
Abstract
The utility of cancer antigen 125 (CA-125) levels as an adjunct method of monitoring patients with uterine papillary serous carcinoma (UPSC) or endometrial serous carcinoma after surgery and adjuvant treatment has been reported. Our goal was to determine the significance of rising CA-125 levels within the normal range in these patients in the posttreatment surveillance setting. All patients with UPSC who underwent surgical staging and had preoperative CA-125 measurement from 1999 to 2008 were included in this analysis. Information was extracted from records to assess the changes in CA-125 values with clinical and/or radiographic detection of recurrence. Of the 56 evaluable patients, 23 (41%) recurred. Of the 23 patients that recurred, 11 had serial CA-125 levels measured in remission. Elevated CA-125 levels at diagnosis were significantly associated with disease recurrence and advanced stage (P = .01, P = .001, respectively). The rise in CA-125 by 10 U/mL in the normal range and ≥15 U/mL were associated with disease recurrence (P < .001, P < .001, respectively). In multivariate analysis, only CA-125 level ≥15 U/mL was significantly associated with worse progression-free survival. In this small cohort of patients with recurrent UPSC after remission, surveillance of CA-125 levels may have a role in disease surveillance and management.
Introduction
Endometrial cancer remains the most common gynecologic malignancy in women in the United States. 1 In 2012, approximately 47 130 new cases and 8010 deaths are estimated to occur from the uterine corpus. 2 The rate of endometrial cancer continues to rise and the increase in mortality may be related to the increased rate of advanced-stage cancers at the time of diagnosis. High-risk histology such as uterine papillary serous carcinoma (UPSC) or endometrial serous carcinoma is associated with advanced stage at diagnosis and poor prognosis and survival.1,3,4 While UPSC represents only 10% to 15% of all endometrial cancer diagnosed in the United States, it accounts for up to 39% of endometrial cancer-related deaths.1,3–5 When compared with the more common endometrioid adenocarcinoma of the endometrium, patients with UPSC often present with extrauterine disease at time of diagnosis and have an overall poorer prognosis with a predilection for distant metastasis and recurrence.1,3,4
The serum marker cancer antigen 125 (CA-125) has been shown to be useful for monitoring therapeutic response and in the surveillance of patients with epithelial ovarian cancer (EOC). 1 In endometrial cancer, CA-125 has been correlated with extrauterine disease and is associated with survival.6–8 However, these studies included all histologic subtypes of endometrial carcinoma. The clinical and histological similarities between UPSC and EOC have led investigators to study the potential role of CA-125 to evaluate disease status in women with UPSC. 1 To date, several studies have established a correlation between preoperative levels of CA-125 and presence of extrauterine disease at the time of surgery as well as advanced International Federation of Gynecology and Obstetrics (FIGO) stage in women with UPSC.9–11 Moreover, CA-125 has been shown to be correlated with survival in this aggressive disease.10–12
For patients with EOC undergoing treatment, the commonly used Gynecologic Cancer Intergroup definition of disease progression based on CA-125 alone involves at least doubling of the upper limit of the normal CA-125 value (laboratory dependent but commonly set as 35 U/mL) or doubling of the nadir CA-125, dependent upon whether the baseline CA-125 value normalizes during treatment or not. 13 More recently, different nadir values and trends of elevated CA-125 values within the normal range have been shown to be prognostic of recurrence and survival in patients with ovarian cancer.14–18 The objective of our study was to evaluate the clinical significance of rising CA-125 levels within the normal range (≤35 U/mL) in patients with UPSC.
Methods
Using a prospectively maintained institutional endometrial cancer database, all patients with the histologically confirmed diagnosis of UPSC between 1999 and 2008 were identified. All patients underwent comprehensive surgical staging and cytoreduction and received adjuvant treatment at the Albert Einstein College of Medicine/Montefiore Medical Center. Patient records were reviewed for age, body mass index, race, stage of disease, survival, and recurrence. The CA-125 values were screened for availability on all patients from the time of diagnosis to recurrence or the last clinical follow-up. All CA-125 levels were measured at our institution utilizing the IMMULITE 2000 OM-MA, which is a solid-phase, 2-site chemiluminescent–immunometric assay, and a first-generation CA-125 detection system. This assay utilizes a murine monoclonal antibody for the capture and a rabbit polyclonal antibody for detection of the CA-125 antigen. Fifty-six patients met the above criteria and had serially recorded CA-125 levels. In general, CA-125 levels were measured preoperatively, then after every cycle of chemotherapy, followed by every 3 to 6 months during remission. The upper limit of normal for CA-125 is 35 U/mL. The CA-125 levels >35 U/mL at time of diagnosis divided the patients into marker positive (MP) and marker negative (MN) groups.
