
Abstract
Background:
Stability of insulin varies on storage conditions, handling, and types of formulations, and in Tanzania, unreliable refrigeration and climate fluctuations can compromise storage, which can reduce potency. Real-world data are crucial for optimizing diabetes management in developing countries. Previous studies have reported mixed findings, linking insulin degradation to temperature fluctuations, formulation issues, and distribution challenges. This study assessed the impact of storage conditions on insulin content during usage among diabetic patients at Bugando Medical Centre (BMC).
Methods:
This cross-sectional study, conducted from April to July 2024 in Mwanza, assessed the quality of 16 batches of insulin using the high-performance liquid chromatograph (HPLC) method. Insulin samples were collected from 48 diabetic patients attending the diabetic clinic at BMC and analyzed for physical appearance, identity, and concentration, while storage conditions were monitored using a Bluetooth temperature data logger.
Results:
Of the 16 insulin batches analyzed, 7 (43.8%) had low active insulin content, while 4 batches (25%) contained no active insulin at all. Among the 48 patients sampled, 24 (50%) were using substandard insulin. Of the 26 patients who used 2 separate vials, 15 had at least 1 vial that failed to meet standard specifications. Among the 20 patients using a single combined vial, 7 (35%) had low insulin content.
Conclusion:
All patients stored insulin within recommended temperature conditions; however, several samples were substandard, with some batches failing specifications. While 56.2% met United States Pharmacopeia (USP) requirements, the remaining showed variability and reduced concentrations.
Keywords
Introduction
Diabetes mellitus (DM) continues to pose a significant public health and economic burden, particularly in low- and middle-income countries (LMICs). 1 Insulin therapy remains essential for individuals with type 1 diabetes and for patients with advanced type 2 diabetes who do not achieve adequate glycemic control with oral antidiabetic agents. 2
Structurally, insulin is a peptide hormone composed of 51 amino acids arranged in 2 polypeptide chains (A and B) linked by disulfide bonds. 3 While earlier insulin products were derived from animal sources, advances in biotechnology led to the development of recombinant human insulin formulations. 4 Differences in molecular structure, formulation composition, and manufacturing processes across insulin products necessitate careful evaluation of their stability under various storage conditions. 5
Because insulin is a protein-based therapeutic, its physicochemical stability is highly susceptible to environmental influences. Temperature fluctuations, changes in pH, agitation, and mechanical stress can compromise structural integrity. 6 Standard recommendations advise that unopened insulin vials be stored at 2–8 °C, whereas in-use products may be kept at room temperature (typically 20-30 °C) for a limited duration, commonly up to 28 days. 7 Exposure to temperatures outside these ranges can accelerate degradation, reduce potency, and increase the risk of poor glycemic control. Pharmacopeial standards, such as those of the United States Pharmacopeia (USP), require that insulin products maintain 95% to 105% of their labeled potency throughout their shelf life. Deviation from these standards poses significant risks for diabetes management.8,9
Although international guidelines for insulin storage are well established, maintaining optimal storage conditions can be challenging in resource-limited settings. 10 In Tanzania and similar LMICs, patients may face unreliable electricity supply, limited access to refrigeration, high energy costs, and reliance on alternative cooling methods.10,11 Such environmental conditions raise concerns regarding the preservation of insulin quality at the household level.
In addition to temperature-related instability, insulin may undergo structural alterations when subjected to repeated agitation or mechanical stress during routine handling. These stressors can promote molecular unfolding, aggregation, fibril formation, and precipitation, ultimately reducing active drug content. 12 Beyond storage conditions, insulin quality can be affected by manufacturing inconsistencies, cold chain failures, and suboptimal formulation. 7 In 2009, Eli Lilly received a $10 million settlement from its distribution contractor after an insulin shipment was exposed to freezing temperatures. 7
Given the combined challenges of environmental exposure, household storage constraints, and potential supply chain vulnerabilities, there is a critical need to generate context-specific evidence on insulin quality in Tanzania. This study therefore evaluates the potency of in-use insulin samples collected directly from diabetic patients. By examining products stored under actual household conditions, the study aims to provide empirical data that may inform public health interventions, strengthen patient education on storage practices, and support strategies to safeguard insulin quality across the distribution range.
Materials and Methods
Study Design, Duration, and Setting
This was a cross-sectional laboratory-based study design conducted between April and July 2024. Diabetic patients on insulin were identified at Bugando Medical Centre (BMC) in Mwanza, Tanzania. This is a tertiary referral hospital providing health care to patients around the Lake Victoria area and from the other 30 regions in Tanzania. The hospital provides a variety of specialized and super specialized health services along with research, training, and consultation. Approximately 50 diabetic patients are attended on average per visit and 2 diabetic clinics are carried out per week (Bugando Medical Records, 2023).
Sample Size Estimation
The insulin samples used in this study were obtained from a research investigation on contamination during administration and various household storage practices. 13 The Kish-Leslie formula is commonly used to estimate sample sizes for cross-sectional studies where the primary objective is to determine a proportion or prevalence within a population. In this study, the aim was to estimate the proportion of insulin samples that may be compromised in quality among diabetic patients at Bugando Medical Centre. The sample size was estimated based on the previous study;14,15 the estimated sample size was 80 insulin vials.
Sampling Procedure, Inclusion, and Exclusion Criteria
We used the clinic patient register to identify diabetic patients on insulin therapy. We identified 51 patients whom we purposively sampled and conveniently recruited into our study. Each of the patients was consulted on insulin usage, and 30 reported using 2 insulin vials (intermediate-acting and short/rapid-acting insulin), while 21 used single insulin vials containing both intermediate-acting and short/rapid-acting insulin. The patients were requested to come with the vials during their next clinic visit. However, for those who did not come with their vials, home visits were conducted to collect them. In all patients, we replace their insulin not to interrupt their treatment. Although our estimated sample size was 80, we received and analyzed 74 samples from 16 batches; 6 samples were excluded due to a lack of manufacturing date or expiry date and another reason was insufficient volume of insulin sample required for analytical test. During collection, the insulin vials and cartridges were transported to the Tanzania Medicine and Medical Device Authority (TMDA); to minimize potential degradation during transportation, insulin samples were stored in a sterile cooling box. Of the 16 batches of the insulin samples analyzed, 11 (68.7%) were obtained directly from patients during their clinic visits, while the remaining samples were collected through home visits. All samples were collected after approximately 3 weeks of in-use duration to ensure consistency in assessing insulin quality under real-world storage conditions.
