
Abstract
The endometria of women treated with long-term progestin-only contraceptives (LTPOCs) display abnormally enlarged, fragile blood vessels, decreased endometrial blood flow, oxidative stress, and unpredictable focal abnormal endometrial bleeding. Because human studies on the effects of LTPOC treatment are constrained for ethical and practical reasons, we assessed the suitability of nonoophorectomized guinea pigs (GPs) to best mimic the hormonal milieu of women. The present study demonstrates that treatment of GPs parallels the morphological changes following LTPOC treatment of the human endometrium and ovaries. Specifically, treatment resulted in larger hyperemic, uteri compared with controls. Histopathologic and immunohistochemical analysis demonstrated fewer endometrial glands, decreased luminal mucus, increased numbers of blood vessels, and focal hemorrhage. While increased staining for the cell mitosis marker, Ki67, was present in the zona functionalis, no such increase occurred in the basalis. Lastly, effects on vasomotor features of uterine arteries suggest changes that favor increased resistance and reduced blood flow promoting decreased ability to withstand elevations in transmural pressure.
Introduction
Use of long-term progestin-only contraceptives (LTPOCs) offers a discrete and highly effective family planning method. 1 –3 Unlike estrogen-containing contraceptives, LTPOCs can be used safely during lactation and by patients in which estrogen use is contraindicated. 4 Their prolonged action makes these agents ideal for use by women with limited access to medical care, who need a cost-effective, discrete contraception. 5 A number of LTPOCs, as exemplified by Implanon which releases the third-generation progestin etonogestrel (Eto) from a single implantable rod, inhibit ovulation by preventing the mid-cycle luteinizing hormone surge. During the initial phase of therapy, Eto suppresses follicular development and estradiol (E2) production. However, ovarian steroidogenic activity increases after 6 months. 6
Abnormal uterine bleeding (AUB) following LTPOC administration is primarily responsible for the high discontinuation rate of these agents. 7 –9 Histological sections of endometria from LTPOC-treated patients display aberrant angiogenesis with abnormally enlarged, thin-walled, fragile blood vessels as well as evidence of inflammation and focal hemorrhage. Moreover, LTPOC treatment resulted in reduced endometrial perfusion and increased endometrial oxidative damage.8,10 Unpredictable uterine bleeding patterns associated with LTPOC treatment reflect a combination of these changes in endometrial vessels coupled with a disrupted vascular support stemming from altered proteolysis and repair of the perivascular extracellular matrix (ECM) structure accompanying abnormal angiogenesis.
Progress in further elucidation of the local mechanisms that elicit LTPOC-associated AUB has been hampered by methodological difficulties in conducting relevant human studies. These include patients with a tendency to discontinue and/or abandon LTPOC contraception, as well as the impracticality and ethical proscriptions against obtaining sequential specimens from the same patient over a prolonged period of time. These problems are compounded by the relatively small size of the endometrial samples generally available. 11 The current study focused on the guinea pig (GP) as a relevant animal model with which to overcome these difficulties. Female GPs and women share similar uterine morphology and reproductive endocrine patterns and both exhibit hemochorial placentation. 12 For example in women, in some other primates, and in female GPs, circulating progesterone (P4) during pregnancy is maintained at elevated levels and uterine contractions are initiated by functional P4 withdrawal.
Methods
The GPs were surgically implanted subcutaneously (SQ) with 49-day sustained-release silastic pellets (1 mm in diameter) containing Eto (n = 5) or a sham pellet (n = 5). Briefly, GPs were premedicated with meloxicam (0.1 mg/kg) by (SQ) injection, anesthetized using isoflurane inhalation with a precision vaporizer and face mask and given 0.25 to 0.5 ml of bupivicaine 0.25% SQ at the surgical site prior to make the incision to provide additional local anesthesia. The surgical site was disinfected by cleaning the skin using alternating providone iodine and isopropyl alcohol swabs 3×. Next a 0.5 cm incision was made and pellets placed SQ versus 0.5 cm cranial to the incision. The incision was closed with surgical glue (VetClose Butler Animal Health, Dublin, Ohio). The GPs were given a second dose of meloxicam 24 hours postoperatively. At the end of the experimental period, the blood was collected as a terminal procedure from the caudal vena cava and GPs rendered unconscious by CO2 narcosis or isofluorane anesthesia. After blood collection, GPs were euthanized by exsanguination and tissues (ie, uteri, ovaries, rear leg) harvested. Ovaries and uteri were immersion fixed in 10% neutral-buffered formalin and the rear legs fixed in Bouin fixative (Ricca Chemical Corporation, Arlington, Texas). Tissues were processed, embedded, sectioned, and stained with hematoxylin and eosin (HE) using standard techniques. 13 Histopathologic assessment was carried out by one of the authors (C.J.B.) who was blinded to the experimental manipulation. All animal procedures were approved by the Yale Institutional Animal Care and Use committee.
