
Abstract
The purpose of this study was to explore the effects of cumulus cells on vitreous cryopreservation of human mature oocytes and clinical pregnancy outcomes. The study was divided into group A (cumulus cells were removed from the oocytes before freezing) containing 24 participants and 193 oocytes and group B (cumulus cells were retained with the oocytes before freezing) containing 26 participants and 240 oocytes. Based on no significant differences in age, duration of infertility, infertile causes, and number of retrieved oocytes between both groups when oocytes were retrieved from infertile women, we found that the survival rate of post thaw oocytes (88% vs 58%), cleavage rate (80% vs 56%), and high-quality embryo rate (75% vs 59%) were significantly higher in group B than in group A. Under the conditions that there were no significant differences between the 2 groups in the general status of the participants undergoing embryo transfer, the embryo implantation rate (37% vs 15%) and the clinical pregnancy rate (50% vs 17%) were significantly higher in group B than in group A, all with Ps < .05. We conclude that the retention of cumulus cells can improve the developmental competence of vitrified–thawed human mature oocytes and clinical pregnancy outcomes.
Introduction
With the development of assisted reproductive technology such as in vitro fertilization–embryo transfer (IVF-ET), cryopresrvation technique becomes more and more important. Oocyte cryopreservation has been a focus in reproductive research because it can avoid many ethical problems. Oocyte is the largest cell with complex structures in human body. Freezing readily causes irreversible lesion of oocytes, and even death, so human egg bank has not been established to this day. In recent years, with the development of vitreous cryopreservation, the survival rate and fertility rate of vitrified–thawed oocytes have been greatly increased, but the embryo implantation rate and clinical pregnancy rate have not been improved.1,2 This may be that cryopreservation easily causes damage on cytoskeletal structures such as spindle, 3 ,4 while cytoskeletal structures are closely related to the developmental potentiality of embryos. Cumulus cells, granular cells, which surround oocytes, provide nutrient substance for and transmit signals to oocytes. Cumulus cells play an important role in oocyte maturation and development in vitro. However, there have been different conclusions about whether cumulus cells can improve the survival rate and developmental competence of frozen–thawed oocytes. 5 -7 It has been found that the survival rate is higher in vitrified–thawed human germinal vesicle-denuded oocyte (GV-DO) than germinal vesicle-cumulus oocyte complex (GV-COC),7 suggesting that cumulus cells may limit the degree and speed of dehydration. However, Imoedehme and Sigue 8 have reported that the survival rate is significantly higher in frozen–thawed oocytes with cumulus than in frozen–thawed cumulus cell-free oocytes. Cytoskeleton is necessary for normal development of oocytes. Little research has been done on the role of cumulus cells in oocyte cryopreservation. In this study, to provide theoretical basis for clinical cryopreservation of oocytes, the effects of cumulus cells on embryo development and clinical pregnancy outcomes of vitrified–thawed human mature oocytes were retrospectively analyzed.
Materials and Methods
All study methods were approved by the Ethics Committee of the First Affiliated Hospital of Zhengzhou University. All the participants enrolled into the study gave written formal consent to participate.
Participants
Between October 2007 and April 2010, 50 infertile women undergoing IVF-ET of vitrified–thawed oocytes in our reproductive medical center were enrolled in this study. The inclusion criteria were (1) age 35 years or younger, (2) no polycystic ovarian syndrome, (3) no history of hereditary or familial disease, (4) with normal chromosomes, (5) couple without communicable disease. Among the 50 participants, all oocytes from 17 participants were cryopreserved with vitrification technology because epididymal and testicular sperm aspiration failed and there were no donor sperms on the day of oocyte retrieval; after oocytes were retrieved from the other 33 participants (>20 per participant), partial oocytes underwent vitreous cryopreservation following informed consent of patients. Eighteen participants underwent IVF-ET of own vitrified–thawed oocytes, 17 participants underwent IVF-ET of donor sperms and vitrified–thawed oocytes, and 15 participants underwent IVF-ET of donor vitrified–thawed oocytes. The donors received reexamination 6 months after oocyte freezing to know whether human immunodeficiency virus (HIV) is negative and blood type is the same as that of recipients. The donors and recipients signed informed consents in a double-blind manner, and all methods were approved by the Ethics Committee of our hospital. The study was divided into group A (cumulus cells were removed from the oocytes before freezing) containing 24 participants and 193 oocytes and group B (cumulus cells were retained with the oocytes before freezing) containing 26 participants and 240 oocytes.