Upon arrival at the TMDA, laboratory scientists washed their hands and wore sterile gloves to ensure no contamination was transferred to the insulin vials from laboratory personnel. Each sample (vial or cartridge) was then labeled with the date and time of collection, type of insulin, storage condition, and expiry date. To prevent contamination during the withdrawal of insulin, the caps of the vials/cartridges were disinfected with 70% alcohol. Sterile insulin syringes were used to withdraw insulin from the vials/cartridges for analytical test.
Household Insulin Storage Condition
Patients were provided with temperature data loggers to monitor household storage conditions. This study employed the same devices and standardized procedures as those used in our previous study, which evaluated insulin samples collected from pharmacies. 11
Material and Reagents
Reagents used included human insulin CRS batch 5 (EDQM, Strasbourg, France), Water (Sigma-Aldrich, Milli-Q water purification system, United States), orthophosphoric acid, and sodium anhydrous sulfate (Sigma-Aldrich, analytical grade, United States). Apparatus that was used include measuring cylinder (Pyrex Measuring Cylinder [Make: Pyrex, United States]), volumetric flask (Class A Volumetric Flask [Make: Duran, Germany]), beaker (Beaker: Pyrex Beaker [Make: Pyrex, United States]), thermometer (H–B Instrument Thermometer [Make: H–B Instrument, United States]), and analytical scale (Mettler Toledo Analytical Balance [Make: Mettler Toledo, Switzerland]).
Equipment
The HPLC machine (Model: Agilent 1260 Infinity II HPLC System: Agilent Technologies, United States) which was used for quantification of human insulin from samples collected. pH meter (Mettler Toledo Seven Compact S220 pH Meter [Make: Mettler Toledo]) for measuring pH, sonicator (Branson SFX150 Sonifier [Make: Branson, United States]) for sonication, blue tooth temperature data logger (Verigo Model PA3 [Make: United Kingdom]).
Data Collection Procedure
Data on unopened insulin products, which served as the control group, were obtained from pharmacy samples and had been previously published. 11 All human insulin samples collected from patients with DM were visually inspected for physical appearance, and their storage conditions were continuously monitored. In addition, relevant labeling information including manufacturing date, expiry date, batch number, generic name, and brand name was recorded. A structured questionnaire was also administered to collect sociodemographic information from the participants.
System Suitability Test and Identification Test
System suitability solution of 1.5 mg/mL of human insulin in 0.01 N hydrochloric acid was prepared and allowed to stand at room temperature for not less than 3 days (NLT 3 days) to obtain a solution containing NLT 5% of A-21 desamido insulin human. The prepared solution was injected into HPLC, and the mobile phase was prepared according to the USP monograph. The system suitability requirements are: Peak resolution NLT 2.0 between human insulin and A-21 desamido human insulin, system suitability solution. Tailing factor not more than (NMT 1.8). The retention time of the major peak of the sample solution corresponds to that of the standard solution, as obtained in the assay; it will confirm the identity.