Immunohistochemistry (IHC) was conducted as previously described. 14 Specifically, sections (4 μm) of formalin-fixed, paraffin-embedded uteri were cut, deparaffinized, rehydrated, and washed in Tris-buffered saline (TBS: 20 mmol/L Tris-HCl, 150 mmol/L NaCl pH 7.6). Tris-buffered saline was used for all subsequent washes and for antibody dilution. Antigen retrieval was carried out by incubating sections in high pH target retrieval solution (DAKO, Copenhagen, Denmark), in a microwave oven at 750 W for 15 minutes. Sections were subsequently rinsed in 3% hydrogen peroxide to block endogenous peroxidase and incubated overnight at 4°C with antibodies against von Willebrand factor (vWF) using a rabbit polyclonal antibody directed against vWF (AB6994 primary antibody; Abcam, Cambridge, Massachusetts) at 1 to 10 000 dilution or a rabbit anti-human Ki67 clone SP6 (Biocare Medical, Concord, California) at 1 to 200 dilution. Slides were then washed 3× with TBS for 5 minutes and incubated with the universal-labeled streptavidin biotin (LSAB) kit (DAKO). After again washing 3× for 5 minutes in TBS, sections were stained with 3,3′-diaminobenzidine tetrahydrochloride (Sigma-Aldrich, St Louis, Missouri), used as a chromogen substrate, and counterstained with Harris hematoxylin (Leica Microsystems. Richmond Illinois). The reaction was stopped by washing the sections in distilled water, and slides were mounted and observed under a light microscope. Staining specificity was tested by substituting nonimmune serum for the primary antibody.
Immunostaining for vWF and Ki67 in the GP endometrium were evaluated by both an experienced pathologist and an experienced immunohistochemist (C.J.B. and G.K.), employing a semiquantitative method in accordance with the following scoring system: 3, marked staining; 2, moderate staining; 1, weak staining; and 0.5 low to no staining. Parallel staining for the Ki67 antigen was carried out to assess the proliferation of cells. The total number of vessels in controls versus Eto-treated animals was assessed with image J (NIH software [http://rsb.info.nih.gov/ij/]) by selecting a minimum of 3 different areas of equal size from 3 different animals using photos taken at the same magnification (×100). The same procedure was used for calculating the relative number of vessels.
Immunoassay
Levels of circulating E2 were measured by enzyme-linked immunosorbent assay (ELISA) Cayman Chemical (Ann Arbor, Michigan). The interassay variation is 23% (at the low-end E2 concentrations) and intra-assay variation is 21% (at low-end E2 concentrations).
Uterine Artery Studies
The entire uterus was removed, immersed in cold (4oC) 4-(2-hydroxyethyl)-1-piperazineethanesulfonic acid (HEPES)-physiological saline solution (HEPES-PSS) and shipped overnight to Vermont for vascular measurements. Upon receipt, the uterus was placed in a Petri dish filled with HEPES-PSS containing (in mmol/L) 141.8 NaCl, 4.7 KCl, 1.7 MgSO4, 0.5 EDTA, 2.8 CaCl2, 10 HEPES, 1.2 KH2PO4, and 5 glucose; pH was adjusted to 7.4 using 1 N NaOH; 0.1 mmol/L papavarine; and 10 µmol/L diltiazem were added to fully relax the vasculature prior to making measurements of the main uterine artery length and inner diameters with a flexible ruler and a dissecting microscope fitted with an eyepiece micrometer, respectively. Radial artery segments (1-2 mm long) were dissected free from connective and adipose tissue and transferred to the chamber of a small-vessel arteriograph. One end of the vessel was tied onto a glass cannula and flushed of any luminal contents by increasing the pressure before securing the distal end onto a second cannula using a servo-null pressure system (Living Systems Instrumentation, St. Albans, Vermont). All vessels were initially pressurized to 10 mm Hg and equilibrated for 45 to 60 minutes, HEPES-PSS at 37°C and pH 7.4 before beginning the experiment. Lumen diameter was measured using a video dimension analyzer (LSI) in conjunction with data-acquisition software (Ionoptix, Milton, MA). Following equilibration, intraluminal pressure was increased to 25 mm Hg and superfused with a depolarizing solution containing high potassium chloride (80 mmol/L) to induce constriction. Once constriction was achieved and stable for about 10 minutes, intraluminal pressure was increased stepwise to 200 mm Hg while measuring changes in lumen diameter. This procedure allowed us to evaluate the ability of the vessel to withstand changes in wall tension and thereby assess the comparative contractility of vessels from Eto versus placebo-treated animals.
Statistics
All statistical analyses were conducted using the Mann-Whitney test using Sigma Stat (Systat Software Inc, Chicago, Illinois) to allow for 5 degrees of freedom and a desired power of >0.8. The significance (P < .05) of differences in arterial dimensions and reactivity were determined using an unpaired t test.
Results
Morphologic examination of GP uteri at necropsy demonstrated the expected changes in size, weight, and gross morphological appearance following LTPOC treatment (Figure 1A and Table 1). Uteri exposed to Eto displayed significantly greater size and weight compared with the controls (Figure 1D and Table 1) and had subjectively increased mucous production and hyperemia (Figure 1E, F). Additionally, the cross-sectional area of the uteri derived from the controls was statistically smaller than those from the Eto-treated animals (Table 1).
