
Abstract
Background:
Diabetes care generates substantial volumes of sharp and plastic waste, creating both safety and environmental concerns. We evaluated disposal practices for insulin-related sharps and devices among people with diabetes and assessed their awareness, attitudes, and sense of responsibility regarding appropriate disposal and environmental impact of diabetes-care waste.
Method:
We conducted a cross-sectional survey at the 2 hospital sites in Singapore. Adults with diabetes using insulin devices were eligible. An anonymized survey collected data on demographics, history and duration of diabetes diagnosis, sharps disposal practices, awareness of recycling and attitudes toward responsibility on safe sharps disposal and environmental sustainability. Descriptive statistics, correlations, and logistic regressions were carried out.
Results:
Sixty patients (mean age 46.0 ± 13.6 years; 56.7% female) completed the survey. Although 76.7% reported receiving advice on safe sharps disposal, only 6.7% used designated sharps containers for lancets while 25.0% discarded lancets directly into general waste; around half used plastic bottles whereas 20% used plastic bags or discarded insulin needles and syringes directly into general waste. Participants generally acknowledged that improper sharps disposal is a serious safety problem and considered proper disposal their personal responsibility. Receipt of advice from health care professionals was independently associated with safer sharps disposal (~20-fold higher odds, P = .002). Seventy-five percent were unaware that plastics in insulin pens are not recycled, and 55% did not know of available recycling facilities.
Conclusions:
Despite high perceived personal responsibility, disposal practices and recycling awareness among insulin users remain inadequate. Clearer guidance, structured education, and more accessible disposal and recycling infrastructure are needed.
Introduction
Diabetes mellitus is one of the most prevalent chronic conditions worldwide and it is projected to affect 589 million people by 2050. 1 Its management requires lifelong treatment with medications, glucose-monitoring supplies, and drug delivery devices. 2 Medical devices used by people with diabetes (PwD) range from insulin pens, needles, syringes and lancets to blood glucose-monitoring supplies, insulin pumps, and continuous glucose monitoring (CGM) systems. Many of these diabetes-related medical devices are intended for single-use to meet sterility and safety requirements, and they often contain multiple components, including plastics, packaging, electronic materials, all of which are discarded after use. 3 For example, a single-use packaging and applicator from CGM can generate about 58 to 108 g of waste per sensor. 4 Insulin pumps and pens can also generate about 1.2 and 1.4 kg of plastic and electronic waste per month. 5 Although some materials may degrade under specific conditions, this process is typically slow and not designed to break down rapidly after disposal. Consequently, most of this waste persists in the environment unless it is appropriately recovered or recycled. 6 Recent literature has further highlighted the scale of this waste stream, with household-level studies showing that diabetes devices contribute meaningful amounts of plastic, battery and electronic waste, and reviews emphasizing that much of this material persists unless it is recovered or recycled. 5
Improper disposal of diabetes-related waste raises important safety concerns. Used insulin needles, lancets, and other sharps can expose family members, waste handlers, and the wider community to needlestick injuries and potential infection risk.7,8 Ideally, these materials should be discarded as hazardous health care waste, but in reality, disposal practices are often suboptimal, with reports of sharps being discarded in household rubbish, burned, and buried. 9 Disposal guidance also varies between countries and in many settings,10,11 these materials ultimately enter general waste streams rather than being handled as health care waste.12,13 Given the frequency with which PwD use sharps and blood glucose monitoring supplies, it is particularly relevant to evaluate disposal practices and disposal-related safety concerns in this group of individuals. Beyond these safety risks, diabetes-related waste also reflects a broader sustainability challenge: the routine use of high-volume, single-use medical products contribute not only to waste burdens but also to the wider material and carbon footprint of health care.
