
Abstract
The aim of this study was to evaluate inflammatory response in chronic anovulating infertility women undergoing intracytoplasmic sperm injection. Thirteen infertile women with chronic anovulation and 23 normally ovulating women were prospectively evaluated. N-acetylglucosaminidase (NAG), myeloperoxidase (MPO), monocyte chemoattractant protein 1 (MCP-1), and C-reactive protein (CRP) concentrations were evaluated in serum and follicular fluid. Women with chronic anovulation presented higher NAG and MPO activity in follicular fluid when compared with normally ovulating women. Serum MPO activity was higher in the control group compared to the chronic anovulation group. Both serum and follicular fluid CRP concentrations were higher in women with chronic anovulation in comparison with the control group. Higher MCP-1 follicular fluid concentrations and serum levels of CRP were associated with the occurrence of ovarian hyperstimulation syndrome. Patients with chronic anovulation exhibited significantly higher follicle macrophage/neutrophil activation as well as unspecific inflammatory response by comparison with normally ovulating women.
Keywords
Introduction
Chronic anovulation is a common and heterogeneous ovarian disorder affecting women of reproductive age with a prevalence of approximately 5% to 10% worldwide. 1, 2 Since the initial report, our knowledge of the endocrine mechanism underlying the clinical signs of the syndrome still remains unclear, incomplete, and often misleading. 3 Mammalian ovulation has been compared to an inflammatory reaction, in which leucocytes are the most mobilized cells. 4 ,5 It seems that there are cyclic changes in the leukocyte population in the ovary and that these cell types actively participate in the functional and structural changes of the follicle and corpus luteum. 6 ,7
Much interest has been focused on the mechanisms involved in the activation and recruitment of leukocytes into inflammation tissues. There are several studies that have directly demonstrated the necessity of leukocytes for a full ovulatory response. Neutrophils are the dominant immune cells at the early stage of an acute inflammation and also during ovulation. Macrophage is the other major cell type that is recruited to an inflammatory site during the early stage and this cell type is also present in the ovary at ovulation. 4 –8 Among the products implicated in the mechanisms underlying inflammatory processes, myeloperoxidase (MPO), which is released from neutrophil–azurophilic granules, has been extensively used as a marker for measuring polymorphonuclear leukocyte accumulation in tissue samples. 9 N-acetyl-beta-glucosaminidase (NAG), a lysosomal enzyme, has been employed to monitor macrophage accumulation/activation in a variety of animal and human tissues. 10
Chemokines are small (8-12 kDa) secretory proteins that play a key role in inflammatory reactions by mediating leukocyte migration. Monocyte chemotactic protein 1 (MCP-1) is a potent activator of monocytes, T lymphocytes, and basophils. Research data have suggested that it may be involved in the cyclic changes within the ovary. 11 Another inflammatory acute phase marker, the active phase C-reactive protein (CRP) which is produced by the liver, has been reported to be increased in women with chronic anovulation in comparison with those with regular ovulatory cycles as well as during controlled ovarian hyperstimulation (COH) for in vitro fertilization (IVF). 12 ,13 –15
Several investigations have suggested that women with chronic anovulation and polycystic ovary syndrome (PCOS) are in a constant chronic inflammatory status, while others describe chronic anovulation and PCOS as a low-grade inflammation disorder. 16 –18 The term low-grade inflammation identifies a condition characterized by the increase in the circulation of several mediators of inflammation in response to a noxious stimulus. Molecules, such as tumor necrosis factor-alpha (TNF-α), interleukin (IL) 1, IL-6, and CRP, are classically related to low-grade inflammation. Many studies have demonstrated that in women with PCOS a positive relationship exists between CRP values and insulin resistance, body weight, and fatty mass.18–20 C-reactive protein is a circulating marker of the proinflammatory state in PCOS, as evidenced by the 2-fold elevation in circulating CRP in women with the disorder compared with controls. 19
Unraveling the role of inflammatory markers in PCOS remains a challenge. The metabolic environment has a direct effect on the ovarian follicular microenvironment and may be associated with inflammation and increased oxidative stress, which has been associated with decreased developmental potential of the oocyte. 21 The evaluation of substances present in human follicular fluid, which originate from plasma or are produced by follicular structures, reflects oocyte maturation and can be used to assess oocyte quality. 22 Several ovulation-associated mediators are produced by most leukocyte subtypes including neutrophils, macrophages, and mast cells. It seems that there are cyclic changes in the leukocyte population in the ovary, which is vital for normal ovarian function. 6 Given the critical role of inflammation in the ovulatory process, the present study was undertaken to evaluate inflammatory responses at both systemic and local levels in patients with anovulatory infertility and normally ovulating women undergoing intracytoplasmic sperm injection (ICSI).
Material and Methods
The study protocol was approved by the national and local Ethics Committee and written informed consent was also obtained from all participants before the procedure.
Thirteen patients with chronic anovulation (study group) and 23 normally ovulating women (control group), both undergoing ICSI and embryo transfer were prospectively studied. Concentrations of NAG, MPO, MCP-1, and CRP were evaluated in serum and follicular fluids obtained at the time of oocyte retrieval. Inclusion criteria for the study group were patients with chronic oligo- (6 or fewer menses per year) or amenorrhea, with 12 or more follicles (2-9 mm in diameter) in 1 or both ovaries with increased ovarian volume (>10 cm3) at transvaginal ultrasound evaluation which fulfills the Rotterdam Criteria for PCOS. However, no laboratory tests to exclude secondary causes of hyperandrogenism or diagnose metabolic syndrome were performed. 23 ,24 The control group included patients with regular menses and levels of progesterone above 5 ng/mL in the luteal phase of the preceding menstrual cycle, indicating normal ovulation. 25 ,26 Indication for ICSI in both groups was male factor infertility.
