
Abstract
This study was designed to investigate whether endometrial receptivity genes are altered in infertile patients with intramural leiomyomas (IM) not distorting the endometrial cavity undergoing myomectomy. We measured endometrial HOXA-10, HOXA-11, LIF, ITGB3, and ITGAV messenger RNA (mRNA) expressions levels before and after myomectomy/metroplasty during mid-luteal phase in participants with IM, submucosal leiomyomas (SM), and septate uterus and fertile participants without fibroids. Initial endometrial sampling was obtained at the time of surgery, and second sampling was obtained 3 months after myomectomy/metroplasty. Expressions of each gene were evaluated using real-time reverse transcriptase polymerase chain reaction (RT-PCR). A trend toward decreased endometrial HOXA-10, HOXA-11, and ITGAV mRNA expression was detected in both SM and IM groups before myomectomy when compared to both fertile group and septate uterus. However, the differences failed to show statistical significance. After myomectomy of IM, we have detected 12.8-fold increase in endometrial HOXA-10 mRNA expression and 9.0-fold increase in endometrial HOXA-11 mRNA expression. This increase in endometrial HOXA-10 and 11 mRNA expression was significant. Accordingly, 2 patients having intramural fibroids greater than 5 cm were able to remain pregnant after myomectomy. Conversely, submucosal myomectomy did not cause any significant effect on endometrial receptivity markers. Likewise, all markers of endometrial receptivity remained unchanged after metroplasty. Myomectomy of IM have favorable effect on endometrial HOXA-10 and 11 mRNA expression.
Keywords
Introduction
The incidence of uterine leiomyomas in infertile women without obvious cause for infertility is estimated to be 1% to 2%. 1,2 Depending on their localization, submucosal leiomyomas (SM) and intramural leiomyomas (IM) have been implicated in the infertility etiology. 1,3 Significantly lower implantation and pregnancy rates have been reported in women with SM. 4 Submucosal myomectomy increases pregnancy rate of these patients. 5,6 Contrary to previous beliefs, reduced implantation and pregnancy rates have been noted in women with intramural fibroids, even in the normal endometrial cavity. 4,7 Surgical removal of intramural fibroids greater than 4 cm may therefore improve pregnancy and delivery rates. 5 . Conversely, subserosal leiomyomas do not affect pregnancy rates. 7 Host myometrium of the myomatous uterus differs from normal myometrium 8 . Several hypothesis including inhibition of sperm and blastocyst transport, dysfunctional uterine contractility, and defective implantation have been suggested to explain how leiomyomas cause infertility, but none is definitive. 1,9,10 Recent immunocytochemical study has demonstrated that concentrations of estrogen receptors increased in the host myometrium of women with leiomyomas. 11 This may disturb the subendometrial myometrial contractions. The causal relationship in this regard appearing to be more evident for SM. 8 However, a recent comprehensive review by Donnez and Jadoul highlighted the lack of scientific evidence necessary to establish a causal relationship between leiomyomas and infertility or to evaluate the potentially beneficial effects of surgery on the reproductive outcome. 12
Uterine septum is the most common type of congenital uterine malformation, approximately with 80% to 90% of all uterine malformations. It has been reported that presence of septate uterus may cause infertility. 13,14 It is plausible that uterine septum adversely affects the endometrium and hence impair endometrial receptivity. Nevertheless, little is known how uterine septum lead to infertility.
To date, it remains to be clarified whether surgical treatment of uterine fibroids and uterine septum improves endometrial receptivity. Most of the researchers have shown a better reproductive outcome after myomectomy, and the difference is evident when the leiomyoma was the only identifiable cause of infertility. 15,16 Likewise, many studies have confirmed the validity of metroplasty to improve reproductive functions. 14,17,18 However, increased pregnancy rates following myomectomy and metroplasty are based on the only clinical observations. 14,17,18 We, therefore, have little information how myomectomy and metroplasty improve fertility, and little is known which molecular events occur inside the endometrium following endometrium surgery. HOXA-10 is a member of the abdominal B-related subclass of homeobox genes. 19
HOXA-10 messenger RNA (mRNA) expression is necessary for successful endometrial receptivity. 20 In the secretory phase at the time of implantation, endometrial HOXA-10 mRNA expression is upregulated 20 and improve the endometrial receptivity. 21 Moreover, HOXA-10 mRNA expression regulates downstream target genes, which are involved in implantation including integrin β3. 22 Similar to HOXA-10 mRNA, endometrial HOXA-11 mRNA expression has an important role in endometrial development and implantation. 23 A recent study has demonstrated that endometrial HOXA-10 and HOXA-11 mRNA expression in patients with SM is altered, whereas those of patients with IM are comparable to controls. 24
Integrins are heterodimeric integral membrane proteins composed of an α and β chains. ITGAV gene encodes the αv protein that is a member of the integrin family. Integrin αv has heterodimerized with β3 chain (ITGB3) that is expressed on the luminal and glandular epithelium of the endometrium where facilitates angiogenesis and embryo attachment. 25,26 Its aberrant expression in a variety of reproductive disorders including luteal phase defect, endometriosis, polycystic ovarian syndrome, and tubal disease suggests a critical role for this protein. 27 -29 In humans, endometrial leukemia inhibitory factor (LIF) mRNA expression is essential for blastocyst implantation, and its expression increases in the secretory phase. 30,31
Unfortunately, there is no comprehensive endometrial study investigating the effects of myomectomy and metroplasty on expression patterns of endometrial receptivity markers such as homeobox genes and integrins. In this study, we attempted to investigate whether myomectomy of IM alters endometrial HOXA-10, HOXA-11, ITGB3, ITGAV, and LIF mRNA expression in infertile women with IM not distorting the endometrial cavity. We evaluated expression of these genes in endometrium before and after myomectomy during the mid-secretory phase. In addition, to assess the specificity of the results, we included infertile women with SM, uterine septum, and fertile women without uterine leiomyomas as controls.