Controlled Ovarian Hyperstimulation and Oocyte Collection
Downregulation by a long gonadotrophin-releasing hormone agonist (GnRH-α, commodity name: triptorelin) protocol was adopted in these patients. After attaining the standards of downregulation, gonadotrophin therapy began until the time of human chorionic gonadotropin (HCG) administration. Oocytes were collected by transvaginal ultrasound-guided puncture 36 hours later. 9
Treatment of Oocytes Before Freezing
In group A, oocytes were treated with hyaluronidase to remove large mucous mass followed by soft blow with a fine-drawn Pasteur pipette to thoroughly get rid of the cumulus cells surrounding oocytes. In group B, the same was done to treat large mucous mass as that in Group A, but the cumulus cells were retained.
Freezing and Thawing of Mature Oocytes
According to the instruction manual of vitrifaction reagent (purchased from MediCult, Denmark), oocytes were first placed in a mixture of 7.5% ethylene glycol and 7.5% dimethyl sulfoxide (DMSO) for 5 minutes at room temperature. After the treatment the oocytes became round, then shrunk, and then again became round in shape, and the oocytes were transferred into a mixture containing 15% ethylene glycol, 15% DMSO, and 0.5 mol/L sucrose, and swiftly loaded in the cryotop with a Pasteur pipette, with <3 oocytes in each cryotop and then were immediately immersed into liquid nitrogen for <1 minute. After thawing, the oocytes were placed in 1.0 mol/L sucrose solution at 37°C, then quickly transferred into 0.5 mol/L sucrose for 3 minutes at room temperature, followed by placement into the following solutions in order including 0.25 mol/L sucrose for 3 minutes, 20% human serum albumin + phosphate-buffered saline (PBS) for 3 minutes and then transferred to 20% human serum albumin + PBS for 3 minutes at 37°C, finally, into equilibrized culture solution. The survival criteria of vitrified–thawed oocytes include good refraction, transparency, no marked cytoplasmic shrinkage, intact zona pellucida, and cell membrane. 10
Endometrial Preparation
Endometrial preparation was performed according to the routine estrogen-progestational hormone (E-P) cycle of our reproduction center. 11
In Vitro Fertilization–Embryo Transfer
The thawed survived oocytes were cultured for 3 hours and then subject to intracytoplasmic sperm injection (ICSI). Fertilization was observed 16 to 18 hours after injection, and the cleavage and embryo development were observed following culture in the cleavage medium for 24 hours. One to three high-quality embryos were selected for embryo transfer on the second or third day of post fertilization. If there were sufficient high-quality embryos, 2 embryos were transferred in the participants younger than 35-year-old, and 3 in the participants with more than or equal to 2 transferred cycles. All embryos were incubated with the assistance of lasers. It was defined as clinical pregnancy when gestational sac was seen under B ultrasonography 35 days after embryo transfer. Luteal support lasted until 12-week gestation.
Statistical Analysis
SPSS 11.0 package (SPSS Inc, Chicago, Illinois) was used for statistical analysis. Differences in the continuous variables between the 2 groups were compared using the independent sample t test (Student t test) and variables were expressed as χ ± s. The chi-square test and Fisher exact probability test were used to analyze the numeration data. Statistical significance was established at P < .05.
Results
General Status of Participants in the 2 Groups When Oocytes Were Retrieved From Infertile Women
There were no significant differences in age, duration of infertility, infertile causes, and number of retrieved oocytes between both groups, all with Ps > .05 (Table 1).
