
Abstract
Objective:
To evaluate the efficacy of 2 different regimens for labor induction in patients with unfavorable cervix not responsive to a first dose of dinoprostone vaginal insert.
Methods:
Between November, 2011 and June, 2014, 338 patients underwent induction of labor. After standard 24 hours treatment, 94 singleton term pregnancies remained with a Bishop score ≤6 and were randomized into 2 different regimens: repeated vaginal dinoprostone (group A, n = 47) or intravenous oxytocin (group B, n = 47). Primary outcome was vaginal delivery, and the secondary outcomes were interval between labor induction and delivery and operative delivery rates.
Results:
Vaginal deliveries were significantly higher (group A: 26/47 (55.3%) and group B 16/47 (34.0%), P < .05), and cesarean sections were significantly lower (group A 21/47 (44.7%) and group B 31/47 (66%), P < .05) in patients who received a double dose of dinoprostone. The intervals between labor induction and onset of labor and between labor induction and delivery were lower in the group treated with oxytocin. Neonatal outcomes were similar in the 2 groups.
Conclusion:
A second dinoprostone vaginal insert is an effective and safe choice for patients with unfavorable cervix not responsive to a first 24 hours administration of dinoprostone for cervical ripening, and its use is associated with lower cesarean section rates.
Introduction
Induction of labor is the artificial initiation of labor before its spontaneous onset to deliver the fetoplacental unit. The goal of induction is to achieve a successful vaginal delivery that is as natural as possible. Appropriate and timely cervical remodeling is key for successful birth. Cervical remodeling can be loosely divided into 4 distinct but overlapping phases termed softening, ripening, dilation, and postpartum repair. 1 The Bishop score summarizes the cervical conditions and represents the phenotype of cervical histological changes.
Ripening occurs in the weeks or days preceding birth in women. Consequently, labor induction when the cervix is unripe, as suggested by a low Bishop score, is associated with higher incidence of prolonged labor, operative vaginal delivery, and cesarean delivery. 2,3
In women with an unfavorable cervix, all regimens of vaginal prostaglandin E2 (PGE2) are effective in improving cervical status and reducing oxytocin augmentation and meconium staining when compared with placebo or no treatment. 4 However, no studies have evaluated how to continue the induction in case of no response.
We designed a study to evaluate the efficacy of two different regimens for labor induction in patients with unfavorable cervix not responsive to a first dose of dinoprostone. The main outcome of the study was vaginal delivery, and the secondary outcomes were interval between labor induction and delivery and operative delivery rates.
Materials and Methods
This was a prospective, randomized study of pregnant women undergoing labor induction at the Unit of Obstetrics and Gynecology, Luigi Sacco Hospital, University of Milan, between November, 2011 and June, 2014. Inclusion criteria were singleton gestation, vertex presentation, gestation age ≥37 weeks, normal preinduction fetal heart rate tracing, and labor induction with a Bishop score ≤6.
Exclusion criteria were previous cesarean section or previous uterine surgery, hypersensitivity to dinoprostone or to any of the excipients, fetal malpresentation, placenta previa, estimated fetal weight ≥ 4500 g, and any contraindication for vaginal delivery. The study was approved by the Institutional Review Board of our hospital (2011-000563-28). All patients provided written informed consent.
Study Protocol
According to our clinical protocol, patients who underwent labor induction were treated with dinoprostone vaginal insert (Propess, Ferring, Saint-Prex, Switzerland). The dinoprostone suppository was inserted high in the posterior vaginal fornix. According to our clinical protocol, the suppository was removed if labor did not start within 24 hours or if uterine hyperstimulation occurred. Patients who delivered or were in labor within 24 hours were excluded from the study. After 24 hours, patients not responsive to a first dose of dinoprostone, with a Bishop score still less than or equal to 6, were randomized into 2 different regimens: repeated vaginal dinoprostone 10 mg (group A) or intravenous oxytocin (group B) after an interval of 30 minutes. The randomization was done by opening sequentially numbered opaque envelopes containing cards stating the drug for induction.