Materials and Methods
This case–control study included 28 participants: 7 with SM, 7 with IM not distorting the endometrium, 7 septate uterus, and 7 fertile controls with macroscopically normal pelvic cavities who were undergoing tubal sterilization or reversal of tubal sterilization. We investigated the expression levels of HOXA-10, HOXA-11, LIF, ITGB3, and ITGAV mRNA in the endometrium of 14 infertile patients undergoing a routine workup and being diagnosed by transvaginal ultrasonography as having submucosal or intramural myomas as their sole cause of infertility. The diagnosis of septate uterus was made by American Society for Reproductive Medicine (ASRM) classification criteria. 32 Submucosal fibroids were classified by the European Society of Hysteroscopy. Type 0: pedunculated SM which do not have intramural interference; type I: stemless SM having less than 50% intramural interference; and type II: stemless SM having more than 50% intramural involvement. 33
All of the infertile women underwent a routine laboratory and radiological examination to diagnose the underlying factors of infertility. The infertile women had normal mid-luteal progesterone levels indicating the presence of ovulation, normal 2 semen analyses evaluated at least 3 weeks apart and upon 3 to 7 days of abstinence and normal hysterosalpingography with bilateral tubal patency and the only detectable cause of infertility was uterine fibroids. The fertile women enrolled as the control groups had at least 2 children and had no history of infertility or habitual abortion.
All the participants were required to meet the inclusion criteria: (1) presence of pathological diagnosis of uterine fibroids in women who underwent myomectomy, (2) no hormonal medication and intrauterine contraception use within the last 6 months before enrollment to the study, (3) patients with regular menstrual cycles, and (4) minimum 2 years of infertility duration. The following exclusion criteria were applied: (1) previous medication use; (2) previous endometrial pathology such as Asherman syndrome or endometrial polyp; (3) diagnosis of pelvic inflammatory disease, deep endometriosis, adenomyosis, and hydrosalphinx at the time of the study; (4) previous surgeries that might affect the original shape of the uterus and endometrial cavity, such as metroplasty, myomectomy and prior removal of part of uterus; (5) history of habitual abortion; (6) infertility etiology other than fibroids and uterine septum; (7) mechanical distortion of the endometrial cavity by intramural fibroids; (8) patients with male factor infertility or bilateral tubal occlusion; and (9) women with out of date endometrium on the pathological evaluation of endometrium.
All participants with intramural fibroids underwent saline infusion sonography (SIS) and office hysteroscopy for assessment of mechanical distortion of the endometrial cavity. Presence of mechanical distortion of the endometrialcavity by intramural fibroids was excluded from study. Following office hysteroscopy and SIS, all participants in SM group underwent hysteroscopic myomectomy. Patients with intramural fibroids underwent laparotomic myomectomy. Participants having septate uterus underwent hysteroscopic septum resection (metroplasty). Women having SM underwent hysteroscopic myomectomy by using 2 steps technique.
All patients, independent of group, were selected for the present study on the basis of consistent histological findings, menstrual history, and serum progesterone levels. The mid-luteal phase was calculated as the 7 to 9 days after the ultrasonographic confirmation of ovulation and was confirmed by endometrial histological dating and serum progesterone levels. All menstrual cycles studied in the current study were ovulatory according to mid-luteal serum progesterone >10 ng/mL. Endometrial samples were obtained just prior to myomectomy or uterine septum resection and respective endometrial tissues 3 months after the surgery using an endometrial pipella catheter during mid-luteal phase. In addition, endometrial tissues were obtained from healthy fertile women during mid-luteal phase. Endometrial dating was performed by an independent pathologist. Hematoxylin and eosin and periodic acid-Schiff stained specimens were evaluated according to the histopathological criteria of Noyes et al. 34 An out-of-date biopsy was defined as a lag of ≥3 days between the chronological and the histological day. 35 The study protocol was approved by the institutional Ethical Committee for Research on Human Subjects.
RT-PCR
Sample preparation
The tissue samples (at least a 30 mg) were immediately transferred into RNA stabilization buffer (RNALater, Qiagen, Hilden, Germany) to stabilize and protect RNA in tissue and subsequently stored at -−80°C until used. Tissue samples were homogenized in RNALater using a TissueLyser (Qiagen, Hilden, Germany).
Total RNA isolation
Total RNA was isolated using the RNeasy Mini Kit (Qiagen, Hilden, Germany) from the homogenized tissue samples. From each sample, RNA quantity and purity were measured spectrophotometrically using the MaestroNano (Maestrogen, nano, Taiwan).
Reverse transcription complementary DNA synthesis
Complementery DNA (cDNA) was obtained by using QuantiTect Reverse Transcription (Qiagen, Hilden, Germany) kit. This system consists of 2 major steps, reverse transcription and removing genomic DNA. Genomic DNA eliminated by incubating each RNA sample in Wipeout buffer at 42°C. Following that, reverse transcription mix (1 µL Quantiscript Reverse Transcriptase, 4 µL Quantiscript RT Buffer, and 1 µL RT Primer Mix) and target RNA at 1 µg concentration in 20 µL total volume were prepared on ice reverse transcription procedure. Reaction mix was incubated at 42°C for 15 minutes and then was kept at 95°C for 3 minutes to inactivate reverse transcriptase. The Quantiscript Reverse Transcriptase (Qiagen, Hilden, Germany) used in that system has high affinity to RNA and was optimized for RNA at a range of 10 pg to 1 µg concentrations.