Assisted Reproductive Technology
All patients were downregulated with gonadotropin-releasing hormone (GnRH) agonist (3.75 mg; leuprolide acetate depot suspension—Lectrum, Novartis, Entre Rios, Argentina) administered in the midluteal phase of the preceding cycle or at the first day of the stimulation cycle. Subsequent COH with human menopausal gonadotropin ([hMG] Merional Meizler; 150-300 IU/d) was started once there was no sonographic evidence of ovarian follicular activity (endometrium thickness <5 mm and no leading follicles in both ovaries). Human chorionic gonadotropin ([hCG] 10.000 IU—Choriomon; Meizler, São Paulo, Brazil) was administered when at least 2 of the leading follicles exceeded 17 mm diameter each. Oocyte retrieval was performed 35 to 36 hours later using vaginal ultrasound guidance. Follicular fluid from follicles >16 mm in diameter was collected and fluid with blood contamination and flushing was discarded. Both fluid and blood samples were centrifuged (200g, 10 minutes), and supernatants of serum and follicular fluids were carefully extracted and were then frozen at −80°C until analysis.
Metaphase II oocytes, identified by the presence of the first polar body, were injected. Single sperm injection (ICSI) was performed 3 to 6 hours after oocyte retrieval using previously described techniques and equipments. 27 Embryos of day 2/3 were transferred back to the uterine cavity using a fine transcervical catheter (Sydney; COOK Medical, St. Petersburg, FL, USA.) under ultrasound guidance. All women received luteal phase supplementation (natural micronized progesterone 200 mg vaginally thrice daily [tid]—Evocanil; Zodiac, São Paulo, Brazil) for 2 weeks until the result of the pregnancy blood test (β-hCG) was available. Progesterone supplementation was continued up to the 12th week of pregnancy.
Evaluation of NAG Activity
Accumulation of mononuclear cells in follicular fluid and serum was quantified by measuring the levels of NAG, a lysosomal enzyme present in high levels in activated macrophages.
28
An aliquot of the follicular fluid and serum supernatant was homogenized in NaCl solution (0.9% weight/volume [w/v] plus 0.1% volume/volume [v/v] Triton X-100-Promega) and then centrifuged at 3000g for 10 minutes at 4°C. Supernatant samples (100 μL) were incubated for 10 minutes with 100 μL of p-nitrophenyl-N-acetyl-beta-
Analysis of MPO Activity
The extent at which neutrophil accumulated in follicular fluid and serum was measured by MPO activity assays as previously described in the literature. 28 An aliquot of follicular fluid and serum supernatant was homogenized in pH 4.7 buffer (0.1 mol/L NaCl, 0.02 mol/L NaPO4, 0.015 mol/L Na EDTA) and centrifuged at 12000 g for 10 minutes. The supernatants were then resuspended in 0.05 mol/L NaPO4 buffer (pH 5.4) containing 0.5% hexadecyltrimethylammonium bromide (HTAB) followed by 3 freeze–thaw cycles using liquid nitrogen. The activity of MPO in the samples was assayed by measuring the change in absorbance (OD) at 450 nm using tetramethylbenzidine (1.6 mmol/L) and H2O2 (0.3 mmol/L). The reaction was terminated by the addition of 50 µL of H2SO4 (4 mol/L). Results were expressed in OD.
Evaluation of MCP-1 Concentration
Immunoactive MCP-1 both in serum supernatant and in follicular fluid was measured using the kit LINCOplex Cytokine Analytes/Serum - HCYTO-60K by enzyme-linked immunosorbent assay (ELISA). It is a multiplex assay kit manufactured by LINCO Research, Inc. located in Missouri, USA. The sensitivity of the assay for MCP-1 was 1.29 pg/mL. Inter- and intra-assay coefficients of variations were 65%CV and 11.1%CV, respectively.
Evaluation of CRP Concentration
Serum supernatant and follicular fluid concentrations of CRP were determined with a high-sensitivity immunonephelometric assay (Dade Behring Inc, Newark, Delaware, EUA) using an automated clinical chemistry analyzer. Specific antibodies coated with polystyrene particles form a complex with CRP in the measured study sample. The amount of scattered light is directly proportional to the size of the antigen–antibody complex and reflects the high-sensitivity CRP (hs-CRP) concentration present in the study sample with a detection limit of 0.0175 mg/dL.
Statistical Analysis
Statistical analysis was performed with the SPSS 16.0 software package (SPSS Inc, Chicago, Illinois). Results are presented as means ± standard error of the mean (SEM). Data were analyzed using Student t paired and unpaired tests to evaluate significant differences between the groups. The level of significance was set at P < .05. Power calculations based on the expected or desired effect size showed that 13 patients in the case group and 23 in the control group showed a confidence level of 95%, statistical power of 80%, and a minimal detectable difference of 1 standard deviation (SD).
Results
The age range of the patients from both groups was 20 to 37 years (mean 28.9 ± 0.6 years). The mean body mass index (BMI) was 21.7 ± 0.4 kg/cm2 (ranging from 17.6 to 28 kg/cm2). Primary infertility was evidenced in 31 women (86.1%) and secondary in 5 cases (13.9%). No significant difference was observed between groups regarding age, duration of infertility, or BMI (Table 1). Patients with chronic anovulation presented with higher basal luteinizing hormone (LH), number of antral follicles, and ovarian volume prior to induction compared with normally ovulating women. In addition, there was no significant difference concerning the amount of hMG units used, number of oocytes retrieved, number of mature oocytes (MII), number of embryos transferred, and fertilization rates between the groups studied (Table 1).
