
Abstract
The objective of this study was to assess effectiveness and safety of Depo-Provera (medroxyprogesterone acetate) in treatment of endometrial hyperplasia (EH) and to compare it with norethisterone acetate (NETA) as an oral progestogen treatment. One hundred forty six women aged 35 to 50 years with abnormal uterine bleeding and diagnosed as having EH were randomized to receive either Depo-Provera, one injection every 3 months for 6 months (2 doses), or oral cyclic NETA, 15 mg daily for 14 days per cycle for 6 months. Primary outcome measure was regression of EH. Secondary outcome variables were side effects of treatment, persistence/progression of EH during follow-up period. After 6 months of treatment, Depo-Provera was more successful in achieving regression of nonatypical EH than NETA (67 [91.8%] of 73 women vs 49 [67.1%] of 73, respectively), and the difference between the 2 groups was statistically significant (relative risk: 1.37; 95% confidence interval: 1.15-1.63, P = .048*). Adverse effects were relatively common with moderate differences between the 2 groups. This is the first randomized study comparing Depo-Provera with an oral progestogen as a treatment for EH. Depo-Provera is an effective and safe treatment for EH without atypia.
Introduction
Endometrial hyperplasia (EH) is defined as abnormal, noninvasive proliferation of the endometrial glands. Similar to endometrial carcinoma (ECa), EH is estrogen dependent. 1 Based on architectural complexity and nuclear cytology, EH is classified into simple or complex, without or with cytological atypia. 2 Endometrial hyperplasia presents commonly with abnormal uterine bleeding (AUB). 3,4 However, its clinical importance largely relates to the risk of progression to ECa. 5 Management of EH is a subject of considerable debate. 3,6 Hysterectomy has been preferred as treatment for EH with atypia because of fear of progression to ECa and/or concern that unsampled carcinoma may have been coexisting. 3,6 –8 The risk of coexisting carcinoma has been reported in 17% to 43% of women diagnosed as having EH with atypia. 9 –11 There is still argument regarding the merits of hysterectomy against progestogen treatment for women with complex and atypical EH. 1,12 However, treatment with oral progestogens (norethisterone acetate [NETA], medroxyprogesterone acetate [MPA], megestrol [MGA] … etc) has been established as an alternative for patients where surgery is not possible or not desired. 2,3,7,8,12 Regression of EH following use of progestogens has been described several decades ago and, since then, further studies indicated that even ECa may respond to progestogen treatment. 2 Nevertheless, there are limited data regarding long-term outcomes for women with EH treated with progestogens, with claims that efficacy of progestogen therapy is often limited. 3,6,8 Several studies report a wide range of risks for recurrence, after initial regression, persistence, or progression of EH in women treated with progestogens following cessation of therapy. These risks varied between 0% and 60% for complex EH and between 10% and 100% for EH with atypia. 1,2,13,14 As no universally agreed guidelines exist, wide variation in type of progestogen, dose, and length of treatment course has been noted, with lack of reference to women’s characteristics that predict successful progestogen treatment. 15 This makes it difficult to compare results of different studies and to provide a basis for agreement. 2,10,14,16 Marsden and Hacker, in a review of the management of EH, concluded that the optimal dosage of progestogens has not been investigated, and the regimens advocated are essentially arbitrary. 6 Injectable Depo-Provera (MPA) has been proved as an effective and safe long-acting reversible contraceptive for decades. Its greater effectiveness, reduced adverse effects, and relatively reduced cost when compared with other hormonal and nonhormonal contraceptives have been established. 17 It is therefore reasonable to postulate that Depo-Provera, as a long-acting progestogen, would be similarly useful as a treatment for EH and perhaps more acceptable to some women given its relatively reduced adverse effects. Despite that the commonest reason for people not choosing this method of contraception is needle phobia; being given by injection may be an advantage as it takes compliance off women who fear forgetting taking their tablets. Also, this route of administration suits women with impaired mental capacity and patients with other forms of disabilities and special needs. 18 Depo-Provera upregulates progesterone receptors in the endometrium causing decidualization of the hyperplastic endometrium which promotes shedding and loss of thickness. The drug is, therefore, effective in reversing EH. 18,19 The number of studies which have been conducted assessing efficacy and safety of Depo-Provera in treatment of EH is not accurately known but is believed to be very little (K. Razvi, G. Lusley, I. Etherington, personal communications, August 31 – September 2 2015). Data on use of Depo-Provera in treatment of EH are, therefore, insufficient to provide good evidence and do not meet the necessary requirements to suggest innovative recommendations for treatment. Knowledge of these variables is of paramount importance for the objective of guiding gynecologists and other health care givers in management of women with EH and also for patient education purposes. The scope for further research is, therefore, obvious. The objective of this study was to assess effectiveness and safety of Depo-Provera in treatment of EH and to compare it with NETA as an oral progestogen treatment.