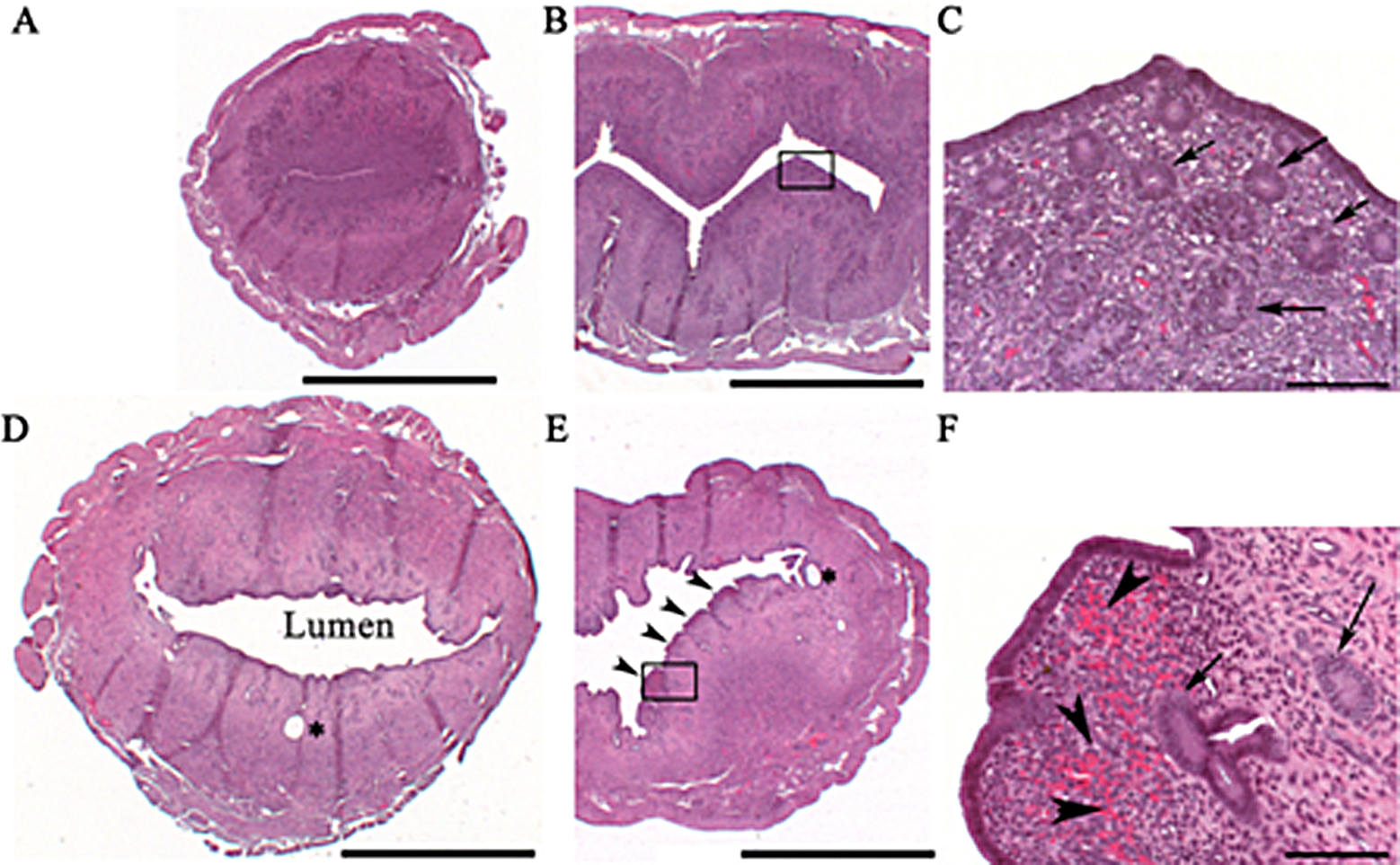
Histopathological analysis of uterine sections from the controls and etonogestrel (Eto)-treated animals. Controls displayed typical endometrial gland number and morphology (A, B, C, arrows), Eto-treated uteri displayed a marked increase in luminal mucous but fewer glands (D, E, F arrows; and Table 1). The Eto-exposed uteri displayed multifocal areas of endometrial hyperemia and hemorrhage subjacent to the endometrial epithelium (E, F, arrowheads), whereas the controls showed no such changes. Eto-treated uteri also occasionally displayed dilated or cystic glands (*, D, E).
