
Abstract
Preterm birth is defined as birth before 37 weeks’ gestational age. With an incidence of 7% to 11%, it is one of the major causes of perinatal mortality and morbidity. Preterm birth is considered a clinical syndrome, which arises from different pathological processes that activate prematurely one or more components of the mechanisms leading to parturition. The premature activation of labor may be caused by multiple pathological conditions; in particular a deregulation of the immune system and an exaggeration of inflammatory processes represent common central mechanisms. The complex pathogenesis, the main risk factors and the different therapeutic options will be described in the present review. Since its incidence is still increasing in the last decades, the goal is to improve the primary and secondary prevention.
Introduction
Preterm birth (PTB) is defined as birth before 37 weeks’ gestational age, occurs with an incidence of 7% to 11%, and is the major obstetric syndrome because it the most important cause of perinatal mortality and morbidity. 1
On the basis of the clinical presentation, PTB can be phenotypically classified as (i) spontaneous PTB (sPTB) when preterm labor (PTL) onsets spontaneously, (ii) preterm prelabor rupture of membranes (pPROMs), and (iii) iatrogenic PTB (iPTB) when delivery is indicated for pregnancy complications. 2 The first 2 clinical conditions are often combined. A new classification system is under construction in order to better define the PTB and to present a prototype to be used worldwide; 3 since it is not yet defined, the above mentioned will be presently used. 4
The complex etiopathogenesis of sPTB is still unclear, but it is almost accepted that sPTB may be considered a clinical syndrome arising from different pathological processes that activate prematurely one or more components of the mechanisms leading to parturition. 5 Therefore, term birth and sPTB are fundamentally the same process except for the gestational age at which they occur and share a “common pathway.” The uterine components of this pathway include (i) triggering of myometrial contractility; (ii) cervical ripening (dilation and effacement); and (iii) decidual/membrane activation. 5 In this scenario, mechanical and endocrine mechanisms, immune system responses, inflammatory signals, and release of several molecules such as cytokines, prostaglandins (PGs), and oxytocin (OT) contribute among others to the activation of contractions in human uterus. 6
Understanding the Mechanisms of Myometrial Contractions at the Time of Labor
The exact sequence of events leading to the onset of human labor is not known completely but the transition from myometrial quiescence to activation of myometrial contractility represents a central phenomenon. Interestingly, the uterus lacks a pacemaker that regulates contractions: indeed, the uterine myometrium is capable of converting a tissue with relatively low connectivity between individual myocytes into a tissue with extensive physical connections, thus permitting the transmission of contractility from a triggering point to the full organ. 7
During labor, the critical aspect represented by the synchronous activity of myometrial cells alternated with periods of relaxation 8,9 is regulated both by the presence of connections between muscular cells and by the release of some important mediators.
Regarding mechanical implications of muscular cells, it is well known that during labor, myometrial cells are connected by gap junctions that are created by multimers of connexin 43, thus promoting myometrial contractions. 6 The presence of these junctions contributes in achieving coordinated and synchronous myometrial contractions. Connections between myocytes during labor are also formed by paracrine release of PGs and local release of calcium. Prostaglandins are of primary importance in the initiation and maintenance of labor in humans. A major intrauterine source of PGs is amnion, which synthesizes increased amounts of PGE2 at term labor.
In fact, PGs are well known to be stimulators of myometrial contractions, by the activation of the phosphatidylinositol signaling pathway resulting in the generation of cytosolic calcium oscillations. 10 Moreover, PGE receptors have been reported to activate multiple second messenger pathways, including modulation of adenylate cyclase activity, inositol phosphate production, and regulation of cytosolic calcium. 11
On the other hand, an increased release of intracellular calcium has been shown to lead to uterine contractility by promoting myosin–actin interactions. 7 Actin and myosin represent the so-called contraction-associated proteins and their interaction determines myocyte contractility. 12 In order to make this interaction possible, actin must be converted from a globular form to a filamentous form, and it must also attach to the cytoskeleton at focal points in the cell membrane; this attachment allows the development of tension and these focal points connect the cell to the underlying matrix. 13,14 Actin partner, myosin, is activated when it is phosphorylated by myosin light-chain kinase and activated by calmodulin and increased intracellular calcium. 15 Therefore, it is clear that these events are mutually reinforcing.
A key role is played by OT, a nonapeptide secreted by hypothalamus but also synthesized by placenta and amnion. 16 The OT locally produced in the placenta is likely to be more important than circulating OT for the mechanism of labor, increasing connexin 43 levels and upregulating morphologic gap junctions. 17 In this way, OT promotes myometrial contractility by increasing the intracellular calcium and the production of PGs, by binding OT receptors in myometrium whose expression increases during labor. 18 Indeed channels through which calcium is released open when an activating ligand reduces the electrochemical gradient across the myocyte membrane. These ligand-regulated channels, which release calcium from intracellular stores, are activated by PGs and OT, which in turn activate some membrane proteins, Gαq, linked to enzymatic cascade. The most important enzyme is represented by phospholipase C that when it is activated in turn activates protein kinase C and releases inositol triphosphate. Protein kinase C probably activates myosin light-chain kinase, and inositol triphosphate releases calcium from intracellular stores. 19 But in the myocyte membrane, there are systems that promote relaxation through Gα2 pathways that oppose these pathways by increasing intracellular cyclic adenosine monophosphate (cAMP) and activating protein kinase A. These enzymes inactivate myosin light-chain kinase. During labor, a shift in the balance of these opposing systems promotes myocyte contraction. 20
The upregulation of proinflammatory cytokines within laboring myometrium stimulates and potentiates uterine contractions. 21 Among others, interleukin (IL)-1β induces basal and stores operated calcium entry in myometrial smooth muscle cells and together with tumor necrosis factor (TNF)-α stimulate arachidonic acid release and expression of cyclooxygenase (COX)-2, thus increasing PGs production in myometrial cell via greater nuclear factor kappa B (NF-κB) activity. 21 The NF-kB is a ubiquitous transcription factor that acts as a critical signal transduction pathway for regulating a variety of genes that are involved in immune and inflammatory responses, developmental processes, cellular growth, and apoptosis. 22 Activation of NF-kB in gestational tissues has been thought to be an integral part of the final phase of parturition and is involved in the biochemical changes associated with labor. 23
The critical “clock” underlying all these mechanisms is represented by hormonal changes crucial for the transition from myometrial quiescence to contractility. Progesterone and corticotropin-releasing hormone (CRH) have a critical role in pregnancy and labor. 6
Progesterone blocks myometrial contraction and maintains pregnancy, while its withdrawal transforms the myometrium to the laboring state, 6 remaining, however, at high levels throughout pregnancy and during labor. 24 In myometrium, there are 2 major isoforms of progesterone receptor, PR-A and PR-B, and their expression may contribute to the functional withdrawal of progesterone during labor. In myometrial cells during labor, the ratio of PR-A-PR-B in messenger RNA (mRNA) increases 2- to 3-fold compared with the nonlaboring state, mainly due to overexpression of PR-A. This change induces a “functional estrogen activation” through increased estrogen receptor expression. 25 In addition, PR-A are likely to suppress the transcriptional activity of PR-B, which is the main receptor for the nuclear signal transduction of progesterone. 26 Apart from myometrial contractions, the functional progesterone withdrawal may also contribute to the cervical changes during labor. 27
Placenta acts through CRH as a “clock” that controls the length of pregnancy and represents the main source of this neurohormone, acting via autocrine, paracrine, and endocrine mechanisms. 28 Corticotropin-releasing hormone is recognized as the hypothalamic neuropeptide that regulates the hypothalamus–pituitary–adrenal (HPA) axis in mammals, orchestrating neuroendocrine, autonomic, and immunologic responses to stress. During pregnancy, placenta represents the main source of CRH, acting via autocrine, paracrine, and endocrine mechanisms by playing a critical role in the maintenance of pregnancy via modulation of neuroendocrine and inflammatory events leading to physiological parturition or to sPTB. 29,30 Placental CRH stimulates adrenocorticotropic hormone (ACTH) production from placenta and fetal pituitary, that in turn stimulates fetal adrenals to produce dehydroepiandrosterone (DHEA), dehydroepiandrosterone-sulphate (DHEA-S), and cortisol, thus contributing to fetal stress axis activation and fetal lung maturation during parturition. 31 Placental CRH also exerts a direct effect by stimulating fetal adrenal zone cells via DHEA secretion and placenta estrogen metabolization that favors parturition. 32,33 Corticotropin-releasing hormone may also facilitate the expression of contraction-associated genes and may increase the myometrial response to PGs, modulating therefore the onset of labor. 34
Recently, it has been postulated that the molecular mechanisms subtending uterine contraction may differ, at least in part, between preterm and term labor. A recent study has attempted to differentiate at genomic level the molecular events that initiate and maintain myometrial activity in human labor at term and preterm. 35 Interestingly, a set of genes have been defined as the preterm initiator set, which also included the transporter, adenosine triphosphate (ATP)-binding cassette, subfamily A member 3 (ABCA3) whose protein is a member of the ABC1 subfamily. The function of ABCA3 in myometrium is unknown, but one possible role in the initiation of inflammation-associated sPTB could involve the exposure and presentation of potential antigens that trigger inflammation as a secondary response to the initiating event. 35 Moreover, it is becoming increasingly clear that the pattern of cytokine expression differs in preterm and term labor. 36 Therefore, cytokine expression may also differ among various tissues at different gestations myometrium. In fact, it was shown that levels of cytokines such as IL-1β, IL-6, and IL-8 were higher in term laboring myometrial samples than in PTL ones. 37 In conclusion, through gene profiling, a specific set of labor activation/repression genes (the effector gene set) has been identified, whose expression is unaffected by the timing of labor. In addition, while the effector gene set is unchanged by the gestational age at labor, sPTB and term labor differ dramatically in their initiator gene sets. 35 This findings are consistent with the suggestion that there are alternative pathways for preterm and term labor that trigger a common phenotype.