Participants and Methods
Study Design
This prospective randomized trial was carried out at Zagazig University Hospital (ZUH), Zagazig, Egypt, over the period from February 2013 to January 2015. Potential candidates for the study have been attending the gynecological out-patient clinic at ZUH in view of AUB. They were investigated and treated as per the hospital protocol. Women with histologically confirmed nonatypical EH (simple or complex) were approached for recruitment. The study protocol was approved by the local research and ethics committee of ZUH. Eligible women were counseled, and a clear explanation of the interventions was given. A written informed consent was then obtained prior to start of trial from those who agreed to participate.
Sample Size
On the assumption that, in women with simple EH without atypia, the rate of regression after 6 months treatment with oral progestogens was 50% to 80%, 13,20,21 the authors considered that an improvement of 20% in the rate of regression after treatment with Depo-Provera would be clinically important. Accordingly, a power analysis indicated that a total of 144 participants (72 in each group) would have to be recruited to achieve a study power of 80% with 5% error and 95% confidence interval (95% CI) in order to prove the hypothesis is correct. However, allowing for potential exclusions for various reasons, the aim was to recruit a total of 158 women.
Inclusion Criteria
Pre-menopausal and perimenopausal women aged 35 to 50 years with an ongoing menstrual cycle for at least 6 months before the onset of AUB, with histologically confirmed nonatypical EH (simple or complex) according to the World Health Organization (WHO) 94 classification, 14,22 who have a negative cervical (Papanicolaou’s) smear within 3 years, nonpregnant, and would like to preserve the uterus (avoid hysterectomy) were eligible.
Exclusion Criteria
Women who were pregnant, < 35 or > 50 years of age; postmenopausal (amenorrhea for at least 12 months after the last menstrual period), with histologically confirmed EH (simple or complex) with atypia, distorted, and/or enlarged (>12 cm) uterine cavity; other uterine pathology, for example, submucosal fibroids, adnexal mass, previous endometrial ablation, hypersensitivity to progestogens, active genital tract infection; history of breast or genital tract cancer; liver disease; thromboembolic disease; epilepsy; migraine; asthma or cardiac or renal dysfunction; diabetes; hypertension; those declining hormonal treatment; women on any medication which might affect the menstrual blood loss within the previous 6 months, for example, steroid hormones or anticoagulants; and women at risk of osteoporosis were ineligible.
Interventions
Women were subjected to thorough history taking and clinical examination. A blood sample was taken to check for hemoglobin concentration. Uterine anatomy and endometrial thickness (ET) were checked by a transvaginal ultrasound (TVS).
Histopathology
A biopsy (endometrial Pipelle sample) was then taken and immediately soaked in a separate 10 mL glass with 10% formaldehyde. To preserve the participants’ confidentiality, samples/biopsies were given unique identification codes specific for every individual participant. Biopsies were sent to the histopathological unit at the Department of Pathology, Zagazig University Faculty of Medicine (ZUFM), where they were processed, and hematoxylin-eosin stained sections were examined under a light microscope. They were, then, interpreted according to the WHO-94 classification. 14,22 The histopathologist was blinded to the clinical findings and to which treatment group the woman belonged. For quality control purposes, histopathological slides were then reviewed by a panel of senior staff members of the unit.
Management Allocation (Randomization)
This was carried out by an independent biostatistician not involved in the study who created a computer-generated randomization sequence using serially numbered, opaque, sealed envelopes. After recruitment, the randomization envelope was opened by a member of the nursing staff not involved in the study. Neither researchers nor participants knew, prior to start of trial, to which group a particular woman was allocated. Participants were divided into 2 groups according to the treatment intervention. They were randomized in a proportion of 1:1 as follows: Depo-Provera group (73 participants): MPA (Depo-Provera 150 mg/1 mL vial, Pfizer Manufacturing Belgium NV/SA, Puurs, Belgium) was administered as deep intramuscular injection in the gluteal or deltoid muscle once every 3 months. Vials had to be shaken vigorously just before use to ensure that the dose being administered represents a uniform suspension and Cyclic oral progestogen group (73 participants): cyclic oral NETA (Steronate 5 mg tablet, Hi Pharma for Manufacturing Pharmaceuticals and Chemicals, 1st Industrial Zone, El-Obour City, Cairo, Egypt) was administered as 1 tablet 3 times daily for 14 days per cycle starting from day 12 up to day 25 (inclusive).