Until onset of labor, patients were hospitalized in the same setting. A 30-minute electronic fetal monitoring was performed every 6 hours in group A and continuously since oxytocin administration in group B.
The rate of oxytocin infusion was increased to achieve regular moderate to strong contractions as described in American College of Obstetricians and Gynecologists (ACOG) guidelines. 5 Briefly, oxytocin was begun at a rate of 8 mU/min and adjusted every 30 to 40 minutes, according to the uterine contractions with a maximum infusion rate of 36 to 40 mU/min. Effective contractions were defined as 3 contractions each lasting 30 to 60 seconds within 10 minutes.
Active labor was defined as cervical dilatation of 3 cm or more with a regular effective uterine contraction pattern. Failure to progress was defined as no cervical dilatation in a 4-hour interval in the active phase of labor or no descent in a 3-hour interval during the second stage of labor.
Continuous electronic fetal monitoring was performed during active labor. Classification and management of fetal heart rate were defined according to ACOG guidelines. Tachysystole was defined as 5 contractions in a 10-minute period for at least 30 minutes or a single contraction lasting at least 2 minutes. 6 Uterine hyperstimulation was managed by removing the vaginal insert or stopping the oxytocin infusion. 7 Failed induction of labor was defined as failure to enter the active phase of labor within 6 hours after maximum dosage of oxytocin infusion. Clinical management was performed by a group of providers working in our delivery unit.
Outcome Measures
The primary outcome was vaginal delivery rate. The secondary outcomes were interval between labor induction and delivery and operative delivery rates.
Sample Size Estimation
A total sample size of 158 (79 per group) women was required to provide 85% power and a 5% significance level to show a difference. To verify these assumptions, one interim analysis had been preplanned at the time when at least 50% of study participants had been randomized. The study was stopped for less efficacy of oxytocin treatment at the time of the first planned interim analysis.
Statistical Analysis
Significance of differences between patients using the dinoprostone and intravenous oxytocin was assessed by a t test for continuous variables, and by the Fisher exact test for 2 × 2 tables. Significance was set at P < .05.
Results
Between November, 2011 and June, 2014, 338 patients underwent labor induction and were treated using dinoprostone vaginal insert (Propess, Ferring, Saint-Prex, Switzerland
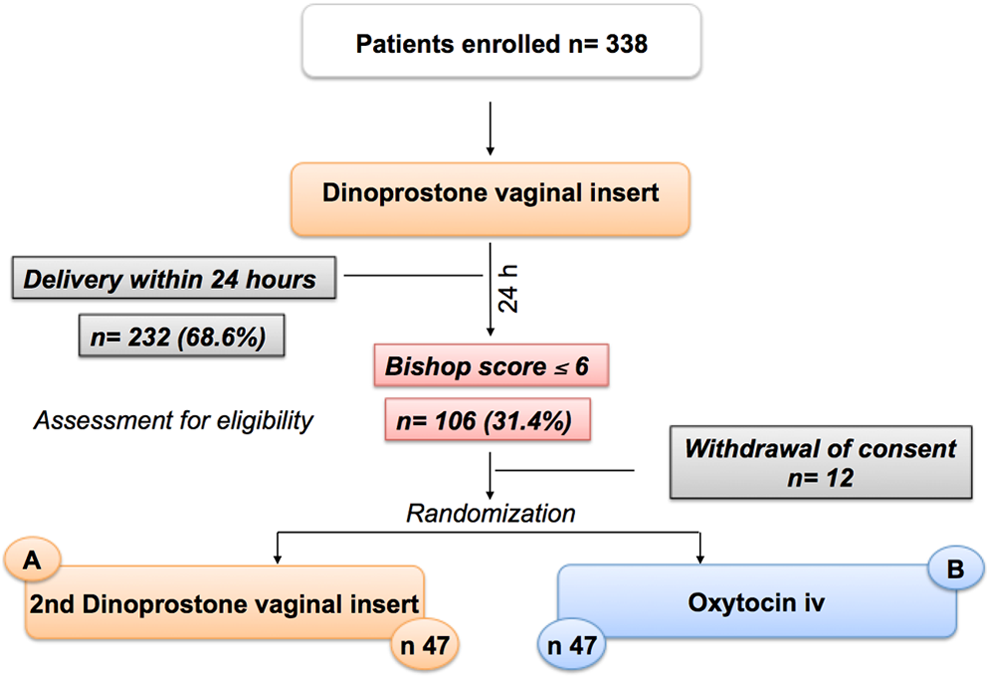
Diagram showing the flow of participants before and after randomization.