Etiopathogenesis of sPTB
Spontaneous PTB is characterized by a deregulation of the immune system and an exaggeration of inflammatory processes. 5
A precise pathogenetic mechanism cannot be established in most cases, but an increasing number of risk factors have been demonstrated to be associated with sPTB, by interacting to cause a transition from uterine quiescence to premature onset of sPTB or pPROM. 38
There are many maternal or fetal factors that have been associated with the risk of sPTB, 39 and they can be classified in periconceptional, obstetrics, or pregnancy associated. Risk factors include the following:
Periconceptional Socioeconomic characteristics: black women are 3 times more likely to have a PTL than women from other racial.
40
Low socioeconomic status, low and high maternal ages, and single marital status are associated with sPTB.
41
Nutritional status: a low body mass index (BMI), low serum concentrations of iron, folate, or zinc are associated with high risk of sPTB.
42
Stress: mothers experiencing psychological stress are at increased risk of sPTB, and a role of CRH is proposed.
31
Systemic diseases: thyroid diseases, asthma, diabetes, and hypertension, are associated with increased rates of sPTB.
43
Obstetrics Previous sPTB: the recurrence risk in women with a previous sPTB ranges between 15% and 50%, depending on the number and gestational age of previous deliveries, and the risk is inversely related to the gestational age of previous sPTB.
44
Interval between pregnancies: An interpregnancy interval of less than 6 months confers an increased risk of sPTB.
45
Previous uterine surgery: History of myomectomy, cervical cone biopsy, or loop electrocautery excision procedures have been associated with an increase in sPTB.
46
Smoke: Tobacco use increases the risk of sPTB. Both nicotine and carbon monoxide are powerful vasoconstrictors and are associated with placental damage and decreased uteroplacental blood flow, leading to fetal growth restriction and sPTB.
47
Pregnancy-associated risk factors Local or systemic infections: infections, such as pyelonephritis and asymptomatic bacteriuria, are associated with sPTB.
38
Periodontal disease has received widespread scrutiny, suggesting an increased risk independent of other factors.
48
Intrauterine infection: intrauterine infection is an important condition leading to sPTB and related to the activation of the innate immune system. The microorganisms most commonly reported are genital mycoplasmas.
49
the mechanism by which bacterial vaginosis is associated with sPTB is unknown, but microorganisms probably ascend into the uterus before or early during pregnancy.
50
Multiple pregnancy: multiple gestations carry a risk of sPTB and result in 15% to 20% of all sPTB. Uterine overdistension, resulting in contractions and pPROM, is the causative mechanism for the rate of increased risk.
51
Cervical shortening and insufficiency: cervical shortening is a risk factor for sPTB. So, the shorter the cervix, the greater the risk of sPTB.
52
Vaginal bleeding: vaginal bleeding caused by placental abruption or placenta praevia is associated with a very high risk of PTL.
53
The premature activation of labor may be caused by multiple pathological conditions, like (i) intrauterine infection, (ii) stress and immune disorders, (iii) genetic risk factors, (iv) uteroplacental insufficiency, (v) uterine overdistension, and (vi) cervical insufficiency, 5 Among these conditions, a deregulation of the immune system and an exaggeration of inflammatory processes represent common central mechanisms leading to sPTB.
Intrauterine Infection
A common component of many pathological conditions leading to sPTB is inflammation at the maternal–fetal interface, and its pathogenetic mechanisms are related to activation of the innate immune system. 5,54 In this scenario, placenta, fetal membranes, and myometrium represent key tissues activating the inflammatory pathway throughout the upregulation of several molecules such as proinflammatory IL-1β, TNF-α, and IL-8, chemokines, and PGs. 55 It is now validated that the molecular signals for the onset of parturition, whether parturition at term and preterm has features characteristic of inflammatory processes, based on a balance between pro- and anti-inflammatory pathways. 56 In fact, accumulating evidence suggests that labor is an inflammatory process, characterized by an influx of inflammatory cells into the myometrium and cervix, with concomitant increases in vascular and leukocyte adhesion molecule expression and increased proinflammatory cytokine production by transmigrated leukocytes. 5,57 In sPTB, these mechanisms are activated first during pregnancy.