Treatment course lasted for 6 months for all participants in the 2 treatment groups. No changes to study design took place after trial has started. Participants were reviewed 3 and 6 months after start of treatment. At each visit, a TVS was carried out to assess ET, and women were interviewed with emphasis on the menstrual history (disappearance, persistence, or worsening of AUB), compliance to scheduled treatment, and also about side effects of treatment—if any. A repeat Pipelle endometrial sample/biopsy was taken only at the sixth month visit. At the end of trial, women were asked to report whether they were satisfied with their scheduled treatment.
Women with histologically confirmed atypical EH (simple and complex) were excluded from the outset. They have undergone hysterectomy as primary treatment and were followed up as per hospital protocol. However, this part of management was beyond the scope of this study.
Outcome Measures
The primary outcome measure was regression of EH. Regular proliferative endometrium or exaggerated progestogen effect with atrophic glands and pseudodecidualized stroma was considered as a treatment effect. Secondary outcome variables included reported side effects of treatment (persisting or worsening AUB, nausea, weight gain … etc), and persistence/progression of EH during follow-up period.
Statistical Methods
Statistical Package for Social Sciences version 20.0 (SPSS, Statistics for Windows, IBM Corp, Armonk, New York) was used for all statistical analyses. For assessment of the primary outcome, the histological findings of the endometrial specimens were analyzed according to the principle of