Clinical Data of Patients With Chronic Anovulation (Cases) and Normally Ovulating Women (Control Group) a
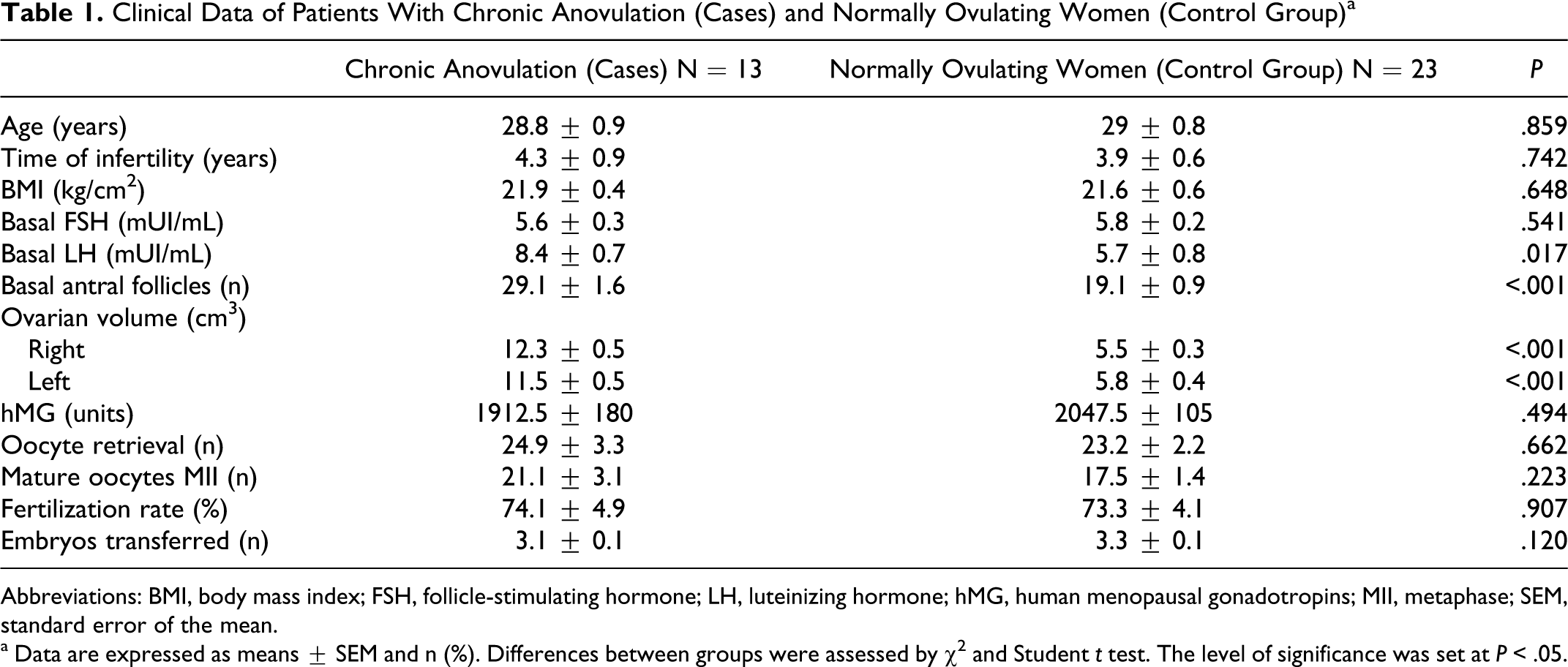
Abbreviations: BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone; hMG, human menopausal gonadotropins; MII, metaphase; SEM, standard error of the mean.
a Data are expressed as means ± SEM and n (%). Differences between groups were assessed by χ 2 and Student t test. The level of significance was set at P < .05.
Activity of NAG
Patients with chronic anovulation showed higher follicular fluid NAG activity (187.9 ± 7.7 vs 216.3 ± 15.8 nmol/L; P = .025) compared with the control group (Figure 1). Activity of NAG was not associated with a higher number of oocytes retrieved, mature oocytes (MII), occurrence of ovarian hyperstimulation syndrome (OHSS) or pregnancy (Table 2).
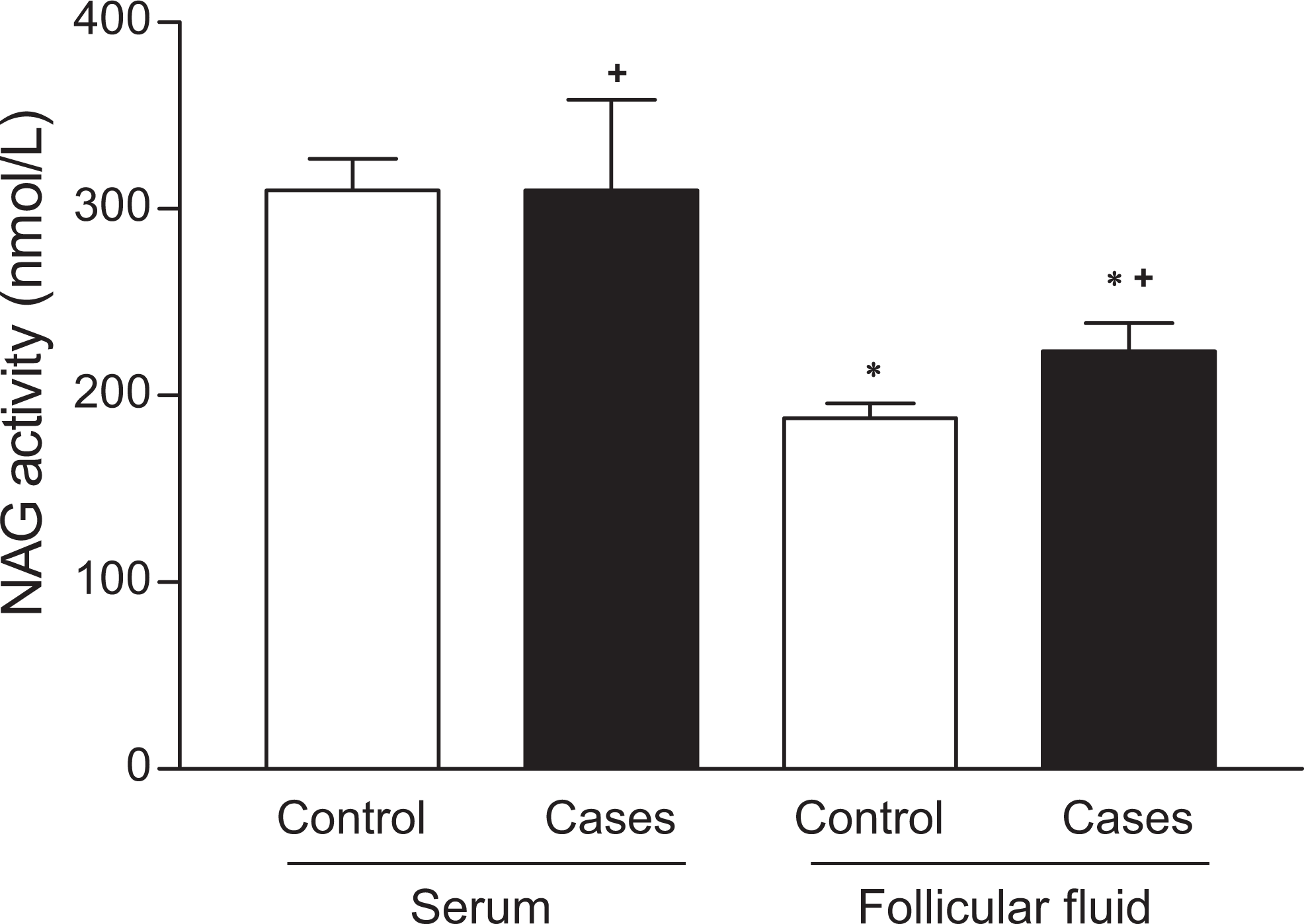
Evaluation of serum and follicular fluid NAG activity in control group (n = 23) and in patients with chronic anovulation (n = 13). NAG indicates N-acetilglucosaminidase. The data were