Under an inflammatory context, at least 40% of sPTB are associated with intrauterine infection. 58 In individual cases, it is often difficult to determine whether infection is the cause or the consequence of processes leading to sPTB. However, the link between infection and sPTB has long been recognized and increasing evidence confirms that infection and inflammation are a primary cause of a large number of sPTB. 59
Indeed, ripening of the cervix, rupture of the membranes, and myometrial contractility, which represent key mechanisms underlying the pathway of labor, are all associated with the activation of inflammatory pathways. Proinflammatory cytokines stimulate the production of matrix metalloproteinases (MMP) -2, -8, -9, COX-2, collagenases, and PGs involved in the softening and dilation of the cervix, resulting in the rupture of the membranes. 60 Finally, TNF-α and IL-1β increase uterine contractility, the local expression of COX-2, and the production of PGE2; IL-6 upregulates the expression of OT receptors on myometrial cells, contributing to increased myometrial contractility. Interestingly, each of these events in some way or other is governed by the canonical inflammatory transcription factors, Nf-kB. 61 This DNA-binding protein is activated by stimuli that induce labor and in turn regulate the expression of molecules involved in the parturition process; Nf-kB either directly controls the genes encoding the cytokines and chemokines or controls the genes that encode the rate-limiting enzymes that manufacture the mediators. 62
In conclusion, the link between intrauterine infection and sPTB is well recognized, and we are nearing a complete picture of the molecular pathways by which infection leads to labor; however, important questions regarding the mechanistic overlap between infectious and noninfectious causes of labor need further studies. 59
Stress, Endocrine, and Immune Disorders
In addition to inflammation, stress is a key pathological event leading to the premature activation of labor. Labor, both at term and preterm, represents a potent stressful condition, 63 and stress response involves both neuroendocrine and immune functions, by increasing secretion of CRH, key pivotal factor activated by all stressful conditions and modulating the endocrine, metabolic, immune, and behavioral responses, via ACTH, cortisol, and adrenaline secretions. 64
During pregnancy, CRH is mainly produced by placenta and gestational tissues and modulates uteroplacental blood flow, myometrial contractility, maternal–fetal HPA axis, and fetoplacental inflammatory/immune response. 29 Plasma and amniotic fluid levels and placental mRNA expression of CRH are higher in women delivering preterm, 65 particularly when this condition is associated with vaginal infection or microbial invasion of the amniotic cavity. 66 Moreover, CRH expression in placental tissues collected from women delivered preterm is even higher in the presence of histological chorioamnionitis, corroborating the role of CRH in inflammatory events occurring in sPTB. 67
A feed-forward loop exists between CRH and proinflammatory cytokines: placental CRH enhances the lipopolysaccharide (LPS)-induced IL-1β secretion, and IL-1β in turn increases CRH production. 68 When an inflammatory process occurs, or maternal and/or fetal physiological and pathological stress occurs, a placental expression of stress-related pathways is activated. 69 To corroborate this evidence, it was demonstrated that a relationship exists between stressful life events or poor social circumstances, psychological and environment and sPTB, suggesting that external environmental events are responsible for this syndrome, 70 by modulating placental products, such as ACTH, cortisol, and PGs. 29,31
In conclusion, stress during pregnancy may activate (a) local neuroendocrine pathways; (b) an immune/inflammatory pathway thus increasing susceptibility to intrauterine and fetal inflammatory processes. 71
Genetic Risk Factors
There is increasing evidence regarding a genetic predisposition of the mother as a potential cause for sPTB. Indeed, a previous sPTB and a history of sPTB in relatives such as the mother, full sister, or maternal half-sister also significantly increases a woman’s risk of sPTB. 72 Despite recognition of a familiar component to sPTB, no specific mode of inheritance has been found for sPTB attributable to genetic factors, and no common genetic variants have been confirmed yet as contributing to sPTB. 72
Nevertheless, for several years, a genetic predisposition to infectious diseases has been discussed as well as varying genetic control mechanisms of clinically apparent infection, 73 involving a number of polymorphisms as candidate genes possibly related with a predisposition to sPTB. Particular interest is attributed to gene polymorphisms regulating the maternal immunologic response during pregnancy, potentially causing an inadequate immunologic response to an infectious stimulus.
The hypothesis of an inflammation triggered inadequate immunologic response with a consecutively increased risk of sPTB, which is supported by many evidences that demonstrated, for example, that TNF2 allele shows an inadequate and exaggerated inflammatory response to an infectious stimulus and this condition represents a higher risk of developing complications during the course of infections. 74 In contrast, a polymorphism that mediates a reduced immunologic response because of a decrease in the production of IL-6 was reported to be protective and to lower the risk for sPTB and pPROM. 75
Therefore, maternal genetic predisposition may result in an increased risk of sPTB. 76 The findings of ongoing studies are very valuable for designing future genome-wide and candidate gene trials that will allow us to develop a better etiologic and biologic understanding of sPTB.
Uteroplacental Insufficiency
Disorders of deep placentation are well recognized as an important etiopathogenetic mechanism for several complications of pregnancy. In fact, it is now clear that disorders of deep placentation are present not only in preeclampsia and intrauterine growth restriction (IUGR) but in other obstetrical syndromes, such as sPTB. To corroborate this affirmation there are many evidences attesting that failure of physiologic transformation of the spiral arteries is present in spontaneous abortion, sPTB, and abruptio placentae. 77
The most common histopathological lesion found in the placenta of patients with spontaneous sPTB is acute inflammation (acute chorioamnionitis and funisitis), but vascular lesions represent the second most common pathological aspect of placental tissue related with this condition. 78,79 Placenta from women delivering preterm presents a greater degree of failed transformation of the spiral arteries in the myometrial and decidual segments than women delivering at term. 80 The reasons why some women with failure of physiologic transformation of the spiral arteries develop PTL, or other obstetrical syndromes, are still unknown. Furthermore, vascular and inflammatory lesions of prematurely delivered placenta are not exclusive conditions but may affect this organ in combination as samples collected from some patients have shown. 5
Concerning vascular lesion observed in placenta of sPTB patients, they may be classified as maternal lesions such as failure of physiological transformation of the myometrial segment of the spiral arteries, atherosis, thrombosis of the spiral arteries (a form of decidual vasculopathy), or a combination of these lesions, and fetal lesions including a decrease in number of arterioles in the villi and fetal arterial thrombosis. All these lesions could lead to sPTB by causing uteroplacental ischemia, although the precise mechanisms responsible for the onset of sPTB have not been determined. It has been proposed that uteroplacental ischemia can activate the renin–angiotensin system that finally can induce myometrial contractility directly 81 or through the release of PGs. 82 Another key role has been proposed for thrombin released after decidual necrosis and hemorrhage started by severe uteroplacental ischemia: thrombin may activate the common pathway of parturition, leading to sPTB. 77
Uterine Overdistension
Uterine overdistension, resulting in contractions and/or pPROM, represents an important risk factor of sPTB, 5 including several conditions such as Müllerian duct abnormalities, polyhydramnios, and multiple pregnancy. In physiological conditions, intra-amniotic pressure remains relatively constant throughout gestation despite the growth of the fetus and placenta. 83 However, stretching may induce myometrial contractility, PGs release, expression of gap junction protein or connexin 43, and increased OT receptor expression in pregnant and nonpregnant myometrium. 84 Stretch may not only induce myometrial contractility but may also modify the contractile response through “mechanoelectrical feedback.” Mechanical forces associated with uterine overdistension may result in the activation of mechanisms leading to membrane rupture. Women with multiple gestations and those with certain Müllerian duct anomalies may also present premature cervical ripening, a mechanism in which IL-8, 85 MMP-1, 86 PGs, 87 and nitric oxide 88 are all implied. Since these mediators are produced in response to membrane stretch, they may exert part of their biological effects in parturition by stimulating extracellular matrix degradation of the cervix.
Separate mechanisms of the disease, as inflammation and stress, may operate in conjunction with uterine overdistension to activate the common components of labor.
Cervical Insufficiency
Uterine cervical modifications play a central role in sPTB and are one of the main indicators for the clinical diagnosis of this syndrome. Classically, the term cervical insufficiency was used to describe a disorder in which painless cervical dilation led to recurrent second trimester pregnancy losses/births of otherwise normal pregnancies. Risk factors for cervical insufficiency can be congenital or more commonly acquired. 89
Congenital risk factors include, for example, collagen abnormalities and uterine anomalies; 90 indeed acquired conditions are represented by surgical trauma and traumatic damage to the structural integrity of the cervix but also by cervicovaginal infection that plays a significant role in labor activation. 91 In terms of clinical presentation, the uterine cervix effaces and dilates in the absence of pain, contractions, and vaginal blood loss. The membranes generally protrude into the vagina, and their rupture is followed by a rapid and almost painless delivery. The diagnosis of these conditions is usually made after exclusion of other potential causes of recurrent pregnancy loss. 5
Predictive Biomarkers of sPTB
A predictive biomarker is defined as a physiological or pathophysiologic biochemical or biomolecular alteration at the organ, tissue, cell, or subcellular level in response to an exposure that is measurable in biological samples and become the signature of the onset of disease, underlying disease process, or phenotypic outcome. 92 Biomarkers are used in various fields of medicine, and concerning sPTB, they could be useful for the implementation of screening in asymptomatic and symptomatic pregnant patients. Biological fluids, such as amniotic fluid, urine, cervical mucus, vaginal secretions, serum or plasma and saliva, have been used over the years to assess the value of biomarkers for the prediction of sPTB. In this context, they would be useful both for the prevention of sPTB in women at risk and for the early detection of a threatened sPTB.