Differences Among Control and Eto-Treated GPs a
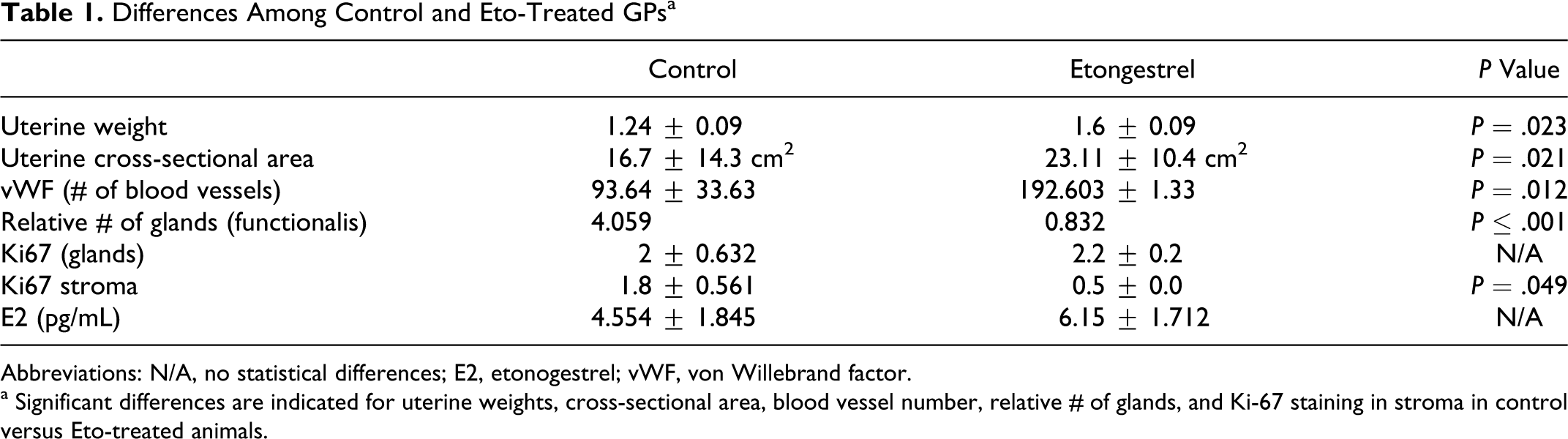
Abbreviations: N/A, no statistical differences; E2, etonogestrel; vWF, von Willebrand factor.
a Significant differences are indicated for uterine weights, cross-sectional area, blood vessel number, relative # of glands, and Ki-67 staining in stroma in control versus Eto-treated animals.
Histopathological analysis of uterine sections from control and Eto-treated animals displayed marked differences. Whereas controls displayed typical endometrial gland number and morphology (Figure 1A, B, C, arrows), Eto-treated uteri displayed a marked increase in luminal mucous but fewer glands (Figure 1D, E, F arrows and Table 1). The Eto uteri also displayed multifocal areas of endometrial hyperemia and hemorrhage subjacent to the endometrial epithelium (Figure 1E, F, arrowheads), whereas the controls showed no such changes. The Eto-treated uteri also occasionally displayed dilated or cystic glands (Figure 1D, E*).
Because there is an association between some LTPOCs and significant bone loss, 15 we conducted a histopathologic review of the femur from each GP. Treatment by Eto showed no significant differences in bone morphology (data not shown). Immunostaining of control endometria for vWF demonstrated normally scattered blood vessels within the functionalis (Figure 2A, B arrows), whereas the endometria from Eto-treated GPs demonstrated increased number of blood vessels throughout both endometrium and myometrium (Figure 2C, D arrows and Table 1).