Table 1 presents the characteristics of the population. The two groups were similar in terms of maternal age, parity, prepregnancy body mass index (BMI) and gestational weight gain, Bishop score, and gestational age at labor induction. The Bishop score was not significantly different at labor induction but was greater at randomization in the group treated with oxytocin (group A: 2.6 ± 1.2; group B: 3.5 ± 1.9).
Characteristics of the Population.a
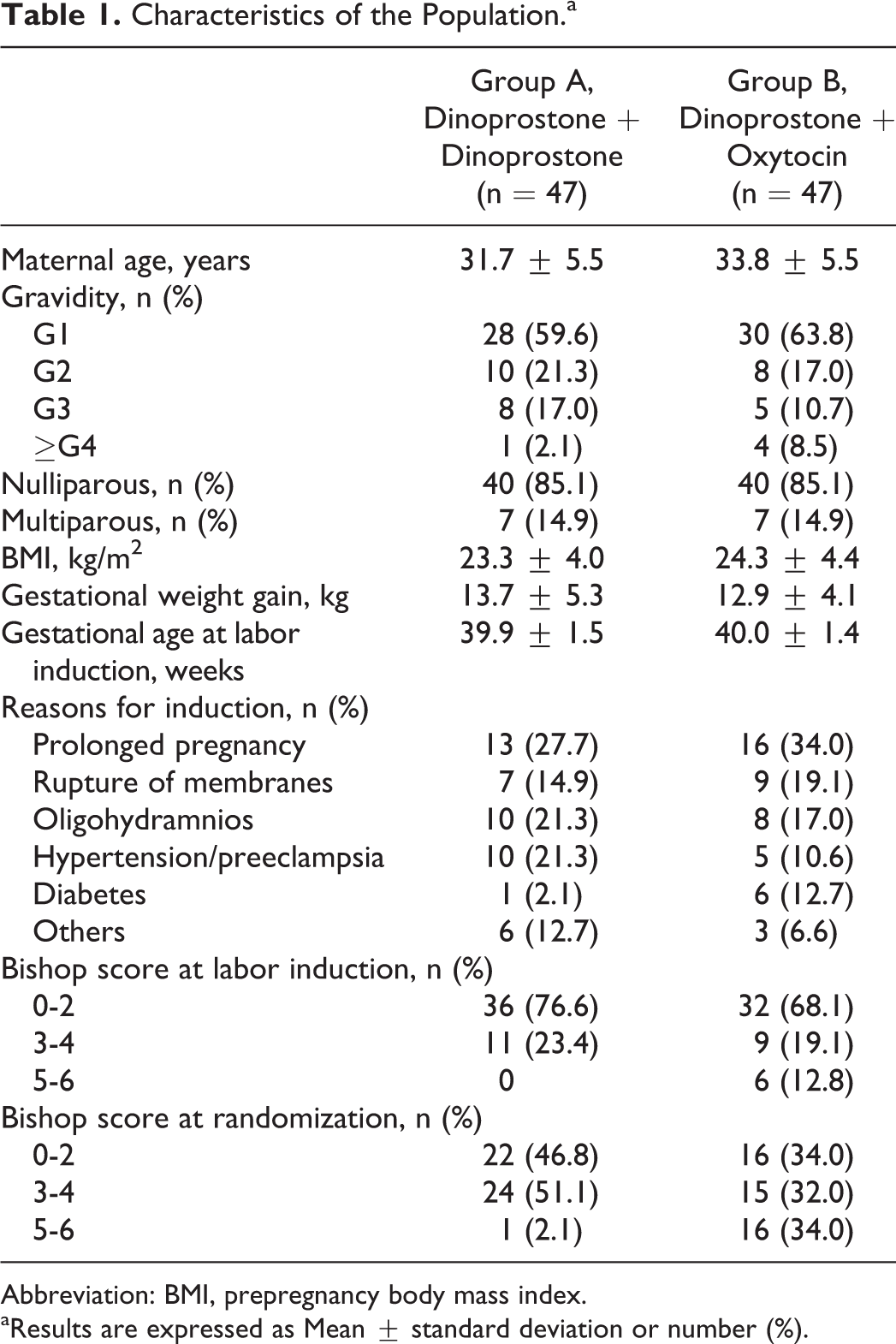
Abbreviation: BMI, prepregnancy body mass index.