General Status of Participants in the 2 Groups a
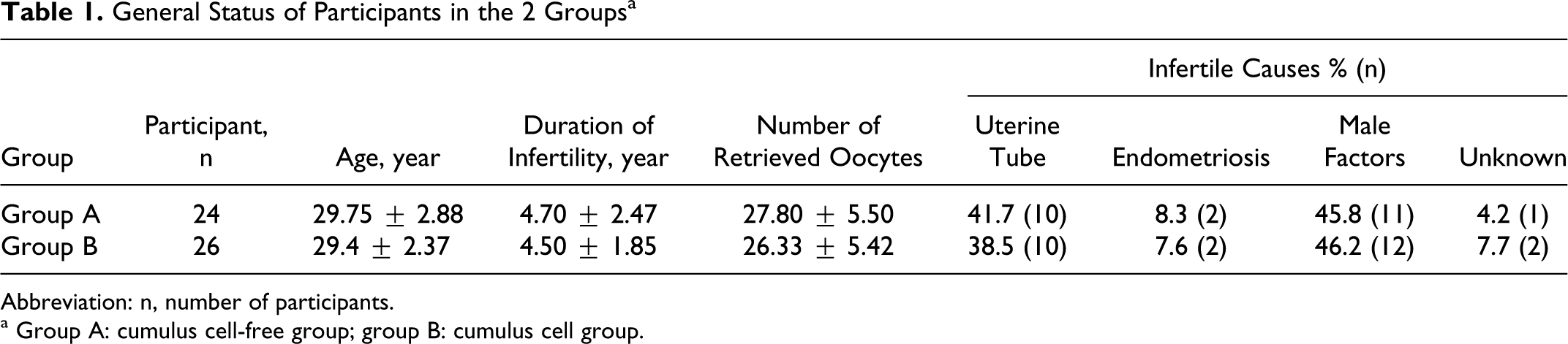
Abbreviation: n, number of participants.
a Group A: cumulus cell-free group; group B: cumulus cell group.
The Effect of Cumulus Cells on the Embryo Development of Vitrified–Thawing Human Mature Oocytes
The post thaw oocyte survival rate (88% vs 58%), cleavage rate (80% vs 56%), and high-quality embryo (75% vs 59%) were significantly higher in group B than in group A (Table 2). Embryo grading criteria are (1) grade I: uniform blastomere with intact zona pellucida and <10% fragment, (2) grade II: slightly nonuniform blastomere with <10% fragment, (3) grade III: blastomere as that in grade II with intact zona pellucida and <50% fragment, (4) grade IV: blastomere being viable, (5) grade V: 2 pronucleus (PN) in day 2 or delayed fertilization, and (6) grade VI: inviable embryo, blastomere lysis. High-quality embryo includes grade I and grade II embryos.
Effects of Cumulus Cells on the Embryo Development of Vitrified–Thawed Human Mature Oocytes a
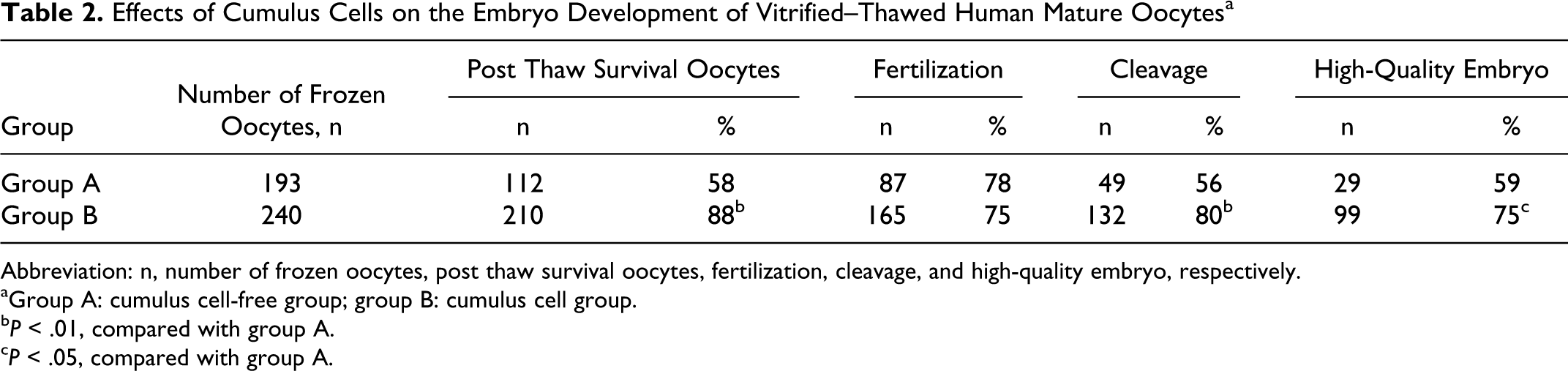
Abbreviation: n, number of frozen oocytes, post thaw survival oocytes, fertilization, cleavage, and high-quality embryo, respectively.