Expression of HOXA-10, HOXA-11, LIF, ITGAV, and ITGB3 genes by In-House RT-PCR
Primers used in that study have been designed by PrimerDesign (Primer Design Ltd, United Kingdom). In addition, standard positive controls for each gene were synthesized by PrimerDesign to analyze polymerase chain reaction (PCR) reaction efficacy. β-Actin gene (ACTB) was used as house-keeping gene. The mRNA level of each sample was normalized to that of the β-actin mRNA level. Real-time PCR reaction was performed by using Quantitect Probe PCR Kit (Qiagen, Hilden, Germany) and RotorGeneQ (Qiagen, Hilden, Germany) Real-time PCR device according to manufacturers’ instructions. Real-time PCR results are expressed as cycle threshold (Ct), delta Ct (▵Ct) and ddCt (▵▵Ct). For calculation of average Ct values, each endometrial sample is studied 3 times (Figure 1). Sequences and accession numbers of all primers designed to be used as forward and reverse primers for RT-PCR are:
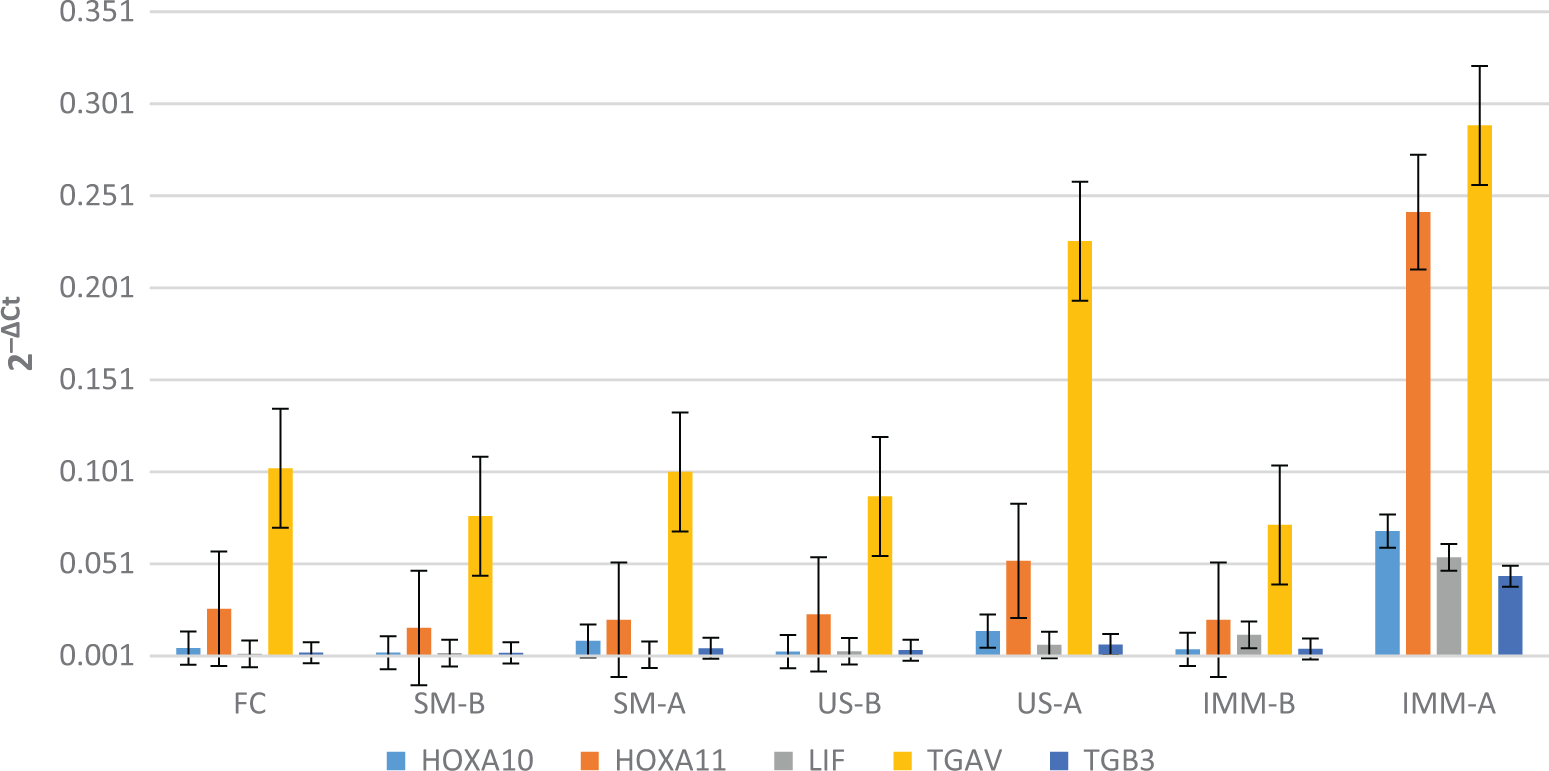
The 2−▵CT value of HOXA-10, HOXA-11, LIF, ITGAV, and ITGB3 mRNA expression in all groups. FC indicates fertile control; IM-B, before intramural myomectomy; IM-A, after intramural myomectomy; SM-B, before submucosal myomectomy; SM-A, after submucosal myomectomy; US-B, before uterine septum resection; US-A, after uterine septum resection.
HOXA-10(NM_018951), F-5′-GGTTTGTTCTGACTTTTTGTTTCT-3′, R-5′-TGACACTTAGGACAATATCTATCTCTA-3′; HOXA-11(NM_005523), F-5′-AGTTCTTTCTTCAGCGTCTACATT-3′, R-5′-TTTTTCCTTCATTCTCCTGTTCTG-3′; LIF(NM_002309), F-5′-GGAGGTCACTTGGCATTCAG-3′, R-5′-GGAAGAGAACGAAGAACCTACC-3′; ITGAV(NM_002210), F-5′-AAACAGAATTTGTAAGTTGGCAGAT-3′, R-5′-GGTGACATTGAGATGGGTAGTG-3′; ITGB3(NM_000212), F-5′-ACCATCTCTTTACCTCCTAATTCC-3′, R-5′-CTGGCTCTACAATAGCACTCTC-3′; ACTB(NM_001101), F-5′-GCAAGCAGGAGTATGACGAGT-3′, R-5′-CAAGAAAGGGTGTAACGCAACTAA-3′.