Several reviews have addressed the issue of predictability of sPTB and, according to one of the most recent reviews, a total of 116 different biomarkers were reported and were assayed from 1973 to 2008, but unfortunately most of them showed poor predictability. 92,93
Taking into account the different pathogenetic mechanisms of sPTB, biomarkers can be divided into inflammatory/infectious, hormonal, vascular, stress related, extracellular matrix degradation–related, and genetic (Table 1). Furthermore, considering the new technologies available today, proteomics and proteomics-related biomarkers deserve a separate comment.
Classification of Major sPTB Biomarkers.
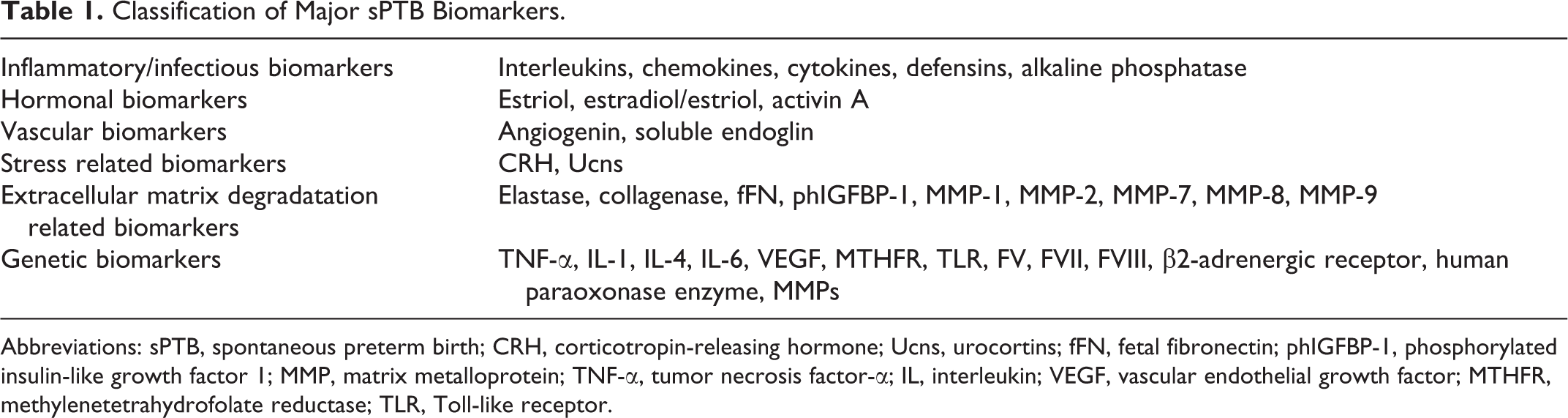
Abbreviations: sPTB, spontaneous preterm birth; CRH, corticotropin-releasing hormone; Ucns, urocortins; fFN, fetal fibronectin; phIGFBP-1, phosphorylated insulin-like growth factor 1; MMP, matrix metalloprotein; TNF-α, tumor necrosis factor-α; IL, interleukin; VEGF, vascular endothelial growth factor; MTHFR, methylenetetrahydrofolate reductase; TLR, Toll-like receptor.
Inflammation/Infectious Biomarkers
Interleukin 2, 6, 8, and 10, TNF-α, granulocyte colony-stimulating factor (GCS-F), stromal cell-derived factor 1α, interferon-γ, MMP-8, secretory leukocyte proteinase inhibitor, soluble vascular cell adhesion molecule 1, soluble intercellular adhesion molecule 1, C-reactive protein, ferritin, and alkaline phosphatase have been more or less correlated with the sPTB. 93,94
Among these, the biomarker with the greatest predictive value is IL-6. Its concentration in cervical fluid is significantly higher at 22 to 25 weeks of gestation in asymptomatic patients who will deliver preterm (in particular <35 weeks) than in controls; IL-6 is significantly associated with a positive cervicovaginal fetal fibronectin (fFN) test and the association is particularly strong within 4 weeks of testing 95 ; moreover, measured in cervical–vaginal fluid of symptomatic women, affected by threatened sPTB, IL-6 demonstrates the ability to predict delivery within 2 and 7 days with a sensitivity and specificity of 60% and 77% for predicting delivery within 2 days, and 62% and 80% for predicting delivery within 7 days, similarly to the performance of fFN test and similarly to cervical dilation experienced through vaginal examination cervical dilatation. 96 Furthermore, in asymptomatic women undergoing mid-trimester amniocentesis, patients with subsequent sPTB within 32 weeks of gestation had a higher median amniotic fluid IL-6 concentration than those who delivered at term, showing an association of IL-6 levels in amniotic fluid and early sPTB. 97
Hormonal Biomarkers
Placenta represents the major endocrine organ during pregnancy 98 and an association between estriol and sPTB has shown. Salivary estriol levels are higher in patients who deliver preterm than in women who deliver at term, and this difference appears as early as at 24 to 26 weeks of gestation and continues until 34 to 36 weeks. 99 The sensitivity of the test is higher in low-risk women than in high-risk women (86% vs 67%), while the negative predictive values (NPVs) of the test are extremely high in both populations (97% vs 95%). The relative risks of developing sPTB with a positive test result were 6.3 in low-risk population and 3.6 in high-risk population. 100 In symptomatic women, salivary estriol is associated with an increased risk of delivery within 2 weeks, but its clinical utility as a routine screening test to predict sPTB in asymptomatic women has not been established. 101 The assessment of the estriol/estradiol ratio may be a useful marker to predict sPTB. In fact, an increase in estriol production is related to the timing of the onset of labor, however, a pivotal event of parturition is represented by a change in the ratio of the estradiol and estriol as labor approaches, leading to a more than 10-fold excess of estriol. Since estriol/estradiol increased in the month before delivery, creating an estrogenic environment at the onset of labor, the estriol increase, and the altered estriol/estradiol ratios may be clinically useful in predicting sPTB. 102
Among growth factors, the detection of high maternal serum activin A concentrations in women who will delivery preterm suggests a role for the molecule in this pathological condition. 103
Stress-Related Biomarkers
Corticotropin-releasing hormone is involved in pathogenetic mechanisms leading to sPTB in which inflammatory and infective pathways represent key events. 66 Maternal plasma CRH levels at mid-gestation are higher in women who subsequently have sPTB than in pregnant women delivering at term 104 ; a further study concerning women with threatened sPTB shows that maternal plasma CRH concentrations are significantly greater in those women giving birth within 24 hours compared to those in women who did not or those in normal individuals. 105 Overall, the measurement of maternal serum CRH would not satisfy the requisites of a screening test for sPTB in a low-risk population, although it should be considered a potential marker to be used in populations with a higher risk.
Maternal plasma urocortin (Ucn) levels are increased in sPTB. 106 Urocortin is a neuropeptide belonging to CRH family, which is expressed by gestational tissues such as amnion, chorion, decidua, trophoblast, and myometrium and is measurable in maternal and fetal plasma. In women with threatened sPTB, maternal plasma Ucn levels increased in patients who experience sPTB before 34 weeks of pregnancy; and among women laboring prematurely the Ucn levels are higher in those delivering within 7 days, compared with those delivering later 106 ; therefore, this measurement provides a promising new biochemical marker to add significant prognostic information for predicting sPTB among women at risk.
Extracellular Matrix Degradation–Related Biomarkers
With regard to extracellular matrix degradation–related biomarkers, fFN is an extracellular matrix protein found at the interface between the chorion and decidua parietalis, and it is normally undetectable in the cervix and vagina after 24 weeks of gestation. Its detection at a concentration of more than 50 ng/mL in the cervicovaginal secretions after this gestational age is associated with an increased risk of sPTB, 107 with a high NPV (88%) and a low positive predictive value ([PPV] 24%), 107 and it is currently used in the clinical practice.