aGroup A: cumulus cell-free group; group B: cumulus cell group.
b P < .01, compared with group A.
c P < .05, compared with group A.
Effects of Cumulus Cells on the Pregnancy Outcomes of Vitrified–Thawed Human Mature Oocytes
There were no significant differences in age (34.7 ± 5.04 vs 36.30 ± 5.41) and endometrial thickness (10.15 ± 1.79 vs 10.13 ± 1.75) on the day of embryo transfer and in the number of transferred embryos (1.67 ± 0.48 vs 1.88 ± 0.52) between both groups, all with Ps > .05, when infertile women underwent embryo transfer. The embryo implantation (37.3% vs 15%) and clinical pregnancy (50% vs 17%) rates were significantly higher in group B than in group A, all with Ps < .05 (Table 3).
Effects of Cumulus Cells on Pregnancy Outcomes of Vitrified–Thawed Human Mature Oocytes a
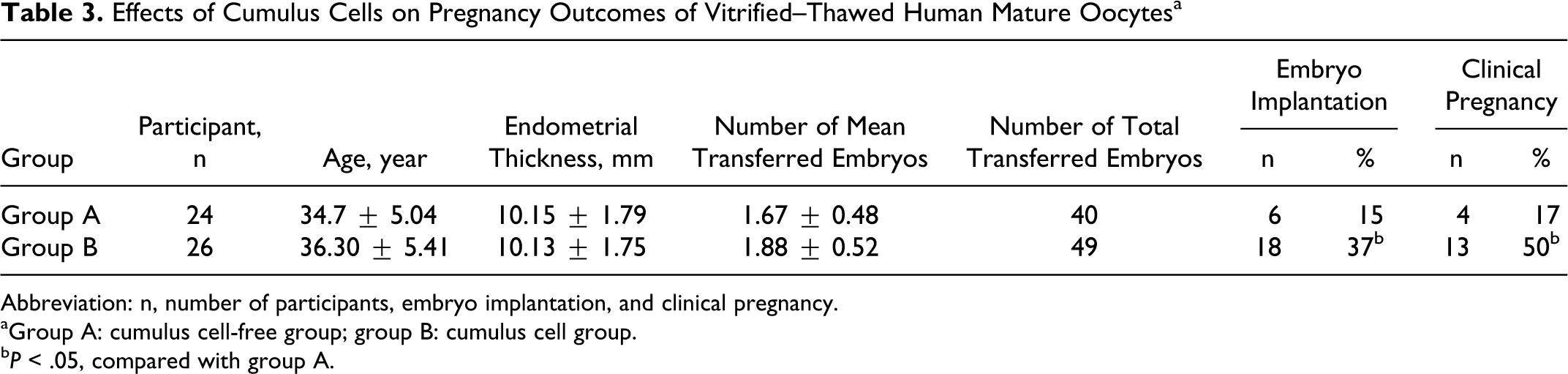
Abbreviation: n, number of participants, embryo implantation, and clinical pregnancy.
aGroup A: cumulus cell-free group; group B: cumulus cell group.
b P < .05, compared with group A.