Climate change is one of the greatest threats to human health. The consequences of climate change are already felt across multiple domains, including disruptions in food production, reduced water availability and quality, biodiversity loss, and a growing strain on health care systems. 14 At the same time, the health care sector is itself a substantial contributor to this crisis, accounting for approximately 5% of global greenhouse gas emissions, thereby paradoxically contributing to the very environmental changes that threaten population health. 15 In this context, diabetes-related waste should be considered not only as a disposal and safety issue but also as part of the broader sustainability effort to reduce environmental and climate impacts of health care. Against this backdrop, our study aimed to evaluate a pilot study on the disposal practices for used insulin-related sharps and devices among PwD in Singapore, and to assess awareness, attitudes, and perceived responsibility regarding appropriate disposal and the environmental impact of diabetes care–related waste.
Method
Study Design
This pilot study was conducted as a cross-sectional survey was conducted at the National University Hospital and Ng Teng Fong General Hospital in Singapore from February 2025 to January 2026. The study was approved by the National Healthcare Group Domain Specific Ethics Review Board (reference number: 2024-4426). In Singapore, insulin pens and syringes, and capillary blood glucose monitoring remain more commonly used than CGM, partly because CGM uptake has historically been limited by lack of reimbursement, particularly in persons with type 2 diabetes. We examined disposal practices for used insulin-related sharps and devices among people with diabetes, including used insulin needles, insulin pens, and insulin pump consumables and assessed participants’ awareness, attitudes, and practices regarding appropriate disposal channels for used insulin pens and other diabetes-related devices.
Study Population
All adults with diabetes, gestational diabetes, or diabetes during pregnancy who use insulin needles, pens, or pumps were eligible to participate. Participants were approached by their physician. Participants who expressed interest were invited to complete a survey via a Quick Response code. Participants were encouraged to complete the survey while waiting for their doctor’s consultation in the appointment room, or after their consultation. The survey was developed in English and participants who were unable to understand or read English were excluded from the study.
Survey
The survey questionnaire (Supplemental Appendix 1) was developed based on similar surveys that were previously published.16-23 The survey collected information on participants’ demographics (age, gender, education level), duration of diabetes, duration of insulin use, type of insulin delivery device (syringe, pen device, or insulin pump), frequency of insulin needle changes, and disposal habits of insulin needles, pens, and lancets. Participants’ self-rated perceptions of responsibility for proper disposal and awareness of plastic waste associated with diabetes care devices were also assessed.
The survey consisted of multiple-choice, open-ended, and 5-point or 10-point Likert scale items. Questions on perceived responsibility for proper insulin needles/pen disposal were rated on a 5-point Likert scale, with “0” being strongly disagree and “4” representing strongly agree. The survey questions were hosted on FormSG, a secure Singapore government digital form platform designed for anonymized data collection. Responses were anonymized to reduce social desirability bias.
Statistical Analysis
Descriptive statistics were reported as numbers (percentages) for categorical variables and means ± standard deviations (SD) for continuous variables. Pearson’s correlation coefficient (rp) was used to assess associations between continuous variables measured on interval or ratio scales, while Spearman’s rank correlation coefficient (rs) was used for ordinal variables. For selected analyses, nominal variables were recoded into dichotomous categories for analyses (ie, “no advice received” vs “advice received from health care professionals). Logistic regression models were conducted for the following dependent variables: (1) practice safe disposal of sharps (“How do you dispose the lancets you use to check your blood sugar?” and “If you are disposing used insulin needles and syringes, what type of container do you use?”), (2) needlestick injury (“Have you ever accidentally pricked yourself or has anyone else been accidentally pricked by your insulin needles?”), (3) awareness of recycling (“I am aware that I could bring the insulin pens back to the hospital to be recycled”), and (4) practice of recycling (“I am aware that I could bring the insulin pens back to the hospital to be recycled and I do it all the time.”). Independent variables of these models were age, level of education, duration of diabetes, advice from health care providers, and frequency of insulin injection per day.
