
Abstract
Background:
Ultrasound frequently detects hyperechogenic tissue at recent insulin infusion sites in youth using automated insulin delivery, but its short-term clinical significance is unclear.
Methods:
In this post hoc paired analysis of a prior 4-week prospective study, participants were included if they had both hyperechogenic and normoechogenic findings at the most recently used infusion site across 3 visits. Insulin dose and continuous glucose monitoring metrics from days 1 to 2 after infusion-set placement were compared within participants.
Results:
Seventeen participants met the inclusion criteria. Insulin dose and continuous glucose monitoring–derived outcomes did not differ significantly between tissue categories. Time since infusion-set removal differed between categories (1.6 vs 2.1 days, P = .049).
Conclusions:
In this paired analysis, binary ultrasound classification alone did not explain short-term glycemic variation.
Keywords
Background
Automated insulin delivery (AID) systems have become standard of care in pediatric type 1 diabetes management, improving glycemic outcomes while reducing treatment burden.1-4 Their performance also depends on reliable subcutaneous insulin absorption, making infusion-site tissue characteristics clinically relevant.
Ultrasound can detect tissue changes associated with insulin delivery. Hyperechogenic areas are frequently observed at recent infusion sites after 6 to 9 months of pump use. 5 Hyperechogenicity reflects increased tissue density, although its pathophysiology remains unclear, and has been used as a marker of subclinical lipohypertrophy. 6 In a recent pediatric study, hyperechogenic areas were frequently detected at recent infusion sites without palpable lipohypertrophy but were closely associated with time since infusion-set removal. 7
Because insulin infusion into lipohypertrophic tissue impairs absorption, 8 we hypothesized that infusion into ultrasound-detected hyperechogenic tissue might similarly alter insulin requirements and glycemic outcomes. In this post hoc paired analysis, we therefore compared outcomes within individuals when insulin was delivered into tissue later classified by ultrasound as hyperechogenic versus normoechogenic.
Methods
This was a post hoc paired analysis of a 4-week single-center observational study of 40 children and adolescents with type 1 diabetes recruited from Steno Diabetes Center Copenhagen, Denmark. Participants were users of AID systems 7 —Tandem T:slim X2 and MiniMed 780G. Ultrasound examinations of the most recently used infusion site were performed at 3 visits. Participants were eligible if they demonstrated both hyperechogenic and normoechogenic subcutaneous tissue at different visits, enabling paired within-participant comparison. No efforts were made in attempt to compare glycemic or subcutaneous tissue changes between types of AID systems. All participants used a standard 3-day infusion set with a Teflon cannula of 6 mm length.
Hyperechogenicity was defined as a visually increased echogenic signal in subcutaneous tissue compared with surrounding areas, as previously described. 5 For each qualifying visit, insulin and continuous glucose monitoring (CGM) data were extracted for days 1 and 2 after infusion-set placement at the assessed site. This was done to fairly compare CGM data across participants who may have had disparities in infusion-set wear time. Outcomes were insulin dose (U/kg/d), time in range (TIR, 3.9-10.0 mmol/L), time in tight range (TITR, 3.9-7.8 mmol/L), time above range (TAR, >10.0 mmol/L), time below range (TBR, <3.9 mmol/L), mean glucose, glucose standard deviation, and coefficient of variation. Mean values across days 1 and 2 were calculated for each visit and averaged by ultrasound classification. Within-participant comparisons were performed using paired t tests. Results are presented descriptively with P-values; no adjustment for multiple comparisons was performed. In this analysis, the day of infusion-set change (eg, Wednesday) was defined as day 0, with subsequent calendar days incrementing by one (eg, Thursday = day 1, Friday = day 2, etc).
The first author performed all clinical and ultrasound examinations, as well as validation and interpretation, using a Philips Lumify handheld ultrasound device (Philips, Amsterdam, the Netherlands). The first author was trained by Christina Kinnander, MD, PhD, Department of Radiology, Herlev and Gentofte University Hospital, who also provided expert support in interpreting ultrasound images and confirming diagnoses when findings were uncertain.