All the patients with serial measurable CA-125 values monitored during their remission period were included in the analysis. Baseline CA-125 level was defined as the nadir level in remission. Trends of interest included increase in CA-125 levels by 10 U/mL from the nadir levels and CA-125 ≥15 U/mL while in remission.
Statistical Analysis
Categorical data were compared using Fisher exact test. Continuous data were compared between groups using the Mann-Whitney U test with the knowledge that the distributions between groups were similar and a location shift would determine a difference between groups. Difference in survival was displayed using Kaplan-Meier methodology, and Cox-Proportional Hazards model was used for multivariate regression in survival. Proportions were estimated using a Bayesian Frame work, where the data were distributed according to the binomial model and the proportion was distributed according to the β distribution, using Jeffery noninformative prior. All statistical analysis was performed using R v 2.12.2.
Results
Out of the 165 patients with UPSC screened within this time period, a total of 56 eligible patients were identified with a mean follow-up of 51 months. Twenty-three patients (41%) developed recurrence of UPSC with a mean interval of 21 months, and 11 (19%) of the 23 patients that recurred had serial CA-125 levels followed during remission. Demographic data are presented in Table 1. Patients were divided into 2 groups the recurrence group, which included those with documented radiographic and/or clinical/histological evidence of recurrent disease after a period of documented clinical remission, and the nonrecurrent group. As expected, patients with stage III/IV disease were more likely to recur when compared to patients with stage I/II disease (P < .001). Overall, the distribution by stage