
Abstract
Narrowing of the uterine spiral arterioles below the deciduomyometrial junction is 1 of the key pathophysiological changes in women with preeclampsia. The contribution of pelvic autonomic nerves to decidualization and impaired placentation in preeclampsia is not clear. Placental bed biopsies were obtained from 10 women with preeclampsia and 23 nornotensive women at Caesarean section. We stained them with anti-S100 and CD34 antibodies to detect the presence of nerve fibers and blood vessels, respectively. We detected S100-immunoactive nerve fibers in the myometrium but not in the decidua in both groups of women. S100-immunoactive nerve fiber density in the placental bed myometrium was significantly increased in women with preeclampsia compared to normotensive women. There was no clear relationship between the densities of nerve fibers and CD34-positive blood vessels in these biopsies. These results suggest increased nerve fibers in the placental bed myometrium may play a role in the pathogenesis of the preeclampsia.
Introduction
Preeclampsia is a pregnancy-specific disease characterized by hypertension and proteinuria. It occurs in 5% to 8% of all pregnancies and results in significant maternal and neonatal morbidity and mortality. 1–3 It is widely accepted that deficient trophoblast invasion of the spiral arteries leading to inadequate blood supply to the fetus is the central pathological feature. 4,5 Impaired remodeling of the uterine spiral arteries during the second wave of trophoblast invasion appears to be pivotal in the pathogenesis of the condition. 3
Remodeling of the spiral arteries is a complex process determined by the interaction of many factors between decidua and junctional zone myometrium. 3–6 Impaired remodeling of spiral arteries may result from an imbalance of angiogenic factors causing preeclampsia. 1 High circulating levels of antiangiogenic factors such as soluble Fms-like tyrosine kinase 1 (sFlt1), soluble endoglin (sEng), neurokinin B, and low circulating levels of angiogenic factors including placental growth factor (PlGF), and vascular endothelial growth factor (VEGF) are risk predictors of preeclampsia. 4,6,7
Angiogenesis and neurogenesis share common mechanisms in following specific paths to their respective targets. 8 Many angiogenic factors (eg, VEGF) have both neurogenic activity and angiogenic effects, whereas many neurogenic factors, such as neuropilin 1 and nerve growth factor (NGF), contribute to angiogenesis. 9–17 Recently, NGF, a neurotrophin that plays an important role in promoting neurotrophic and neurotropic effects in sympathetic neurons has been considered an angiogenic factor and found to correlate with microvascular density. 14,18 In women with preeclampsia, plasma concentrations of NGF are significantly reduced compared with normotensive women, suggesting that both angiogenesis and neurogenesis may be decreased in the placental bed myometrium in women with preeclampsia. 19,20
In late pregnancy, there are relatively few nerve fibers in myometrium; there is little or no information in early pregnancy. 21–23 Prepregnancy injuries to uterine nerves result from common problems including persistent straining during defecation that gives rise to neural proliferation with production of large volumes of many different cytokines. 24 Continuing defecatory problems in early pregnancy may contribute new injuries, continuing cytokine production, and interference with decidualization. 25 We propose that focal loss of nerve fibers below the endometrial-myometrial interface may prevent appropriate decidualization and placentation, resulting in the characteristic vascular changes in the spiral arteries over varying degrees of the placental bed.
Patients and Methods
This study included 23 healthy normotensive pregnant women as controls and 10 women with preeclampsia at Women’s Hospital between June 2010 and October 2010. All were delivered by Cesarean section without labor. Patient characteristics are given in Table 1. Preeclampsia was defined by (a) systolic blood pressure of more than 140 mm Hg and diastolic blood pressure of more than 90 mm Hg after 20 weeks’ of gestation in a previously normotensive patient; (b) new onset proteinuria (>300 mg of protein in a 24-hour urine collection or 1 dipstick or greater than 2 occasions at least 4 hours apart); and (c) resolution of hypertension and proteinuria by 12 weeks postpartum. Patients with baseline hypertension, proteinuria, or renal disease were excluded. The Human Ethics Committees of the Women’s Hospital, Zhejiang University School of Medicine approved this study, and all pregnant women gave their informed consent for participation.
Participant Demographics and S100-Positive Nerve Fibers and CD34-Positive Vessels in the Placental Bed

a Median (range).
b Percentage = Pregnant women with S100 or CD34-positive staining/total pregnant women.
c Mean (±SD).