Assay Test
An assay test is an analytical method used to assess the purity, potency, or content of a particular substance within a sample. The analytical procedure for concentration determination was carried out according to the USP monograph. 16
Statistical Analysis
Statistical analysis was performed using STATA version 15 for data obtained from the questionnaire, while Microsoft Excel was used to analyze assay results from different brands of human insulin collected in Mwanza, Tanzania. Descriptive statistics, including mean, standard deviation, and percentage, were used to summarize the data.
Results
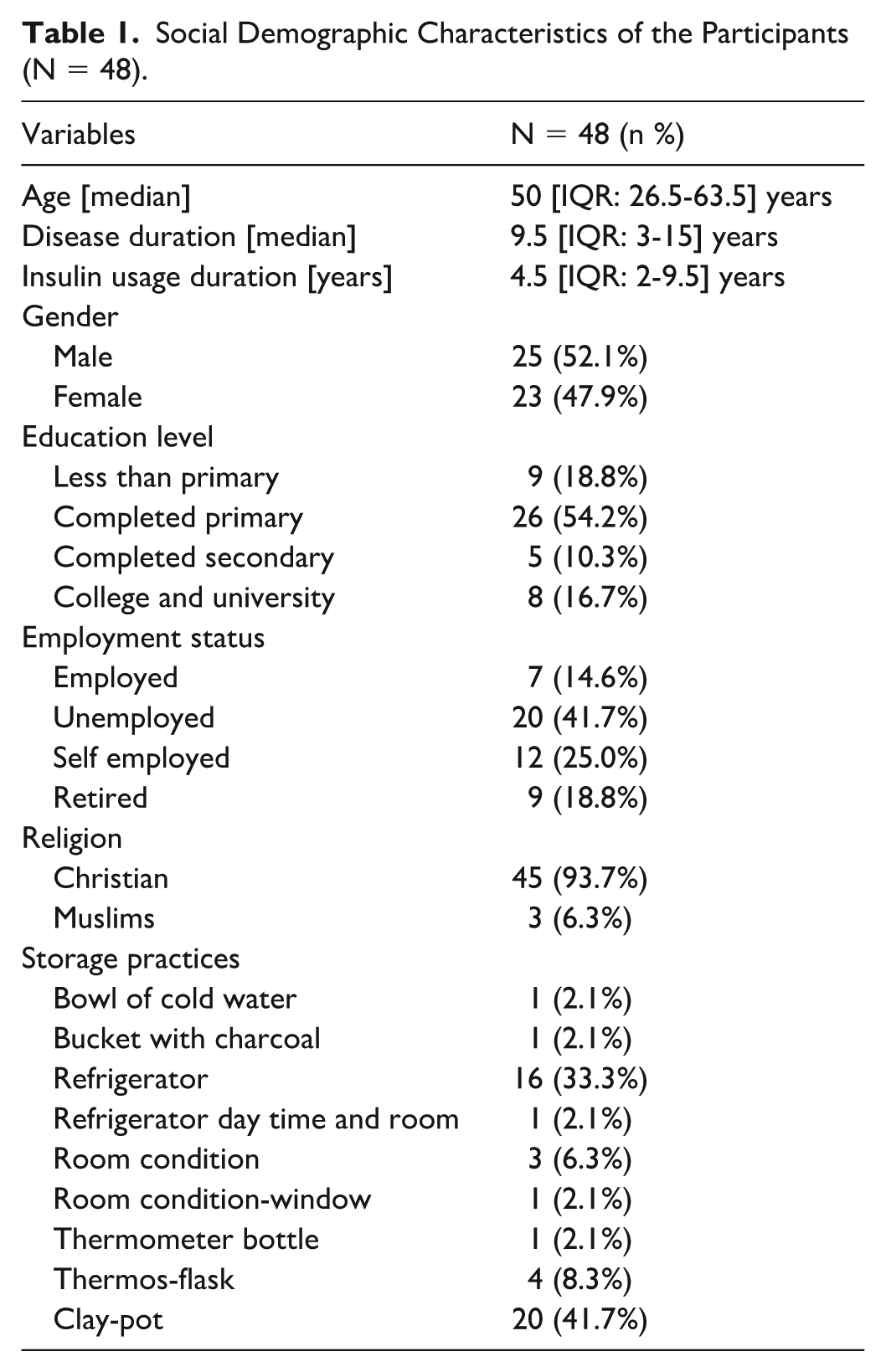
A total of 48 diabetic patients were recruited from the BMC diabetic clinic. Half of the patients were male 25 (52.1%). The median age of study participants is 50 [interquartile range [IQR] = 26-63.5] years. In addition, half of the participants had been living with the disease for nearly 9 years and had been using insulin for nearly 5 years. About half, 26 (54.2%), of the patients had attained primary school education, 20 (41.7%) were not married, and 20 (41.7%) were unemployed. Out of the 48 DM patients enrolled, 20 (41.7%) stored their human insulin in a clay pot, which is a traditional evaporative cooling method commonly used in settings with limited or unreliable electricity. In contrast, 16 patients (33.3%) used a refrigerator for storage. The higher proportion using clay pots indicates that many patients rely on non-electric storage options due to either inconsistent access to refrigeration or socioeconomic constraints. The sociodemographic characteristics of the study participants are summarized in Table 1.
Social Demographic Characteristics of the Participants (N = 48).
Household Storage Conditions for Insulin During Use
Temperature monitoring in all 48 DM patients revealed that insulin stored at room temperature had a maximum mean kinetic temperature of 31.2 °C, a minimum of 29.2 °C, and an overall mean of 29.3 °C. In contrast, insulin samples stored in clay pots, refrigerators, and thermos flasks were maintained within the required temperature range during the study period, with mean kinetic temperatures of 20.4 °C, 3.8 °C, and 17.5 °C, respectively. The minimum and maximum mean kinetic temperatures for these storage methods were as follows: clay pots (9.2 °C-22.2 °C), refrigerators (3 °C-4.9 °C), and thermos flasks (17 °C-18 °C). Due to limitations of the temperature loggers used, time outside the recommended temperature range (TOR) could not be assessed. Therefore, while mean kinetic temperature (MKT) provides an overall estimate of thermal exposure, it does not capture short-term temperature excursions, and caution is required when interpreting the relationship between storage conditions and insulin potency.
System Suitability
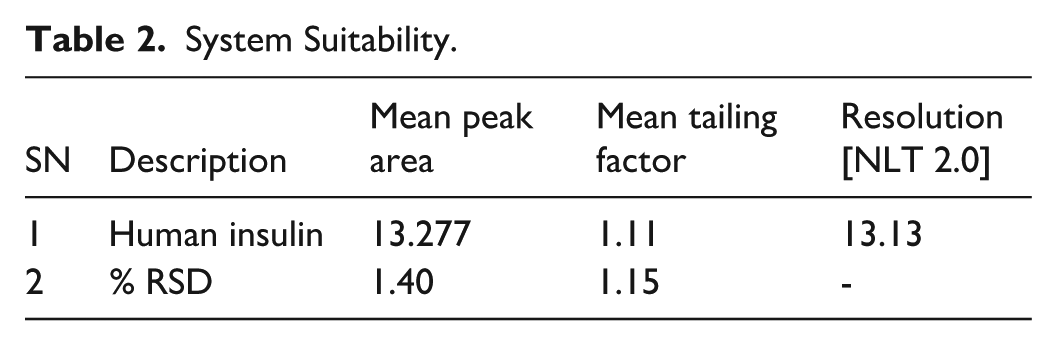
System suitability testing confirmed adequate chromatographic performance. The system achieved a resolution of NLT 2.0, indicating sufficient separation efficiency, and a tailing factor of 1.11 with a relative standard deviation (RSD) of 1.15%, demonstrating acceptable peak symmetry. These results confirm that the analytical system met the required suitability criteria as shown in Table 2.
System Suitability.