Of particular interest is also an indicator of tissue damage of the choriodecidual interface called phosphorylated insulin-like growth factor 1 (phIGFBP-1), currently used in the clinical practice. This protein is contained in decidua, therefore, as the delivery approaches, fetal membranes begin to detach from the decidua parietalis and phIGFBP-1 leaks into cervical secretions. On the basis of these considerations, its detection in the cervicovaginal secretions is a current method to predict sPTB. Regarding the diagnostic accuracy, phIGFBP-1 test has a sensitivity of 0.39; a specificity of 0.76; a PPV of 0.24 and a NPV of 0.86 for delivery <37 weeks. 108
Genetic Biomarkers
In the sPTB genesis, a possible role of genetics has also been hypothesized. Polymorphisms of certain critical genes may be responsible for the different mechanisms leading to sPTB. Most of the studies linking genetic polymorphisms to prematurity have demonstrated genetic alterations in these mediators responsible for regulating the inflammatory response. 109 In particular, these gene alterations contribute to sPTB by stimulation of proinflammatory mediators or inhibition of those with anti-inflammatory effects. Genetic alterations in several proinflammatory cytokines (TNF-α, IL-1, IL-4, and IL-6) have been studied as possible etiologic mechanisms to PTB. Between these, the strongest evidence of a causal link to PTB is in alterations of TNF-α.
Apart from the gene polymorphisms related to inflammatory mechanisms, many others have also been identified that confer an increased risk of sPTB. These include genetic alterations in vascular endothelial growth factor, 110 the methylenetetrahydrofolate reductase (MTHFR) enzyme 111 ; factor V, VII, or VII 112,113 ; Toll-like receptor 114 ; b2-adrenergic receptor 115,116 ; and the human paraoxonase enzyme. 117 Furthermore, polymorphisms of several MMPs (MMP-1, MMP-8, and MMP-9) have been associated with an increased risk of sPTB in case of pPROM. 118 –120
Proteomics-Related Biomarkers
Advances in molecular biology have led to the development of proteomics. It refers to the study of the complete protein complement, or proteome, of the host in relation to the disease or phenotype of interest. 40
Several proteins (proteomic profile), identified in cervicovaginal fluid at 24 to 28 weeks of gestation by liquid chromatography tandem-mass spectrometry, have been recently identified as potential biomarkers of sPTB. Three proteins (desmoplakin isoform 1, stratifin, and thrombospondin 1 precursor) are significantly elevated in women who deliver between 28 and 32 weeks of gestation, compared with the controls at >37 weeks of gestation. 121) These recent and encouraging results suggest a possible role for preoteomics in the prediction of sPTB in a recent future.
Preventive Interventions for sPTB
It is well known that when the mechanisms that lead to sPTB have already triggered, the possibility to treat patients and arrest the process is poor. Over the years, the possibility to put in practice new strategies aiming to prevent rather treat sPTB has opened new perspectives in the obstetric management of this obstetric syndrome, still burdened by high neonatal mortality and morbidity.
In the following paragraphs, the most used current strategies to prevent sPTB are briefly analyzed.
Progesterone
Progesterone has a role in preventing sPTB in women at risk. This hormone is produced by the corpus luteum in early pregnancy and by the placenta from 7 to 9 weeks of pregnancy, since its suppression during the first trimester of gestation leads to abortion. 122
Concerning the mechanisms of action, progesterone affects 2 fundamental processes implicated in the pathophysiology of sPTB: inflammation and myometrial contractility.
Progesterone has an anti-inflammatory role by (i) inhibiting NF-kB, (ii) COX-2 and PG synthesis, 123 and (iii) reducing the production of proinflammatory cytokines. 124 Pretreating fetoplacental arteries with progesterone significantly decreased the production of IL-6 after stimulation by LPS, a mimetic of infection. 125
Progesterone plays a significant role in maintaining uterine quiescence in the latter half of pregnancy by limiting the production of stimulatory PGs and inhibiting the expression of contraction-associated protein genes (ion channels, OT and PGs receptors, and gap junctions) within the myometrium. 126,127 Therefore, despite progesterone levels in maternal circulation do not change significantly in the weeks before labor, the onset of labor, at term, and preterm, it is associated with a functional withdrawal of progesterone at uterus level. 128,129 Therefore, these concepts provide the rationale for the use of progesterone for the prevention of sPTB.
Several randomized trials, from 2003 till 2011, evaluated the effect of either 17-alpha-hydroxy-progesterone caproate (17P) given intramuscularly or natural progesterone given vaginally or orally for prevention of sPTB. 130
In 2011, the US Food and Drug Administration (FDA) has approved the use of 17P supplementation during pregnancy to reduce the risk of recurrent sPTB in women with a history of at least one prior sPTB. This is the first time that the FDA has approved a medication for the prevention of sPTB, representing moreover the first approval of a drug specifically for use in pregnancy in almost 15 years. In particular, intramuscular 17P weekly administered is recommended in women with a prior sPTB, from 16 to 20 weeks through 36 weeks of gestation to prevent sPTB in any subsequent pregnancy. There is also evidence that women with cervical shortening (<15 mm) diagnosed by transvaginal ultrasound prior to 24 weeks may also benefit, although this indication has not yet been approved by the FDA. 130
In women with singleton gestation, no prior sPTB, and cervical length <20 mm at 24 weeks, the use of vaginal progesterone, either 90-mg gel or 200-mg suppository, is associated with reduced sPTB and perinatal morbidity and mortality; while in case of a prior sPTB, the administration of 17P 250 mg intramuscularly weekly, preferably starting at 16 to 20 weeks until 36 weeks, is recommended, emphasizing that the issue of universal cervical length screening of singleton gestations without prior sPTB for the prevention of sPTB remains an object of debate. 131
A meta-analysis, including 5 trials, demonstrates that the treatment with vaginal progesterone in asymptomatic women with a sonographic cervical length <25 mm at mid-trimester is associated with a significant reduction in the rate of sPTB, respiratory distress syndrome, neonatal morbidity and mortality, birth weight <1500 g, admission to neonatal intensive care unit, and requirement for mechanical ventilation in singleton pregnancies, with no significant differences between the vaginal progesterone and placebo groups in the rate of adverse maternal events or congenital anomalies. It is therefore suggested to perform transvaginal sonographic measurement of cervical length at 19 to 24 weeks of gestation, considering the use of vaginal progesterone at a dose of 90 mg daily in patients with a short cervix, mainly in those with a cervical length between 10 and 20 mm, from 20 to 36 weeks of gestation. 132
However, in a recent randomized controlled trial including women with singleton pregnancies hospitalized for sPTB at 24 to 31 weeks of gestation with a cervical length <25 mm and undergoing tocolysis, the administration of 500 mg of intramuscular 17P after tocolysis ended, repeated semiweekly until 36 weeks or sPTB, did not prolong pregnancy significantly, 133 suggesting that once the pathologic processes of sPTB begin, progesterone treatment is no longer effective.
Despite its relevant preventive use in singleton pregnancies, progestogens have not been associated with the prevention of sPTB in case of multiple gestations, 131,132,134 although recently it has shown a significantly decreased risk of neonatal morbidity and mortality in association with treatment with vaginal progesterone 90 mg/dL daily. 132 Further studies are needed to investigate on this area.
Cervical Pessary
Cervical pessary is a silicone device that has been used in the past 50 years to prevent sPTB. 135 A randomized clinical trial has recently examined its role in the prevention of sPTB in asymptomatic women with singleton pregnancies, with a transvaginal ultrasound finding of short cervical length (less than 25 mm) at 20 to 23 weeks. Comparing women treated with cervical pessary and controls, sPTB < 34 weeks was significantly less frequent in the pessary group than in the expectant management group, with no serious adverse effect associated with the use of this device. 136 Furthermore, the benefits of the cervical pessary have also been hypothesized in multiple pregnancies, with different trials still in progress.
Cervical Cerclage
First performed in 1902, cerclage may be distinguished in different types, as defined by the RCOG: (a) history indicated, when suggested by woman’s obstetric or gynecological history, in case of previous spontaneous second-trimester loss or sPTB, (b) ultrasound indicated, as a therapeutic measure in cases of cervical length shortening seen on transvaginal ultrasound and rescue cerclage, and (c) as a salvage measure in case of premature cervical dilatation with exposed fetal membranes in the vagina.