Statistical Analysis
The relative gene expression was determined by using the 2−ΔΔCT comparative method with RT2 Profiller PCR Array Data Analysis version 5.5 (SABiosciences, Qiagen, Hilden). All data were normalized according to ACTB gene (β-actin) mRNA content. Fold-change (2-▵▵CT) is the normalized gene expression (2-▵CT) in the patient group divided the normalized gene expression (2-▵CT) in the fertile control. Fold change greater than 3 indicates a positive- or an upregulation, and the fold-regulation is equal to the fold change. Fold change less than 2 indicates a negative or downregulation, and the fold-regulation is the negative inverse of the fold change.
Comparative RNA expression analysis in all groups versus fertile control (calibrator) was performed as follows:
Fertile control group: ▵Ct = Ct (target gene) − ▵Ct (housekeeping gene; ACTB)
Patient group: ▵Ct = Ct (target gene) − ▵Ct (housekeeping gene; ACTB)
▵▵Ct = ▵Ct (patient group) − ▵Ct (fertile control group)
Fold ratio = 2-▵▵CT
The normality distribution of data was performed by using Kolmogrov- Smirrnoff test, and all variables were skewed normally. The continuous variables were analyzed by analysis of variance test with post hoc Tukey’s procedure and Mann-Whitney U test. The categorical data were analyzed by the Pearson chi-square test. A P value <.05 was considered significant. The results are expressed as mean and standard deviation. Fold increase was considered positive for transcript overexpression when the corresponding mRNA level was at least 3-fold higher than that of initial transcript expression, negative if lower than 2-fold.The data were analyzed by using the Statistical Package for Social Sciences software 19.0 for Windows package software (SPSS, Inc, Chicago, Illinois).
Results
The average patients age was 31.3 years (range 27-34 years). Of 7 participants with SM, 2 had a single pedinculated fibroid (type 0); 3 had less than 50% intramural involvement (type 1); and 2 had more than 50% intramural involvement (type 2). The average number of submucosal fibroids was 1.71 (range 1-3), and the average size of 5 sessile and 2 pedinculated fibroids were 3 cm. Of seven women with IM, 3 had a single fibroid, 4 had myomas more than 1. The average number of intramural fibroids was 2.42 (range 1-4), and the average size of these fibroids was found to be 4.29 cm. In regard to the average size and numbers of fibroids there were no significant difference between submucosal and intramural groups. Of 7 participants with uterine septum, 4 had totally division of uterine cavity and cervical canal, 3 had partially division of uterine cavity without partially septate cervix. Between the study groups, there were no differences in mean age, fertility history, or other medical conditions. No differences in serum concentrations of progesterone were detected among groups. All endometrial samples underwent histologic evaluation, and normal secretory endometrium was identified.
We were able to completely remove all fibroids located on the mural region. Similarly, uterine septum was successfully resected in all pariticipants. Two pedinculated fibroids were removed successfully. Complete resections of the submucosal and mural components of the fibroids were achieved in all 3 type 1 cases. Despite 2 steps hysteroscopic myomectomy technique, surgical removal of mural components of the 2 cases those having more than 50% intramural involvement (type 2) were incomplete. During the 6-month follow-up period, pregnancy did not occur after the myomectomy of pedinculated submucosal fibroids. One case with type 1 SM and 1 case with type 2 SM became pregnant. In the intramural myomectomy group, only 2 patients were able to remain pregnant. Interestingly, their fibroids size were found to be greater than 5 cm. But one of them ended in early miscarriage. After the metroplasty, only 1 patient was able to remain pregnant.