Identification of Active Insulin in a Sample and Its Degradation Products
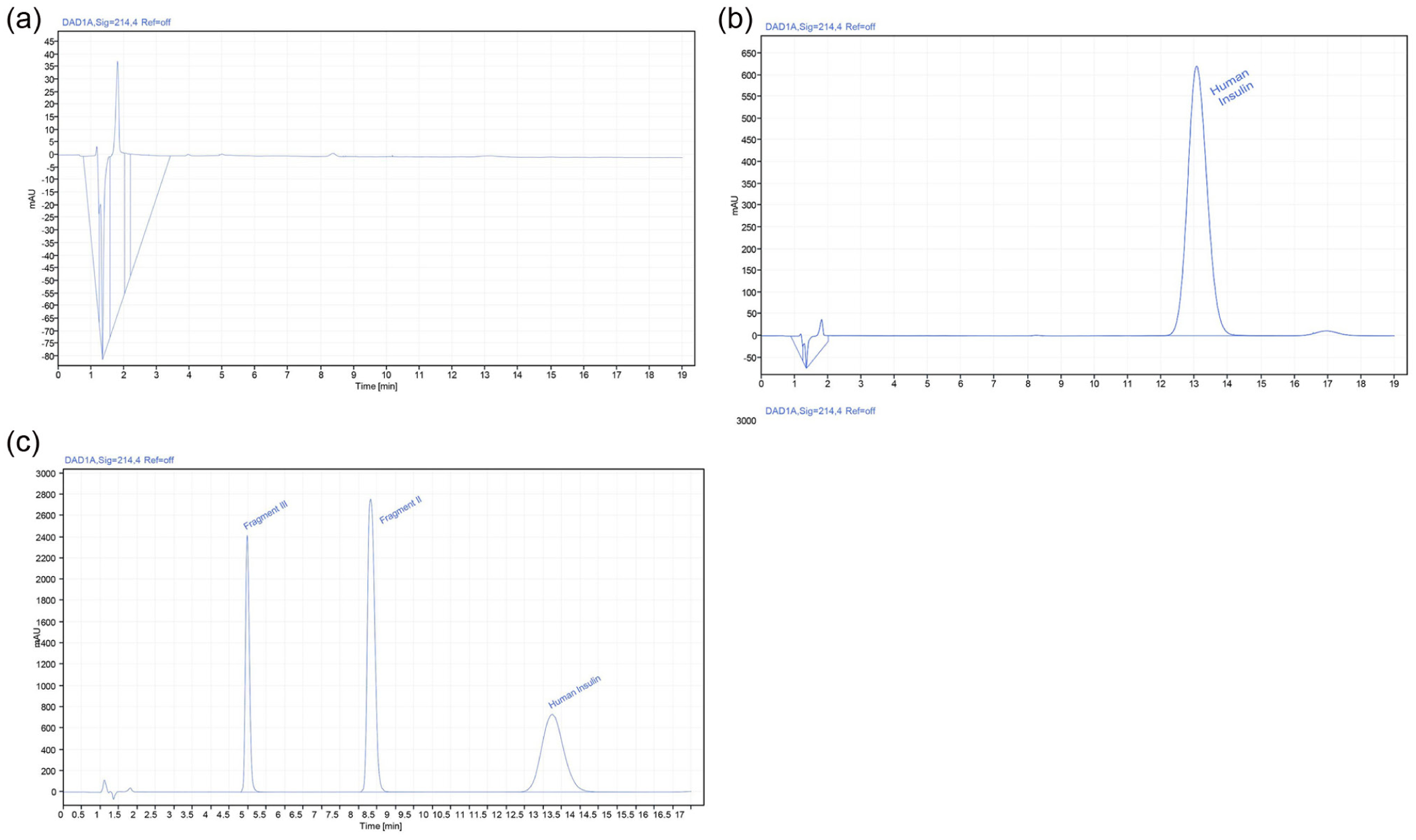
The retention times for the samples aligned with those of the reference standard, with mean retention times of 13.42 ± 0.2 for the samples and 13.45 ± 0.2 for the standard. Figure 1 demonstrates the presence of active insulin in the analyzed sample; however, the sample peak height was lower than that of the reference standard, suggesting a lower insulin concentration. In contrast, Figure 2 showed no detectable active insulin during the analysis. Figure 3 further demonstrates the presence of active insulin in another analyzed sample, with the measured concentration meeting the acceptable limits specified in the USP monograph.
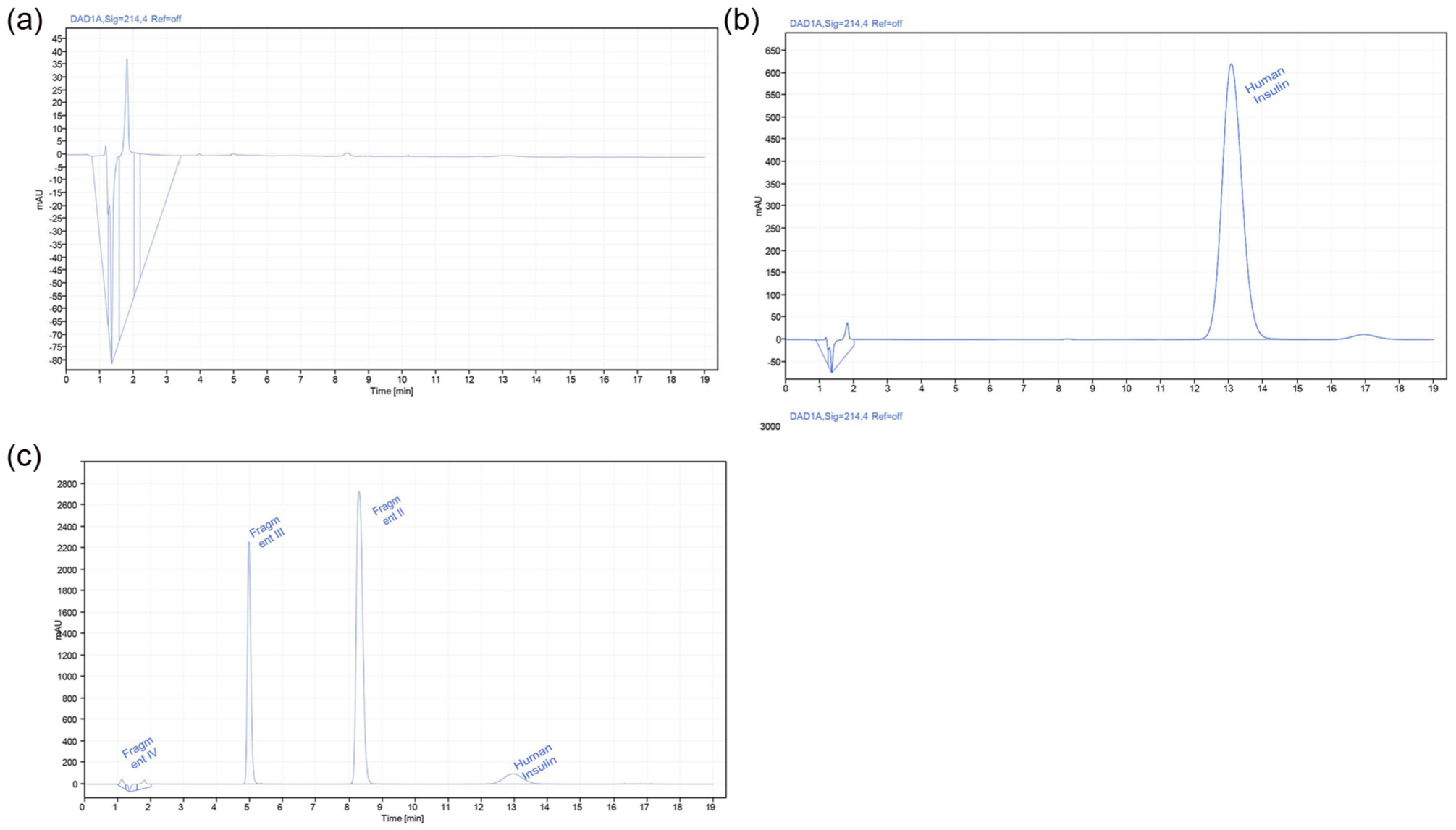
Chromatograms for the blank, reference standard solution of human insulin, and sample: (a) a chromatogram on the upper left shows the blank, (b) a chromatogram on the upper right shows the reference standard solution of human insulin CRS, and (c) a chromatogram on the lower left (with a batch no. TB6060622) shows human insulin samples. The mobile phase was acetonitrile and solution A in a 26:74 ratio, with detection at 214 nm.
