
Abstract

Prediabetes is commonly defined by intermediate glycemic ranges between normoglycemia and diabetes and is associated with an increased risk of progression to type 2 diabetes mellitus (T2DM) and cardiometabolic complications. 1 Current approaches to identifying prediabetes rely primarily on static glycemic thresholds such as hemoglobin A1c (HbA1c), fasting plasma glucose (FPG), or impaired glucose tolerance (IGT) during an oral glucose tolerance test (OGTT). Despite its clinical significance, a substantial proportion of individuals with prediabetes remain undiagnosed, as conventional tests may not fully capture dynamic disturbances in glucose regulation. 1
Increasing evidence suggests that dysglycemia may be better understood as a continuum rather than a discrete transition from normoglycemia to diabetes. Conceptual frameworks have proposed that the traditional category of prediabetes may oversimplify a heterogeneous metabolic process that evolves through progressive stages of glycemic dysregulation. 2 Technologies capable of capturing dynamic glucose patterns may therefore offer additional insight into early metabolic disturbances. In this context, studies using continuous glucose monitoring (CGM) have demonstrated that individuals without diagnosed diabetes can exhibit markedly different glycemic patterns during daily life despite normal conventional laboratory values.3-5
A recent systematic review and meta-analysis quantified differences in CGM metrics between individuals with prediabetes and those with normoglycemia, including 1657 participants across 10 studies. 6 Prediabetes was consistently associated with significantly higher values across multiple dynamic CGM parameters: mean amplitude of glycemic excursions (MAGE; mean difference [MD] = 9.81 mg/dL, 95% CI = 4.31-15.31), time above range greater than 140 mg/dL (TAR; MD = 5.68%, 95% CI = 1.04-10.32), 24-hour mean glucose (MD = 7.91 mg/dL, 95% CI = 6.27-9.55), and coefficient of variation (CV; MD = 1.54%, 95% CI = 0.67-2.41). These findings provide the first quantitative evidence that CGM can detect statistically significant differences between prediabetes and normoglycemia using metrics that reflect glucose dynamics rather than single-point measurements. We hypothesize that a stage of CGM-detectable dysglycemia may precede conventional prediabetes thresholds, characterized by dynamic alterations in glucose regulation despite normal HbA1c and FPG; however, prospective longitudinal validation is required to confirm this concept.
Within the staging framework proposed by Shah et al, 2 CGM-derived metrics, particularly MAGE, TAR, mean glucose, and CV, could serve as complementary tools in metabolic risk stratification, especially in individuals with borderline or discordant HbA1c and FPG values. Integrating CGM into existing frameworks need not require redefining diagnostic thresholds; rather, it offers a physiologically richer characterization of glycemic dysregulation that static tests cannot provide (Figure 1).