aResults are expressed as Mean ± standard deviation or number (%).
Amniotomy was used as a part of labor induction protocol in 3 patients of group A and in 7 patients of group B. Mean maximum oxytocin dose was 18.7 mU/min in group A and 18.9 mU/min in group B. Mean duration of use of oxytocin infusion was 6.7 hours in group A and 6.9 hours in group B.
Table 2 presents delivery outcomes in the two groups. Gestational age at delivery was similar in the two groups. The number of vaginal deliveries was significantly higher in the group of patients who received a second dose of dinoprostone compared to women treated using oxytocin (group A: 55.3% vs group B: 34%; P < .05). Consequently, cesarean section rate was significantly higher in patients treated using oxytocin compared to patients who received a second dose of dinoprostone (group A: 44.7% vs group B: 66%; P < .05).
Delivery Outcomes.
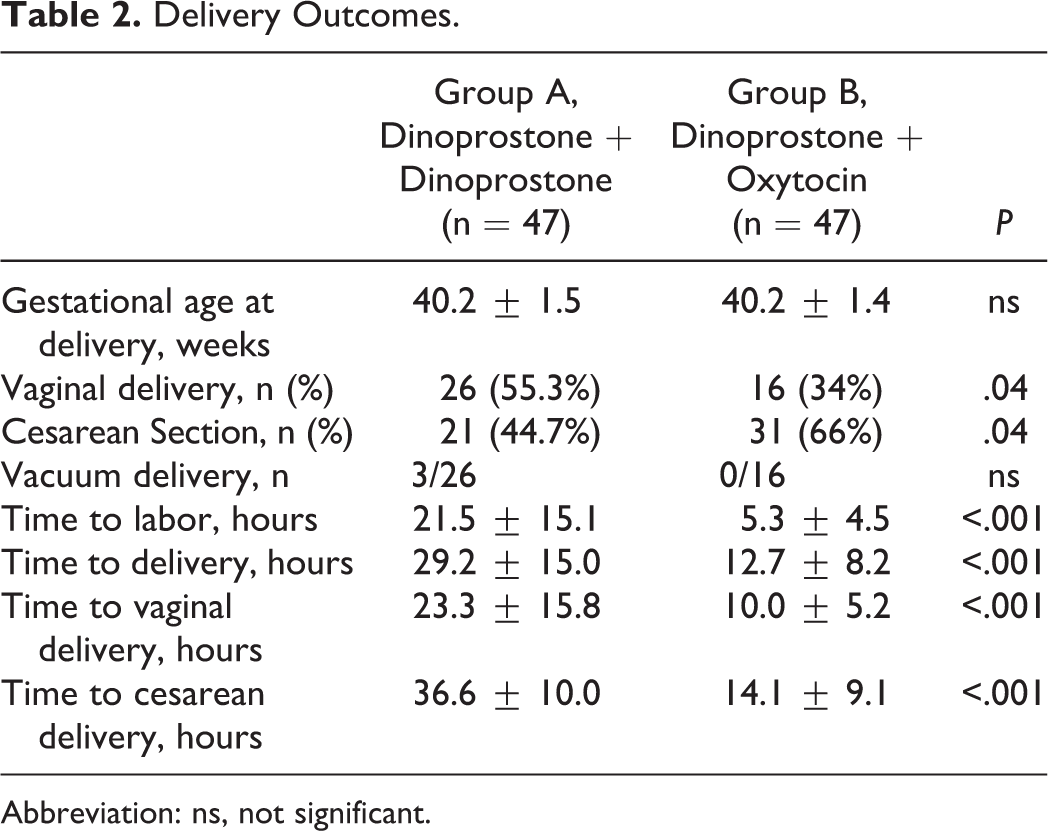
Abbreviation: ns, not significant.
