronic health record systems in which the in-hospital patients’ medications and BG results are accessible in real-time.
Our study team developed an automatable algorithm that determines the most responsible medication for each in-hospital BG < 5.0 mmol/L event, and recommends the extent of its dose decrease. A BG < 5.0 mmol/L was chosen because it is below the desired glucose range for noncritically ill in-hospital patients.2-4 The automatable algorithm (Table 1) contains three steps: (1) define the duration of action to determine the hypoglycemic medication(s) active in the patient; (2) establish a hierarchy of hypoglycemic medication potency; (3) recommend the dose decrease for the most responsible hypoglycemic medication.
Recommendation for Dose Decrease of the Most Responsible Hypoglycemic Medication: Follow Step 1, Step 2, and This Table for Step 3.
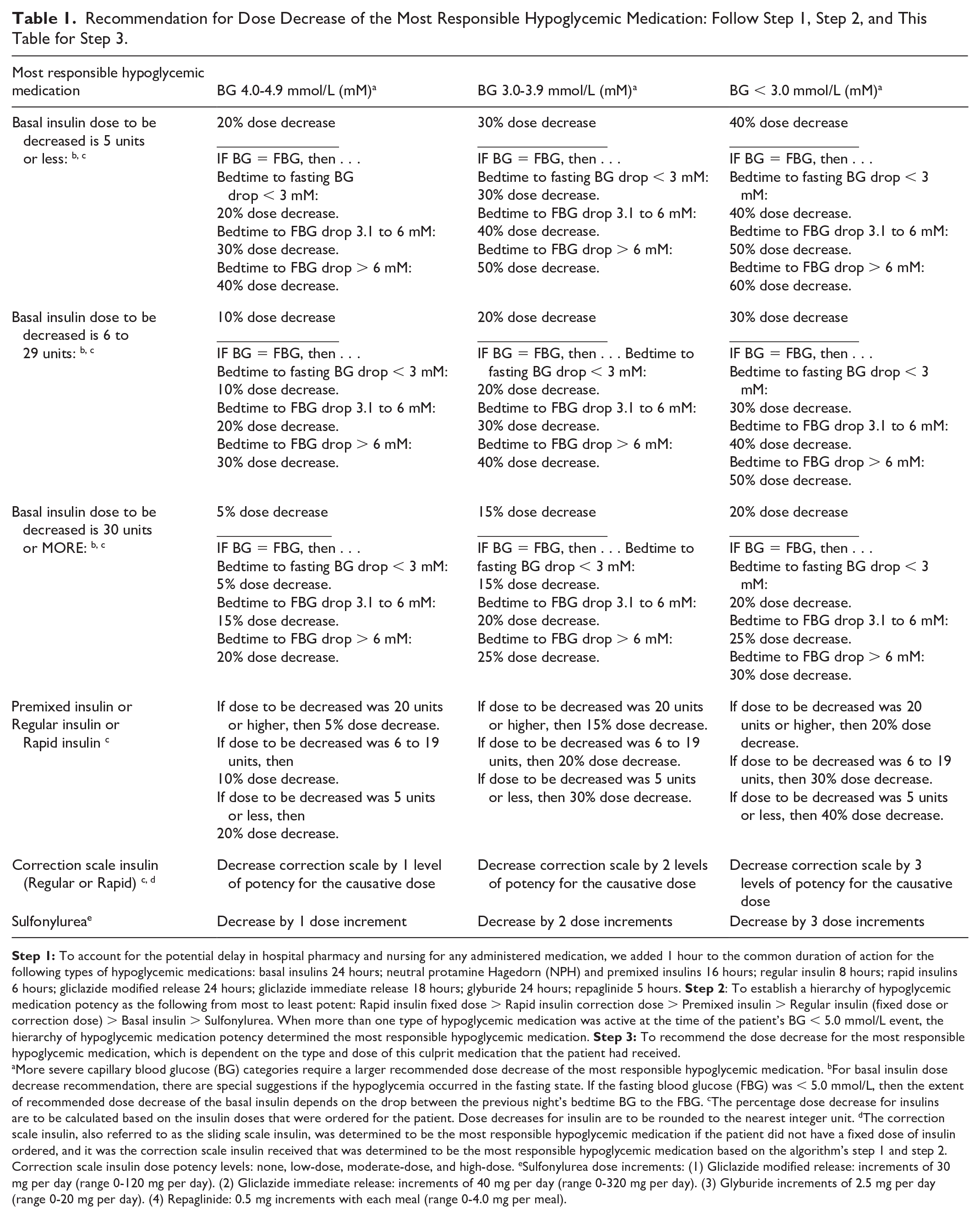
More severe capillary blood glucose (BG) categories require a larger recommended dose decrease of the most responsible hypoglycemic medication. bFor basal insulin dose decrease recommendation, there are special suggestions if the hypoglycemia occurred in the fasting state. If the fasting blood glucose (FBG) was < 5.0 mmol/L, then the extent of recommended dose decrease of the basal insulin depends on the drop between the previous night’s bedtime BG to the FBG. cThe percentage dose decrease for insulins are to be calculated based on the insulin doses that were ordered for the patient. Dose decreases for insulin are to be rounded to the nearest integer unit. dThe correction scale insulin, also referred to as the sliding scale insulin, was determined to be the most responsible hypoglycemic medication if the patient did not have a fixed dose of insulin ordered, and it was the correction scale insulin received that was determined to be the most responsible hypoglycemic medication based on the algorithm’s step 1 and step 2. Correction scale insulin dose potency levels: none, low-dose, moderate-dose, and high-dose. eSulfonylurea dose increments: (1) Gliclazide modified release: increments of 30 mg per day (range 0-120 mg per day). (2) Gliclazide immediate release: increments of 40 mg per day (range 0-320 mg per day). (3) Glyburide increments of 2.5 mg per day (range 0-20 mg per day). (4) Repaglinide: 0.5 mg increments with each meal (range 0-4.0 mg per meal).
Our study trained certified diabetes educators (CDEs) to act reflexively like a software program running the automatable algorithm. From 23 October to 17 December 2023, the study’s CDEs worked shifts that covered 39% of the time. Alert messages were sent to the attending teams for 568 inpatient BG < 5.0 mmol/L events. Retrospective review of each of the algorithm’s recommendations showed that they were clinically-justified.
Compared to the same 8-week span in 2022, during this 2023 study, the number of BG < 4.0 mmol/L events decreased from 861 to 771 (P = .0002). The more severe BG < 3.0 mmol/L incidents decreased from 19.5% to 14.5% (P = .008).
Limitations of this algorithm include when a clinician chooses to decrease the doses of more than one of the hypoglycemic medications. Our algorithm is a potential starting point upon which future studies of DM technology software programming could build upon. Future studies could also integrate all classes of medications potentially influencing glucose levels, as well as other factors such as physiotherapy sessions, diet adjustments, and so on, into the software program that is connected with electronic medication ordering.
Footnotes
Acknowledgements
None.
Abbreviations
BG, Blood glucose; CDEs, certified diabetes educators; DM, diabetes mellitus.
Contributorship
CJS, HL, and J.Sh designed the study. LGM, J.Sa, and AGM participated in carrying out the study and data collection. LGM and CJS analyzed the data. All authors contributed to writing the manuscript. All authors approved the final version of the manuscript that is submitted. CJS is the guarantor for this study.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding was provided by The Ottawa Hospital Academic Medical Organization, grant number 2022-23 Innovation Fund TOH-23-017.
Ethics
The Ottawa Health Science Network Research Ethics Board exempted this study because this was a Quality Improvement study.