of patients in this study was similar when compared to a historical review of patients with UPSC—31 (55.4%) with disease limited to uterine corpus, 7 (12.5%) with stage II disease, 12 (21.4%) and 6 (10.7%) with stages III and IV disease, respectively. Treatment was significantly different among the 2 groups. Specifically, 94% of the patients in the nonrecurrent group received combination of platinum- and taxane-based chemotherapy with radiation therapy, compared to 60.9% in the recurrent group (P ≤ .001).
Patient Characteristics.
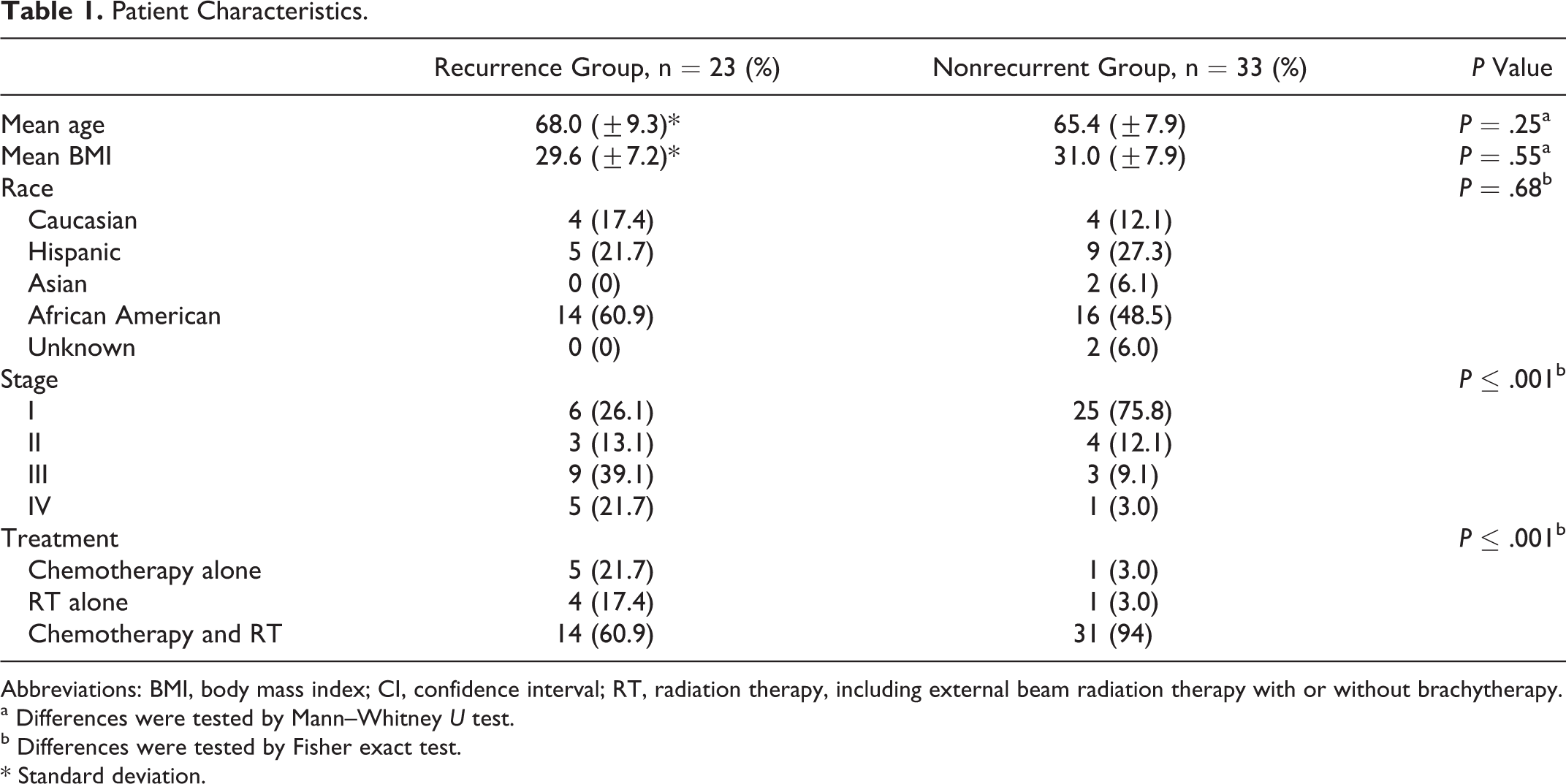
Abbreviations: BMI, body mass index; CI, confidence interval; RT, radiation therapy, including external beam radiation therapy with or without brachytherapy.
a Differences were tested by Mann–Whitney U test.
b Differences were tested by Fisher exact test. * Standard deviation.
Next, we analyzed the association between the marker status at time of diagnosis and stage of disease (Table 2). Of the 56 patients, 14 patients (25%) were MP and 42 (75%) were MN at the time of diagnosis. Of the MP patients, 10% or 71.4% presented with advanced stage disease, stages III and IV, while the majority of MN patients, 34 (80.9%) had early stage disease. Marker positivity at the time of diagnosis was significantly associated with advanced stage of disease, P < .001. Table 2 also highlights the association between marker status and disease recurrence. Of the 23 patients that recurred, 10 (43.5%) were MP and 29 (87.9%) in nonrecurrent group were MN. Therefore, elevated CA-125 levels at the time of diagnosis were significantly associated with disease recurrence (P = .01).
Association Between Stage and Disease Recurrence With Marker Status at Diagnosis.a
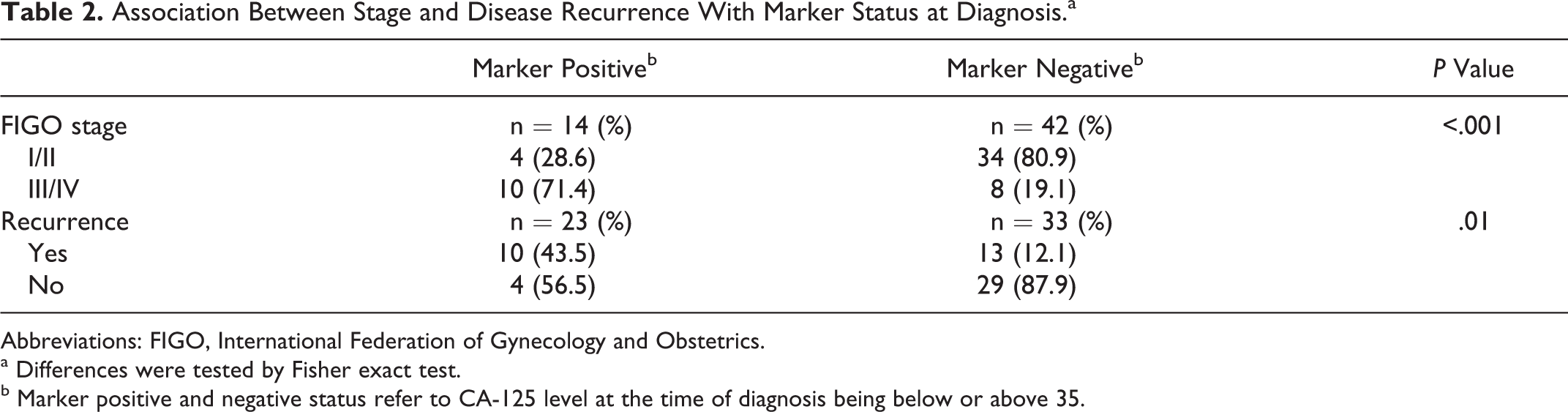
Abbreviations: FIGO, International Federation of Gynecology and Obstetrics.