analyzed using t Student paired and unpaired tests. Significance level was established at P < .05. *marks black bars (cases) that differ at P < .05 from controls and +marks follicular fluid bars that differ at P < .05 from serum.
Association Between Number of Oocyte Retrieval, Mature Oocytes (MII), Occurrence of Ovarian Hyperstimulation Syndrome, and Pregnancy With Follicular Fluid and Serum NAG, MPO, MCP-1 and CRP Concentration Levels in Anovulating Infertile Patients (cases) and Normally Ovulating Women (control) Undergoing ICSIa,b
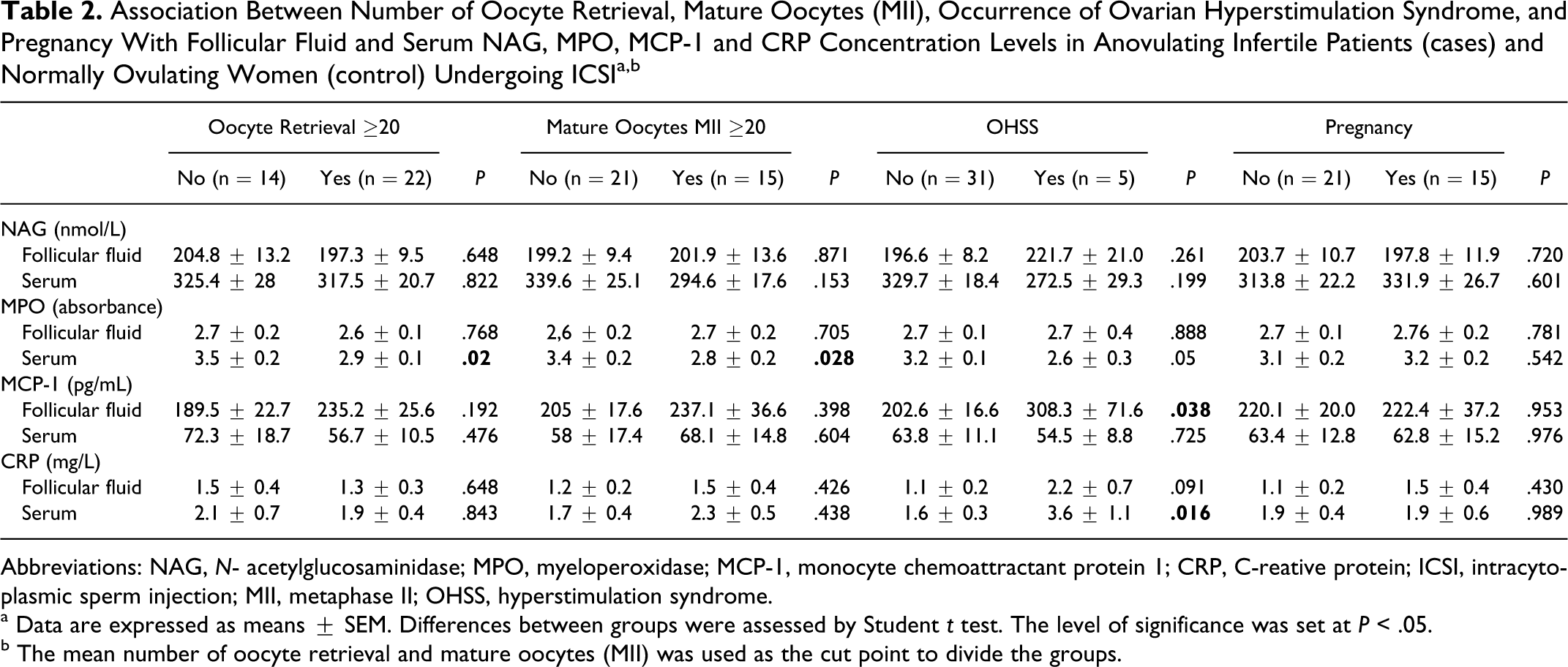
Abbreviations: NAG, N- acetylglucosaminidase; MPO, myeloperoxidase; MCP-1, monocyte chemoattractant protein 1; CRP, C-reative protein; ICSI, intracytoplasmic sperm injection; MII, metaphase II; OHSS, hyperstimulation syndrome.
a Data are expressed as means ± SEM. Differences between groups were assessed by Student t test. The level of significance was set at P < .05.
b The mean number of oocyte retrieval and mature oocytes (MII) was used as the cut point to divide the groups.