Concerning the surgical technique, cerclage can be distinguished as (i) transvaginal (McDonald), (ii) high transvaginal (Shirodkar), (iii) transabdominal, and (iv) occlusion. However, the use and efficacy of cerclage in these different groups is highly controversial, since there are contradictory results in individual studies and meta-analyses.
In a retrospective study, cerclage placement was performed in patients with an ultrasonographic evidence of cervical length ≤15 mm, between 14 and 24 weeks of gestation and did not reduce the rate of sPTB and increased the risk of pPROM, as compared to women with the same clinical conditions without cerclage 137 ; while in a more recent meta-analysis cerclage seems beneficial in a population of women with a previous sPTB (or second-trimester loss) and asymptomatic cervical shortening (<25 mm) between 14 and 24 weeks shown by transvaginal ultrasound imaging or cervical dilatation confirmed by physical examination. 138 Both these studies refer to singleton pregnancies; conversely, in twin pregnancy the use of cerclage has been associated with a higher incidence of sPTB. 139
Management of sPTB
Nowadays the correct diagnosis and subsequent treatment of sPTB still represents a clinical issue. The management of women presenting with sPTB should include (i) early identification of risk factors and timely diagnosis of sPTB, (ii) identification of the etiology of sPTB, (iii) evaluation of fetal well-being, and (iv) administration of therapy when indicated to improve fetal/neonatal outcome.
In the clinical practice, obstetricians should focus on the concept that interventions to reduce the likelihood of delivery should be reserved for women with sPTB at a gestational age at which a delay in delivery will provide benefit to the newborn. In this scenario, the choice of administering tocolytic agents should be always evaluated on the basis of fetomaternal clinical conditions. 140,141 It remains plausible that, for selected women, such as those requiring transfer to tertiary center for neonatal care or time to complete a course of corticosteroids, there may be benefit associated with tocolysis. 140,141
The purpose of using drugs for the management of sPTB is to prolong pregnancy to term or long enough to increase gestational age and infant birth weight substantially, while an effective regimen of corticosteroids can be administered to enhance fetal lung development. These “golden hours” need to be optimized by in utero transfer of the mother to a tertiary center with neonatal facilities and administration of antenatal corticosteroids to the mother. 142
Principal topics of management of a woman at risk for sPTB include (i) monitoring fetal heart and uterine contractions; (ii) considering antenatal transfer of the mother and fetus to a hospital equipped to take care of preterm infants; (iii) tocolysis if gestational age is <32 weeks; (iv) administering antibiotics in case of pPROM; and (v) administering corticosteroids. Bed rest is commonly recommended but has not been proved to be efficacious in halting sPTB. 143
Tocolytics
Tocolytic therapy should provide short-term prolongation of pregnancy, enabling the administration of antenatal corticosteroids for fetal lung development as well as transport, if indicated, to a tertiary facility. However, no evidence exists that tocolytic therapy has any direct favorable effect on neonatal outcomes or that any prolongation of pregnancy afforded by tocolytics actually translates into statistically significant neonatal benefit. 140 In obstetric practice, the use of tocolytic agents should be individualized and based on the fetomaternal conditions, potential side effects of the tocolytic drugs, and gestational age.
In fact, several pathological conditions exist in which tocolysis is contraindicated such as intrauterine fetal demise, lethal fetal anomalies, non-reassuring fetal status, severe preeclampsia or eclampsia, maternal bleeding with hemodynamic instability, chorioamnionitis, and maternal contraindications to tocolysis. 140
There are a variety of tocolytic agents in current use, which act on the uterus in different ways. The most common are calcium channel blockers, beta mimetics, magnesium sulphate, COX inhibitors, and OT-receptor antagonists (Table 2).
Tocolytic Agents.
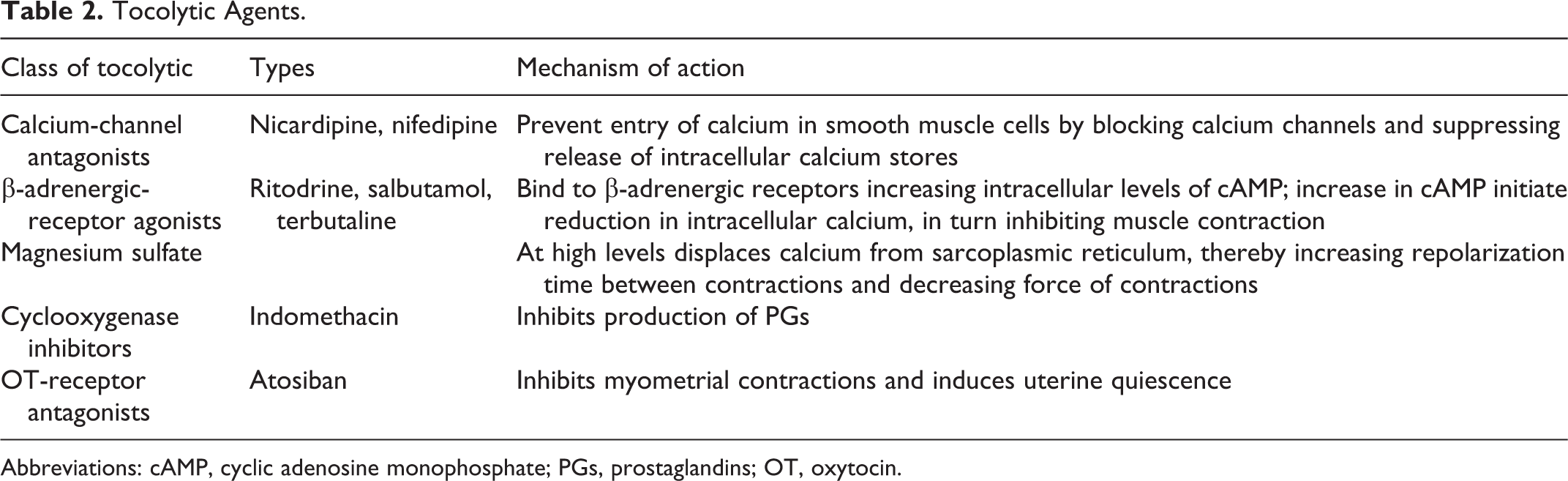
Abbreviations: cAMP, cyclic adenosine monophosphate; PGs, prostaglandins; OT, oxytocin.
The “choice” of tocolyic agent, which could improve neonatal outcome with no maternal or neonatal side effect, has not yet surfaced. Currently, in the management of PTL the use tocolytic agents is finalized to permit in utero transfer to a tertiary center and concomitant use of antenatal corticosteroids. 144 However, the management of sPTB should depend not only on administering uterine contraction inhibitors if possible, but also on understanding the etiology, risk factors, and pathologic processes leading to PTL; on the basis of these considerations, in the clinical practice prediction, diagnosis, and the possibility to take direct and effective measures should always follow the same path.
β-adrenergic-receptor agonists
β-adrenergic-receptor agonists are the most widely used agents in clinical practice of threatened sPTB. 145 The β-adrenergic-receptor agonists cause myometrial relaxation by binding to β2-adrenergic receptors and subsequently increasing the levels of intracellular cyclic AMP. An increase in intracellular cyclic AMP activates protein kinase, which inactivates myosin light-chain kinase, thus diminishing myometrial contractility. 146 The most common β-adrenergic-receptor agonists employed in clinical practice is ritodrine; its effect in prolonging the gestational age of sPTB is definite but limited to only 2 days. 147 Although 2 days are enough for inducing maturity of fetal lung by corticosteroids, ritodrine cannot prolong labor to term effectively.