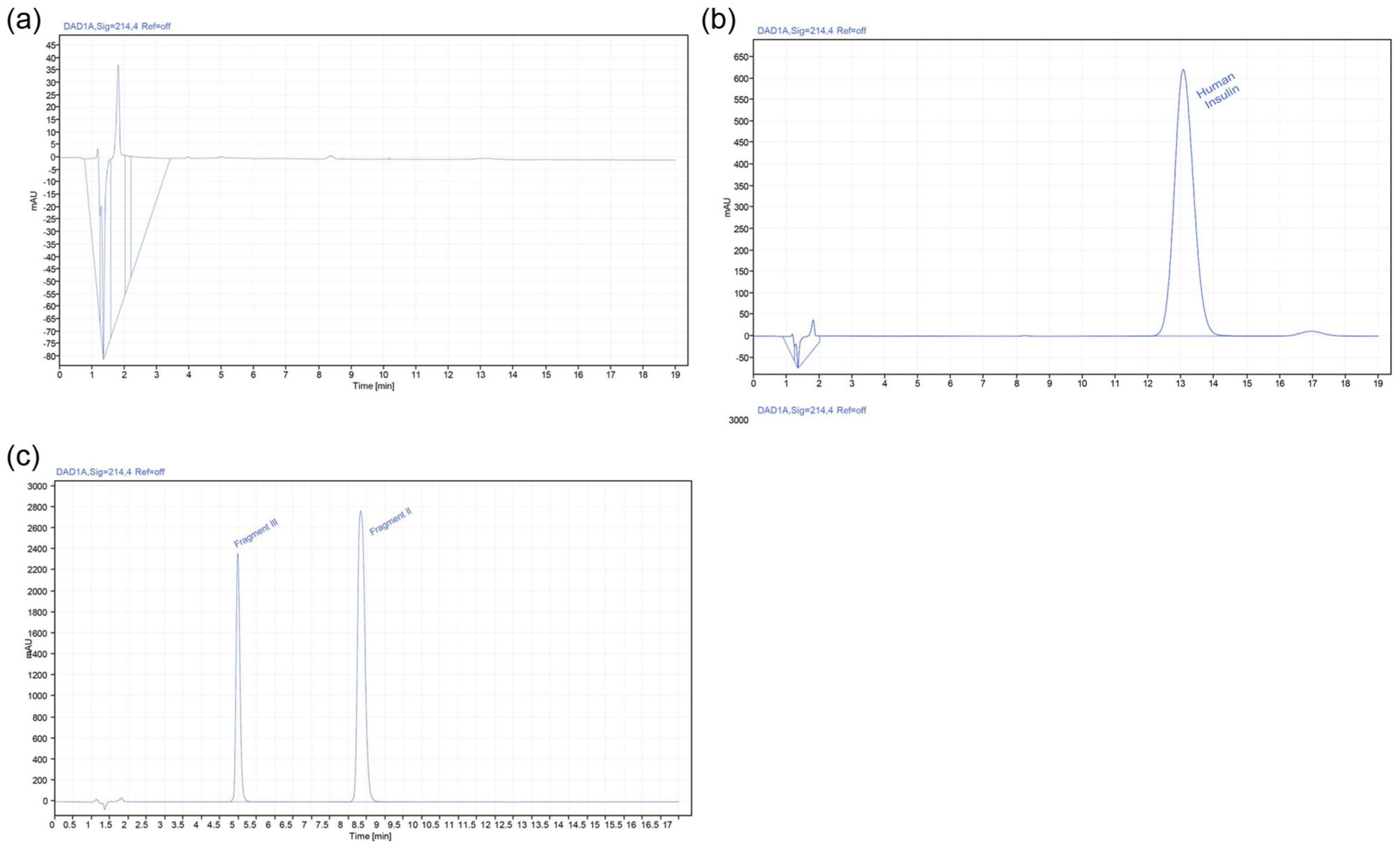
Chromatograms for the blank, reference standard solution of human insulin, and samples: (a) A chromatogram on the upper left shows the blank, (b) a chromatogram on the upper right shows the reference standard solution of human insulin CRS, and (c) a chromatogram on the lower left (with a batch no. D393054A) shows human insulin samples. The mobile phase was acetonitrile and solution A in a 26:74 ratio, with detection at 214 nm.
Chromatograms for the blank, reference standard solution of human insulin, and samples: (a) a chromatogram on the upper left shows the blank, (b) a chromatogram on the upper right shows the reference standard solution of human insulin CRS, and (c) a chromatogram on the lower left (with a batch no. D386743E) shows human insulin samples. The mobile phase was acetonitrile and solution A in a 26:74 ratio, with detection at 214 nm.