Results
Of the 40 participants in the original study, 17 met the inclusion criteria by demonstrating both hyperechogenic and normoechogenic tissue across visits. Median age was 11 years (range, 6-18), 8 participants were female, and median diabetes duration was 4 years (range, 1-16).
No significant within-participant differences were observed in insulin dose or glycemic metrics. Mean insulin dose was 0.70 ± 0.28 U/kg/d for sites later classified as hyperechogenic and 0.66 ± 0.24 U/kg/d for sites classified as normoechogenic (P = .6). TIR, TITR, TAR, TBR, mean glucose, glucose standard deviation, and coefficient of variation were also similar between categories (see Table 1).
Paired Comparison of Insulin Dose and Glycemic Metrics for Hyperechogenic Versus Normoechogenic Sites.
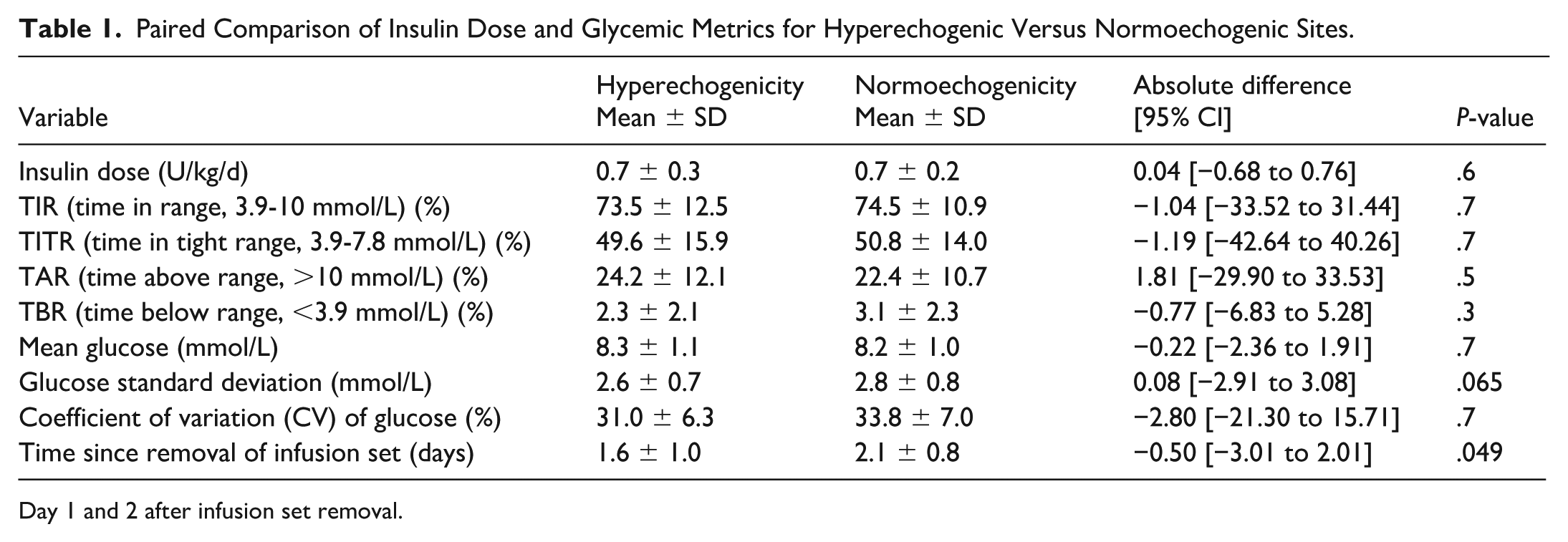
Day 1 and 2 after infusion set removal.
In contrast, the interval between infusion-set removal and ultrasound examination differed between categories: hyperechogenic findings were observed closer to infusion-set removal than normoechogenic findings (1.6 ± 1.0 vs 2.1 ± 0.8 days, P = .049; see Figure 1).
