
Abstract
Myoinositol (MI) and
Background
Polycystic ovary syndrome (PCOS) is the most common cause of infertility, ovarian dysfunction, and menstrual irregularity, affecting 5% to 10% of women of reproductive age. 1 Both the etiology and diagnosis of the syndrome are controversial. The pathogenesis of PCOS has been linked to the development of insulin resistance and hyperinsulinemia. Indeed, hyperinsulinemia due to insulin resistance occurs in approximately 80% of women with PCOS and central obesity, as well as in 30% to 40% of lean women diagnosed with PCOS. 2,3 The exact cause of the insulin resistance observed in women with PCOS is still unknown, although it has been hypothesized that an altered insulin signal transduction in patients with PCOS may cause insulin resistance that in turn induces abnormal ovarian steroidogenesis. 4,5 For this reason, among the treatments routinely used, women with PCOS seem to respond favorably to insulin-sensitizing drugs, such as metformin or thiazolidinediones. 6,7 However, these drugs are not devoid of side effects—nausea and diarrhea have often been reported following metformin treatment, while the use of thiazolidinediones has been related to weight gain and, more recently, to cardiovascular events, 5 fragility fractures, 8 and bladder cancer. 9
Inositol (hexahydroxycyclohexane), a 6-carbon polyol belonging to cyclitols (polyhydroxy-cycloalkanes), plays a key role in multiple cellular processes that control glucose metabolism. Inositol is present in nature as 9 possible isomers; among them, 2 were proven to be insulin mediators: myoinositol (MI) and
Based on literature data and on the fact that inositol phospholipids are follicle-stimulating hormone (FSH) second messengers, 14 we developed a theory 15 in which we speculated that patients with PCOS having hyperinsulinemia present an enhanced MI to DCI epimerization in the ovary, which in turn would lead to MI deficiency in the ovary that would impair FSH signaling, resulting in reduced oocyte quality and increased risk of ovarian hyperstimulation syndrome. 15
In the present study, we make an attempt to support this theory, by testing follicular fluid of either patients with PCOS or healthy women for MI and DCI content.
Methods
Participants
A total of 20 healthy women and 20 patients with hyperinsulinemic PCOS, aged 25 to 40 years and referred to our center for in vitro fertilization (IVF) cycles due to male infertility factors, were recruited in this study. Before entering the study, a written informed consent was obtained from all participants. All healthy women were required to have regular ovulatory menstrual cycles (luteal-phase progesterone [P], >10 nmol/L), a normal body mass index (BMI), not taken medications or exogenous hormones in the past 24 months, no past or current reproductive endocrine problems. Polycystic ovary syndrome was diagnosed according to the criteria established by the European Society for Human Reproduction and Embryology (ESHRE) and the American Society for Reproductive Medicine (ASRM) in Rotterdam in 2003 (2 out of 3 criteria) 16,17 : (1) oligo-anovulation, (2) hyperandrogenism (clinical or biochemical), and/or (3) presence of 12 or more follicles in each ovary, measuring 2 to 9 mm in diameter, and/or increased ovarian volume (>10 mL). An additional inclusion criterion for women with PCOS was hyperinsulinemia defined as fasting insulin higher than 10 μU/mL. 18,19
Sample Collection
Follicular fluid was derived from spontaneous cycles both for healthy participants and for participants with PCOS. Starting from day 10 and defining as “cycle day 1,” the first day of menstrual bleeding, transvaginal ultrasounds were performed daily or every 2 days to follow follicle growth. When the dominant follicle reached at least 16 mm in diameter and the endometrium had a thickness of at least 8 mm, a human chorionic gonadotropin (HCG) injection was given and 34 hours later the follicular fluid was collected. Sample was collected using a vaginal probe attached with a double lumen needle. After oocyte isolation, follicular fluid was centrifuged at 600g for 10 minutes at room temperature. Supernatant was stored at −80°C until MI and DCI quantification. The institutional review board of our institution approved the study.
Sample Analysis
Both MI and DCI were determined as previously described. 20 Quantification of MI and DCI was performed by Chelab Pharma Division (Treviso, Italy) using gas chromatography–mass spectrometry (GC-MS) analysis after extraction with organic solvents and derivatization. Injection (1.0 μL) was performed in a split-less mode at 270°C and a capillary column Agilent 122-5532 DB-5 ms (0.25 mm × 30 m × 0.25 μm) was used. Total run-time was 15 minutes: oven at 70°C from 0 to 1 minute; 20°C/min to 150°C; 10°C/min to 240°C; 4 minutes at 320°C postrun. The flow rate was fixed at 1.2 mL/min, and the results were analyzed by an MS 5973 Network Series detector in sim mode.