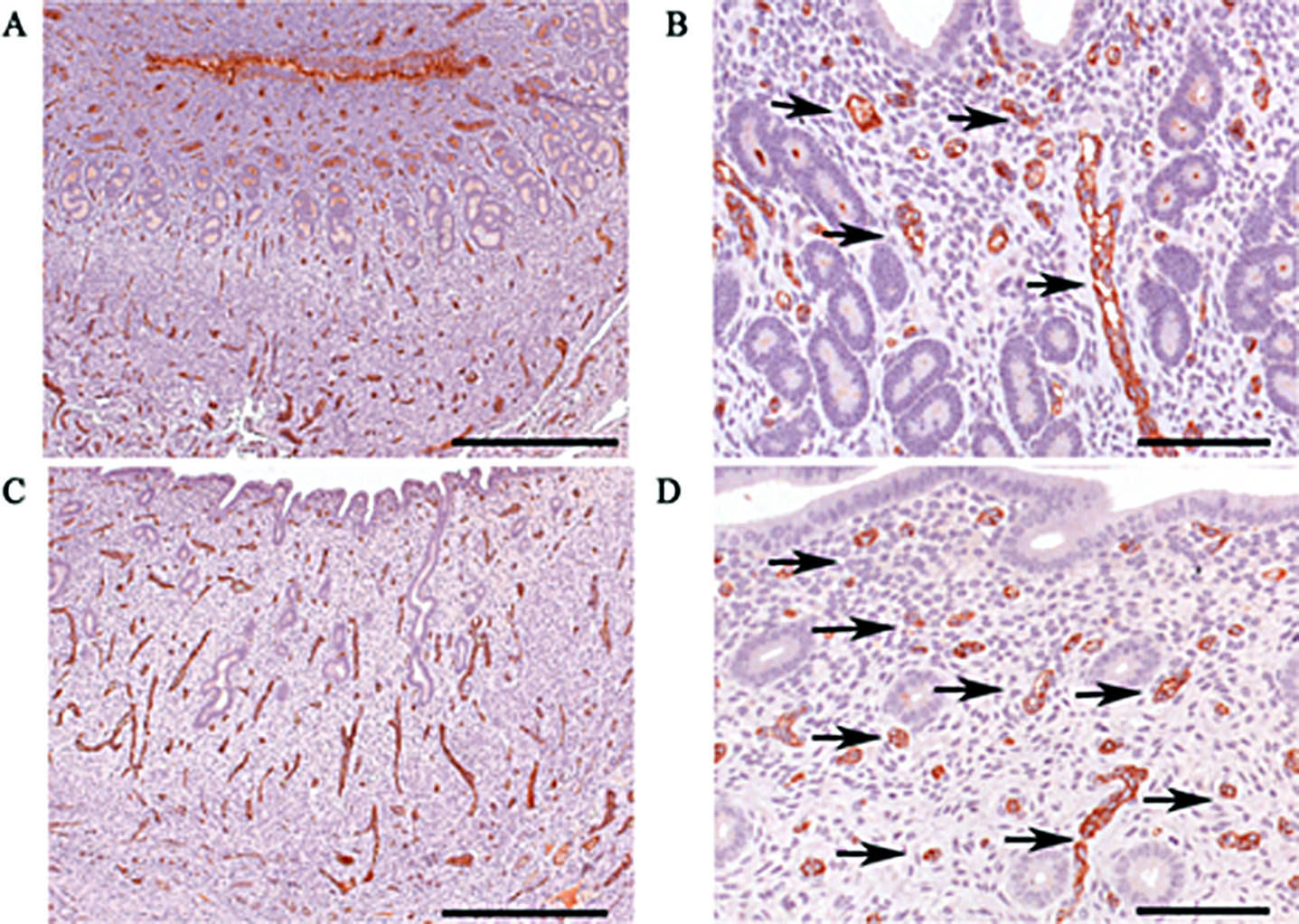
von Willebrand factor (vWF) immunohistochemistry of control and etonogestrel (Eto)-treated endometria. Scattered blood vessels stained for vWF are observed within the functionalis of controls (A, B arrows), whereas endometria from Eto-treated guinea pigs (GPs) demonstrated increased number of blood vessels throughout both endometrium and myometrium (C, D arrows; and Table 1).
Uterine arteries from Eto-treated animals were significantly longer and narrower than those from vehicle (placebo)-treated controls (Table 2, Figure 3A). Furthermore, radial arteries from Eto-treated GPs were functionally hyperreactive, as they developed more tone in a high-potassium depolarizing solution (Figure 3B). When the transmural pressure was elevated, however, they were less able to maintain constriction (Figure 4), that is were more prone to forced dilatation in response to an increase in wall tension. Together, these observations favor an increase in uterine resistance, tissue hypoxia, and an increased likelihood of endometrial bleeding.
Changes in Main Uterine Artery Length and Intraluminal Diameter in Eto-Treated Versus Placebo (Control) Animals a
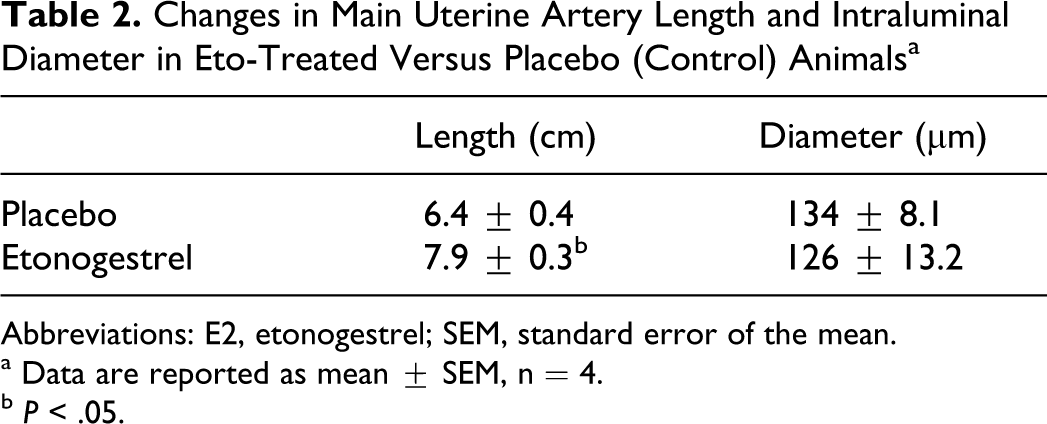
Abbreviations: E2, etonogestrel; SEM, standard error of the mean.
a Data are reported as mean ± SEM, n = 4.
b P < .05.