Immunohistochemistry
A biopsy (0.5 × 1.0 × 1.0 cm 3 ) including consecutive decidual and myometrial tissues was taken from the placental bed within 10 minutes of delivery. We fixed the biopsy in buffered formalin and processed it for routine hematoxylin and eosin staining. Microscopic examination confirmed placental bed tissue before staining for nerves and vessels. Immunohistochemical staining with anti-S100 protein and anti-CD34 was performed to determine the presence of nerves and vessels in the decidua and myometrium, respectively. 26 Briefly, after retrieving the antigen for S100 and CD34, we stained serial, 4μ thickness sections, with polyclonal rabbit anti-S100 antibody (dilution 1:2000, Z031129; Dako Cytomation, Denmark) and the monoclonal mouse CD34 antibody (dilution 1:500, QBEnd10; Dako Cytomation) for 60 minutes at room temperature. We washed the sections in phosphate-buffered saline (PBS) and incubated with Envision-labeled polymer-alkaline phosphatase mouse/rabbit (EnVisiont/HRP/Mo, GK400105; EnVisiont/HRP/Rb, GK400305/15; Novocastra, UK) for 60 minutes. We visualized the antigen–antibody reaction using diaminobenzidine as chromogen (DAB, GK346810; Novocastra). After washing, we counterstained the sections with Mayer’s hematoxylin, then dehydrated and mounted them. Normal vulval skin was used as a positive control, and PBS was used as a negative control. Concentrations were matched with the concentrations of the S100 antibody and CD34, respectively. An experienced gynecological pathologist at the department of pathology in Women’s Hospital, Zhejiang University School of Medicine, evaluated the slides. If there were no immunoactive, nerve fibers, or vessels appeared on the slides, we defined them as a negative case, otherwise we designated them as a positive case and counted the percentage (positive cases/total cases) and positive nerve fibers or vessels.
Quantification of Nerve Fiber and Microvascular Density
We used the technique of microvascular density quantification 26,27 to count the number of nerve fibers and vessels identified by S100 and CD34 staining in the decidua and myometrium, respectively. Briefly, following immunostaining, we scanned the entire section including the decidua and myometrium at low power (100×) to identify “hot spots” (a hot spot = 1 × 1 mm 2 ), which represent the highest areas of the distribution of nerve fibers and vessels. We counted individual nerve fibers and vessels under high power (400×) to obtain a nerve or a vessel count in a defined area. We calculated the average nerve or vessel count in 5 hot spots. The results were expressed as the mean (± standard deviation [SD]) number of nerve fibers per mm2 or vessels per mm2 in each specimen from all the decidual and myometrial samples. A single observer who was blinded to the sample background counted the number of S100-positive nerve fibers and CD34-positive vessels.
Statistical Analysis
We used the Statistical Package for the Social Sciences Version 13.0 to perform statistical analyses. The t test was used to compare the differences in the density of CD34 immunostaining vessels in the decidua and myometrium between groups because the measured values of the variables were normally distributed. The Mann-Whitney U test was used to compare the differences in the density of S100-immunoactive nerve fibers in the decidua and myometrium between groups since the measured values of the variables were not normally distributed. The χ2 test was used to compare the differences in the percentage of S100-positive nerve fibers in the decidua and myometrium between groups. The Pearson’s correlation test was used to compare the correlation between the density of CD34-positive vessels and S100-positive nerve fibers in the decidua and myometrium in either group. Differences were considered significant at P < .05.
Results
There were no statistical differences between pregnant women with and without preeclampsia regarding their age, gravid, abortion, gestation age, Apgar score, or birth weight (Table 1). Anti-S100 immunoreactive nerve fibers were detected in the placental bed myometrium but not in the decidua in all the study participants (Figure 1A and B). We found abnormal nerve fibers stained with S100 near blood vessels in the placental bed myometrium in women with preeclampsia (Figure 1A). The percentage of S100-immunoreactive nerve fibers was 80% (8 of 10) in women with preeclampsia, and 26.1% (6 of 23) in women without preeclampsia (Table 1). The percentage of S100-immunoreactive nerve fibers in the placental bed myometrium was significantly higher in women with preeclampsia compared to normotensive women (χ2 = 8.294, P = .004). The median (range) density of S100-immunoreactive nerve fibers in the placental bed myometrium was 0.70 (0-4.25)/mm2 in women with preeclampsia, and 0 (0-1.25)/mm2 in women without preeclampsia (Table 1). There was a significant difference in S100-immunoreactive nerve fiber density in the placental bed myometrium between women with and without preeclamsia (Z = 2.747, P = .006).