intention to treat (excluding participants withdrawn or lost to follow-up). Main hypotheses were answered by comparing the number of women with regressed hyperplasia in each of the 2 treatment groups at the end of treatment using simple univariate statistics. Quantitative variables were compared between the 2 groups using the Student t test and presented as means and standard deviations [± SD]. Qualitative variables were compared between the 2 groups using the chi-square test or Fisher exact test. Proportion, relative risk (RR), and 95% CI were used when appropriate. P
Results
A total of 146 women with EH without atypia completed the 6 months treatment between February 2013 and January 2015 and were included in final analysis. Figure 1 represents the flow chart of recruitment. Demographic and baseline characteristics of all participants are shown in Table 1. The 2 study groups were similar in all characteristics that were recorded. Responses after 6 months treatment are shown in Table 2, while Table 3 shows side effects of treatment in all participants. The majority of women suffered some adverse effects during treatment, with only 18 participants reporting no adverse effects at all: 8 in the Depo-Provera group, and 10 in the cyclic oral group. However, the overall satisfaction with treatment was high with no statistically significant difference between the 2 groups (P > .05).
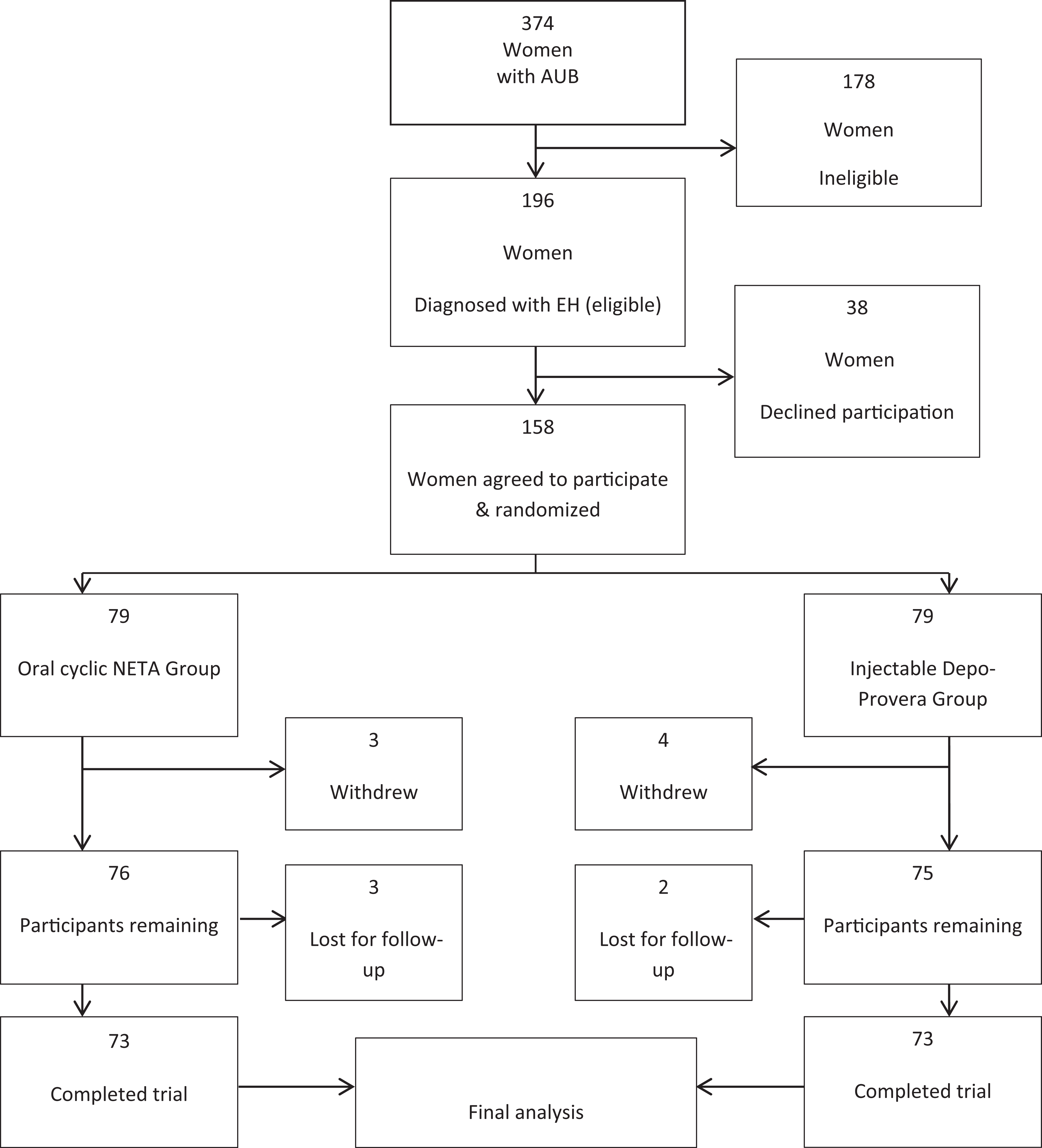
Flow chart of recruitment.
Demographic Data of All Participants.a
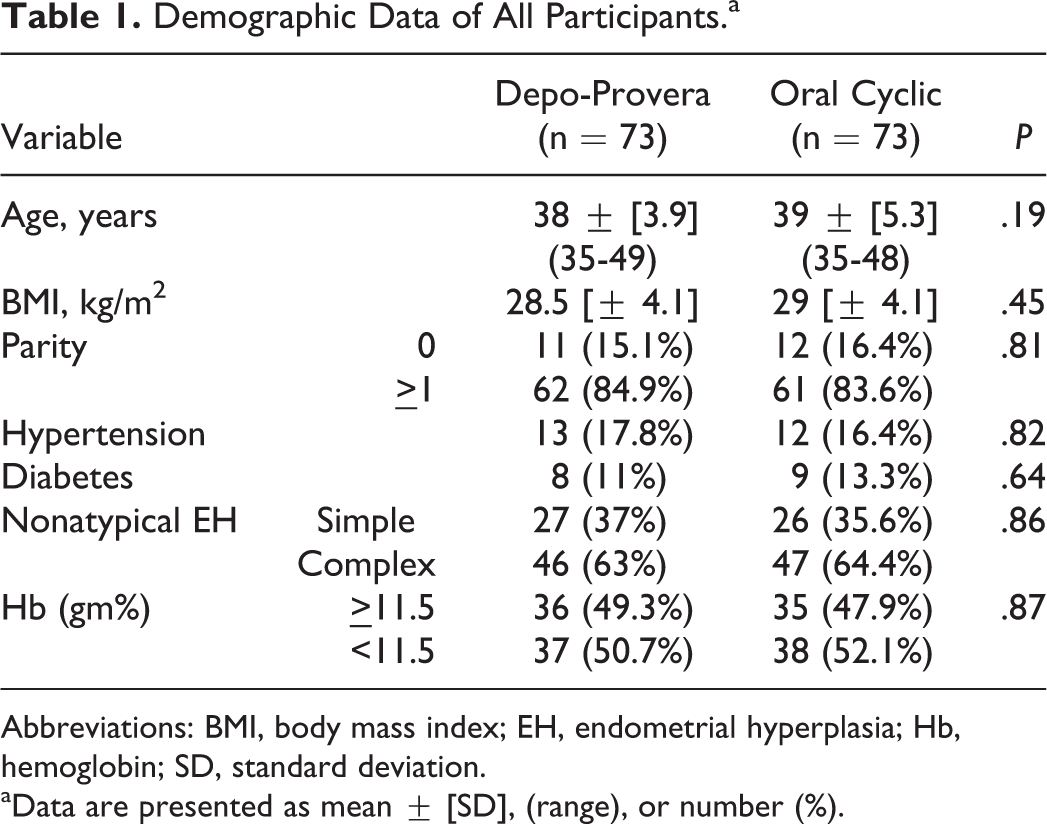
Abbreviations: BMI, body mass index; EH, endometrial hyperplasia; Hb, hemoglobin; SD, standard deviation.