Endometrial mRNA Expression Levels of Receptivity Genes in the SM, IM, and Uterine Septum Groups Before the Surgery
Expression levels of HOXA-10, HOXA-11, and ITGAV mRNA were lower in the endometrium of infertile patients with SM and IM before myomectomy as compared with healthy fertile controls. However, the differences failed to show statistical significance. Likewise, there were no statistically significant differences between the SM and IM groups in terms of endometrial HOXA-10 and HOXA-11 mRNA expression levels before surgery (Table 1 and Figure 1).
Comparison of Preoperative and Postoperative Endometrial HOXA-10, HOXA-11, LIF, ITGAV, and ITGB3 mRNA Expression Between Women With IM, SM, and Uterine Septum.
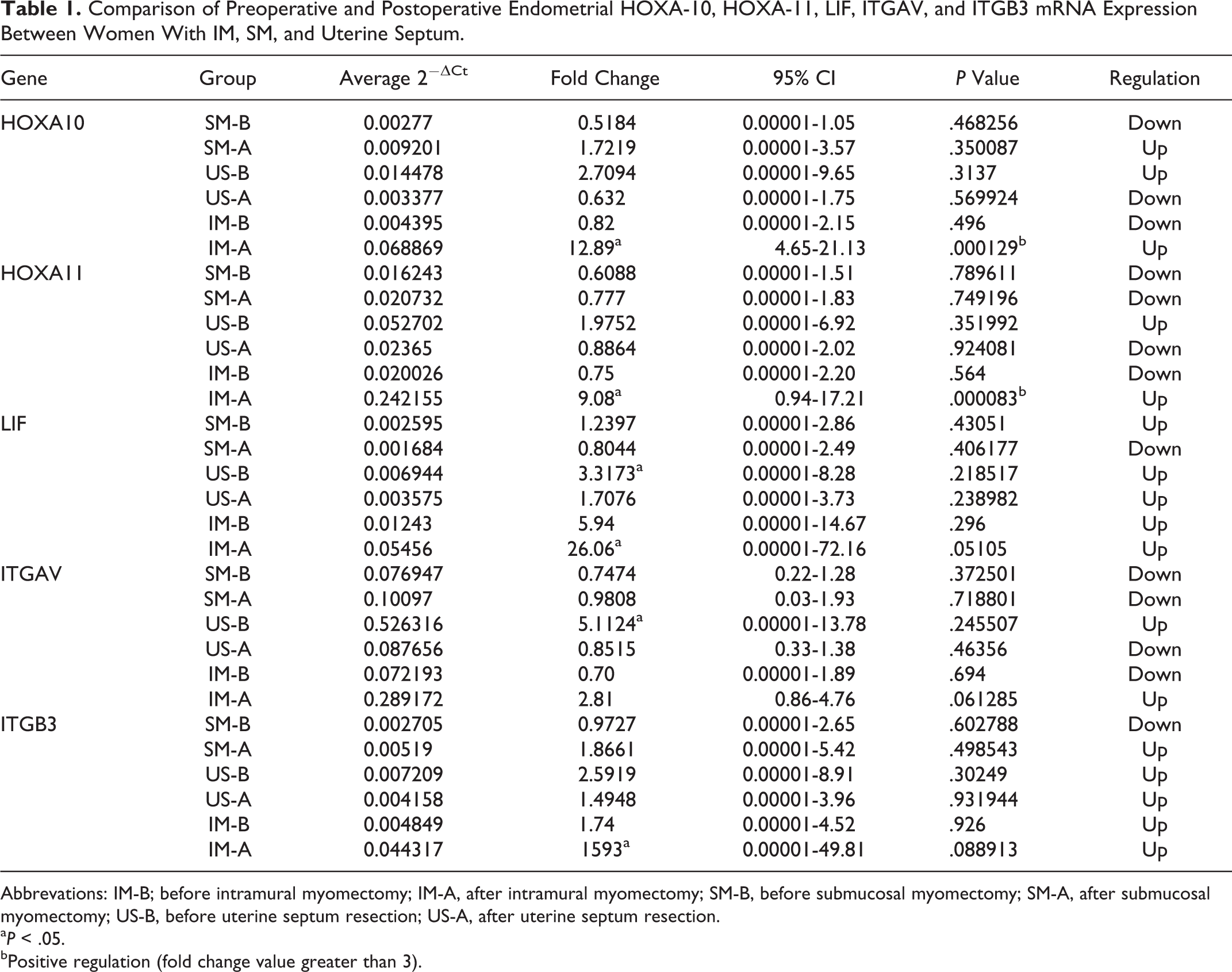
Abbrevations: IM-B; before intramural myomectomy; IM-A, after intramural myomectomy; SM-B, before submucosal myomectomy; SM-A, after submucosal myomectomy; US-B, before uterine septum resection; US-A, after uterine septum resection.
a P < .05.
bPositive regulation (fold change value greater than 3).
When compared to fertile controls, mRNA expression levels of 5 studied receptivity genes were found to be insignificantly upregulated in women with uterine septum before metroplasty.
Similarly, when compared to uterine fibroids, insignificant upregulation was detected in endometrial HOXA-10 and HOXA-11 mRNA expression levels in women with uterine septum before surgery.
Endometrial mRNA Expression Levels of Receptivity Genes in the SM, IM, and Uterine Septum Groups After the Surgery
Surgical removal of IM have upregulated the endometrial HOXA-10 and 11 mRNA expression levels. This upregulation in endometrial HOXA-10 mRNA expression levels has reached the statistical significance (0.004 vs 0.06; P < .0001). Similarly, expression levels of HOXA-11 mRNA after myomectomy were significant (0.02 vs 0.2; P < .00008). After myomectomy of IM, we have detected 12.8-fold increase in endometrial HOXA-10 mRNA expression and 9.0-fold increase in endometrial HOXA-11 mRNA expression (Table 1 and Figure 2). Fold change increase in HOXA-10 and HOXA-11 mRNA was statistically significant When compared to preoperative fold change values, postoperative fold change values of women with IM with respect to LIF, ITGB3, and ITGAV were found to be increased. After myomectomy of IM, we have detected 26.0-fold increase in endometrial LIF mRNA expression, 15.9-fold increase in endometrial ITGB3 mRNA expression, and 2.81-fold increase in endometrail ITGAV mRNA expression (Table 1 and Figure 2).This increase in fold change values for LIF and ITGB3 mRNA expression was found to be greater than 3, which indicate positive regulation, but they did not reach the statistical significance (P = .051 and .08, respectively). Likewise, fold increase in postoperative ITGAV mRNA expression in the IM group was insignificant (2.81-fold, P = .06).
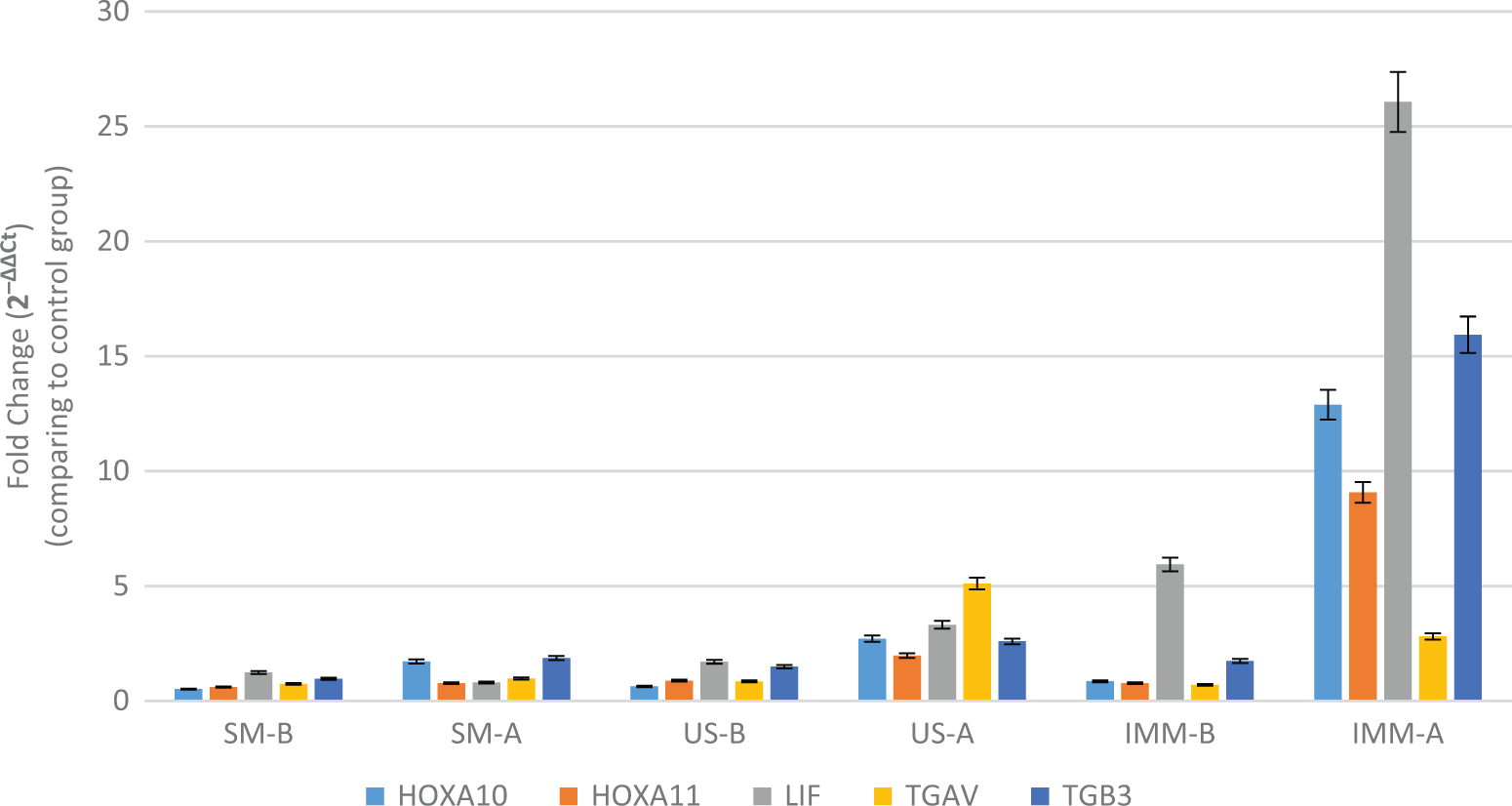
The relative gene expression was determined by using the 2−ΔΔCT method. All data were compared to the fertile controls and normalized to β-actin (ACTB) gene messenger RNA (mRNA) content. Record the 12.8-fold increase in HOXA-10, 9.0-fold increase in HOXA-11, 26.0-fold icrease in LIF, and 15.9-fold increase in ITGB3 mRNA expression after myomectomy.