Statistics
Results are presented as mean ± standard deviation (SD). The follicular concentrations of MI and DCI in healthy participants and in patients with PCOS were analyzed by the nonparametric Kruskal-Wallis test performed by GraphPad Prism software (La Jolla, California).
Results
The characteristics of both study groups are outlined in Table 1. As shown, healthy women and women with PCOS were similar in age and had similar BMI and FSH levels. However, women with PCOS were significantly more insulin resistant (higher Homeostatic model assessment (HOMA-IR), P < .01and lower quantitative insulin sensitivity check index (QUIKI), P < .01), hyperinsulinemic (P < .01), and displayed higher LH levels (P < .01) than healthy women. Furthermore, glucose levels tended to be higher in women with PCOS.
Demographic Characteristic. In the present table, demographic characteristic of both study groups are listed.
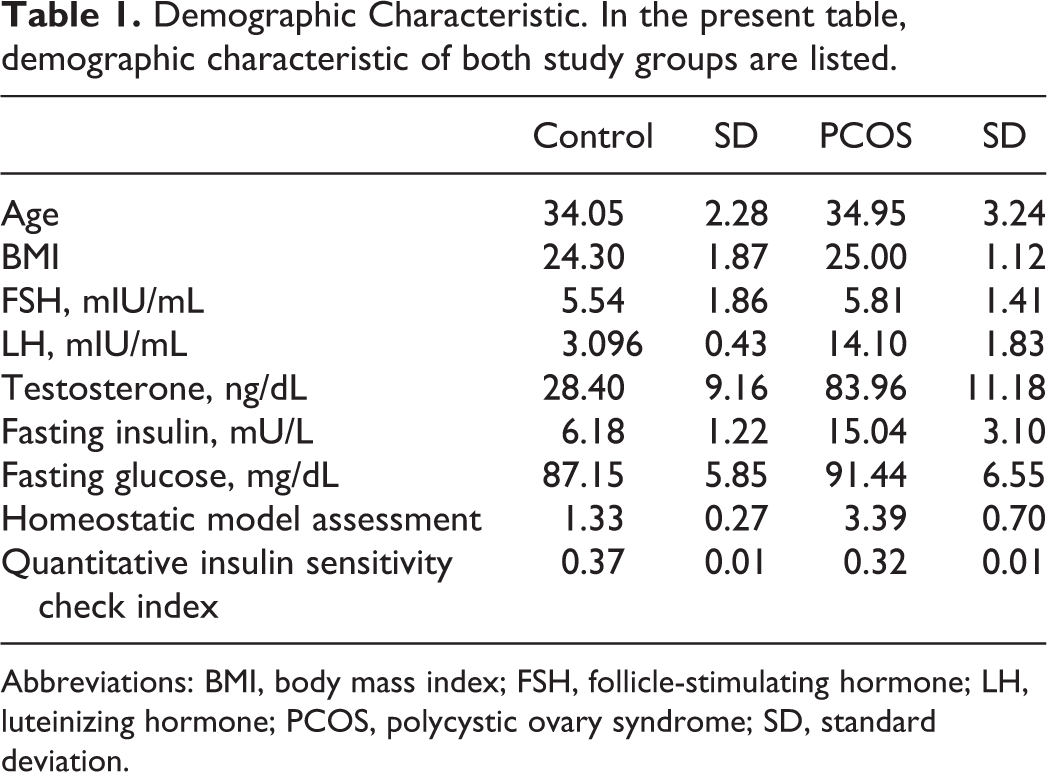
Abbreviations: BMI, body mass index; FSH, follicle-stimulating hormone; LH, luteinizing hormone; PCOS, polycystic ovary syndrome; SD, standard deviation.
The results of our study showed that the MI content was significantly lower in the follicular fluid of patients with PCOS than that in healthy women (patients with PCOS: 3.00 ± 1.22 μmol/L and healthy women: 22.68 ± 1.38 μmol/L; P < .001). Conversely, women with PCOS had significantly higher follicular DCI content than that of healthy women (patients with PCOS: 16.65 ± 2.01 μmol/L and healthy women: 0.22 ± 0.08 μmol/L; P < .001). As a consequence, the MI-DCI ratio was 100:1 in healthy women, while it dropped to 0.2:1 in patients with hyperinsulinemic PCOS (Figure 1). Mean values of MI-DCI ratio were 119.21 ± 46 μmol/L (range from 60.27 to 209.45 μmol/L) and 0.18 ± 0.08 μmol/L (range from 0.05 to 0.38 μmol/L) for healthy participants and participants with PCOS, respectively.