Results
Demographics and History of Diabetes
A total of 60 responses were collected between February 2025 and January 2026. The mean age of the survey responders was 46.0 ± 13.6 years and 34 (56.7%) were female. Fifty-two percent of the participants reported duration of diabetes of more than 10 years. Forty percent of the participants had attained a university education or higher. Among the participants, 23 (38.3%) had type 1 diabetes mellitus, 35 (58.3%) had type 2 diabetes mellitus, and 2 (3.3%) had gestational diabetes mellitus. Of the responses, 88.3% used insulin pen devices, 5 (8.3%) insulin syringes, and 2 participants (3.3%) used insulin pump. Of those who used insulin, the mean insulin injections per day was 3.0 ± 1.4 times (Table 1).
Represents the Baseline Demographics of the Survey Respondents.
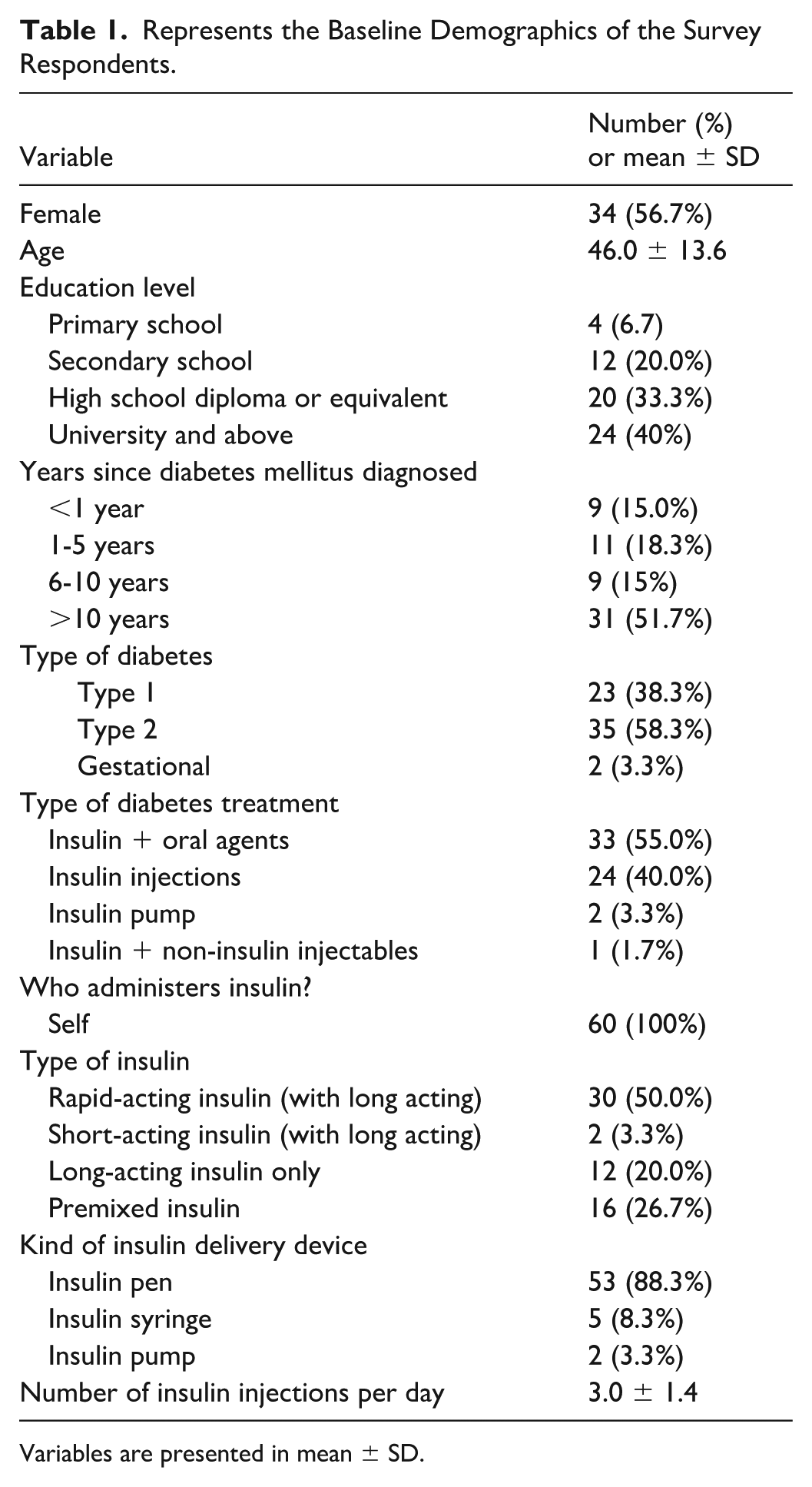
Variables are presented in mean ± SD.