In 2011, the FDA issued a warning regarding the use of terbutaline to treat sPTB because of reports of serious maternal side effects. 148 Another review reported possible deleterious behavioral effects in offspring after in utero exposure to β-adrenergic-receptor agonists. 149 These data suggest that the use of terbutaline should be limited to short-term inpatient use as a tocolytic or for the acute antepartum therapy of uterine tachysystole. Maternal side effects of β-adrenergic-receptor agonists drugs are sinister. β-adrenergic-receptor agonists lack uterine selectivity and can cause metabolic and cardiovascular side effects. Most serious maternal side effects are pulmonary edema, myocardial ischemia, and heart failure. 150
OT-receptor antagonists
Unlike other tocolytic agents, OT-receptor antagonists have been developed specifically as tocolytics. OT-receptor antagonists block OT receptors in the myometrium, preventing a rise in intracellular calcium, thereby relaxing the myometrium. 151 Atosiban is an OT-receptor antagonist specifically developed for the treatment of PTL. 151 Early reports of the use of atosiban as a tocolytic agent, both in vitro and in animal studies, were promising, and preliminary studies in pregnant and nonpregnant humans have suggested a very low incidence of maternal side effects. 152 Potential maternal side effects are relatively moderate: adverse injection side reaction, nausea, vomiting, headache, chest pain, and hypotension. 153 Atosiban is the only tocolytic that has demonstrated superiority as maintenance therapy over placebo in prolonging pregnancy, but atosiban is not available in the United States. 110 ,154
Calcium-channel antagonists
Calcium-channel antagonists are increasingly used as tocolytic agents. These agents inhibit calcium ions influx across the cell membrane, thereby decreasing the tone in the smooth muscle vascular tone. 155 Among them, nifedipine is the most commonly used to inhibit labor, although nifedipine has been shown to have a more favorable neonatal outcome and better prolongation of gestation, it is not licensed for tocolysis. 156
The mechanism by which nifedipine achieves a reduction in the rate of respiratory distress syndrome is likely by prolonging pregnancy so that interventions, such as administration of antenatal corticosteroids that are known to reduce respiratory distress syndrome, have the opportunity to be effectively implemented. 157 Moreover, it was proposed that neonatal respiratory distress syndrome may also be reduced by a direct effect of nifedipine on improving neonatal pulmonary perfusion. 158 Although nifedipine has been shown to have a more favorable neonatal outcome and better prolongation of gestation, it is not licensed for tocolysis, and there have been concerns about a theoretical risk to fetal and placental circulations with its use. 156 In addition, there is no consensus about the dosage, the route, and the release formulation for a tocolytic regimen for nifedipine.
Cyclooxygenase inhibitors
Cyclooxygenase enzymes are fundamental to the production of PGs and inhibitors that reduce uterine contractions. 159 Cyclooxygenase inhibitors are easily administered (orally or rectally) and have fewer maternal side effects than betamimetics. 160 Cyclooxygenase inhibitors, however, freely cross the placenta and can interfere with PGs homeostasis in the fetus. 161 Some studies have attributed a range of adverse effects in the fetus and neonate to in utero exposure to indomethacin (the most commonly used COX inhibitor) during tocolysis. 162 –164 In fact, they can be administered before 32 weeks and for a maximum of 72 hours. Reported adverse effects include oligohydramnios, renal failure, premature closure of the ductus arteriosus with consequent pulmonary hypertension, persistent patent ductus arteriosus, necrotizing enterocolitis, and intraventricular hemorrhage. 165 The recognition of distinct forms of COX, namely COX-1 and COX-2, led to the development of COX-2-specific inhibitors. COX-2 is specifically associated with myometrial contractility. 166 It is possible that selective inhibition could enable more effective tocolysis with reduced adverse events. The role of COX inhibitors for women in PTL warrants further attention 167 and as with all other tocolytics, indomethacin for short-term treatment of sPTB should be used after carefully weighing the potential benefits and risks. 140
Magnesium sulfate
Magnesium sulfate is commonly used to treat pregnancy-induced hypertension and, though unlicensed, is widely used for tocolysis in the United States. 142 It can decrease uterine activity, but the basis for this tocolytic action is unknown. One possible mechanism is that magnesium competes with calcium for entry into the myometrial cells through voltage-gated channels. 168 However, some systematic review do not show statistically significant differences between magnesium sulfate and placebo to prolong pregnancy. Thus, magnesium sulfate should not currently be recommended or licensed for the management of sPTB. 167 Early observational studies suggested an association between prenatal exposure to magnesium sulfate and the less frequent occurrence of subsequent neurologic morbidities. 169 Subsequently, several large clinical studies have evaluated the evidence regarding magnesium sulfate, neuroprotection, and sPTB. 170,171 Accumulated available evidence suggests that magnesium sulfate reduces the severity and risk of cerebral palsy in surviving infants if administered when birth is anticipated before 32 weeks of gestation. Hospitals that elect to use magnesium sulfate for fetal neuroprotection should develop uniform and specific guidelines for their departments regarding inclusion criteria, treatment regimens, concurrent tocolysis, and monitoring in accordance with one of the larger trials. 140 In conclusion, the use of magnesium sulfate to inhibit acute sPTB has similar limitations when used for pregnancy prolongation. 168 However, if magnesium sulfate is being used in the context of sPTB for fetal neuroprotection and the patient is still experiencing PTL, a different agent could be considered for short-term tocolysis. 140
Bed rest
Bed rest represents one of the most common interventions used for the prevention and/or treatment of threatened PTL. Unfortunately, there are no prospective randomized studies that have independently evaluated the effectiveness of bed rest for the prevention of PTL. Therefore, although a reduction of physical activity may seem appropriate for some women at risk of sPTB, there is no evidence that this intervention will result in a reduction in sPTB. In conclusion, no evidence exists that bed rest should be a standard component of prevention or treatment for sPTB. 172 Furthermore, the potential harm, including venous thromboembolism, bone demineralization, and deconditioning, and the negative effects, such as loss of employment, should not be underestimated. 173,174
Nontocolytics
Antibiotic therapy
Given the abounding data associating various infections with sPTB, it is natural to consider the use of antibiotic and other antimicrobial therapy to prevent sPTB. 175 Based on this concept, the utility of antibiotics to prolong pregnancy and reduce neonatal morbidity in women with sPTB has been evaluated in numerous randomized clinical trials. Regarding women presenting sPTB and intact membranes, data do not demonstrate any benefit from antibiotic therapy, therefore finding no difference between antibiotics and placebo for prolonging pregnancy or preventing sPTB, respiratory distress syndrome, or neonatal sepsis. 176 Thus, antibiotics should not be used in this class of patients. 140
Differently, there are recommendations for antibiotic use in women with pPROM 177 and in group B streptococci carrier status. 178 Preterm prelabor rupture of membrane complicates 2% of pregnancies but is associated with 40% of sPTB and can result in neonatal morbidity and mortality, 179 due to prematurity, sepsis, and pulmonary hypoplasia 180 and in maternal infection and consequently increased risk of chorioamnionitis. Maternal infections are reduced in women exposed to antibiotics 181 and antibiotic treatment is associated with a significant reduction in maternal infections and chorioamnionitis, 182 and with improved neonatal outcome. 183 Erythromycin or penicillin is the antibiotic of choice, since both are associated with a reduction in the numbers of babies born prematurely within 48 hours and who had positive blood cultures. Delivery should be considered at 34 weeks of gestation in women with pPROM; in these cases, the expectant management requires an assessment of the risks related to the development of intrauterine infection. 180
Antenatal corticosteroids
The most beneficial intervention for improvement of neonatal outcomes among patients who give birth preterm is the administration of antenatal corticosteroids.
The administration of antenatal corticosteroids in women at risk of imminent sPTB is strongly associated with decreased neonatal morbidity and mortality. 184 In particular, a significant reduction in rates of neonatal death within the first 24 hours, respiratory distress syndrome (RDS), intraventricular hemorrhage, necrotizing enterocolitis, and patent ductus arteriosus 185 have been demonstrated in women receiving antenatal corticosteroids and their use is safe for the mother.