aData are presented as mean ± [SD], (range), or number (%).
Treatment Responses After 6 Months in All Participants.a
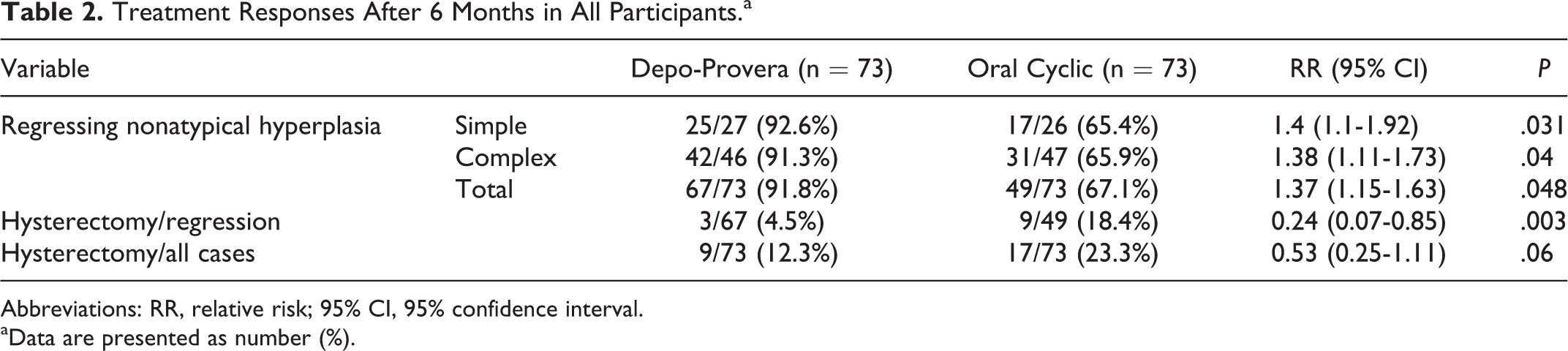
Abbreviations: RR, relative risk; 95% CI, 95% confidence interval.
aData are presented as number (%).