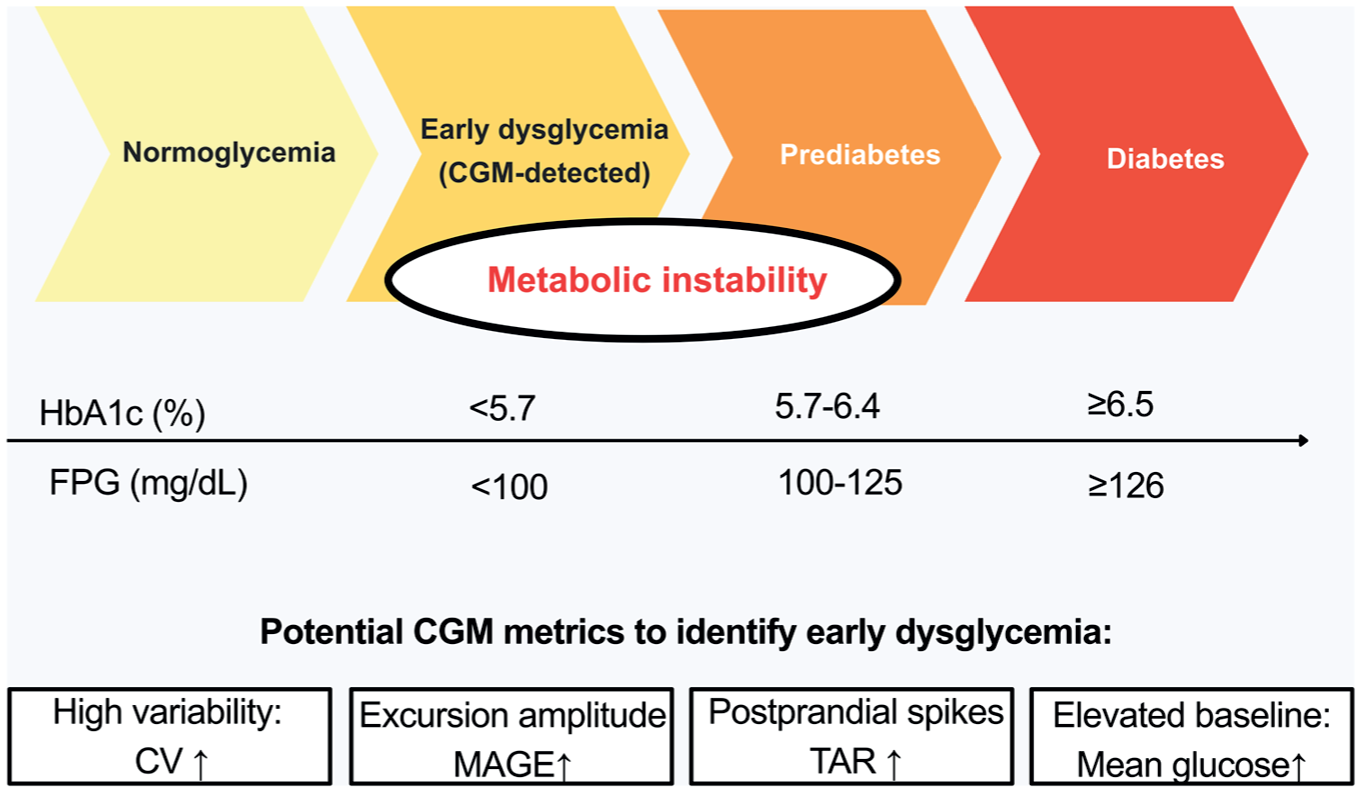
Conceptual model of the glycemic spectrum from normoglycemia to diabetes. An early stage of CGM-detectable dysglycemia is hypothesized to precede conventional prediabetes thresholds, characterized by dynamic alterations in glucose regulation despite normal HbA1c and fasting plasma glucose (FPG); prospective longitudinal validation is required to confirm this concept. Potential CGM-derived metrics to identify early dysglycemia include increased mean amplitude of glycemic excursions (MAGE), elevated time above range (TAR), higher 24-hour mean glucose, and increased coefficient of variation (CV).
With CGM technology becoming increasingly accessible, these dynamic metrics may complement conventional laboratory markers in assessing early metabolic dysregulation in individuals without diabetes. As the available evidence remains predominantly cross-sectional, prospective longitudinal studies incorporating standardized CGM wear protocols are needed to establish whether these metrics contribute predictive value beyond existing tools and to define their role in precision prevention strategies.
Footnotes
Acknowledgements
None to declare.
Abbreviations
CGM, continuous glucose monitoring; CV, coefficient of variation; FPG, fasting plasma glucose; HbA1c, hemoglobin A1c; IGT, impaired glucose tolerance; MAGE, mean amplitude of glycemic excursions; OGTT, oral glucose tolerance test; TAR, time above range; T2DM, type 2 diabetes mellitus.
Author Contributions
All authors contributed equally to the conceptualization, writing, and revision of the manuscript.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Supported by the Semmelweis University Research, Development and Innovation Fund.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.