a Differences were tested by Fisher exact test.
b Marker positive and negative status refer to CA-125 level at the time of diagnosis being below or above 35.
Focusing our analysis on the subgroup of patients that recurred, we analyzed the trends of rising CA-125 levels within the normal range and its clinical implications during remission. Of the 23 patients in the recurrent group, 11 or 48% had serial CA-125 levels followed during remission and remained within the normal range, while others quickly rose above 35 U/mL and were therefore not included in this subgroup analysis. Of the 11 evaluable patients, 6 were MP and 5 were MN at the time of diagnosis. The mean nadir during remission in the recurrent group was 8.1 (SD ± 5.0) U/mL as compared to 4.5 (SD ± 2.7) U/mL in the nonrecurrent group. The CA-125 levels were followed in the remission period with a median frequency of 6, with a range of 2.4 to 32.3 U/mL in the recurrent group and 1 to 17.2 U/mL in the nonrecurrent group. In the recurrent group, 7 or 63.6% had CA-125 levels rising by 10 U/mL while staying within the normal range compared to 1% or 3.0% displaying similar trend in the nonrecurrent group (P < .001). Moreover, 10 or 90.9% of patients in the recurrent group had an absolute rise ≥15 U/mL versus 1 or 3.0% in the nonrecurrent group, P < .001. The rise of CA-125 ≥15 U/mL preceded clinical detection of recurrence by a mean of 4.2 months (range 1.2-8.9 months).