Activity of MPO
Serum MPO activity was higher in the control group by comparison with women with chronic anovulation (3.4 ± 0.1 vs 2.6 ± 0 absorbance; P = .001). The activity of MPO in follicular fluid was higher in the patients with chronic anovulation (2.5 ± 0.1 vs 3.0 ± 0.2 absorbance; P = .030; Figure 2). Serum supernatant MPO activity was associated with a higher number of oocytes retrieved and mature oocytes (MII; Table 2). The activity of MPO was not associated with the occurrence of OHSS neither with the presence of pregnancy nor with absence of pregnancy (Table 2).
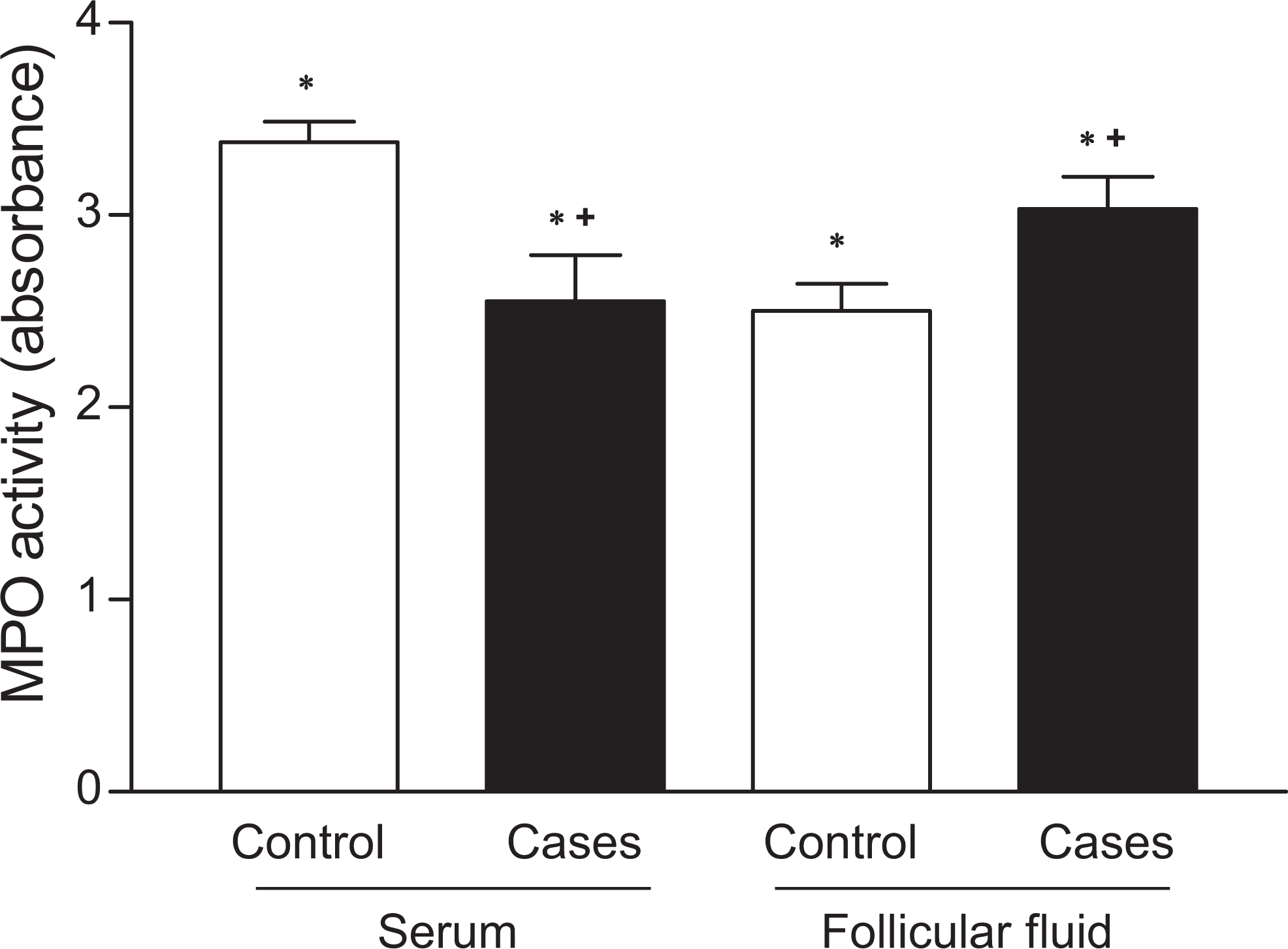
Evaluation of serum and follicular fluid MPO activity in the control group (n = 23) and in patients with chronic anovulation (n = 13). MPO indicates myeloperoxidase. The data were analyzed using t Student paired and unpaired tests. Significance level was established at P < .05. *marks black bars (cases) that differ at P < .05 from controls and +marks follicular fluid bars that differ at P < .05 from serum.
Concentration of MCP-1
No significant difference was observed in MCP-1 concentration between serum supernatant and follicular fluid in both groups under investigation (Figure 3). Concentrations of MCP-1 were not associated with a higher number of oocytes retrieved or with the number of mature oocytes (MII; Table 2). The occurrence of OHSS was associated with higher MCP-1 follicular fluid concentrations (Table 2).