Chromatogram analysis revealed additional peaks in the insulin samples compared to the reference standard. While both showed an active insulin peak at 13 minutes, the samples exhibited 2 extra peaks at approximately 5 and 8 minutes, which were absent in the reference standard. This could suggest the presence of degradation products or excipients in the insulin samples; however, identifying the specific types was beyond the study’s scope.
Insulin Content in Products
The USP requires insulin content to be within 95% to 105% of the labeled content. Of the 19 insulin samples from batch D393054A, 10 (52.6%) were substandard. All 4 samples from batch TB6060222 were also substandard. For batch MT65N41, 2 out of 3 samples (66.6%) were out of specification. In batch D386743E, 1 out of 16 samples (6.25%) failed to meet the required specifications, and both samples from batch BF2201240 failed to meet the specifications. All remaining batches met the required specifications, as shown in Table 3.
Human Insulin Content in the Insulin Vial Which Contains Either Short/Fast or Intermediate-Acting Insulin Used by DM Patients.
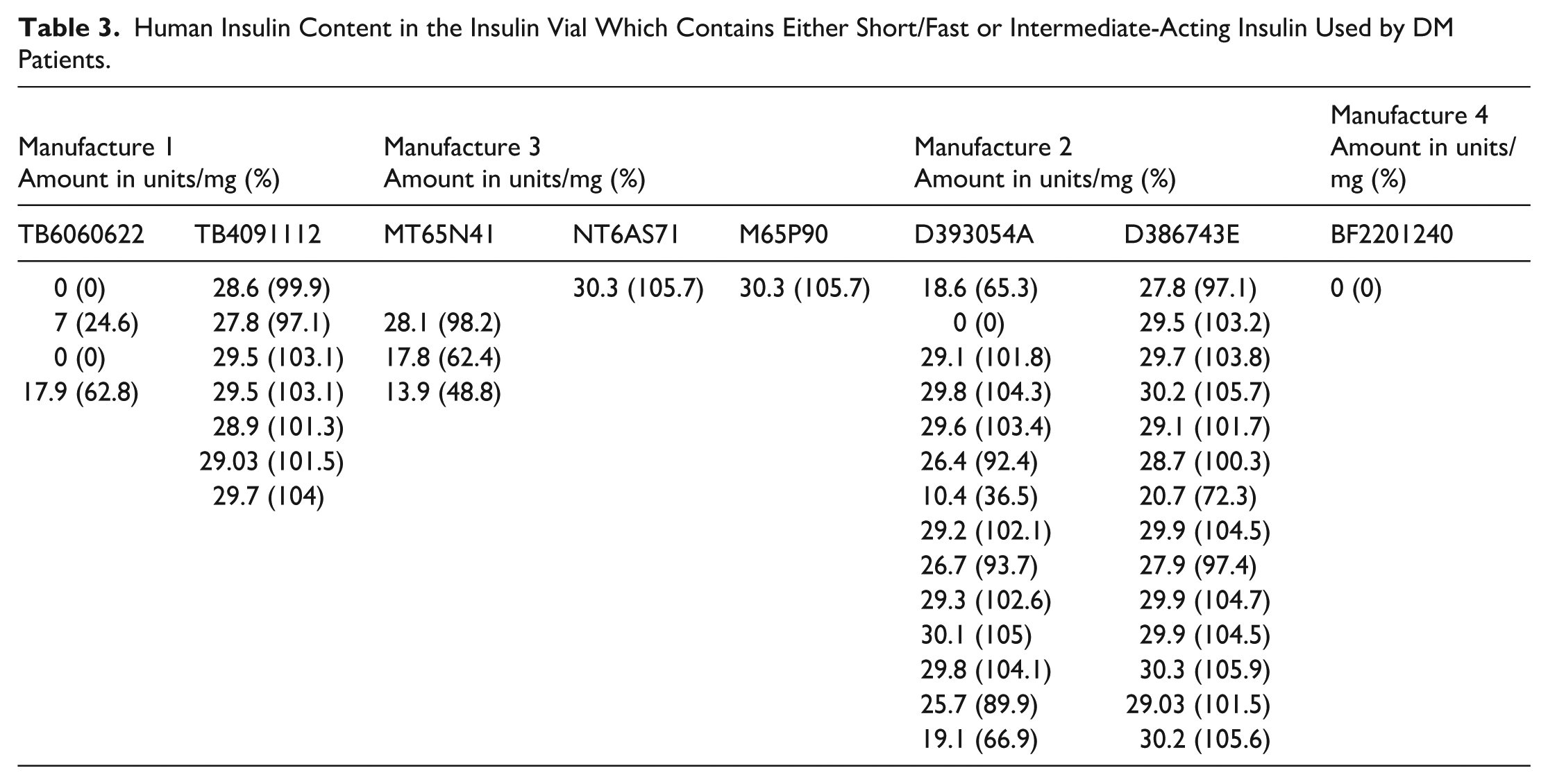
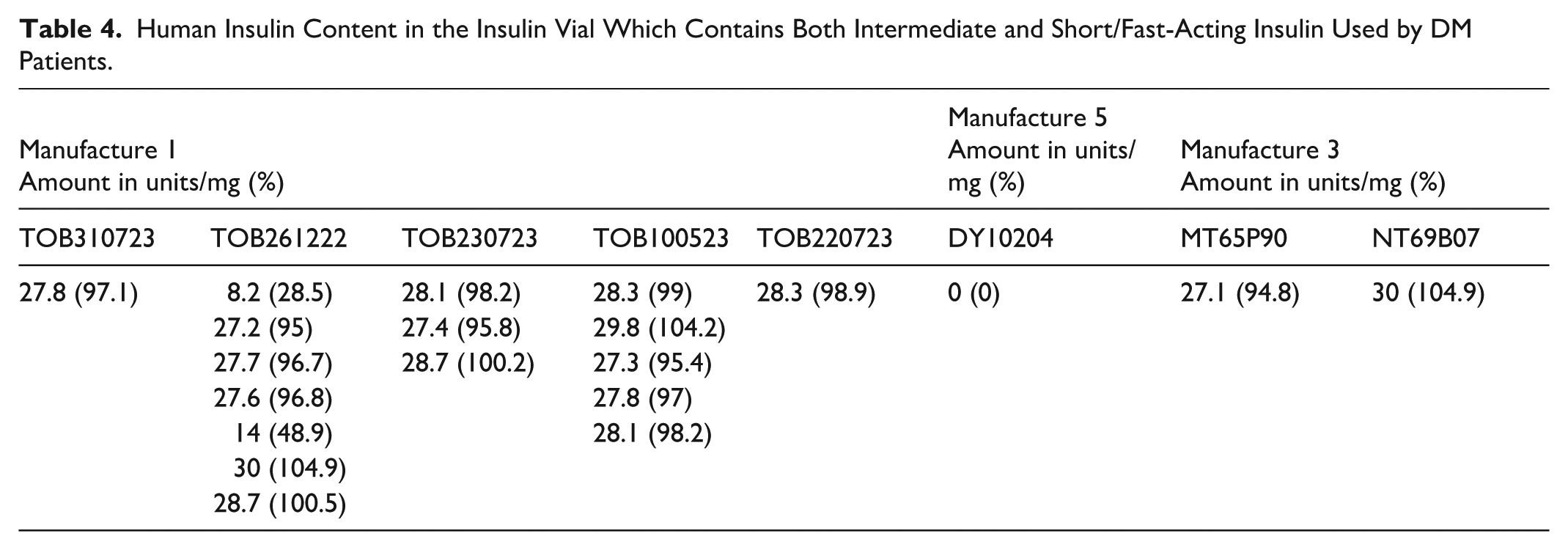
Table 4 summarizes the measured contents of human insulin from vials obtained from diabetic patients during usage (in-use insulin). These patients exclusively used single vials containing both intermediate-acting and short-acting human insulin. The analysis provides insights into insulin content variations within these vials used in diabetes management. Of the 7 samples from batch TOB261222, 2 (28.5%) were substandard, and 1 sample from batch DY10204 failed to meet the required specification. All remaining samples from the other batches met the USP specifications.
Human Insulin Content in the Insulin Vial Which Contains Both Intermediate and Short/Fast-Acting Insulin Used by DM Patients.
Discussion
The current study found that among 48 DM patients, 31 (64.5%) stored their insulin using traditional methods such as clay pots and containers filled with charcoal and water, consistent with findings from previous studies.17,18 Among the 16 batches of human insulin analyzed under these various household storage conditions, 9 (56.2%) met the USP specifications for insulin content per vial or pen. This observation is in line with earlier reports indicating that insulin can remain stable under a range of non-standard storage conditions. 19
Of the 16 batches of human insulin samples analyzed, 12 (75%) were confirmed to contain active human insulin based on their retention times, which matched the reference standard (13.42 ± 0.2) minutes for samples vs (13.45 ± 0.2) minutes for the standard, as shown in Figures 1 and 3. Also, 4 samples did not contain active human insulin, as shown in Tables 3 and 4 and Figure 2. The retention time obtained in the current study for identification purposes was consistent with that reported in a previous method-development study conducted on pharmaceutical preparations. 20
The out-of-specification results observed in batches D393054A and TB6060622 indicate varying concentrations of active insulin among different patients. These variations may be attributed to formulation or manufacturing deficiencies, as well as degradation of the active ingredient during storage, handling, or distribution. This is supported by a previous study conducted in the same setting, which reported that 13.3% of freshly obtained, unused insulin samples stored under recommended conditions were already substandard. These findings suggest that improper household storage alone cannot fully explain the observed out-of-specification results. 11 This is because insulin is among the complex biological product, in which there are so many variables to control during manufacturing.