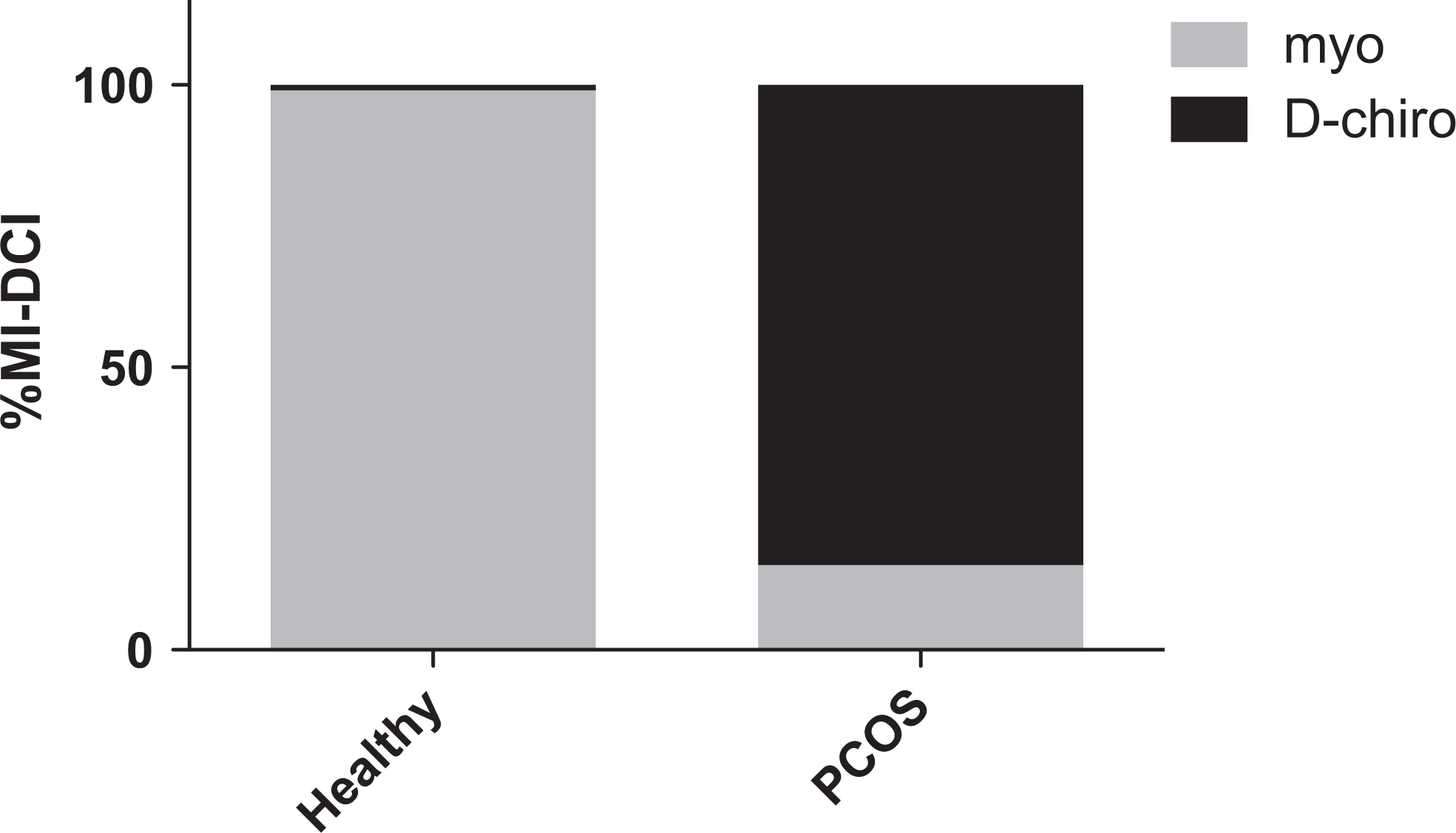
The figure depict the ratio between MI and DCI in healthy women and PCOS patients.