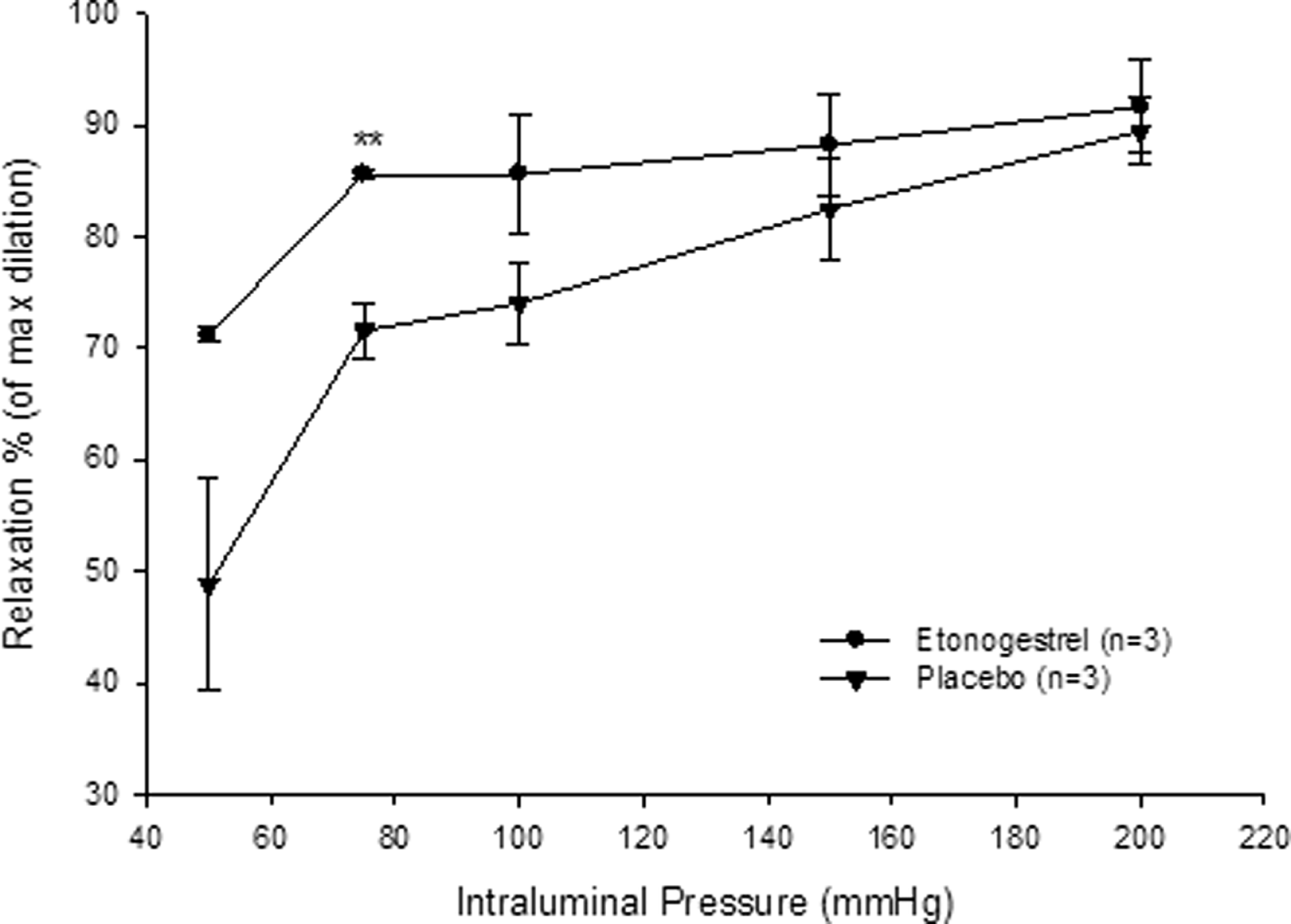
Radial uterine artery relaxation in response to elevations in intraluminal pressure in control (placebo) versus Eto-treated animals. Data are reported as mean ± SEM, n = 4, *P < .01. Eto indicates etonogestrel; SEM, standard error of the mean.