Sharps Disposal Practices
Overall, 48 participants (76.7%) reported having received advice on the disposal of insulin needles. Of the cohort, 63.3% received advice on safe insulin needle disposal practices from diabetes nurse educators. For lancet disposal, 40% of participants used a non-designated container (eg, plastic water bottle), whereas only 6.7% used a designated sharps container. Notably, a quarter of participants discarded their lancets directly into the general rubbish bin without using a container. For used insulin needles and syringes, only 2 (out of 5) participants reported using a designated sharps container; approximately half (51.3%) reported using any plastic bottles; 4 (6.7%) used metal containers; and 12 (20%) used plastic bags or discarded the items directly into the general waste bins. Ten participants (16.7%) reported having accidentally pricked themselves or another person with used sharps. Forty-five percent of the participants were able to find information online regarding safe disposal of insulin needles, while the remaining either reported not being able to find such information or had never tried to look for it (Table 2).
Responses to the Survey Question.
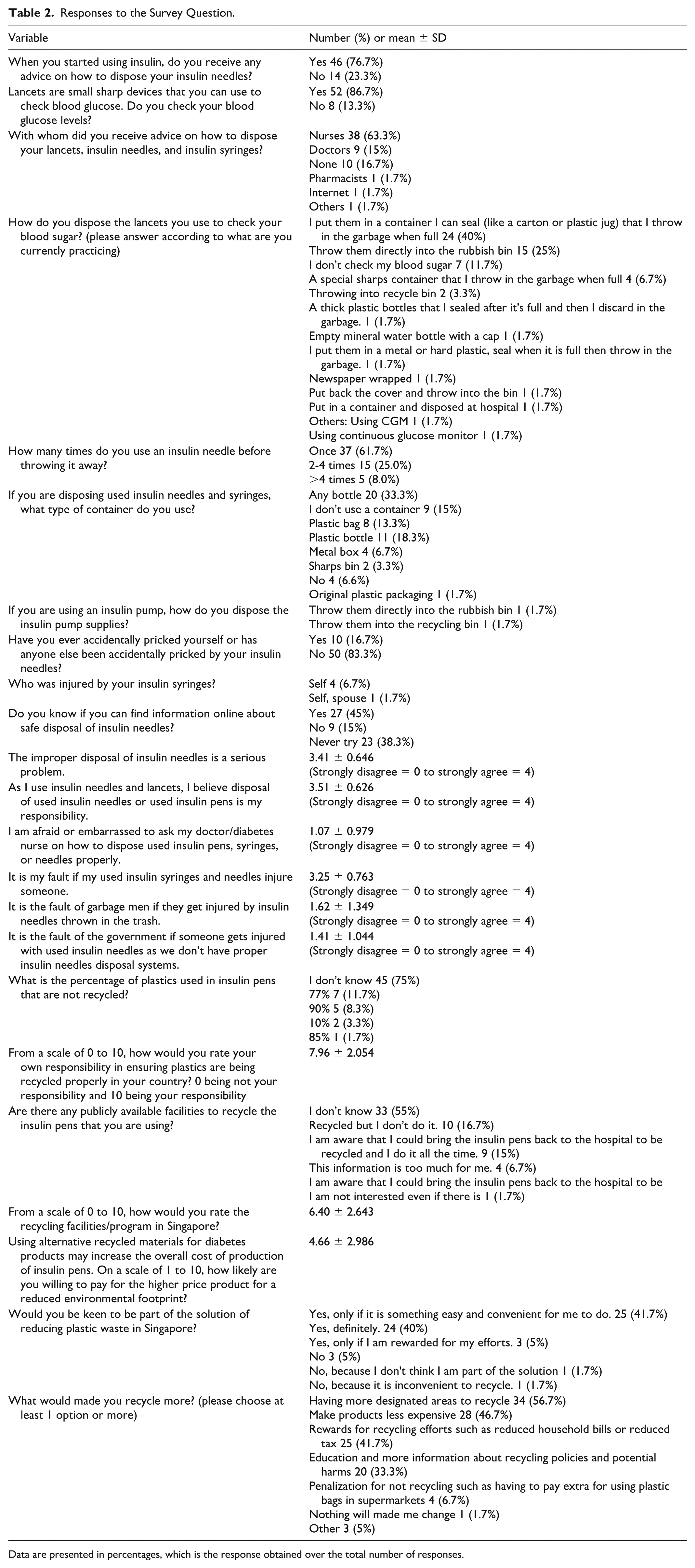
Data are presented in percentages, which is the response obtained over the total number of responses.
Perceived Responsibility for Proper Disposal
Responders generally agreed that improper disposal of insulin needles is a serious problem, and the average Likert scale reported a mean score of 3.4 ± 0.65. Participants also reported that proper disposal of used insulin needles or pens is their responsibility (mean score = 3.5 ± 0.63), and that they would be at fault if the used insulin needles or syringes caused injury to another person (mean score = 3.3 ± 0.76).
By contrast, mean scores for statements attributing blame to waste collection workers (1.6 ± 1.35) or the government (1.4 ± 1.04) were in the disagree-to-uncertain range, indicating that participants were less likely to assign responsibility to external parties. Participants also generally disagreed that they felt afraid or embarrassed to ask their doctor or diabetes nurse about appropriate disposal methods, suggesting that reluctance to seek professional advice was not a major barrier (Table 2).