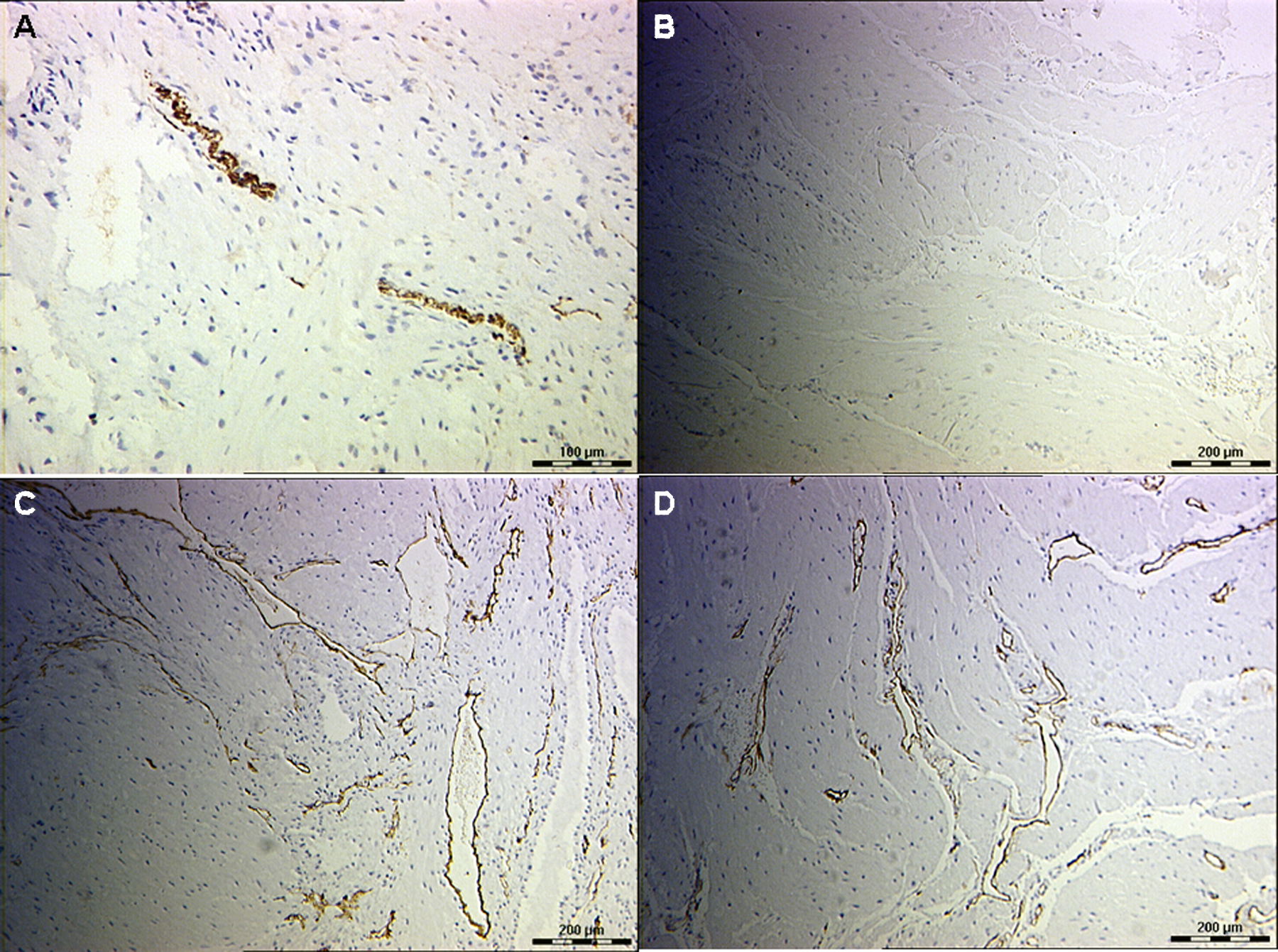
S100-immunostaining nerve fibers and CD34-immunostaining vessels in the placental bed decidua and myometrium in women with and without preeclampsia. (A) Placental bed decidua and myometrium from a women with preeclampsia stained for S100 (original magnification, ×200). Some large nerve fibers and abnormal nerve fibers in the placental bed myometrium could be identified. (B) Placental bed decidua and myometrium from a women without preeclampsia stained for S100 (original magnification, ×200). No nerve fibers could be identified. (C) Placental bed decidua and myometrium from a women with preeclampsia stained for CD34 (original magnification, ×200). More blood vessels stained with CD34 in the placental bed decidua and myometrium could be identified. (D) Placental bed decidua and myometrium from a women without preeclampsia stained for CD34 (original magnification, ×200). More blood vessels stained with CD34 in the placental bed decidua and myometrium could be identified. Scale bars represent 100 μm in (A); 200 μm in (B), (C), and (D).