To compare the distribution of patients with normally rising CA-125 levels in the recurrent and nonrecurrent groups, we performed mean proportions testing (Figure 1A and B). The mean proportion of patients in the recurrence group with CA-125 values rising by 10 U/mL was 83.3% (95% confidence interval [CI]: [54.6, 98.6]). In those patients who remained in remission (nonrecurrent group), only 16.7% (95% CI: [1.4, 45.4]) of this cohort had a similar trend of rise in CA-125. The difference is significant when modeling the data under the Bayesian framework and using classical statistics as measured by chi-square analysis (P < .001). Furthermore, the mean proportion of patients in the recurrence group with CA-125 values rising ≥15 U/mL is 87.5% (95% CI: [64, 99.0]) and only 4.4% (95% CI: [0.3%, 13.3]) in patients who remained in remission, indicating that a rise by 10 U/mL or an absolute value of ≥15 U/mL was significantly associated with recurrence of disease (Figure 1C and D).
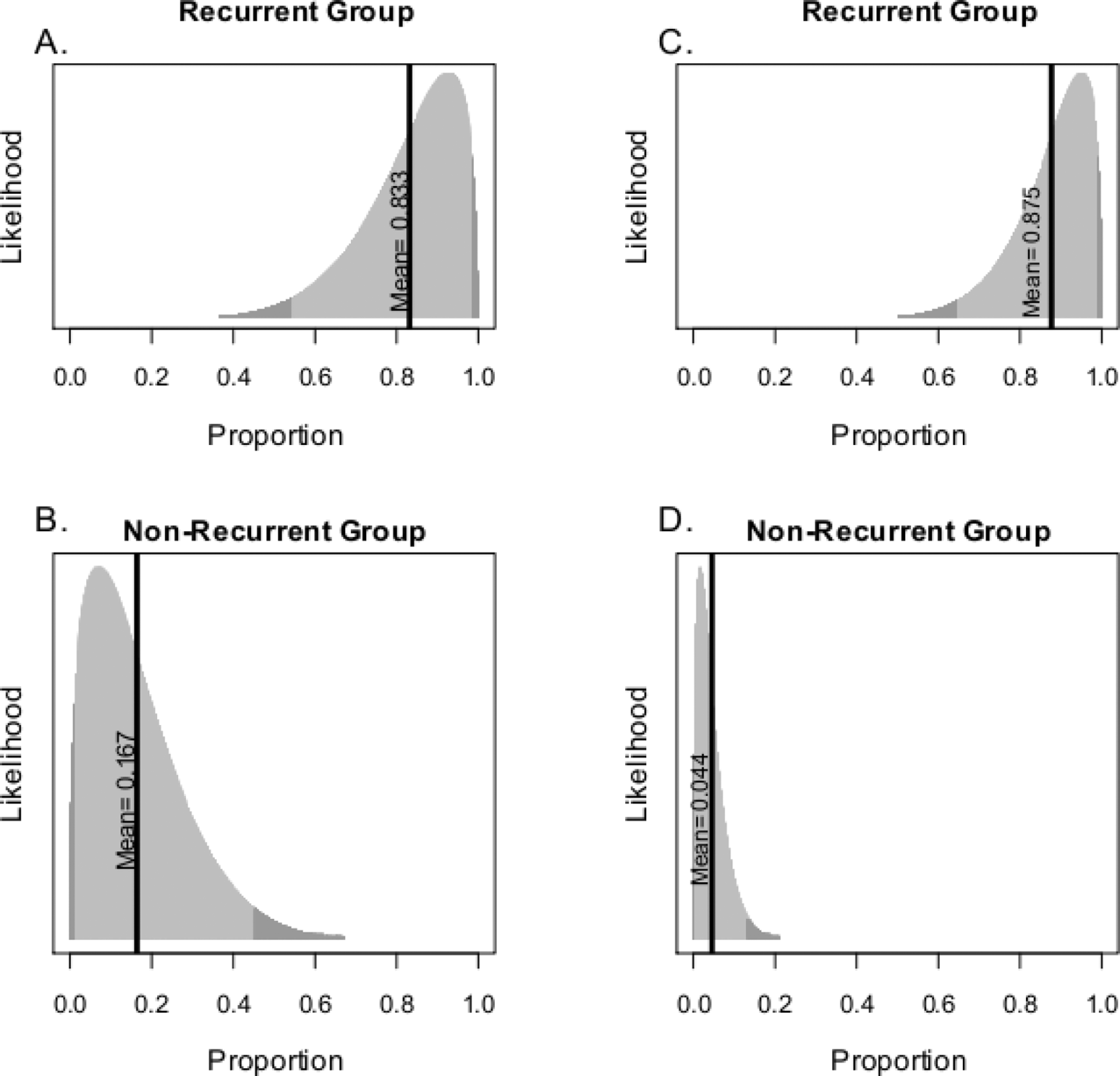
The proportion of patients with CA-125 values rising by 10 U/mL (A and B) and CA-125 ≥15 U/mL (C and D), with or without recurrence. The data were modeled under the Bayesian framework.
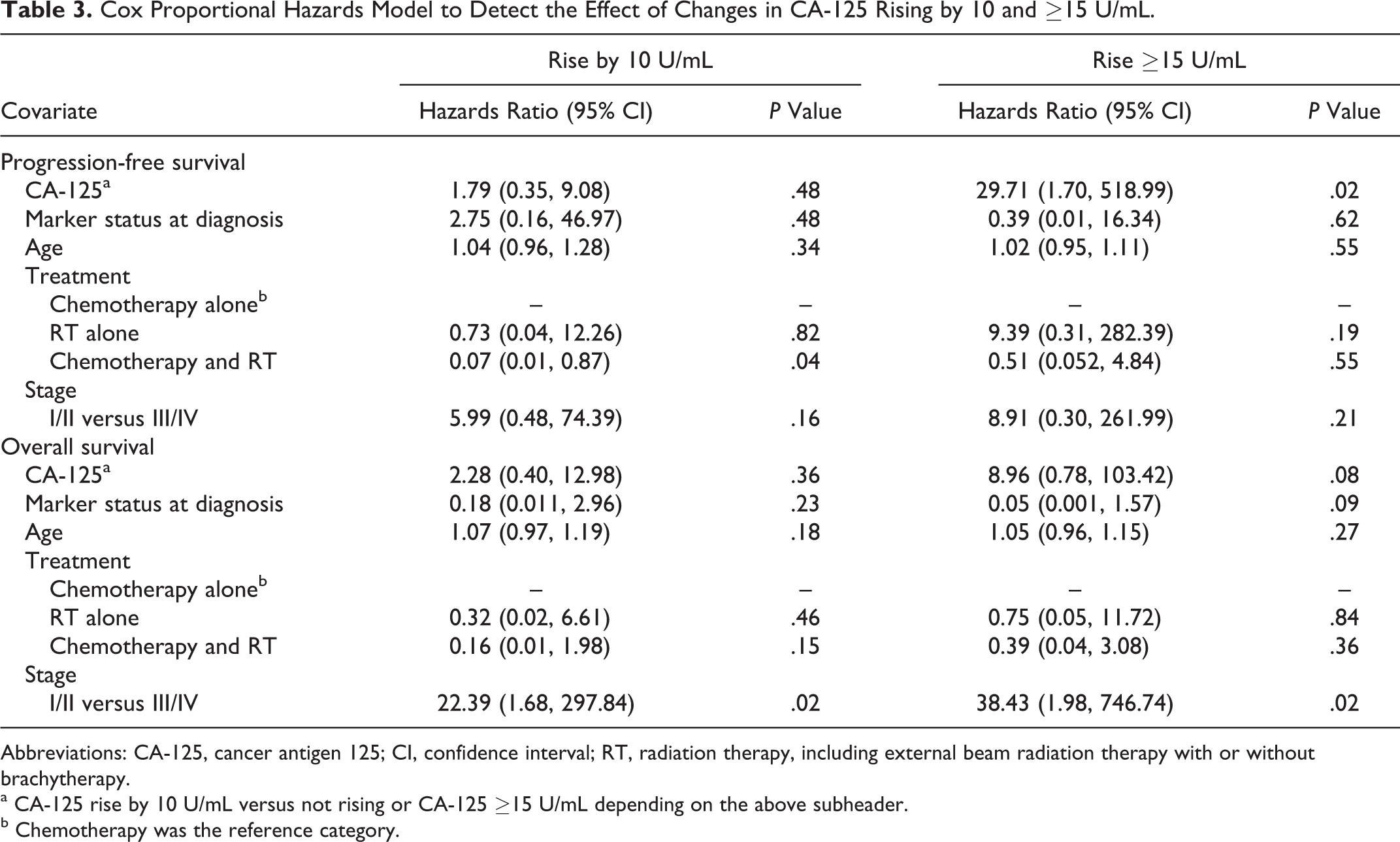