Concerning the mechanisms of action, corticosteroids are involved in fetus lung maturation, promoting surfactant synthesis, increasing lung compliance, reducing vascular permeability, and generating a greater response to postnatal surfactant treatment. Antenatal corticosteroids have maximal effectiveness in preventing neonatal complications of prematurity when delivery is within 2 to 7 days after administration. 186
The most extensively studied and used regimens of corticosteroid treatment for the prevention of RDS is represented by a single course of corticosteroids recommended for pregnant women between 24 weeks of gestation and 34 weeks of gestation who are at risk of sPTB within 7 days. 187 A Cochrane meta-analysis reinforces the beneficial effect of this therapy regardless of membrane status and concludes that a single course of antenatal corticosteroids should be considered routine for all preterm deliveries. 185 Betamethasone and dexamethasone are the most widely studied corticosteroids and have been the preferred antenatal treatments to accelerate fetal lung maturation. The administration of betamethasone or dexamethasone has been shown to decrease neonatal mortality. 188 Treatment, for either a primary or a rescue course, should consist of either two 12-mg doses of betamethasone given intramuscularly 24 hours apart or four 6-mg doses of dexamethasone every 12 hours administered intramuscularly. 122 Because treatment with corticosteroids for less than 24 hours is still associated with significant reductions in neonatal morbidity and mortality, a first dose of antenatal corticosteroids should still be administered even if the ability to give the second dose is unlikely, based on the clinical scenario. 187 However, no additional benefit has been demonstrated for courses of antenatal steroids with dosage intervals shorter than those outlined previously, often referred to as accelerated dosing, even when delivery appears imminent.
Combination of Multiple Parameters to Identify Patients at Risk of sPTB
Primary predictors include most of the classical risk factors for sPTB previously analyzed and may be used to estimate the baseline risk of sPTB and primary prevention would seek to modify these risk factors. Starting from the baseline risk, secondary predictors of sPTB, including signs, symptoms and findings in pregnancy that are known to increase the risk of sPTB may help to adapt the risk of sPTB during the course of pregnancy in individual women. 189
In the absence of reliable clinical predictors of sPTB, the attention has focused on the 2 best and most widely accepted methods of identifying women at high risk of sPTB in both nullipara and multipara: fFN and cervical length (CL) measurements.190).
Cervical Length
Shortened CL is a risk factor for sPTB in both low- and high-risk pregnancies. The risk of spontaneous sPTB increases as CL decreases.
Evaluation of CL may be done either sonographically or through direct physical examination of the cervix. The gold standard for the measurement of CL in pregnancy is transvaginal ultrasonography (TVS) using sterile technique, which has many advantages when compared with digital examination. TVS is objective, reproducible, and acceptable to patients. 191 Cervical changes such as dilatation of the internal cervical os with funneling (beaking) of the membranes can be easily appreciated by TVS but not by digital examination. 192 Moreover, TVS appears to be safe and does not increase the risk of ascending infection even in patients with pPROM. 193,194
Cervical length during pregnancy can range from 25 to 70 mm and ultrasound width of the cervical canal ranges from 2 to 4 mm. 89,195 At 24 weeks, a cervical length of ≤25 mm had a sensitivity of 37%, a specificity of 92%, a PPV of 18%, and a NPV of 97% in predicting spontaneous sPTB at <35 weeks’ gestation. 89 However, the gestational age at which transvaginal ultrasound cervical length is measured significantly affects the calculation of risk of spontaneous sPTB. The sPTB risk increases as the length of the cervix declines and as the gestational age decreases. 196
Routine measurement of CL to identify women at risk for spontaneous sPTB is not currently recommended in otherwise low-risk pregnancies because of the low PPV and absence of proven effective interventions. 197,198,199,200 Nonetheless, implementation of such a screening strategy should be viewed as reasonable and can be considered by individual practitioners. 200 However, serial measurements of CL should be performed in high-risk women to better identify those pregnancies at risk for spontaneous sPTB prior to 35 weeks of gestation. 89,197,198,199
Cervical Length Combined With Other Biochemical and Biophysical Markers
Cervical length and funneling
Funneling of the cervix is defined as the opening of the internal cervical os on ultrasound. The appearance of the cervix on TVS has been described over time as a progression of the letters T, Y, V, and U (Trust Your Vaginal Ultrasound) representing the progressive increasing funneling and decreasing CL. 201 It appears that U shape is more likely to be associated with sPTB, compared with a V-shaped funnel. 196 Nevertheless as an independent finding, funneling does not add appreciably to the risk of early gestational age at delivery associated with a shortened cervical length. So, women with a long cervix and funneling are not at increased risk of preterm delivery 202,196,203
Cervical length and sludge
Amniotic sludge, a collection of echogenic particles next to the internal cervical os, appears as a cluster of free-floating hyperechogenic material within the amniotic fluid near the uterine cervix on ultrasonography. The exact composition of amniotic sludge remains unclear but, based on a single case, bacterial biofilm has been postulated to be an important component. 204,205 Amniotic sludge is an independent risk factor for histologic chorioamnionitis and microbial invasion of the amniotic cavity in women with sPTB and intact membranes. 206,207 Moreover, the presence of sludge is an independent risk factor for pPROM and spontaneous sPTB. 208 Recently, it was shown that dense amniotic sludge, especially when it was associated with short cervical length, was linked with sPTB before 32 weeks’ gestation. 209
The observation that the shorter the cervical length, the greater the likelihood of amniotic fluid “sludge,” 207 has been interpreted as an indication that intra-amniotic infection/inflammation will eventually lead to a short cervix. Alternatively, patients with a short cervix may be at particularly high risk of developing an ascending infection. 210 It is possible that effacement leading to a short distance between the ectocervix and the membranes may disrupt the mucus plug and impair other components of the innate and/or adaptive immunity in the lower genital tract. 204
In conclusion, dense amniotic sludge at mid-trimester ultrasound should be studied further as it appears to be one of the strongest and specific markers of early sPTB. Its prevalence and predictive values should be definitely evaluated in the general population at 18 to 20 weeks’ ultrasound. Recent literature suggests that dense intra-amniotic sludge combined with short cervix is even more predictive of early sPTB and, most likely, of intra-amniotic infection and inflammation. 91,211,212
Cervical length and fFN
Cervical length measurements and fFN measurements are independent risk factors for sPTB. The risk of sPTB is higher if both tests are abnormal than if only 1 is abnormal. 190 Even in women with symptoms of PTL, sPTB is highly unlikely if the CL is longer than 30 mm or if the fFN is negative. (198 In such women, selective use of fFN after CL measurement is more specific than CL alone for predicting sPTB (81% vs 63%, respectively). 213 In light of these and other data showing conclusively that combined use of the CL measurement by TVS and cervicovaginal fFN is more effective for predicting sPTB than any of these methods alone, 2-step testing should be performed in all women with symptoms of PTL to better identify those women at risk of sPTB.
In conclusion the routine employment of secondary predictors as CL, an fFN to screen low risk pregnancies is generally not recommended, but it may be used in the management of women at high risk for sPTB, such as women with previous sPTB or late miscarriage. In these women, secondary predictors can be used as part of a management protocol to individualize patient care. Negative test results would be valuable in reassuring both women and care providers to avoid unnecessary interventions. Positive test results would increase the level of clinical attention and direct more resources to these women. 190 However, the combination of maternal and pregnancy characteristics, ultrasound and laboratory results, and other biomarkers merits more research.
Conclusion
This review provides an overview of the pathogenesis, risk factors, therapeutic options, and prevention of sPTB, highlighting that despite new scientific research and advances in obstetric care, nowadays it is not still possible to prevent this problem, responsible every year of significant rates of neonatal morbidity and mortality. This is not surprising since sPTB represents only the “top of the iceberg” where most etiopathogenic processes are still not completely understood.
In this context, a greater effort is necessary to improve the knowledge of the causes and mechanisms associated with sPTB in order to advance the development of preventive strategies. Investments in maternal health and birth care will improve outcomes for both women and premature newborns.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.