Side Effects in All Participants.a
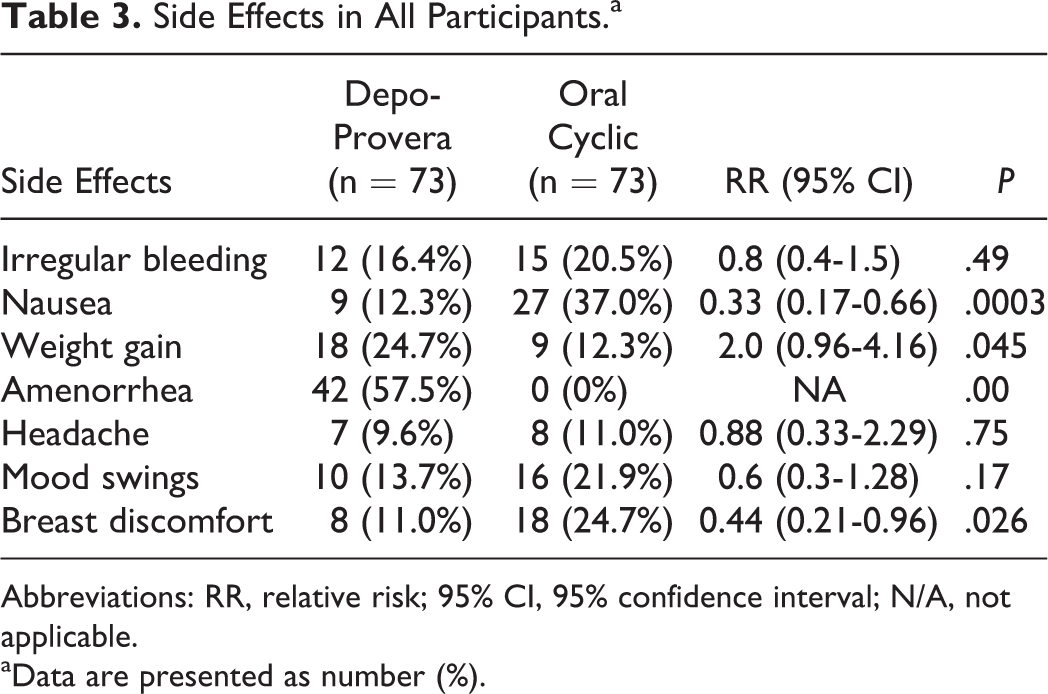
Abbreviations: RR, relative risk; 95% CI, 95% confidence interval; N/A, not applicable.
aData are presented as number (%).
Discussion
Endometrial carcinoma is the most common gynecological malignancy in many parts of the world, especially industrialized countries, and the incidence is on the rise. 14 Because EH represents precursor lesions of endometrial cancer, it seems likely that adequate treatment of its early stages would contribute to reducing the rapid increase in ECa. 15 Very little is known about the incidence of EH. However, an incidence ranging between 56/100 000 woman-years for EH with atypia and 213/100 000 woman-years for complex EH, with an intermediate incidence of 142/100 000 woman-years for simple EH, has been reported with peak incidence in the early 50s and 60s. 2,8 In this study, efficacy of Depo-Provera in treatment of simple and complex EH without atypia in premenopausal and perimenopausal women was evaluated by comparing it with oral NETA. This group of women was chosen as they represent the greatest number of AUB sufferers who require further investigation and management. As far as the authors are aware, this is the first randomized study comparing Depo-Provera with an oral progestogen as a treatment for EH. The use of NETA as a progestogen in this study was because the most commonly used progestogens (MPA and MGA) are not available in Egypt. 13 Bese et al showed that 3 months of cyclic NETA (15 mg/d for 10 days each cycle) treatment reduced both proliferative and apoptotic activities in endometrial tissue with simple nonatypical EH. 16 Similarly, Horn et al treated premenopausal and perimenopausal women with complex and atypical EH with NETA (5 mg/d) or MPA (10 mg/d) for 3 to 5 months, with an overall remission rate of 61.5%. 14 After 6 months of treatment in this study, the injectable Depo-Provera was more successful in achieving regression of nonatypical EH (simple and complex) than the oral cyclic NETA (67 [91.8%] of 73 women vs 49 [67.1%] of 73 women, respectively), and the difference between the 2 groups was statistically significant (RR: 1.37, 95% CI: 1.15-1.63, P = .048*). As shown, treatment with NETA used in this study reduced the treatment failure to 32.9%. Nevertheless, Vereide et al showed that nearly 50% of their participants had persisting EH after 3 months treatment with MPA 10 mg daily for 10 days per cycle. 21 Therefore, oral cyclic progestogen treatment in this study proved to be more effective when continued for 6 months compared with 3 months of treatments reported by previous investigators. Treatment time of not less 6 months to accurately assess response was also recommended by Gunderson et al, in a recent review of women receiving progestogen treatment for atypical EH. 7 However, when meta-analyses of studies were evaluated, the results were less comparable because of variation in type, dose, regimen, and duration of oral treatment. 2,10,14,16,21,23 In this study, women who showed regression of their EH but requested a hysterectomy due to persistent AUB was less in the Depo-Provera group than in the NETA group (3 [4.5%] of 67 participants vs 9 [18.4%] of 49, respectively), and the difference between the 2 groups showed a high statistical significance (RR: 0.24; 95% CI: 0.07-0.85)*; P = .003*). Most women using Depo-Provera experience disruption of menstrual bleeding patterns (eg, irregular or unpredictable bleeding/spotting, rarely, heavy, or continuous bleeding), following the administration of either a single or multiple doses of the drug. As women continue using Depo-Provera, fewer experience irregular bleeding and more experience amenorrhea. 24 Persistent AUB makes it difficult to rely on patient symptoms to assess response to treatment of EH. 13 In this study, the statistically significant reduced hysterectomy rate noted with the use of Depo-Provera is comparable to that achieved with the use of Levonorgestrel- Intrauterine system (LNG-IUS) and supports the view that future use of long-acting progestogen to treat nonatypical EH can reduce the number of potentially unnecessary hysterectomies. 25,26 No atypia or frank carcinoma were noted in the hysterectomy specimens in this study. This may be attributed to the accuracy of the initial diagnosis of EH and further follow-up assessments. Both were carried out using Pipelle endometrial sampling. The accuracy of Pipelle endometrial sampling as compared to endometrial biopsies obtained by cervical dilatation and curettage (D&C) in diagnosing EH has been proved. Demirkiran et al in a recent trial which investigated 673 patients noted that the outcomes of Pipelle and D&C were concordant with each other. 