Finally, Kaplan-Meier survival curves were constructed to demonstrate the progression-free survival and overall survival (PFS and OS). Figure 2 displays the Kaplan-Meier survival curves in patients with and without the specific pattern of change in CA-125 during remission (specifically, a rise in CA-125 levels by 10 U/mL or rising ≥15 U/mL). In Figure 2A and B, both PFS and OS in the patients with a rise by 10 U/mL are lower past 20 months. The median and 95% CI of PFS and OS for patients rising by 10 U/mL are 26.9 months (24.3, -) and 35.5 (35.2, -), respectively, while the median value is not obtained for the patients whose CA-125 levels stayed within the nadir range and did not rise by 10 U/mL. Looking at patients with CA-125 values ≥15 U/mL, similar trends are apparent (Figure 2C and D). The median and 95% CI for PFS and OS in this group are 24.3 months (16.5, -) and 35.5 months (26, -), respectively. A Cox regression analysis showed that patients with CA-125 value ≥15 U/mL is independently associated with worse PFS (hazards ratio [HR]: 29.71, P = .02) and nearing significance for OS (8.96, P = .08) while controlling for potential confounders, including age, marker status at diagnosis, treatment, and stage of disease (Table 3). Furthermore, patients with advanced stage disease (stage III/IV) were independently associated with worse OS when their CA-125 values rose by 10 U/mL, as well as when their CA-125 rose above 15 U/mL (HR = 22.39, P = .02 and HR = 38.43, P = .02, respectively).