Discussion
The results of the present study show that the MI-DCI ratio is clearly altered in patients with hyperinsulinemic PCOS. The first clinical trial that investigated the effects of DCI in patients with PCOS dates back to 1999. 21 Of the 22obese patients with hyperinsulinemic PCOS treated with DCI for 8 weeks, 19 ovulated once compared to the placebo group. 21 These data, however, were not confirmed in a follow-up study. 22
Additional studies showed that MI, besides improving hormonal profile and restoring ovulation, is able to regularize menses in both lean and obese patients with PCOS, reduces the FSH units needed during IVF, and improves oocyte and embryo quality. 23,24 Interestingly, when the effects of MI and DCI on oocyte quality in patients with euglycemic PCOS were compared, it was shown that the total number of oocytes retrieved did not differ in the 2 treatments groups. However, the number of mature oocytes was significantly increased and the number of immature oocytes decreased in the MI group compared to the DCI group. Furthermore, MI-treated patients showed an increase in the mean number of top quality embryos and in the total number of pregnancies compared to DCI-treated women. Last, it was demonstrated that only MI had the ability to reduce the recombinant FSH (rFSH) International Units (IU) administered. 23
As already mentioned, each tissue has a typical MI/DCI conversion rate depending on the specific needs of the 2 different molecules, 10,25 It was shown that the ratio of these 2 insulin mediators was itself insulin dependent. Indeed, in participants with type 2 diabetes, the DCI-MI ratio was reduced and less DCI was synthesized, owing to a reduction in the epimerase activity. 25,26 However, ovaries do not become insulin resistant. 27 –29 On the basis of literature data and the evidence that indicated a higher efficacy of MI over DCI in assisted reproductive technology (ART), 23 we recently developed and published a theory about the existence of a “DCI paradox” in the ovary. 15 We speculated that patients with PCOS having hyperinsulinemia likely present an enhanced MI to DCI epimerization in the ovary; this would result in an increased DCI-MI ratio (ie, overproduction of DCI), which in turn would lead to MI deficiency in the ovary. This MI depletion could eventually be responsible for the poor oocyte quality observed in these patients. 30 Furthermore, because MI supplementation reduces the rFSH IU administrated during IVF cycles, 24,27 it is likely that the MI deficiency in the ovary would also impair FSH signaling, which increases the need for FSH IU (FSH resistance) in order to obtain a controlled ovarian stimulation. 31 This could result eventually in an increased risk of ovarian hyperstimulation syndrome for patients with PCOS.
A recent study by Isabella and Raffone 32 showed that treatment with high doses of DCI may worsen oocyte quality and ovarian response. In their study, 5 groups of patients with PCOS received either placebo or different doses of DCI (300, 600, 1200, and 2400 mg of DCI daily). All treatments were carried out for 8 weeks before FSH administration. The results showed that total FSH units increased significantly in the 2 groups that received the higher doses of DCI. The number of immature oocytes was significantly increased in the 3 groups that received the higher doses of DCI. Conversely, the number of meiosis II (MI) oocytes was significantly lower in the group treated with 2.4 g of DCI than that of the placebo group. Noteworthy, the number of grade I embryos was significantly reduced by DCI supplementation. 32
The altered MI-DCI ratio may be either one of the etiological factors or the consequence of PCOS. In particular, low oocyte quality in patients with PCOS may be linked to the combination of at least 2 factors, namely reduced glucose uptake and reduced MI concentration in the follicular fluid. During the revision process, a new manuscript by Heimark et al 33 was published, in which the authors were able to measure the epimerase enzymatic activity in the theca cells derived from healthy women and women with PCOS, providing partial evidence of DCI. Indeed, in our study we were able to show that the molecular milieu fostering the oocyte is compromised. Therefore, both studies as a whole provide to the scientific community a clear picture of the biological pathways altered in the PCOS. Furthermore, these evidences open new scenarios on the possible PCOS etiopathogenesis, taking into account that the DCI in the ovary is responsible for the insulin-stimulated testosterone production among others. 34
Conclusions
The present data provide the first empirical support to the notion that women with PCOS display a misbalance in the MI-DCI ratio in the ovary, which might impair FSH signaling and worsen oocyte quality, as it has been shown by previously reported data. 24,35 Therefore, these new findings support the concept that a crucial factor for women with PCOS ovarian function is to maintain the physiological ovarian MI-DCI ratio.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.