Surgical removal of SM have upregulated the endometrial HOXA-10 and 11 mRNA expression levels. However, upregulation of HOXA-10 mRNA was insignificant. Likewise, expression levels of endometrial HOXA-11 mRNA after myomectomy of SM did not reach statistical significance (0.01 vs 0.02; P = .7, Table 1 and Figure 1). Fold change values of women undergoing submucosal myomectomy in terms of HOXA-10 and HOXA-11 were found to be insignificant (1.7-fold vs 0.7-fold, respectively). Insignificant downregulation is detected in the LIF and ITGAV mRNA expression after submucosal myomectomy (0.8-fold, P = .40 vs 0.9-fold, P = .71, respectively). Also, upregulation of ITGB3 mRNA expression after submucosal myomectomy was noted as insignificant (1.8-fold, P = .49).
While the expressions levels of HOXA-10, HOXA-11, and ITGAV mRNA have upregulated, ITGB3 and LIF mRNA expressions have downregulated after metroplasty. However, neither downregulation nor upregulation of receptivity genes reach the statistical significance.
Discussion
When reviewing the literature, controversial results are obtained in relations between leiomyomas and infertility research because of the heterogeneity of women suffering from leiomyomas. Patients with different anatomical location of leiomyomas often being included in the same study group. In the context of reproduction, it is well known that the SM, IM, and subserosal leiomyomas have an detrimental effect on fertility outcome in decreasing order of importance. Additional controversial conclusions come from the status of uterine cavity during the diagnosis of leiomyomas. The effect of IM on the endometrial cavity is much more difficult to evaluate. Conflicting results from various studies can be attributed to the unsuitable patient selection and lack of precision in the description of the location of leiomyomas. 36 Presence of leimyomas in women undergoing in vitro fertilization embryo transfer (IVF-ET) do not influence pregnancy rates if they have no force on the endometrial cavity. 37,38 Conversely, the presence of leiomyoma, even one have normal endometrial cavity, decreases pregnancy rates. 7,39 Likewise, Horcajadas et al. 40 have reported that IM do not distorting the endometrial cavity change the expression pattern of some endometrial genes, but the genes involved in endometrial receptivity are not affected. They found that GPx3, placental protein 14, and aldehyde dehydrogenase 3 family, member B2 genes were downregulated in the endometrium with large IM. To avoid these handicaps, the inclusion of patients in our study was restricted to infertile patients with IM having SIS and hysteroscopically normal endometrial cavity. Patients having mechanical distortion of the endometrial cavity by IM were excluded from study. To prove a possible relation between fertility improving and surgical interventions (such as myomectomy or endometrioma resection), appropriate controls without the diseases are required to evaluate endometrial receptivity. 41,42 This was realized in the current study where fertile women were used. On the other hand, a normal appearing endometrial environment in patients with leiomyomas could not be related to the leiomyoma itself but to the infertility. Thus, we used a second control group of infertile women with uterine septum who may have clinical and surgical profiles mimicking those of leiomyomas.