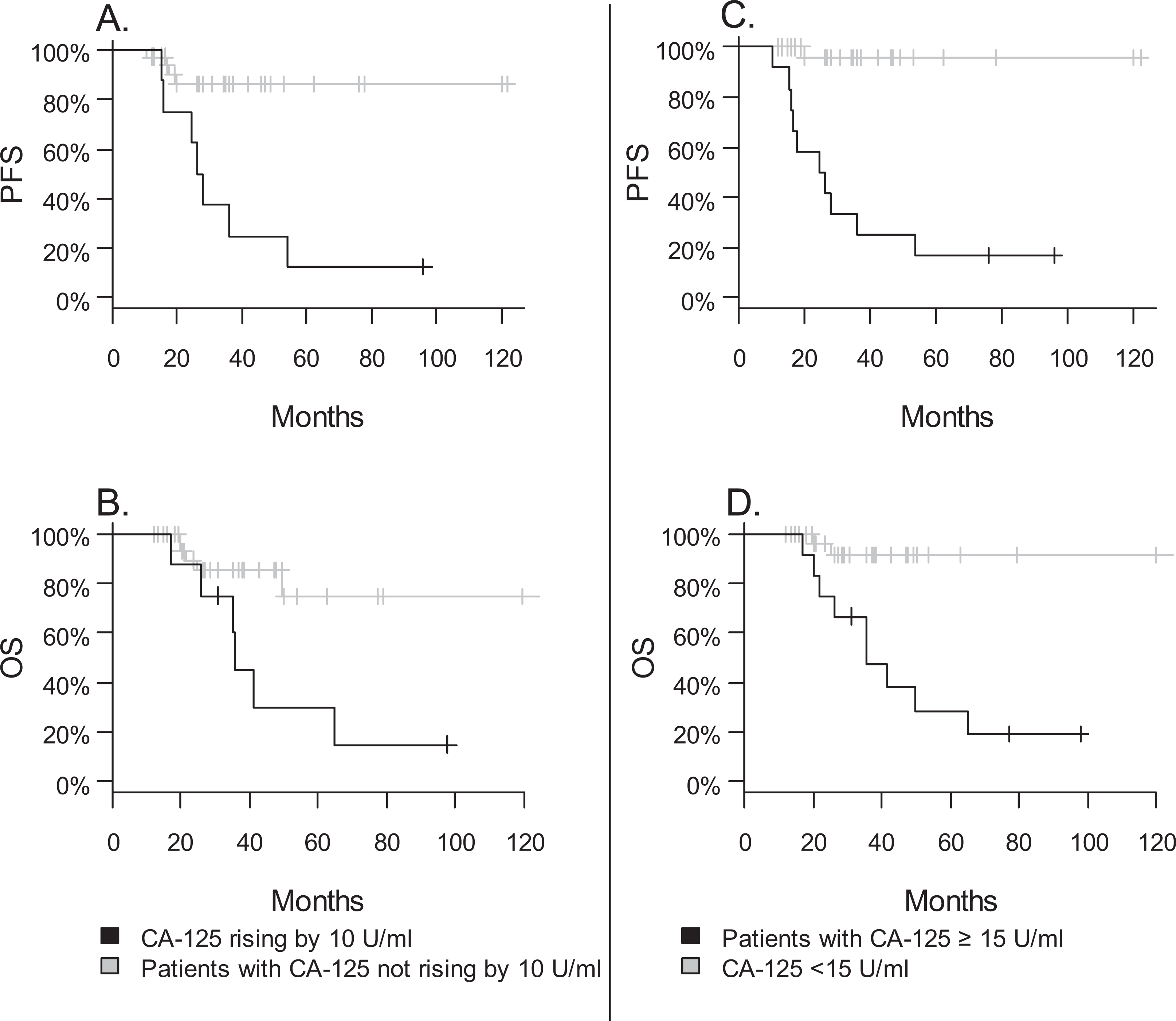
Kaplan-Meier plots of progression-free survival (PFS) and overall survival (OS) between patients who had a rise by 10 U/mL (A and B) and ≥15 U/mL (C and D) and those who did not. PFS indicates progression-free survival; OS, overall survival.
Cox Proportional Hazards Model to Detect the Effect of Changes in CA-125 Rising by 10 and ≥15 U/mL.
Abbreviations: CA-125, cancer antigen 125; CI, confidence interval; RT, radiation therapy, including external beam radiation therapy with or without brachytherapy.
a CA-125 rise by 10 U/mL versus not rising or CA-125 ≥15 U/mL depending on the above subheader.
b Chemotherapy was the reference category.
Discussion
UPSC is a clinically and pathologically distinct subtype of high-risk endometrial cancer. Chemoresistance and the poor prognosis with recurrent disease highlight the need for careful surveillance following treatment and a need to identify a biomarker of disease recurrence or progression. This led us to explore the potential role of serum marker CA-125 in the posttreatment surveillance setting in patients who were in clinical remission.