The 4 samples from batches D393054A, TB6060622, BF2201240, and DY10204 that contained no active human insulin suggest major deficiencies in the manufacturing process, improper storage conditions during distribution, or chemical degradation. These findings highlight the need for stringent quality assurance measures during production, storage, and distribution to ensure the stability and efficacy of human insulin, ultimately safeguarding its therapeutic value for patients. Particularly, patients’ home storage conditions are not the sole factor contributing to reduced active insulin content. Even among patients storing both intermediate- and short/fast-acting insulin in refrigerators or clay pots, at least 1 sample was found to be out of specification; see it in Table 3. This aligns with the World Health Organization (WHO) Technical Report Series No. 961, 2011 (Annex 9), which emphasizes the critical role of proper storage and transport conditions for time and temperature-sensitive pharmaceutical products. Implementing its guidance, including continuous temperature monitoring and adherence to Good Storage and Distribution Practices, is essential in preventing degradation and ensuring insulin quality.
Out-of-specification results were observed even among patients who reported storing insulin in refrigerators. This highlights the importance of temperature monitoring using data loggers as a supplementary quality assurance tool to ensure insulin is consistently stored within the required temperature range. If a cold chain breach occurs, such as prolonged exposure to improper temperatures due to power outages or the practice of switching off refrigerators at night, insulin integrity may be compromised. In such cases, instead of continued use, the affected insulin should be discarded to prevent potential treatment failure.
Of the 16 (batch no. D393054A) human insulin samples stored in clay pots, 9 (56.3%) failed to meet required specifications. This suggests that clay pot storage is not the sole factor contributing to reduced insulin content. Other factors, such as formulation, manufacturing processes, and handling during cold chain distribution, may also play a role. Similarly, of the 3 insulin samples from batch TOB261222 stored in refrigerators, as shown in Table 4, 2 (66.7%) failed to meet specifications. Significant reductions in some samples may be attributed to formulation, manufacturing, or distribution issues. In contrast, less significant deviations could result from power outages or refrigerators being switched off at night.
Among the 3 insulin samples from batches D393054A, D386743E, and TOB261222 that were stored in a thermos flask, only 1 sample from batch D393054A showed reduced insulin content, suggesting that the decrease was not caused by the storage conditions. Additionally, insulin samples stored at room temperature, in a bowl of cold water, and in a charcoal-insulated bucket maintained the required content. We acknowledge that the lack of data on time outside the TOR represents a limitation of the study, as it limits our ability to draw definitive conclusions regarding the role of temperature in the observed out-of-specification findings.