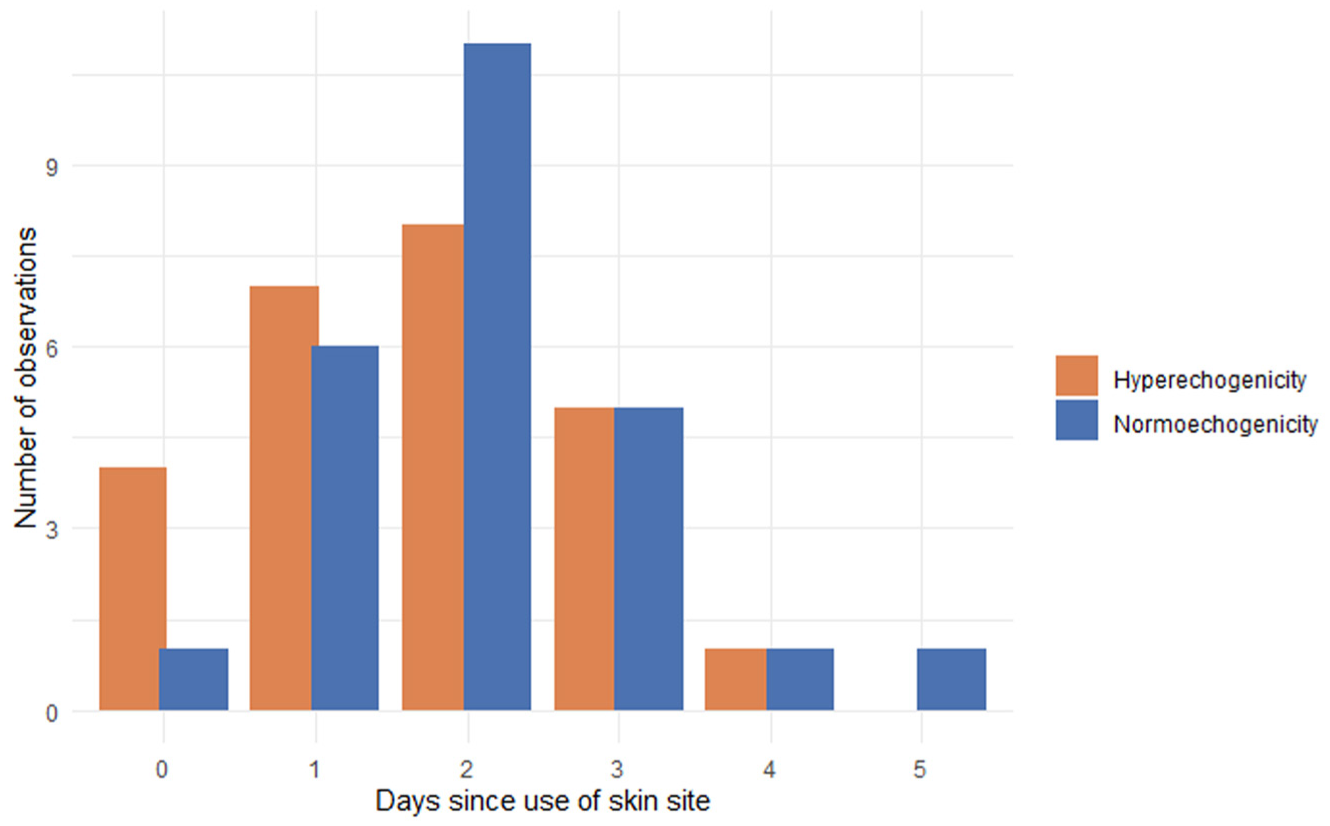
Number of ultrasound investigations demonstrating hyperechogenicity or normoechogenicity, respectively, of the subcutaneous tissue depending on number of days using that specific skin site for infusion of insulin.