27 However, Pipelle biopsy is a cheaper and easier technique compared with D&C. Nevertheless, the same researchers recommended that ultrasonographic findings of endometrium should be considered prior to using whichever modality of endometrial biopsy. A great challenge in endometrial tissue studies is diagnostic reproducibility. 11,28 The lack of standardized pathology review by research pathologists in most studies may contribute to the observed variability in outcomes. 2 It has been argued that conservative management of EH should be limited to young women who want to preserve their fertility or patients with medical comorbidities for whom surgery is hazardous or not feasible. 10 Nevertheless, a recent UK survey pointed out that 52.6% of the UK gynecologists would prefer 2 conservative choices (oral progestogen or LNG-IUS) before deciding a hysterectomy for nonatypical EH. On the other hand, for atypical EH, the majority of them (83.2%) would perform a hysterectomy and would only consider LNG-IUS or oral progestogens as a second or third option in women who wish to retain fertility. 29 In view of the low (< 5%) progression rate of EH without atypia into endometrial cancer, it may be debated that, in this study, hysterectomy was not necessary for those women who have not responded to progestogen treatment in 6 months, and consideration should have been given to continued treatment for a longer period of time. 5 However, these patients opted for hysterectomy rather than continued progestogen therapy. A few limitations of this study need to be addressed. With the exception of the histopathologist who was blinded to the clinical findings of participants and also to which treatment group women belonged, the study was neither blinded nor placebo controlled. Participating women in the 2 treatment groups and their treating health care givers might have been biased. Although designing an injectable placebo was a possible alternative, on dealing with potentially premalignant disorders, treatment with placebo is unethical. Compliance to scheduled treatment was not verified. Finally, follow-up for more than 6 months was not possible due to limited resources. Nevertheless, the strengths of the study are worth mentioning. It was a prospective randomized trial with a statistically predetermined power and sample size calculations, which have been achieved. The main strength was the study design. The 2 treatment groups were equally sized and well balanced, and the investigated variables were evenly distributed among the participants. On evaluating cases of EH for eligibility criteria to be included in the study, the quality of endometrial samples/biopsies was carefully considered. Specimens with scant material, fragmentation, and those lacking preserved tissue architecture were excluded. High quality was also maintained as the histopathologists, blinded to treatment group, independently investigated all endometrial samples in the study in the same laboratory. To further maintain the high quality, histopathological slides were reviewed by a panel of senior staff members of the histopathological unit at Department of Pathology, ZUFM. In this study, the gold standard WHO classification system for EH was used as a basis for tissue selection. The study was limited to only one recruitment center (ZUH). This has the effect of avoiding differences in questioning of the participating women and reporting of adverse effects. All study outcomes were well defined and documented.
Conclusions
To the best of the authors’ knowledge, this is the first randomized study comparing injectable Depo-Provera with an oral progestogen as a treatment for EH. The injectable Depo-provera has been proved as an effective and safe treatment for EH without atypia. Given its availability, apparent safety, and relatively reduced cost, Depo-Provera deserves to be considered in further larger-sized, multi-center, double blind, randomized, placebo-controlled trials prior to recommending it for routine use in women with EH.
Footnotes
Acknowledgements
The authors would like to thank nursing staff and junior medical staff of Obstetrics and Gynecology Department at ZUH for their contribution to collection of the data of this study.
Author’s Note
This work was performed at Zagazig University Hospital, Zagazig, Egypt.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.