Awareness of Plastic Waste
Three-quarters of participants were unaware what proportion of plastic in insulin pens is not recycled. Participants reported a strong sense of personal responsibility for ensuring that plastics are recycled (mean score 8.0 ± 2.05 out of a 10-point Likert scale). However, 55% of respondents were unaware of any publicly available facilities for recycling insulin pens.
Participants were also asked to rate the adequacy and accessibility of existing facilities or programs for diabetes-related plastic waste on a scale of 0 to 10, where higher scores reflected more favorable perceptions. The mean rating was 6.4 ± 2.64 out of 10, suggesting that participants perceived current recycling options as only moderately adequate and accessible. Participants were asked whether they would be willing to pay a higher price for diabetes products made from recycled materials. Participants’ willingness to pay a higher price for insulin-related products was modestly low (rated 4.7 ± 2.99 out of 10). Nonetheless, most participants (86.7%) indicated that they were willing to participate in efforts to reduce plastic waste, particularly if the required action was simple and convenient (41.7%). In addition, participants were asked which measures would be most likely to encourage them to recycle insulin-related plastic waste. The most selected measures were the provision of more designated recycling points (56.7%), lower product cost (46.7%), incentives for recycling, such as reduced household utility bills or tax rebates (41.7%), and more education and information on recycling policies and the environmental harms of plastic waste (33.3%) (Table 2).
Correlations
Older age was associated with lower educational attainment (rs = −0.48, P < .001), longer diabetes duration (rs = 0.38, P = .003), and fewer injections per day (rp = −0.33, P = .011). However, age was not associated with participants’ self-rated sharps disposal practices or participants’ perceived responsibility or awareness of plastic waste. A higher level of education was associated with a shorter duration of diabetes (rs = −0.41, P = .001). Similarly, PwD with higher education level were less likely to agree that the government should be blamed if someone were injured by a used insulin needle (rs = −0.29, P = .027).
