
Abstract
Follicle-stimulating hormone receptor (FSHR) is present on endothelial cells of blood vessels and endometrial glands of the proliferative and secretory endometrium. So far, the expression of FSHR in endometriosis has not been studied. We evaluated FSHR expression in 194 tissue specimens representing 3 relevant types of endometriosis: rectovaginal endometriotic nodules, ovarian endometriotic cysts, and peritoneal endometriotic implants. Specimens of normal endometrium were used as controls. Archival formalin-fixed and paraffin-embedded material was analyzed immunohistochemically with a highly specific monoclonal antihuman FSHR antibody using the peroxidase method. A robust vascular FSHR expression was found in all 194 patients, irrespective of the endometriosis lesion location. Follicle-stimulating hormone receptor was not detected in normal host tissues located more than 5 mm from the lesions. The endometriotic lymphatic vessels do not express FSHR. The density of FSHR-positive vessels in patients with rectovaginal endometriotic nodules was 46.0 ± 5.7 vessels/mm2. Similar values were obtained for ovarian endometriotic cysts and peritoneal endometriosis. The density of FSHR-positive vessels associated with the core of rectovaginal endometriotic nodules was 2-fold higher than that of the perilesional, adjacent normal host tissue (64.2 ± 8.2 vs 27.2 ± 3.2 vessels/mm2, respectively). Expression of FSHR was also detected either in endometriotic glandular epithelial cells, endometriotic stromal cells, or in both cell types (23%, 25%, and 21% of patients, respectively). Normal endometrium expressed FSHR predominately in basalis, in a cellular distribution dependent on hormonal environment. In conclusion, our data suggest novel FSHR expression in endometriotic lesions, qualitatively and quantitatively different from that of normal endometrium.
Introduction
Endometriosis, a common benign disease of the female genital/reproductive system, is defined as functioning endometrium outside the uterine cavity. The endometriotic lesions are found primarily in peritoneum, ovary, and rectovaginal septum. Endometriosis is found in women between the ages of 12 and 80 and affects approximately 10% of reproductive-age women. 1 The high incidence, associated symptoms (pelvic pain and menorrhagia), and side effects (infertility and diminished ovarian reserve) may present a serious clinical problem. Endometriosis is associated with an increased risk of gynecological cancers, such as specific subtypes (ie, clear-cell, low-grade serous, and endometrioid invasive) of ovarian cancers. 2,3 The growth of endometriotic implants is dependent on oestrogens. 4 The latter are mainly synthesized and secreted by the ovary following follicle-stimulating hormone (FSH) activation of aromatase that converts androgen to oestrogen. 5 Because the endometriotic lesions contain estrogen receptors 6 –8 and aromatase, 9 –11 it has been suggested that local estrogen production may stimulate the growth of lesions. 12 However, no data on the expression FSH receptor (FSHR) in endometriotic lesions are available (FSHR is a transmembrane cell surface G protein-coupled receptor. It is primarily expressed in the ovary, where it drives FSH-dependent cell differentiation in healthy women 13 ). Therefore, in the present study, we analyzed the expression of FSHR in 194 samples representing 3 relevant types of endometriosis: rectovaginal endometriotic nodules, ovarian endometriotic cysts, and peritoneal implants.
Material and Methods
Tissue Specimens
We studied archival surgical specimens from 194 patients with endometriosis from the Curie Hospital, Paris, France, and the Cochin Hospital, Paris, France. Paraffin sections were obtained from the Medical University of Bialystok Clinical Hospital, Bialystok, Poland. Endometriosis tissue specimens were fixed in 10% formalin for 48 hours, washed thoroughly with phosphate-buffered saline (PBS), dehydrated in graded ethanol and xylene, and embedded in paraffin. The institutional review board and/or ethics committee at each study site approved the study protocols. Written informed consent was obtained at the time of surgery from all living donors from whom samples were obtained. Donors of normal endometrium tissues also provided written informed consent. The clinicopathological parameters for each patient were obtained from the available clinical data bank.
Antibodies
FSHR monoclonal antibody 323 was produced in ascites and purified as described previously. 14 Goat antimouse immunoglobulin (IgG; Fc specific) polyclonal antibody was purchased from Sigma-Aldrich, Saint Quentin Fallavier, France. Mouse antihuman podoplanin (clone D2-40) was from Dako A/S, Glostrup, Denmark.
Chemicals
Sodium borohydride, 3-amino-9-ethylcarbazole, sodium azide, 30% hydrogen peroxide, goat serum, and hematoxylin Gill solution no. 3 were purchased from Sigma-Aldrich, Saint-Quentin Fallavier, France. Shandon Immu-Mount medium was obtained from Thermo-Scientific, Asniere sur Seine, France.
Immunohistochemistry
Access to tissue antigen sites for antibody attachment was enhanced by incubating slides at 90°C for 40 minutes with 10 mmol/L citrate buffer, pH 6. The sections were incubated with 6% hydrogen peroxide (15 minutes) to block endogenous peroxidase activity. Sodium borohydride (10 mg/mL PBS) was used for 15 minutes to quench free aldehyde groups. Nonspecific antibody binding was blocked by incubating slides with 2% goat serum in PBS (blocking buffer) at room temperature for 2 hours. The slides were incubated with the primary monoclonal antibody (5 µg/mL FSHR323) in blocking buffer overnight at 4°C. 15 Goat antimouse IgG (Fc specific) conjugated to peroxidase (dilution 1:500) was used as a secondary antibody. The chromogen was 3-amino-9-ethylcarbazole. The sections were counterstained with Gill’s hematoxylin for 10 seconds and mounted in Shandon Immu-Mount medium. Paraffin tissue sections of normal nonpregnant cycling endometrium (n = 17 donors) were used as controls. We used paraffin tissue sections incubated with either mouse IgG of the same class as FSHR323 (IgG2a, Sigma M9144) as primary antibodies or only the secondary antibody as negative control experiments. We quantitatively determined the density of FSHR-positive blood vessels associated with the endometriotic lesions by counting the number of stained vessels on digital images of 5 “hotspots” per patient from whole images of sections that were obtained using the Philips Digital Ultra-Fast Scanner 1.6 RA and Philips Image Management System 2.2RA (Philips Electronics Netherlands BV - Philips Digital Pathology Solutions, Best, the Netherlands). Capillaries, arterioles, and venules were identified as described previously. 16 Immunohistochemical analysis of lymphatic vessels was performed on paraffin-embedded sections of endometriotic tissues with the use of the monoclonal antibody D2-40, a marker of lymphatic endothelium, according to the manufacturer’s instructions.