Embryo Transfer and Clinical Pregnancy of Vitrified–Thawed Oocytes in Both Groups
In group A, 10 participants underwent IVF-ET of own vitrified–thawed oocytes and 1 got clinical pregnancy, 9 participants underwent IVF-ET of donor sperms and vitrified–thawed oocytes and 1 got clinical pregnancy, and 5 participants underwent IVF-ET of donor vitrified–thawed oocytes and 2 got clinical pregnancy. In group B, 8 participants underwent IVF-ET of own vitrified–thawed oocytes and 3 obtained clinical pregnancy, 8 participants underwent IVF-ET of donor sperms and vitrified–thawed oocytes and 5 got clinical pregnancy, and 10 participants underwent IVF-ET of donor vitrified–thawed oocytes and 5 got clinical pregnancy (Table 4).
Embryo Transfer and Clinical Pregnancy of Vitrified–Thawed Oocytes in Both Groups a

Abbreviation: n, indicates the number of participants.
a Group A: cumulus cell-free group; group B: cumulus cell group.
Discussion
Oocyte cryopreservation is faced with a key problem, cryodamage. People have constantly explored a cryopreservative method for oocytes which is economical and convenient and can minimize cryodamage. Cumulus cells, granular cells, and surrounding oocytes possess abundant extracellular matrix with rich hyaluronic acid that forms an interlaced network. The network provides nutrient substance for and transmits signals to oocytes, promoting oocyte maturation and development. 12,13 In recent years, there have been conflicting reports on whether cumulus cells can protect oocytes during cryopreservation. Pickring et al 14 found that cumulus cells had no protective effects on oocytes. It has been reported that the post thaw survival rate is significantly higher in the oocytes with intact cumulus cells than in the cumulus cell-free oocytes. 15,16 In this study, based on no significant differences in age, duration of infertility, infertile causes, and number of retrieved oocytes between both groups when the oocytes were retrieved from infertile women, we found that the survival rate of post thaw oocytes (88% vs 58%), cleavage rate (80% vs 56%), and high-quality embryo rate (75% vs 59%) were significantly higher in group B than in group A. Under the conditions that there were no significant differences between the 2 groups in the general status of the participants undergoing embryo transfer; the embryos implantation rate (37% vs 15%) and the clinical pregnancy rate (50% vs 17%) were significantly higher in group B than in group A. Based on the above results, we speculated that during freezing and thawing, cumulus cells may alleviate the dramatic changes in osmotic pressure caused by high concentration vitrifaction reagent, which reduces the damage on oocyte organelles such as spindle and chromosome and improves the survival rate of vitrified–thawed human mature oocytes.
Little research has been done on the role of cumulus cells in oocyte cryopreservation, especially in human mature oocytes. Most relevant studies have been performed in animals and are about the role of cumulus cells in the cryopreservation of immature oocytes. There is a wide range of complex intercellular connectionism such as gap junction between cumulus cells and oocytes. Cumulus cells transport nutrient substance to oocytes, and at the same time, they also are the media that a variety of substances such as hormones and growth factors exert their effects on oocytes. Cumulus cells play an important role in oocyte development. 17 Our study suggests that compared with cumulus cell-free group, the post thaw oocyte survival rate, cleavage rate, high-quality embryo, embryo implantation, and clinical pregnancy are significantly improved in cumulus-cell group. This may be that after thawing of oocytes with cumulus cells, partial survival cumulus cells have a promotive effect on oocyte development. In addition, it is reported that the removal of cumulus cells from the frozen oocytes may lead to a reduction in a key cyclin, affecting oocyte development. 18
Our study suggests that cumulus cells should be retained in vitreous cryopreservation of oocytes to increase vitrified–thawed oocyte survival rate and embryo development competence and to improve the clinical pregnancy outcomes.
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: supported by National High-tech Program (2006AA02Z4A4).