No significant associations were observed between diabetes duration, insulin injection frequency, insulin delivery device type, or lancet use frequency and outcomes related to disposal practices, perceived responsibility, or plastic waste awareness. Participants who had not received disposal advice from health care professionals were less likely to perceive safe disposal of insulin devices as important (rp = −0.29, P = .028) and more likely to report embarrassment or reluctance in asking health care professionals for advice (rp = 0.44, P = .001). Participants who perceived improper insulin needle disposal as a serious issue were more likely to endorse personal responsibility for proper disposal (rp = 0.63, P < .001) and personal fault if injury occurred (rp = 0.27, P = .047). Conversely, participants who gave lower ratings to recycling facilities and programs in Singapore were more likely to require incentives for recycling (rp = 0.35, P = .009) and to indicate that nothing will made me change (rp = 0.28, P = .038).
Logistic Regression Models
Participants who received advice from health care providers on how to dispose lancet, insulin needles, and insulin syringes were nearly 20 times (P = .002) the odds to practice safe disposal of sharps, independent of age, level of education, duration of diabetes, and frequency of insulin injection per day. However, all these factors did not associate with needlestick injury, awareness of recycling, and practice of recycling (Table 3).
Logistic Regression Models.
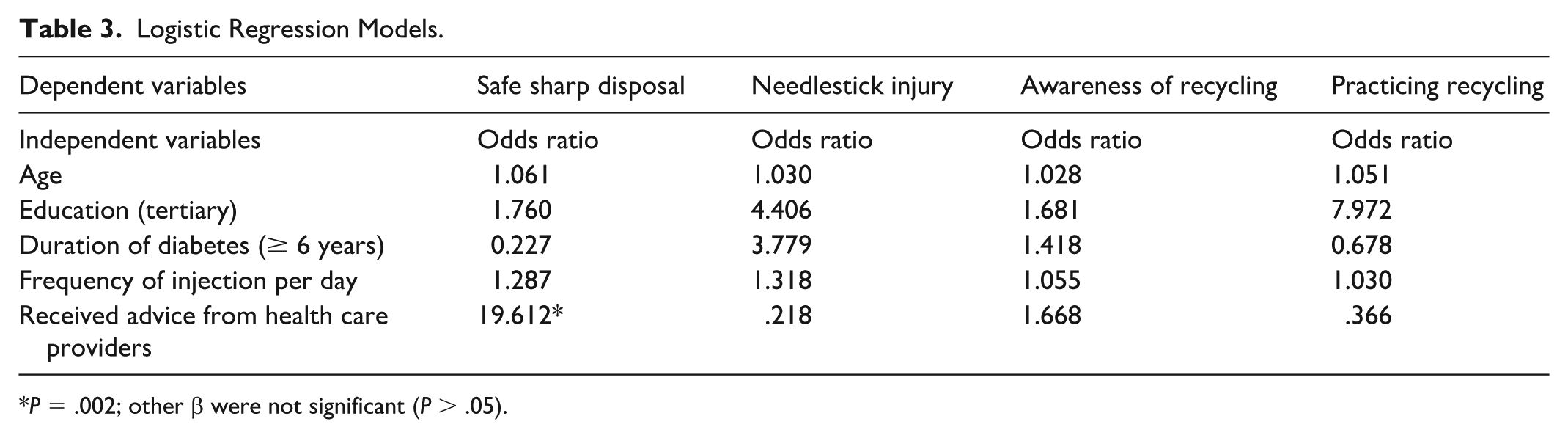
P = .002; other β were not significant (P > .05).