Discussion
In this exploratory paired post hoc analysis, we found no significant within-participant differences in insulin requirements or short-term glycemic outcomes during days 1 to 2 after infusion-set placement when insulin was infused into sites later classified by ultrasound as hyperechogenic versus normoechogenic. These findings should be interpreted in the context of our previously published cohort-level analyses, which showed worsening glycemic outcomes with increasing infusion-set wear time, particularly beyond day 2, and associations between hyperechogenicity and lower TIR in the full cohort. 7 The current findings therefore extend rather than contradict our previous report.
Several factors may explain these results. First, prior work from the original study showed that hyperechogenicity is closely related to timing of ultrasound assessment relative to infusion-set use and removal. 7 In the present analysis, time since infusion-set removal differed significantly between hyperechogenic and normoechogenic areas, suggesting that the ultrasound appearance may partly reflect a transient tissue response and recovery process rather than a stable lesion with uniform metabolic consequences.
Second, hyperechogenicity may not represent a single entity, but rather a spectrum of dynamic tissue responses. From a subcutaneous tissue perspective, increased echogenicity may reflect different underlying processes, including inflammation, edema, tissue remodeling, or early fibrosis, each of which may affect insulin absorption differently. Yu et al 9 categorized lipohypertrophy into ultrasound subtypes—nodular, diffuse, and hypoechoic—and followed their progression over time. In the present study, echogenicity was assessed as a binary finding without subclassification by extent, morphology, or severity, which may have obscured clinically relevant heterogeneity and limited our ability to detect associations between specific tissue changes and glycemic outcomes.
Most previous studies of tissue-related insulin absorption have examined insulin injections into clinically evident lipohypertrophy. For example, Famulla et al and Johansson et al provide mechanistic evidence of an approximately 25% reduction in insulin absorption when insulin is injected into lipohypertrophic tissue.10,11 In those studies, insulin concentrations were quantified in blood under standardized conditions following injections into areas with clinically evident lipohypertrophy. This differs from the present study, which evaluated insulin infusion through an infusion set, where insertion trauma, local inflammation, wear time, and insulin flow around the cannula may also influence outcomes. 7 Therefore, findings from injection studies cannot be directly extrapolated to short-term infusion-set use in areas classified as hyperechogenic by ultrasound. In addition, our study measures insulin delivered over a longer period, which may be influenced by the site of infusion set with or without lipohypertrophy, intake of carbohydrates, physical activity, illness, and so on, making it harder to detect smaller but clinically meaningful effects.
Strengths include the paired within-subject design. Limitations include the small sample size, post hoc exploratory design, binary qualitative ultrasound classification, and potential behavioral and physiological confounders. Future studies should standardize timing of ultrasound assessment relative to infusion-set wear and removal and refine characterization of ultrasound-detected tissue changes.
Conclusions
In this exploratory analysis of children and adolescents using AID systems, we found no significant within-participant differences in insulin dose or short-term glycemic outcomes between hyperechogenic and normoechogenic injection sites.
These findings suggest that, within this selected paired subgroup, binary ultrasound classification alone may not capture the tissue characteristics most relevant to short-term glycemic outcomes. Larger studies are needed to clarify how ultrasound-detected tissue changes interact with wear time, recovery interval, and extent of tissue abnormality.
Ultrasound may detect early or subclinical tissue changes before they are clinically evident, offering a potential tool for individualized infusion site management. Detection of hyperechogenicity or other ultrasound abnormalities could help identify areas that should be avoided for future infusion-set placement, reinforce structured site rotation, and guide targeted patient education on insertion technique and site care. Focused ultrasound assessment of infusion sites can be performed in a few minutes by a trained health care professional, and the increasing availability of portable, lower-cost ultrasound systems may support broader clinical use in diabetes care.
Footnotes
ORCID iDs
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was financially supported by an external research program from Medtronic, but Medtronic had no influence on data collection, analysis, or reports.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.