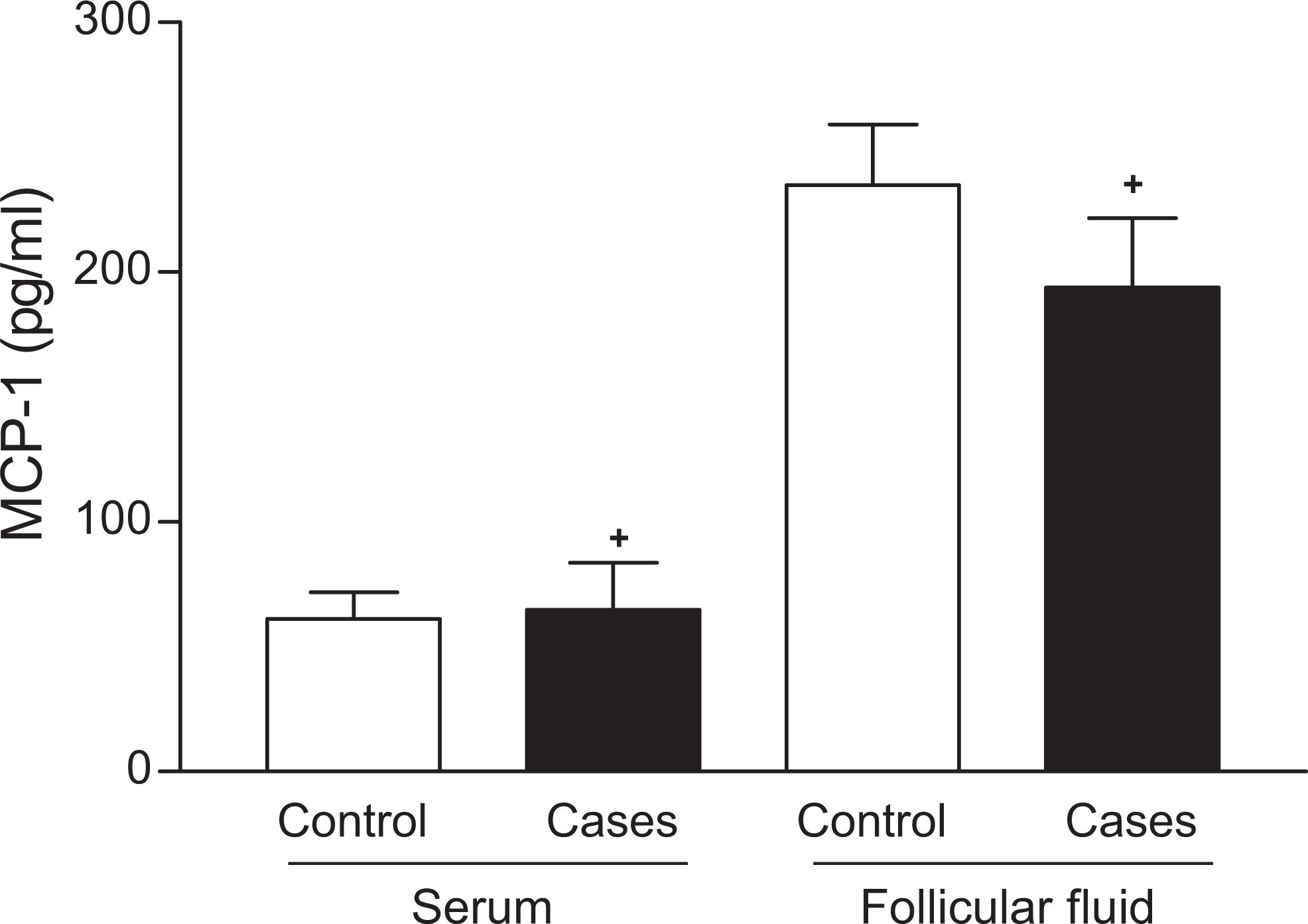
Evaluation of serum and follicular fluid MCP-1 concentration in control group (n = 23) and in patients with chronic anovulation (n = 13). MCP-1 indicates monocyte chemoattractant protein 1. The data were analyzed using t Student paired and unpaired tests. Significance level was established at P < .05. *marks black bars (cases) that differ at P < .05 from controls and +marks follicular fluid bars that differ at P < .05 from serum.
Concentration of CRP
Both serum (1.5 ± 0.3 vs 3.0 ± 0.7 mg/L; P = .024) and follicular fluid (0.9 ± 0.1 vs 2.1 ± 0.4 mg/L; P = .025) CRP concentrations were higher in patients with chronic anovulation compared with the control group (Figure 4). Concentrations of CRP were not associated with a higher number of oocytes retrieved or with the number of mature oocytes (MII; Table 2). Higher serum levels of CRP were also correlated with the occurrence of OHSS (Table 2).