Subgroup Analyses
Subgroup analyses were conducted to compare participants with type 1 and type 2 diabetes mellitus. Participants with type 1 diabetes were younger (38.7 ± 12.4 vs 51.5 ± 11.9 years, P < .001) and more likely to have attained university-level education than those with type 2 diabetes (14 [61%] vs 9 [26%], P = .007). Participants with type 1 diabetes were also more likely to be using a basal-bolus insulin regimen, defined as long-acting insulin combined with rapid-/short-acting insulin, compared with people with type 2 diabetes (21 [91%] vs 9 [26%], P < .0001). In keeping with this, participants with type 1 diabetes reported a higher mean number of insulin injections per day than those with type 2 diabetes (3.74 ± 1.42 vs 2.43 ± 1.12 injections/day, P < .001). There were no significant differences between the 2 groups in gender distribution or type of insulin delivery device used.
Despite these differences in baseline characteristics and insulin treatment patterns, there were no significant differences between participants with type 1 and type 2 diabetes across the variables presented in Table 2, including sharps disposal practices, perceived responsibility for proper disposal, and awareness of plastic waste (all P > .05). Type of diabetes, dichotomized as type 1 versus type 2 diabetes, was also included as a covariate in the logistic regression models presented in Table 3. Diabetes type was not significantly associated with any of the outcomes assessed in the models (all P > .05).
Discussion
This cross-sectional study examines how PwD dispose of diabetes-related devices and how they view responsibility for the disposal of these devices and the associated device-related plastic waste. Several important findings emerged. Most participants recognized improper sharps disposal as a safety risk and took responsibility for proper disposal. However, reported disposal practices remained suboptimal. Only 6.7% used designated sharps containers, while many relied on improvised containers such as plastic bottles. A significant proportion of respondents discarded sharps directly in household waste despite receiving information on safe disposal. In addition, knowledge of the environmental burden associated with diabetes devices and publicly available facilities for recycling insulin pens is low. Overall, our study suggests a gap between awareness, intention, and real-world disposal behavior.
Our results are consistent with previously reported findings. An exploratory study in Malaysia found that a quarter of participants discarded sharps in a rubbish bin without a special container, and less than a fifth had knowledge of sharp disposal. 17 In a systematic review by Wu et al 24 on the waste disposal of sharps outside medical institutions, the authors concluded that knowledge of sharps waste disposal is low among PwD. The majority of PwD also had no formal training in safe disposal methods. Incorrect waste handling, such as throwing sharps into the street, toilet pits, or household dumps, has been reported, potentially leading to needle stick injuries.25,26 A 2022 cross-sectional study of disposal practices of used insulin needles at home in China reported only 10.3% of participants disposed of insulin needles safely, and only 14.8% had previously received instruction on sharps disposal. 18 Likewise, a US survey examining sharps handling and disposal found that one-third of insulin-using respondents disposed of lancets or insulin needles unsafely, most commonly in household trash. 27 Our study findings align with the broader literature, showing that unsafe disposal of medical devices is a common problem among PwD.
Our study also shows that PwD who had not received disposal advice from health care professionals were less likely to perceive safe disposal as important and more reluctant to ask for advice. This is concordant with a published study showing that prior instructions on sharps disposal were independently associated with safer disposal practices, with an adjusted odds ratio of 6.31. 26 Patient education can thus shape risk perception, confidence, and disposal behavior. Structured nurse-led counseling may be a practical avenue for intervention.
Participants also demonstrated a strong sense of personal responsibility for proper disposal, but this did not consistently translate into safe sharps disposal practices. In our survey, participants generally agreed that improper disposal is a serious problem and that they would feel responsible if injury occurred, yet few used dedicated sharps containers, and 16.7% of participants reported needlestick injury to themselves or others. This suggests that awareness and intention may not be sufficient when facilities are limited or disposal advice is unclear. Prior studies have similarly noted that even when people use puncture-resistant containers, they may still ultimately place them in household rubbish because community collection systems are limited or unclear. 18
For every ton of plastic waste from insulin pen recycled, 316.5 kg of carbon emissions would be reduced. 28 Although most participants expressed willingness to be involved in efforts to reduce plastic waste, their knowledge of the environmental footprint of diabetes technology was limited. Our study showed that most participants were unaware of the environmental impacts of diabetes technology (eg, many participants were unaware that insulin pens are largely not recycled, and more than half were unaware of publicly available recycling options). 28 In our hospital in Singapore, a recycling bin designated for insulin pen disposal is available in the waiting area 28 but is often underused. This may reflect limited awareness, inconvenience, or uncertainty about how and where such devices should be recycled. In addition, participants appeared sensitive to higher cost, with relatively low willingness to pay more for diabetes products made from recycled materials. This suggests that while users may support environmentally sustainable practices in principle, they may be less accepting of strategies that increase the out-of-pocket cost of insulin pens, including those where recycling costs are incorporated into the product pricing. These findings suggest that interventions should not focus solely on individual motivation but also on system-level factors such as improving recycling infrastructure, increasing public awareness of available recycling facilities, providing clear guidance on disposal versus recycling pathways, and improving the affordability and accessibility of more sustainable diabetes-care products.