CD34-immunoreactive vessels could be detected in the decidua and myometrium in all the study participants (Figure 1C and D and Table 1). The mean (±SD) microvascular densities stained with CD34 in the decidua and the myometrium of the placental bed were 13.98 ± 3.41/mm2 and 27.85 ± 6.79/mm2 in women with preeclampsia, and 7.34 ± 1.91/mm2 and 14.64 ± 3.70/mm2 in normotensive women, respectively (Table 1). The density of CD34-immunoreactive vessels in the decidua and the myometrium of the placental bed was significantly higher in women with preeclampsia than in women without preeclampsia (t = 5.762, 5.789; P = .000, .000). There was no relationship between CD34-immunoreactive vessels and S100-immunoreactive nerve fibers in the placental bed myometrium in women with or without preeclampsia (r = .095, .302; P = .667, .397).
Discussion
We found that nerve fibers stained with S100 and vessels stained with CD34 in the placental bed myometrium were both increased in preeclampsia. These nerve fibers often demonstrated abnormal morphological appearances typical of regenerating nerve fibers. There was no pattern to the geographical distribution of these nerve fibers within the myometrium, raising the question as to their significance. Specifically, we did not find them in close relationship to the deciduomyometrial junction where we would expect to find narrowing of the spiral arterioles or in close apposition to abnormal spiral arterioles. Given that there is relative denervation of the myometrium in later pregnancy, 21 it is possible that these neural injuries exert their effects in early pregnancy during decidualization and placentation before myometrial hyperplasia and hypertrophy takes place. Prepregnancy injuries to uterine nerves are known to follow straining during defecation, 24 with aberrant reinnervation contributing to chronic pelvic pain, dysmenorrhea, and endometriosis. 25,28,29
Our results also showed an increased density of small vessels in the decidua and the placental bed myometrium in women with preeclampsia compared to normotensive women. Abnormal vascular changes in the uterine spiral arteries may cause impaired remodeling of the spiral artery, leading to preeclampsia. 1–5 However, neurogenic factors have been shown to be required for angiogenesis in tissue damage repair, whereas neurogenesis is in need of angiogenic factors in wound healing, tissue scar, and organ ontogeny. 30–33 A recent study has confirmed that decreased plasma NGF concentrations are negatively correlated with blood pressure in women with preeclampsia. 19 Nerve growth factor is a neurotrophin that stimulates neurite outgrowth in the peripheral and central nervous and modulates differentiation and survival of peripheral neurons. 18 Abnormal expression of NGF in neuronal cells and nonneuronal cells has been shown to affect peripheral nerve development. 34
Khong et al 20 showed an abundance of nerves in the deeper layers of the myometrium with some accompanying vessels to the deciduomyometrial junction in preeclampsia. There were no nerves in the decidua or accompanying spiral arterioles. The authors concluded that nonneurogenic mechanisms may be important in uterine blood flow though they did not specify that they had identified pathological areas associated with narrowing of the spiral arterioles. Many of the biopsies were obtained by curettage in that series. In this study, we used modified biopsy forceps to obtain a biopsy thickness of 10 mm from the uterine surface to ensure a full layer of the placental bed myometrium. It has been suggested that preservation of nerve fibers near or around the uterine spiral arteries would allow for vasomotor modulation of these vessels through neural pathways during pregnancy. 20 The denervation of autonomic neural supply would lead to uterine reinnervation (abnormal nerve fibers). 25
In summary, these preliminary results show that nerve fibers stained with S100 and vessels stained with CD34 in the placental bed myometrium were both increased in women with preeclampsia compared to women without preeclampsia. Further studies of uterine innervation during early pregnancy, targetting areas of narrowed spiral arterioles, may be productive in defining the role of prepregnancy neural injuries in the pathogenesis of reproductive loss.
Footnotes
Acknowledgments
The authors are grateful to Dr MJ Quinn (London, UK) for assisting with the editing of this manuscript.
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The authors received no financial support for the research, authorship, and/or publication of this article.