Vacuum extraction-assisted vaginal delivery was performed in 3 patients in the dinoprostone group and in none of the oxytocin group. The intervals between randomization and onset of labor (group A: 21.5 ± 15.1 hours vs group B: 5.3 ± 4.5 hours; P < .001) and between randomization and delivery (group A: 29.2 ± 15.0 hours vs group B: 12.7 ± 8.2 hours; P < .001) were significantly lower in the group treated with oxytocin. This was found both for vaginal birth (group A: 23.3 ± 15.8 hours vs group B: 10.0 ± 5.2 hours; P < .001) and for cesarean section (Group A: 36.6 ± 10.0 hours vs Group B: 14.1 ± 9.1 hours; P < .001). No significant differences were found for indications to cesarean section (Table 3).
Indications to Cesarean Section.
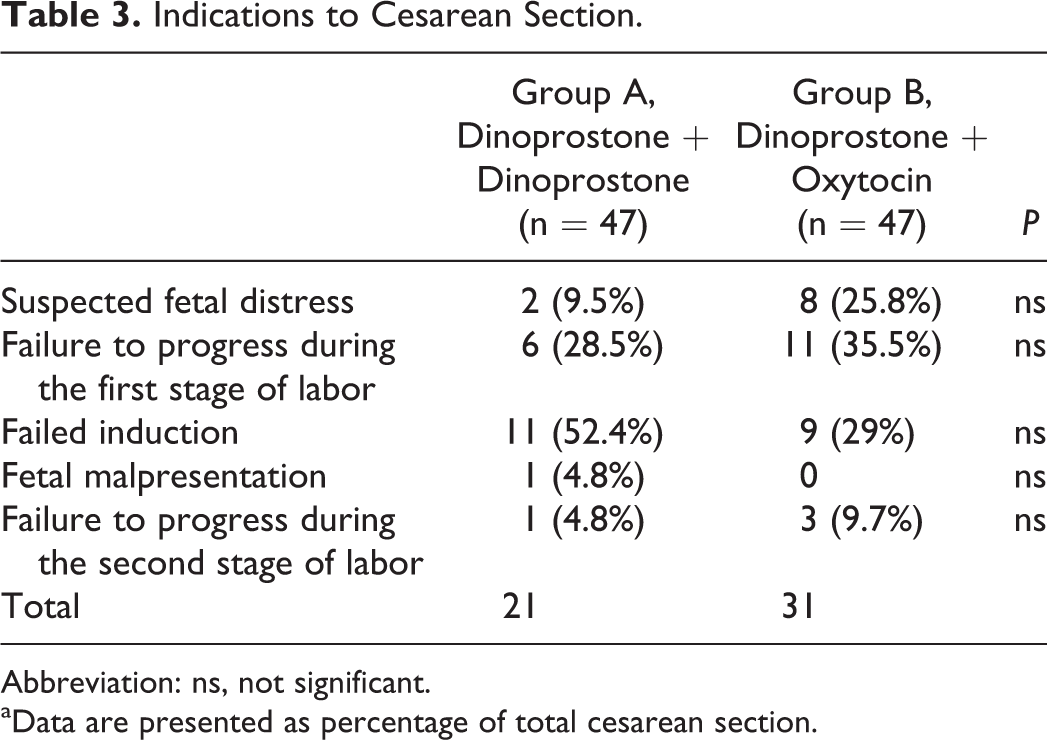
Abbreviation: ns, not significant.
aData are presented as percentage of total cesarean section.