This study has limitations. As a pilot study, the sample size was modest, and recruitment was conducted at 2 hospitals, which may limit the generalizability of the findings to other health care settings and practices. The survey was administered in English, which may have introduced selection bias and limited applicability to the broader diabetes population. Participant responses to the statement that “the improper disposal of insulin needles is a serious problem” should be interpreted with caution, as the perceived meaning of “serious problem” may have varied between individuals. In addition, this was a semi-quantitative study, and no thematic analysis was undertaken; therefore, the findings should be interpreted as preliminary and descriptive rather than as an in-depth qualitative exploration. The reliance on self-reported practices and attitudes may have also introduced recall bias and social desirability bias, although anonymity was used to reduce the latter. Administering the survey only in English may have introduced selection bias and limited the generalizability of the findings in Singapore’s multilingual context. According to the 2020 Census, 82.7% of Singapore residents aged 15 years and above were literate in English, while 74.3% of literate residents were literate in 2 or more languages. 29 Although these figures indicate high levels of English and multi-language literacy nationally, an English-only survey may still have excluded individuals with limited English proficiency or lower confidence in completing health-related questionnaires in English. This may have resulted in under-representation of certain demographic groups, particularly older adults, individuals with lower educational attainment, and those more comfortable communicating in Mandarin, Malay, Tamil, or other languages. As such, the respondent profile and reported practices may not fully reflect the broader diabetes population in Singapore. Future studies should consider multilingual survey administration to improve inclusivity and representativeness. Nevertheless, the survey is timely and addresses several public health priorities, including disposal practices, attitudes, and environmental awareness. The findings provide useful preliminary evidence to inform larger multi-center studies and future intervention design.
Conclusions
This survey suggests that although adults using insulin-related devices in Singapore generally recognize the importance of proper sharps disposal and are willing to reduce device-related plastic waste, disposal practices remain suboptimal, and awareness of recycling pathways is limited. Education from health care professionals appears to be an important modifiable factor. The availability of disposal infrastructure and clearer public guidance are enablers for improving safety and reducing environmental harm from insulin-related sharps.
Supplemental Material
sj-docx-1-dst-10.1177_19322968261461561 – Supplemental material for A Pilot Study on Disposal Practices and Environmental Awareness of Insulin-Related Devices Among People With Diabetes
Supplemental material, sj-docx-1-dst-10.1177_19322968261461561 for A Pilot Study on Disposal Practices and Environmental Awareness of Insulin-Related Devices Among People With Diabetes by Lawrence Siu-Chun Law, Rhea Chatterjea, Chin Meng Khoo, Shih Ling Kao and Pei Chia Eng in Journal of Diabetes Science and Technology
Footnotes
Abbreviations
CGM, continuous glucose monitoring; PwD, people with diabetes; rp, Pearson’s correlation coefficient; rs, Spearman’s rank correlation coefficient; SD, standard deviation.
Author Contributions
Conceptualization: PCE, SLK. Data curation: LS-CL. Writing of original draft: PCE, LS-CL. Analysis of study: LS-CL. Review and editing; all authors.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.