To date, there have been numerous reports establishing CA-125 as a useful marker in both the preoperative setting and surveillance of women with endometrial cancers. 11 In UPSC, CA-125 has been shown to be a useful prognostic marker, as preoperative values have been shown to correlate with stage, and tumor burden.11,12 Its association with disease recurrence and treatment outcome has not been consistently shown, with some reports correlating a rising value of CA-125 with disease recurrence and independently with survival, while others failed to make that association.9–12
While monitoring serum CA-125 values is widely accepted in patients with EOC, there is only one other study that evaluates the utility of monitoring CA-125 in patients with UPSC postsurgery. 10 Our report is also the first study evaluating the clinical significance of rising CA-125 levels within the normal range (0-35 U/mL) in patients with UPSC in clinical remission. These data contribute to the existing literature on the utility of CA-125 as a prognostic marker. Consistent with literature, we showed that abnormal CA-125 levels at the time of diagnosis (>35 U/mL) are significantly associated with advanced stage (FIGO III and IV) and disease recurrence. Our data also suggested changing patterns of CA-125 serum values within the normal range, specifically rising by more than 10 U/mL, or having an absolute value greater than 15 U/mL, are associated with recurrence. Serum CA-125 ≥15 U/mL during the remission period preceded clinical detection of disease recurrence by approximately 4 months. Furthermore, we have shown that irrespective of preoperative CA-125 values, rising CA-125 value ≥15 U/mL is independently associated with worse PFS. While OS survival is not statistically associated with this pattern of change in CA-125, it is worthwhile to note that due to the retrospective nature of this study, a value ≥15 U/mL, if within the normal range, did not trigger earlier management for possible recurrence. These findings suggest that small alterations in CA-125 levels in patients in remission may be predictive of disease recurrence and worse prognosis.
Our study has several limitations. This is a retrospective review of a single institutional experience and includes a small number of patients that may reflect a selection bias that may be reversed by a prospective, large, randomized cohort. Although small, our numbers are comparable to the few existing publications on this subject with a similar distribution of patients by stage as compared to a historical review. 1 Given the inconsistency of CA-125 levels recorded in patients during the remission period, we were unable to evaluate all of our patients who experienced disease recurrence. This highlights a lack of consensus among gynecologic oncologists in recognizing the utility of CA-125 in UPSC surveillance, even within a single institution and further emphasizes the importance of research efforts devoted to surveillance of UPSC. Recently, EORTC 55955, which randomly assigned 559 women with EOC in clinical remission to early treatment or delayed treatment groups after their CA-125 levels exceeded twice the upper limit of normal, reported their finding that early treatment based on biochemical rise in CA-125 solely did not impart a survival benefit. 19 While we recognize the importance of these findings, we believe that our study still holds value. The strength of our study lies in the fact that all patients had comprehensive surgical staging of disease, with central pathologic confirmation of the histology, as well as similar treatment strategy involving platinum and taxane-based chemotherapy with or without radiation. Given the practice pattern in the United States, the majority of the providers and their patients still look to CA-125 to predict disease response in patients with EOC, as well as diseases with a similar clinical course, such as UPSC.
While the disease biology of UPSC remains to be fully elucidated and the clinical significance of “early detection” of recurrence is unclear, findings of “normally” rising CA-125 levels may prompt a discussion between the provider and the patient, leading to an “individualized” treatment plan. Current literature suggests that type II uterine cancer displays a unique molecular signature when compared to type I endometrial cancer, involving higher percentage of p53 mutations, loss of e-cadherin expression, as well as overexpression of Her2/neu. Her2/neu specifically has been studied as a potential target in the treatment of patients with UPSC. Although a multiinstitutional phase II trial (GOG 181b) evaluating single-agent herceptin did not show significant single-agent response in patients with Her2+ endometrial cancer, anti-her2/ neu strategies are currently undergoing evaluation in combination strategies with cytotoxic regimen in phase II trials. Pending the results of these clinical studies, drugs targeting overexpression of Her2 receptors may be considered as a potential adjunct to salvage regimen for patients with recurrent, Her2+ UPSC. 20
In summary, although limited in number, our current findings show that specific trends of rising CA-125 within the normal laboratory range may be clinically significant and precedes disease recurrence. Given the aggressive nature of this tumor, and the lack of other efficacious biomarkers, we recommend monitoring CA-125 in conjunction with history and physical examination during routine office visits for patient follow-up. Our results suggest a potential role for CA-125 to be used as a monitor of surveillance for patients with UPSC in clinical remission.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.