In the present study, a trend toward decreased endometrial HOXA-10, HOXA-11, and ITGAV mRNA expression was noted in the SM and IM groups before surgery compared to controls. However, this downregulation does not reach the statistical significance. In terms of SM, our results are not consistent with the results of previous study which was carried out by Rackow and Taylor. 43 These authors demonstrated that endometrial HOXA-10 and HOXA-11mRNA expressions were significantly decreased in endometrial samples from the participants with SM. 43 They also reported that, compared to endometrium obtained from IM, significantly decreased endometrial HOXA-10 mRNA expression was noted in biopsies obtained from over the SM. In contrast, in our study endometrial HOXA-10 and HOXA-11 mRNA expression levels of submucosal and IM were similar before surgery. In regard to IM, our findings are consistent with the results of Rockow et al. 43 They did not report any difference in endometrial HOXA-10 mRNA expression in women with IM compared to controls. But in contrast to our study, they investigated endometrial HOXA-10 and HOXA-11 mRNA expression during the proliferative phase. Endometrial HOXA-10 mRNA expression varies during the menstrual cycle, with a remarkable increase in the mid-secretory phase. 23 Therefore, endometrial biopsy taken in proliferative phase can lead to misinterpretation of HOXA-10 and 11 mRNA expression. Likewise, Matsuzaki et al 44 showed that 68.8% of patients with leiomyomas had decreased HOXA-10 mRNA expression suggesting that only certain patients with uterine leiomyomas might have alteration of HOXA-10 mRNA expression. However, their study has been conducted on only infertile patients with intramural and subserosal leiomyomas, but patients with SM were excluded.
Many researchers studied on pregnancy outcome after myomectomy but they did not investigate the endometrial receptivity genes before and after myomectomy. They, therefore, concluded improved pregnancy rates after myomectomy based on clinical observations. Bulletti et al have reported that infertile women with leiomyomas have higher delivery rates after myomectomy than infertile women without leiomyomas and infertile women with unoperated leiomyomas. 42 Casini et al 6 also reported similar findings when comparing women having myomectomy to those with no surgical treatment. Similar pregnancy rates have been reported for abdominal, laparoscopic, and hysteroscopic myomectomies. 45 -47 In the current study, intramural myomectomy of patients having normal uterine cavity upregulated the endometrial HOXA-10 and HOXA-11 mRNA expression. After myomectomy of IM, we have detected 12.8-fold increase in HOXA-10 mRNA and 9.0-fold increase in HOXA-11 mRNA expression indicate defective endometrial receptivity although there is no deformation of endometrial cavity. Furthermore, after intramural myomectomy, we have detected 26.0-fold increase in LIF mRNA and 15.9-fold increase in ITGB3 mRNA expression, suggesting positive regulatory effect of myomectomy. Although endometrial HOXA-10 mRNA expression is globally affected in the presence of a SM, 43 we do not have sufficient information about the impact of IM on the molecular environment of endometrium. The present findings and those by Rackow and Taylor 43 suggest that IM not distorting the endometrial cavity may have a detrimental effect on the endometrium that impairs endometrial receptivity.
Endometrium of women with IM may appear histologically normal but, in fact, may show molecular abnormality. In line with, it has been reported that glandular endometrial atrophy is the most frequently noted histological finding secondary to fibroids. 48 Nevertheless, we did not find any specific histological changes in the endometrium of intramural fibroid group. In good agreement with our findings that many animal species suffering form infertility do not display histological evidence of defective endeometrium suggesting presence of endometrial molecular defect. For instance, endometrium of Hoxa10-deficient mice exhibits normal histological appearence. 49 It is, therefore, likely that defective regulation of some growth factors and cytokines inside the endometrial cells of women with IM may be responsible for damaged endometrial receptivity. 50 Harmful signaling molecules that originates from the IM may reach to the endometrium via intercellular communication routes and may contribute to negative endometrial effects.
In addition to endometrium-derived regulatory factors and cytokines bone morphogenetic protein 2 (BMP-2), is a growth factor that belongs to the transforming growth factor β (TGF-β superfamily and has a pivotal role for embryo implantation. 51 We, therefore, hypothesized that reduced implantation and pregnancy rates in women with IM may be secondary to impaired BMP-2-mediated decidualization. Data supporting our hypothesis comes from 2 excellent studies. Sinclair et al. have reported that leiomyoma-derived TGF-β3 induces BMP-2 resistance in endometrium and leads to disturbance on endometrial decidualization. 52 They also showed that treatment of leiomyoma-associated endometrial stromal cells with recombinant human BMP-2 caused the decline in both HOXA-10 and LIF genes expression. Interestingly, inhibition of TGF-β signaling by using TGF-β antibody restored BMP-2-stimulated expression of HOXA10 and LIF genes. 53 These results support the presence of BMP-2 resistance in leiomyoma-associated endometrial stromal cells. 52,53 In view of the above-mentioned studies and our results when taken together interruption of TGF-β signaling may be a potential approach to improve reduced implantaion rates associated with leiomyomas. Accordingly, leiomyoma-derived TGF-β signals can be prevented in either medical treatment or surgical intervention. For now, we do not have any drug that will stop these signals. The only alternative we have is to remove leiomyomas with surgery. Because of TGF-β3 is secreted in large amounts by uterine fibroids 54 surgical removal of IM inhibits TGF-β3 secretion and prevents BMP-2 resistance and increases the expression of HOXA-10 and HOXA-11 mRNA. As a consequence, we can strongly suggest that myomectomy of IM may increase endometrial receptivity by restoring endometrial BMP-2 resistance.
In the present study, surgical removal of IM have caused pronounced effect on endometrium and lead to significant increase in the expression of homeobox genes. During short follow-up period, 2patients having intramural myomectomy were able to remain pregnant. But one of them resulted in a miscarriage. It may be coincidental but both patients’ mymom sizes were greater than 5 cm. Our findings are consistent with the findings of Bulletti et al 5 who suggested that intramural myomectomy is likely to be beneficial for women with intramural fibroids bigger than 4 cm. As a consequence, significant up-regulation of endometrial receptivity markers after myomectomy and conceive of two patients lead us to believe that IM which do not distort the endometrial cavity may disturb the endometrial receptivity. We can conclude that there is a direct link between the IM and the infertility and we can vigorously hope to improve fertility by surgically removing of the IM.