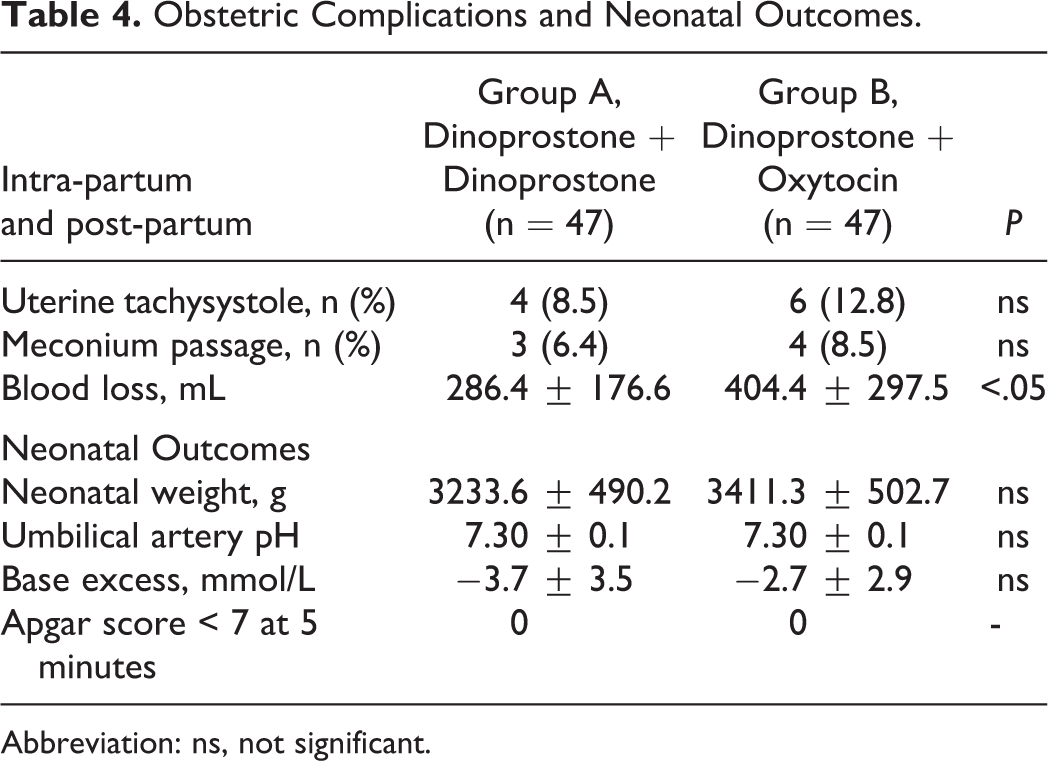
The two groups were similar in terms of presence of uterine tachysystole and meconium passage (Table 4). Mean blood loss was significantly higher in patients treated with oxytocin compared to women who received a second dose of dinoprostone (group A: 286.4 ± 176.6 mL vs group B: 404.4 ± 297.5 mL; P < .05).
Obstetric Complications and Neonatal Outcomes.
Abbreviation: ns, not significant.
There were no significant differences between dinoprostone and oxytocin groups for neonatal weight, umbilical artery pH, umbilical artery base excess, and 5-minute Apgar scores <7 (Table 4).
Discussion
In this randomized controlled trial, we compared 2 different regimes of treatment in patients with an unfavorable cervix not responsive to a first dose of dinoprostone.
We found that a double dose of dinoprostone in patients with a Bishop score ≤6 is associated to a lower rate of cesarean section compared to women treated with oxytocin. However, the intervals between labor induction and onset of labor and between labor induction and delivery were lower in the group treated with oxytocin.