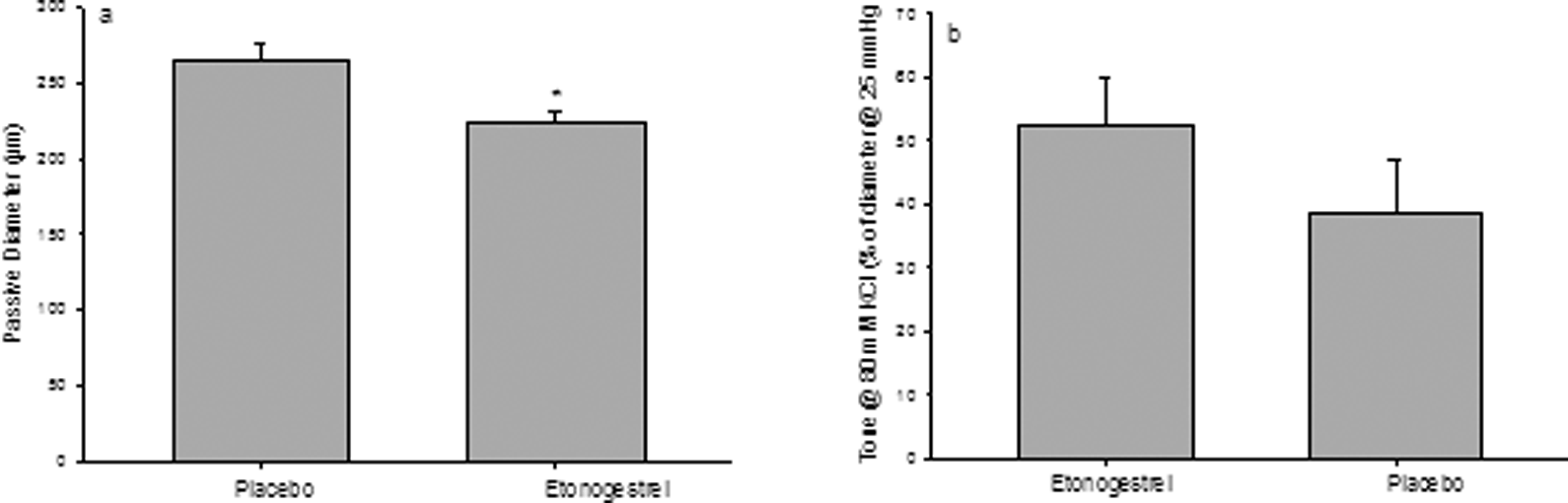
Passive diameter and tone of uterine radial arteries in placebo (control) Eto-treated animals. A, Passive lumen diameters of radial uterine arteries at 25 mm Hg under fully relaxed conditions (papaverine, 10−4 mol/L + diltiazem, 10−5 mol/L). B, Extent of tone in response to 80 mmol/L of KCl at 25 mm Hg. Data are reported as mean ± SEM, n = 4, *P < .05. Eto indicates etonogestrel; SEM, standard error of the mean.
Staining for Ki 67 was carried out to compare cell proliferation between endometria derived from control versus Eto-treated animals. No significant difference in proliferation was observed among the glands between the 2 groups, but stromal cells displayed a significant reduction in Ki 67 staining 1.8 ± 0.561 vs 0.5 ± 0.0 following treatment (Table 1). To ascertain whether differences in proliferation within the same group samples correlated with levels of circulating E2, we assessed the serum E2 levels in Eto versus control GPs. No statistically significant differences in the circulating E2 concentrations after 49 days of treatment were noted in cases versus controls (Table 1). Spearman correlation test also demonstrated no significant relationship between Ki 67 staining and E2 (P = NS). Finally, while no differences in circulating levels of E2 were seen, none of the Eto-treated GP had any visible corpus lutea (Figure 5 lower panels) compared to controls (upper panels*). This is similar to what is initially observed in humans treated with LTPOCs. 16
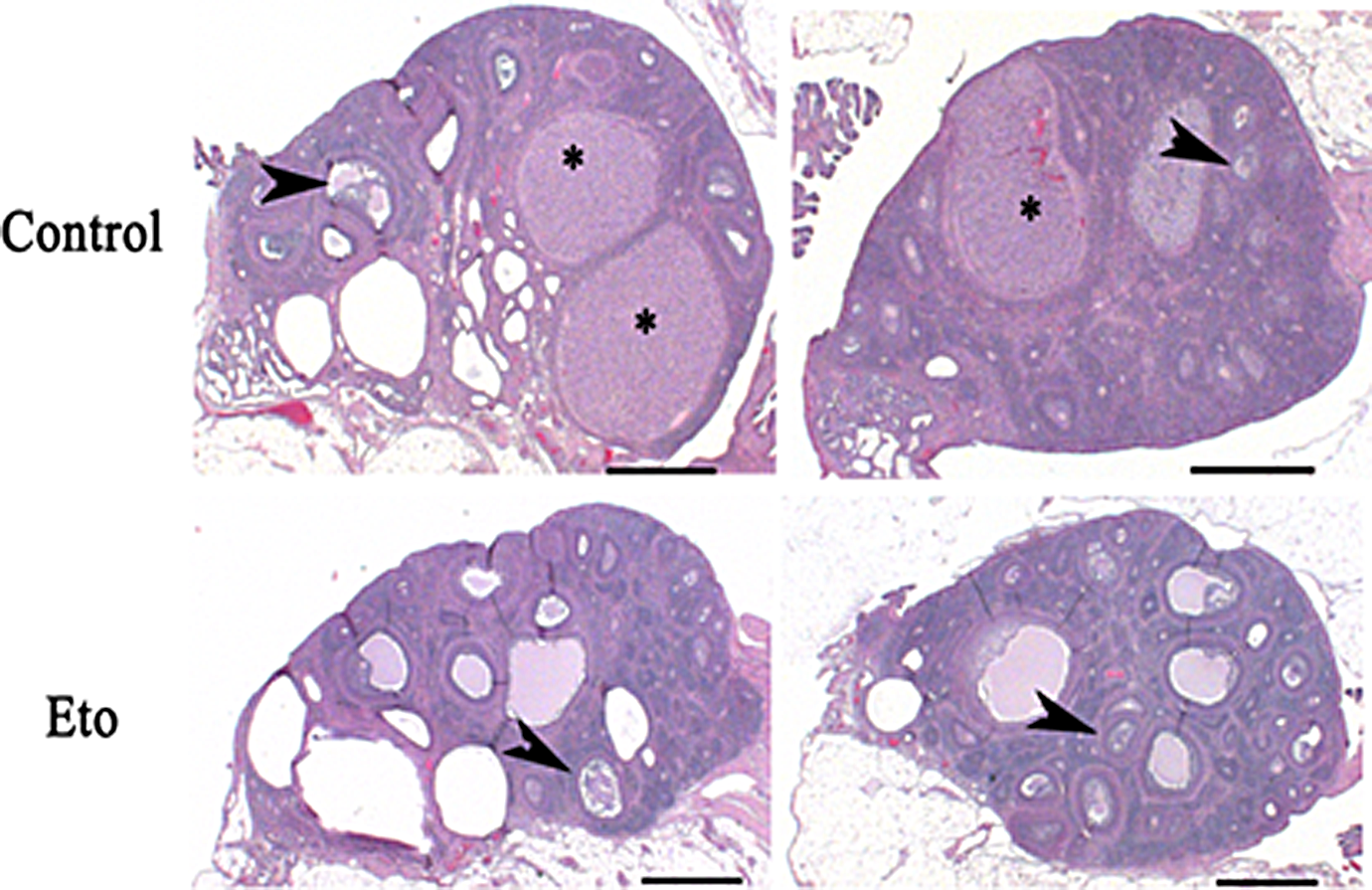
Effect of LTPOC on the ovaries. Although follicles (arrowheads) were visible in both, only controls had visible corpora lutea (*); Eto-treated GPs had no visible corpus lutea. LTPOC indicates long-term progestin-only contraceptive; Eto, etonogestrel; GPs, guinea pigs.
Discussion
Because of their safety and prolonged effectiveness, LTPOCs are ideal for use in underdeveloped countries with limited access to trained medical personnel. Formulations include Depo-Provera, a subdermal injection of medroxy-progesterone acetate (MPA), Mirena, which releases levonorgestrel (LNG) from an intrauterine system, and Implanon, which consists of a subdermally implanted rod that releases Eto. The most frequent complication leading to discontinuation of LTPOC use is AUB, which is not a health issue, but a source of inconvenience, personal distaste, and in certain societies of religious taboo. 2,17
Hickey and colleagues 9 found significantly reduced endometrial perfusion as measured by laser Doppler fluxmetry, 1 month after Implanon insertion. This was accompanied by (1) local hypoxia/reperfusion as indicated by increased production of 8-isoprostane and generation of such reactive oxygen species (ROS) as nitrotyrosine, an oxidative protein damage indicator, and 8-deoxyguanosine, an oxidative DNA damage indicator; (2) aberrant angiogenesis as indicated by decreased expression of angiopoietin 1, a vessel stabilizing factor and increased expression of both angiopoietin 2, a vessel branching and elongation factor, and vascular endothelial cell growth factor (VEGF), the primary mediator of angiogenesis. However, the cause of these profound LTPOC-associated changes in endometrial perfusion remained unexplored and required a suitable animal model.