In the present study, endometrial HOXA-10 and HOXA-11 mRNA expressions were found to be unchanged after myomectomy of SM. Similarly, submucosal myomectomy has not affected the fold change values of HOXA-10 and 11 mRNA. Furthermore, after submucosal myomectomy, we have detected insignificant fold change for LIF, ITGAV, and ITGB3 transcripts. Insignificant upregulation of endometrial HOXA-10 and ITGB3 mRNA expression after submucosal myomectomy can be attributed to the intramural remnants of the SM. In our clinical practise, intramural portion of the some SM could not be fully removed during hysteroscopic myomectomy. Data supporting our “intramural remnants” hypothesis comes from 2 different studies. Horcajadas et al 40 have showed that endometrial GPx3 gene expresses abnormally in the presence of small IM, suggesting that endometrial receptivity may be disturbed in the presence of the small intramural lesions. Consistent with this, Khalaf et al have reported that the presence of small leiomyomas is associated with reduced ongoing pregnancy rates in IVF-ET. 55 Hence, the remaining parts of the SM tissue after myomectomy might continue to send the diffusible signaling molecules which cause the persistence of endometrial receptivity defect. On the other hand, there was a trend toward a higher pregnancy rates after myomectomy of sessile fibroids. During the follow-up, myomectomy of submucosal fibroids with intramural involvement has led to pregnancy in 2 patients. One of them has an intramural remnant due to incomplete resction. These data do not support our “intramural remnant hypothesis.” Inability to conceive of pedinculated fibroid cases after myomectomy suggests that endometrial receptivity cannot benefit from myomectomy. Taken together, submucosal fibroids not only adversely affect fertility through the endometrial receptivity but also they may have a harmful mechanical effect on endometrial receptivity.
Different origin of submucosal fibroids may explain the possible relationship between endometrial receptivity and fibroids which are located in different submucosal areas. Pathophysiological data suggest that SM, which arise from junctional zone myocytes, are distinct from other leiomyomas. 8 As a consequence, SM are likely to have a profound effect on successful implantation. 8 Both myometrium and leiomyomas express HOXA-10 in the menstrual cycle, and stage-specific regulation is evident in both tissues. 56 In addition, SM are associated with a general decrease in HOXA-10 expression in the surrounding endometrium. 21 This finding correlates with the clinical observation that submucous fibroids are detrimental to pregnancy outcome. Hence, we can suggest that endometrial receptivity defect might be continued after submucosal myomectomy due to defective myometrium is seen in the SM. Therefore, incresed clinical pregnancy rates after submucosal myomectomy might be attirubuted to mechanical factors rather than endometrial receptivity defect. However, before concluding submucosal myomectomy does not improve the endometrial molecular defects involved in implantation, a comparison of receptivity markers should be made between patients with submucosal fibroids, which surgically removed as complete and incomplete. Our study has not been conducted in such a way, so our comment of the relationship between submucosal myomectomy and endometrial receptivity markers is not conclusive.
Hysteroscopic septum resection is a simple and safe approach for the removal of the uterine septum. 13,14 Many authors studied on pregnancy outcome after hystroscopic septum resection but they did not investigate the preoperative and postoperative endometrial receptivity markers and concluded improved pregnancy rate after surgery based on clinical observations. 57,58 Recent study by Tomaževič et al 59 have reported that the pregnancy rates before metroplasty are lower than after metroplasty in women undergoing in vitro fertilization. In the present study, we have shown that endometrial receptivity markers upregulated in women with uterine septum before the surgery. However, this upregulation does not reach the statistical significance. Likewise, expression levels of receptivity markers were found to be unchanged after septum resection suggesting preserved endometrial receptivity in patient having uterine septum. In light of this information, one might think that the reason for the increase in pregnancy rates after uterine septum resection may be due to mechanical factors rather than endometrial receptivity defect.
Regardless of the anatomical location, lower reproductive tarct lesions might be associated with implantation failure leading to molecular defect and pathological inflammation in the endometrium 1,41 For influencing the endometrial receptivity, direct contact between the endometrium and solid and/or cystic space occupying lesion is not mandatory. The lesions located along the ovary–endometrium tract might affect the endometrial receptivity markers independent of location. For example, the presence of hydrosalpinx reduces the receptivity of the endometrium by decreasing the expression of LIF and HOXA-10 and can be increased following salpingectomy. 60 -62 Likewise, in a previous study, our group has demonstrated that ovarian endometrioma increases nuclear factor-κB-related endometrial inflammation and laparoscopic removal of endometrioma decreased this inflammation. 41 More recently, we have also reported that surgical removal of endometrioma increases endometrial HOXA-10 and 11 mRNA expression. 63 From the same perspective, the impact of IM on endometrial receptivity appears to be specific to targeted signal pathways including those involving HOX, LIF, and ITGB3 transcripts.
Despite progress in medical therapies, surgery remains a mainstay of leiomyomas treatment. 50 By incresing HOXA-10 and HOXA-11 mRNA expression, myomectomy of IM had favorable affect on endometrium. These findings suggest that IM may affect endometrial receptivity through a specific and selective molecular mechanism of action. These results also imply that the mechanism by which intramural myomectomy impact endometrial receptivity is not simply removal of local mechanical effect over the endometrium but involves inhibition of detrimental signaling to the endometrium. Taken together, our results may explain the reproductive improvement clinically observed in women with IM after myomectomy. In view of the above-mentioned findings, we can assert that IM which do not distort the endometrial cavity might have deleterious effects on endometrial receptivity markers. Despite the short follow-up period and scarcity in the number of cases, we can strongly suggest that intramural myomectomy has a beneficial effect on fertility outcome. In the absence of appropriately designed trials, it is difficult to recommend routine myomectomy for intramural remnants of SM.
Footnotes
Acknowledgments
We are most grateful to all the patients who kindly participated in thepresent study. We also thank theTurkish German Gynecological Resarch and Education Foundation which supported this study.
Authors’ Note
CU, OC, and NC all contributed to the design and preparation of the manuscript and gave final approval of the version to be published. BO carried out gene analysis and interpreted gene results, in addition to drafting methods and graphics, article revision, and final approval of the version to be published.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by the Turkish German Gynecological Resarch and Education Foundation.