Successful labor induction varies widely depending upon several factors, including characteristics of the population being induced such as parity, age, BMI, race, gestational age, neonatal weight, and management of the induction. 8
At term, cervical status is an important factor for predicting the likelihood of successful induction of labor. The Bishop score is the best available tool for assessing cervical status and predicting the likelihood that induction will result in vaginal delivery. If the Bishop score is >8, the likelihood of vaginal delivery is similar whether labor is spontaneous or induced. In contrast, a Bishop score <6 defines an unfavorable cervix and predicts an high rate of failed inductions. 5,9,10
The relationship between a low Bishop score and failed induction, prolonged labor, and a high cesarean birth rate was first described prior to widespread use of cervical ripening agents 2 but has persisted even after the introduction of these agents. 3
Administration of prostaglandins causes dissolution of collagen bundles and an increase in the submucosal water content of the cervix. These modifications lead to cervical changes associated with greater success when labor is then induced with oxytocin. 11 In addition, prostaglandins also cause the uterus to contract and may initiate labor. In this context, a 2014 Cochrane review states that prostaglandins are effective for labor induction and increase the chance of vaginal delivery in 24 hours. 4
Dinoprostone vaginal insert is associated with an average cesarean section rate of 25% (range 10.5%-38.6%) 12 –23 and a rate of vaginal delivery within 24 hours of 59.4% (range 38.2%-81.1%). 13 –20,22,23 Recently, Facchinetti et al 24 proposed that in nulliparous women with an unprepared cervix and intact membranes, the vaginal insert shows a protective effect toward cesarean section.
In our population, considering the effect of dinoprostone administration in eligible patients, 232 patients delivered or were in labor within 24 hours and were excluded from the study. In this group, 20.7% has undergone cesarean section, similarly to reported rates of previous studies.
Studies about prostaglandins administration in patients with low Bishop scores report cesarean section rates and delivery within 24 hours and do not evaluate outcomes in relation to the continuation of labor induction. 12 Our study considers and compares 2 different treatments for patients not responsive to a first dose of dinoprostone. The results suggest that a double dose of dinoprostone is associated with a higher vaginal delivery rate compared to oxytocin regimes. The two populations were similar in terms of gestational age, parity, BMI, and Bishop score at enrollment. On the contrary, the Bishop score at randomization, although unfavorable, was higher in patients randomized to oxytocin. We think that this difference further supports our results, since the Bishop score directly correlates with delivery rates.
To our knowledge, this is the first randomized trial in which 2 different regimes were compared after a failed cervical ripening using dinoprostone vaginal insert. In an observational study, Barbitch et al 25 evidenced that in more than half of cases, the cervical ripening by 2 dinoprostone vaginal inserts is associated to a high vaginal delivery rate. We can speculate that in this setting of low responders, a double dose of prostaglandins together with a gain of one more day could contribute to a better cervical ripening, favoring vaginal delivery.
Uterine tachysystole was observed in 4 (8.5%) patients treated with a double dose of dinoprostone and in 6 (12.8%) women treated with dinoprostone and oxytocin. In all cases, no fetal heart rate alterations were observed, suggesting that both regimes are relatively safe in terms of hyperstimulation. The various PGE2 preparations have up to a 5% rate of uterine tachysystole, which is usually well tolerated and not associated with an adverse outcome. In a meta-analysis comparing the dinoprostone vaginal insert to other prostaglandins, Sanchez-Ramos et al 26 reported that an increased incidence of uterine hyperstimulation is a disadvantage of the vaginal insert. The reported risk of tachysystole with oxytocin varies widely. 27 Concurrent administration of oxytocin and a prostaglandin is believed to increase the risk of tachysystole since both drugs carry a risk of this complication. Additionally, data from human and animal studies show that prostaglandin administration increases uterine sensitivity to oxytocin. Although some studies have not observed a statistically significant increase in excessive uterine activity with their concurrent use, this is likely due to the small number of patients in these studies, differences in methodology (eg, uterine activity was not continuously monitored), and the relatively low frequency of this adverse event. 28 –30 In one such trial, the frequency of uterine tachysystole with concurrent dinoprostone and oxytocin administration was 14% versus 5% with oxytocin alone (P = .20). 28 The incidence of meconium passage and mean blood loss were similar in the two groups, further confirming the safety of both treatments.
In conclusion, our data suggest that a double dose of dinoprostone could represent a safe therapeutic option in term patients with a low Bishop score not responsive to a first dose of dinoprostone vaginal insert.
Further trials are needed to assess whether this choice may be particularly useful in specific subgroups at increased risk of induction failure.
Footnotes
Authors’ Note
Society of Gynecological Investigation (SGI) 61st Annual Scientific Meeting on Florence, Italy, June 26-29 March, 2014 and XXIV European Congress of Perinatal Medicine on Florence, Italy, June 4-7, 2014.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.