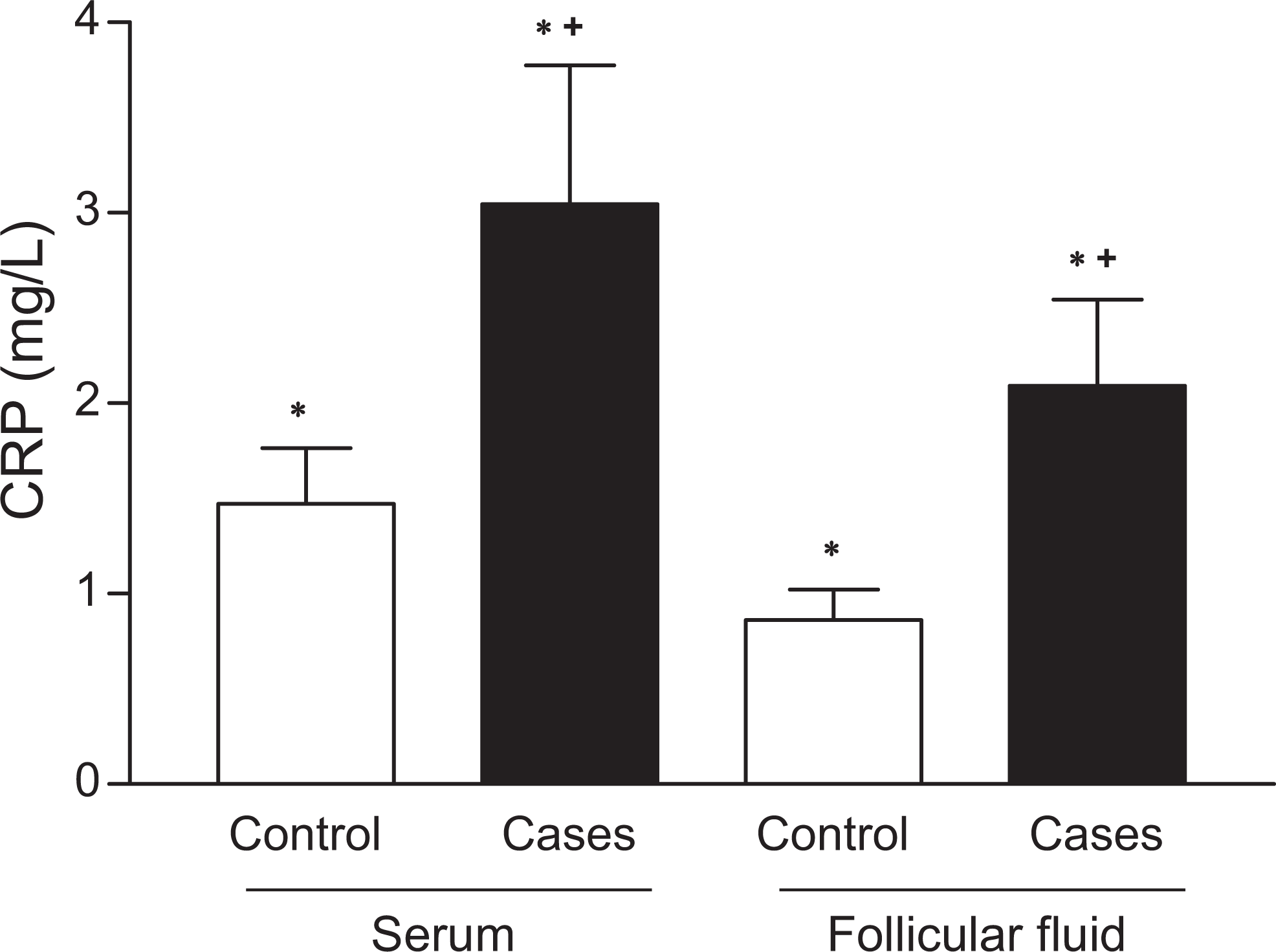
Evaluation of serum and follicular fluid CRP concentration in control group (n = 23) and in patients with chronic anovulation (n = 13). CRP indicates C-reactive protein. The data were analyzed using t Student paired and unpaired tests. Significance level was established at P < .05. *marks black bars (cases) that differ at P < .05 from controls and +marks follicular fluid bars that differ at P < .05 from serum.
Discussion
We report the activity of the inflammatory enzymes MPO and NAG in patients with infertility caused by chronic anovulation and normally ovulating women undergoing ICSI. To the best of our knowledge, no studies regarding the activity of these 2 enzymes in chronic anovulation have been published so far. No significant difference was observed between groups regarding age, duration of infertility, or BMI. Patients with chronic anovulation showed as expected higher basal LH, more antral follicles, and larger ovarian volume prior to COH compared with normally ovulating women. In addition, there was no significant difference concerning the amount of hMG units used, number of oocytes retrieved, number of mature oocytes (MII), number of embryos transferred, and fertilization rates between the groups under study
Determination of the follicular fluid composition may not only lead to an improved understanding of ovarian physiology, especially in regard to follicular development and oocyte maturation, but also offer new possibilities of using selected markers to optimize COH during IVF. 22
The reason for focusing on women undergoing ICSI was the opportunity to study follicular aspirates. The substances present in human follicular fluid, which originate from plasma or are produced by follicular structures, reflect oocyte maturation and can be used to assess oocyte quality. Many cytokines are crucially important for reproductive processes, such as follicular development, ovulation, fertilization, implantation, and embryonic development. The role of cytokines in the function of female reproductive system has been broadly investigated during COH for IVF; and it seems that under COH, the functions of the female reproductive system differ from those of natural cycles. 15 ,29 Thus, the composition of follicular fluid reflects stages of oocyte development by producing indirect biochemical mediators associated with ovarian events including the regulation of steroidogenesis, endothelial injury, local vascular permeability, extracellularmatrix remodeling and cellular proliferation, angiogenesis, and inflammatory activity. 30
Myeloperoxidase is a key enzyme and established marker of oxidative stress. In the present investigation, patients with chronic anovulation showed a lower MPO serum activity and a higher MPO activity in follicular fluid by comparison with normally ovulating women (control group). Furthermore, the higher the number of oocytes retrieved, the higher the MPO serum activity in both groups. Such data suggest that anovulatory patients may have a higher activation of neutrophils in the ovaries, corroborating the hypothesis of higher local inflammatory response, with a higher ovarian response at the time of gonadotrophin stimulation. However, a pilot study evaluating MPO activity in cumulus cells from IVF patients showed that the concentration of MPO varied inversely with the estradiol concentration. 31 The results of this study contradict the inflammatory hypothesis in ovarian response.