In our previous studies, we confirmed the suitability of the GP as a model for LTPOC effects on the human uterus. For example, we evaluated the separate and interactive effects of E2 and MPA on GP-endometrial weight, vascular morphology, oxidative stress, and apoptosis on oophorectomized GPs treated with hormones for 21 days. 14 We observed GP uteri to be enlarged by both E2 and MPA. Of note, MPA alone increased blood vessel density average area, while E2 significantly decreased this parameter. These changes were associated with highly elevated lipid peroxidation, chromatin redistribution, nuclear pyknosis, karyolysis, and increased apoptosis in MPA-exposed uteri. 14 However, because GPs were oophorectomized, some of the progestin changes may have been exaggerated and the conditions did not mimic the hormonal milieu of women treated with LTPOC. 14
In this study, we confirmed the profound angiogenic effects of LTPOC in nonoophorectomized GPs. Moreover, we have now obtained insights into the reduced endometrial perfusion and vessel injury observed in LTPOC-treated human endometrial. Thus, measurements of the uterine vasculature in this model demonstrated the presence of both structural and functional changes that favor increased uterine vascular resistance and downstream hypoxia. Specifically, vessels from treated animals were longer and narrower than those from their placebo-treated counterparts. They also developed more tone in response to potassium depolarization. Interestingly, Eto-exposed uterine arteries were less able to withstand elevations in wall tension secondary to increased transmural pressure and were thus more prone to forced dilatation, a process that leads to the transmission of excessive pressures to smaller, more fragile downstream endometrial vessels, and thereby increase the likelihood of rupture and bleeding as has been noted in women on progestin-only contraceptives. 18,19
Because women receiving LTPOC are not oophorectomized, we sought to develop a model that would better mimic LTPOC treatment in women. In this study we demonstrate that nonoophorectomized GPs display remarkably similar endometrial morphological and vascular changes including focal hemorrhage. Moreover, it appears that these agents directly affect the uterine artery resulting in both vasoconstriction and reperfusion oxidative and mechanical injury. Armed with this robust model, we can now examine various steroidal agents and combinations in an effort to achieve contraception without AUB.
Footnotes
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded by NIH/NICHD 2 RO1 HD 033937.