Samples from batches BF23000685 and BF21003364 were collected from pharmacies, while batch BF22001240 was obtained from patients. All samples originated from the same manufacturer. Particularly, all batches were found to be out of specification despite complying with recommended storage conditions. This pattern may suggest a potential issue related to the formulation or manufacturing process for this product; however, given the study design, no definitive conclusions can be drawn. 11 Finally, during the study, it was observed that patients often carried insulin in handbags or envelopes after dispensing, without using a cooling box. This exposure to extreme temperatures could contribute to degradation. As a result, patients may have unknowingly used degraded insulin.
Study Limitations
The current study has several limitations that should be considered when interpreting the findings. First, baseline (pre-use) insulin content data for the analyzed batches were not available within the current study, which limits the ability to determine whether the observed deviations from pharmacopeial specifications originated prior to patient use or occurred during handling and storage. Although some batches corresponded to those evaluated in a previous study, direct paired comparisons were not systematically conducted. Second, while temperature monitoring was performed using data loggers and summarized using MKT, the devices used did not record time outside the TOR. Consequently, short-term temperature excursions could not be evaluated, limiting the ability to fully characterize temperature-related effects on insulin stability.
In addition, the study relied on a cross-sectional design, which limits the ability to establish temporal relationships between storage conditions and insulin quality. The assessment of insulin quality was based on analytical quantification of insulin concentration using HPLC, which reflects pharmacopeial potency but does not directly measure biological or clinical efficacy. Finally, although some samples were obtained from the same manufacturer and showed similar out-of-specification results, the study design does not allow definitive conclusions regarding the underlying cause (eg, manufacturing, formulation, or distribution factors), and such interpretations should be made with caution.
Clinical Implications
The use of substandard insulin products poses significant risks to diabetes management and patient health. Insulin with low or absent active contents can lead to poor glycemic control, resulting in hyperglycemia and acute complications such as diabetic ketoacidosis (DKA) and hyperosmolar hyperglycemic state (HHS).21,22 Over time, ineffective insulin therapy increases the risk of chronic diabetes complications, including cardiovascular disease, neuropathy, nephropathy, and retinopathy. These conditions not only degrade the quality of life but also escalate health care costs. Therapeutic failures caused by substandard insulin may be misinterpreted as non-compliance or treatment resistance, leading to unnecessary adjustments in treatment regimens. This situation can further frustrate patients, cause psychosocial stress, and erode their trust in health care systems. The broader implications of using poor-quality insulin extend to the health care system, with increased hospitalizations and a higher mortality risk among affected patients.
Another clinical implication of using insulin that has undergone structural changes to form insoluble aggregated amyloid is its potential to trigger immunologic reactions due to the deposition of this insoluble amyloid into subcutaneous. 12 Insulin-derived amyloidosis can lead to poor glycemic control, unpredictable hypoglycemia, and increased insulin requirements due to impaired absorption at affected sites.23,24 This phenomenon has been observed in 30% of diabetic patients undergoing insulin treatment. 12
Policy Implications for Insulin Quality Control in Tanzania
Addressing insulin quality issues in Tanzania requires strengthening quality assurance measures across the entire supply chain. This includes implementation of cold chain quality assurance practices, rigorous testing to ensure insulin products remain potent. Improving and enhancing cold chain distribution infrastructure are critical to preserving insulin efficacy. In addition, regular training for personnel at the TMDA is essential to help identify substandard pharmaceutical products in the market. Coupled with stricter regulatory oversight and enforcement, these measures are vital to upholding quality standards.
Conclusion
In this study, household storage conditions for insulin were within the recommended range for all DM patients. Despite this, several insulin samples were substandard, with some batches exhibiting out-of-specification results even under proper storage conditions. Although 9 (56.2%) batches met USP requirements, the remaining batches showed marked variability and inadequate concentrations.
Supplemental Material
sj-docx-1-dst-10.1177_19322968261459463 – Supplemental material for Quality of In-Use Insulin Under Real-World Storage Conditions in Mwanza, Tanzania
Supplemental material, sj-docx-1-dst-10.1177_19322968261459463 for Quality of In-Use Insulin Under Real-World Storage Conditions in Mwanza, Tanzania by Emmanuel Kimaro, Eveline T. Konje, Benson R. Kidenya, Amani T. Mori and Eliangiringa Kaale in Journal of Diabetes Science and Technology
Footnotes
Acknowledgements
The authors extend their thanks to the Catholic University of Health and Allied Sciences (CUHAS) and the Higher Education and Economic Transformation (HEET) project for funding this study, as well as to the Tanzania Medicine and Medical Devices Authority (TMDA) for their support with laboratory work. We also appreciate the expert reviewers for their valuable feedback, which greatly improved the quality of this article.
Abbreviations
BMC, Bugando Medical Centre; DM, diabetes mellitus; HHS, hyperosmolar hyperglycemic state; HPLC, high-performance liquid chromatograph; IDF, International Diabetes Federation; LMIC, low- and middle-income country; MKT, mean kinetic temperature; NLT, not less than; TMDA, Tanzania Medicine and Medical Device; USP, United States Pharmacopeia.
Authors’ Note
The conclusions and opinions expressed in this article are those of the authors and do not necessarily reflect those of their respective organizations.
Ethical Considerations
This study received ethical approval from the CUHAS/BMC RESEARCH COMMITTEE (CREC), reference number (CREC/746/2024).
Consent to Participate
Informed consent was obtained from all individual participants included in the study. Participants were provided with comprehensive information about the study’s purpose, procedures, potential risks, and benefits, and their participation was entirely voluntary. Written consent forms were signed by each participant, ensuring their understanding and agreement to partake in the research. Patient data were anonymized and stored in password-protected databases.
Consent for Publication
Not applicable.
Author Contributions
EK was responsible for the study’s conception and design, sample collection, data collection, funding acquisition, laboratory work, and manuscript writing. ETK and ATM handled result interpretation, critical manuscript revisions, data validation, and drafting sections of the manuscript. All authors contributed to the manuscript writing and revision. EK supervised the research process and provided the final review and approval of the manuscript. All authors have read and approved the final manuscript and are accountable for their respective contributions.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by the CUHAS and HEET Project, supported by the Government of Tanzania.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Data Availability Statement
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.