N-acetylglucosaminidase, a lysosomal enzyme, has been employed to monitor macrophage accumulation/activation in a variety of animal and human tissues. NAGase is released into some fluids from neutrophils during phagocytosis and cell lysis, and to some degree, by damaged epithelial cells. It accurately reflects the degree of inflammation. As ovulatory abnormalities may have a significant basis in inflammation, it was chosen to test the hypothesis that there is an altered inflammatory response in patients with chronic anovulation in an attempt to search for other cellular markers of an altered inflammatory response in these women. Follicular NAG activity was higher in anovulatory patients when compared with those with normal ovulatory cycles as expected since these women show low-grade inflammation. 18 Increased NAG activity however was not associated with a higher number of oocytes and mature oocytes (MII) retrieved, neither with the occurrence of OHSS nor with pregnancy. As far as we know, our study is the first to report NAG levels in the sera and follicular fluid of IVF patients. Follicular fluid is a product of both the transfer of blood plasma constituents that cross the blood follicular barrier and of the secretory activity of granulosa and thecal cells. Thus, some biochemical characteristics of the follicular fluid surrounding the oocyte may play a critical role in determining oocyte quality and the subsequent potential to achieve fertilization and embryo development. 32 Leukocytes are known to be involved in ovarian regulation by secreting local modulator substances. 33 According to literature data, follicular development and features of the resulting ovary after gonadotrophin stimulation might also modify the pattern of migratory inflammatory cells. 34 Our results have shown a higher level of indirect macrophage local activity in women with chronic anovulation with no further consequences for pregnancy rates or complications in both groups. Such data corroborate the evidence that cellular interactions between the ovary and immune system play a key role in the ovarian cycle, mainly in follicular development and ovulation. 35 Considering the fact that the patients under ovarian hyperstimulation tend to show higher response due to a large follicular pool of oocytes, an increased local inflammatory response was expected. There is a considerable population of macrophages (5%-15% of the cells) within the human ovarian follicle at the time of ovulation, but the role of macrophages in ovarian physiology remains to be established. 36
Serum and follicular levels of MCP-1 showed no significant difference between the groups studied and were not correlated with reproductive outcomes such as pregnancy rates or further complications from COH. Monocyte chemoattractant protein 1 is an important modulator of periovulatory events by attracting and activating macrophages. 37 Such chemokyne in follicular fluid from patients undergoing IVF has been regarded as a possible molecular marker of oocyte maturation. 37 Other investigations have shown that there is a higher expression of MCP-1 in follicular stroma during the ovulatory period in stimulated and natural cycles, which supports the evidence of an undeniable inflammatory response during such phase. 38
The role of chemokines in chronic anovulation has been deeply investigated, but the results remain controversial. 39 These studies showed no significant difference in messenger RNA (mRNA) expression in follicular fluid of colony-stimulating factor 1 (CSF-1), granulocyte–macrophage (GM)-CSF, IL-1b, IL-6, IL-8, and IL-10, MCP-1, and TNF-α from patients with polycystic ovaries undergoing IVF when compared with normally ovulating women. 40 Another study evidenced that serum levels of chemokines such as MCP-1, macrophage inflammatory protein 1α (MIP-1α), and migration inhibitor factor (MIF) were significantly increased in obese patients with polycystic ovaries. 41
In the present investigation, patients with chronic anovulation showed a higher CRP dosage in both follicular fluid and serum. Some studies have suggested that women with PCOS who were not submitted to COH showed a higher serum level of CRP in comparison with those with regular ovulatory cycles. 42 Levin et al reported that high CRP levels during IVF stimulation were associated with failure of conception. 43 Conversely, others found that CRP measurements were not a predictive marker of IVF success. 13 ,15 A study carried out by Orvieto et al encountered higher serum levels of CRP in women after hCG administration, suggesting an association between ovarian hyperstimulation and systemic inflammatory response. 15 C-reactive protein has also been described as a potential indicator of OHSS severity. 44
The relationship between chronic anovulation, risk of OHSS, and a possibly altered systemic inflammatory response remains unclear. 45 Our results have shown a significant association between MCP-1 levels and the occurrence of OHSS. Traditional monitoring of COH during IVF treatment includes ultrasonography plus measurement of serum estradiol levels in order to reduce the incidence and severity of complications such as OHSS, but a reliable marker of OHSS has not been established so far. 46 To date, there is no literature evidence of neither follicular nor abnormal serum levels of MCP-1 being correlated with OHSS. The presence of MCP-1 in the follicular fluid of patients with OHSS might be affected by ovarian intrinsic factors that are released by either its increased volume size or the presence of other chemokines.
The present study has shown a significant association between CRP levels and the occurrence of OHSS, corroborating other investigations. 43 Such association might be due to the acute inflammatory response encountered in OHSS complications. C-reactive protein has a proinflammatory activity and is directly able to activate endothelial cells, induce the synthesis of tissue factors and release of chemokines by monocytes, as well as increase plasminogen activator inhibitor 1 expression. 47 C-reactive protein may also play a role in endothelial cell activation, inflammation, and thrombotic conditions. 48
Our results allow us to conclude that infertile patients with chronic anovulation showed higher macrophage and neutrophil activation in follicular fluid when compared to the control group. This increased inflammatory response however did not appear to influence IVF results. Serum levels of CRP and MCP-1 follicular fluid concentration were inflammatory modulators correlated with OHSS. Leukocyte subtypes are clearly involved in ovulation, but their exact roles in ovarian physiology remains limited. Knowledge about the activity of these cells and their by-products in ovulation may be important to understand the ovulatory process in natural and stimulated cycles. Further clinical studies including larger series of patients and their follow-up could establish the interplay of leukocytes and their by-products in ovarian function/ovulatory process and thus define the real importance of inflammatory markers in infertile patients with chronic anovulation as well as possible markers for oocyte quality and competence.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.