Statistical Analysis
Relationships between vascular FSHR expression and the clinicopathological data were examined using Pearson correlation coefficient. All numerical data are presented as means ± standard deviation (SD). Results were analyzed for statistical significance using a 2-tailed Student test with P < .05 considered significant.
Results
FSHR Protein in Normal Endometrium
FSHR protein in normal endometrium was detected primarily in the stratum basale. Notably, we found 2 distinct patterns of FSHR expression that were dependent on menstrual cycle phase. A faint microvascular endothelial FSHR staining and basolateral localization of FSHR in glandular epithelial cells (GECs) were observed in normal proliferative endometrial tissue (n = 9 donors; Figure 1A). In contrast, the pattern of FSHR expression was completely different in the endometrial secretory phase (n = 8 donors), which exhibited juxtanuclear localization in endometrial GECs (luminal aspect, arrowheads in Figure 1B). Staining of FSHR in blood microvessels was low to undetectable (Figure 1B). The densities of FSHR-positive blood vessels in tissues with eutopic endometrium were 30.2 ± 8.9 vessels/mm2 in proliferative phase and 15.5 ± 5.0 vessels/mm2 in secretory phase. Irrespective of the phase of the menstrual cycle, a faint signal for FSHR protein was detected in normal endometrial stromal cells (SCs) by immunohistochemistry.
Expression of follicle-stimulating hormone receptor (FSHR) in eutopic endometrium. Immunohistochemical analysis was performed on paraffin-embedded sections of human breast cancer tissues with the use of FSHR323 antibody, followed by a secondary peroxidase-coupled antibody visualized with the use of the red-brown peroxidase-reaction product of 3-amino-9-ethylcarbazole. While FSHR is detectable in the basolateral region of endometrial glandular epithelial cells (GECs) of proliferative endometrium (A, arrowheads), in secretory endometrium the FSHR protein has an apical juxtanuclear localization (B, arrows). Low to undetectable FSHR signal is associated with blood vessels (BV) and endometrial stromal cells (SC). (Asterisks mark the lumen of endometrial glands). Bars: 50 µm. (The color version of this figure is available in the online version at http://rs.sagepub.com/.)
FSHR Protein in Endometriotic Lesions
Immunohistochemical studies similar to those described above were performed for 3 types of endometriotic lesions in a total of 194 patients (Table 1). In each of the lesions analyzed, without exception, we detected consistent FSHR protein expression by endothelial cells (Figure 2). In serial sections of endometriotic tissue, the blood vessels showed a strong presence of FSHR, whereas the lymphatic vessels, identified with the use of the monoclonal antibody D2-40, did not express FSHR (Figure 3).
FSHR Expression in Endometriosis and the Associated Vasculature.
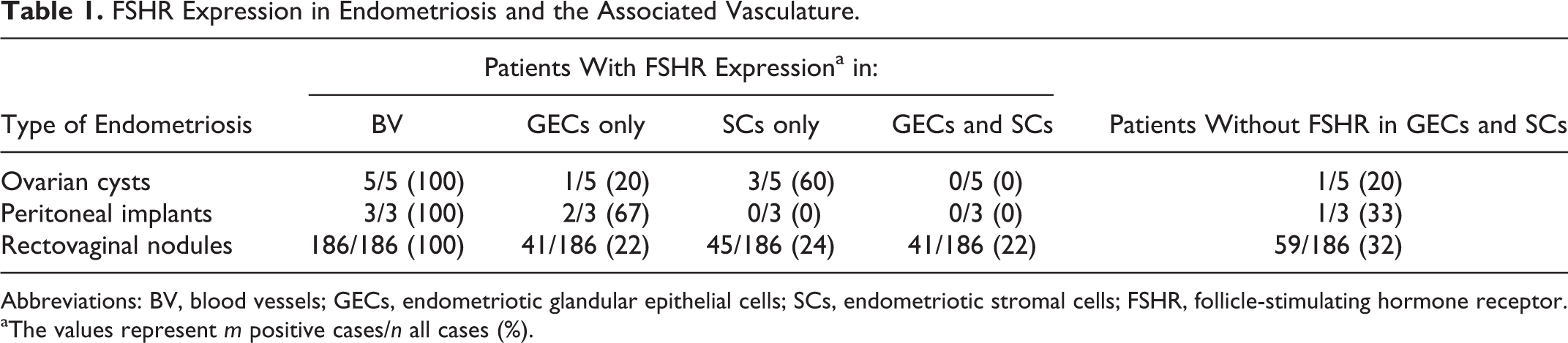
Abbreviations: BV, blood vessels; GECs, endometriotic glandular epithelial cells; SCs, endometriotic stromal cells; FSHR, follicle-stimulating hormone receptor.
aThe values represent m positive cases/n all cases (%).

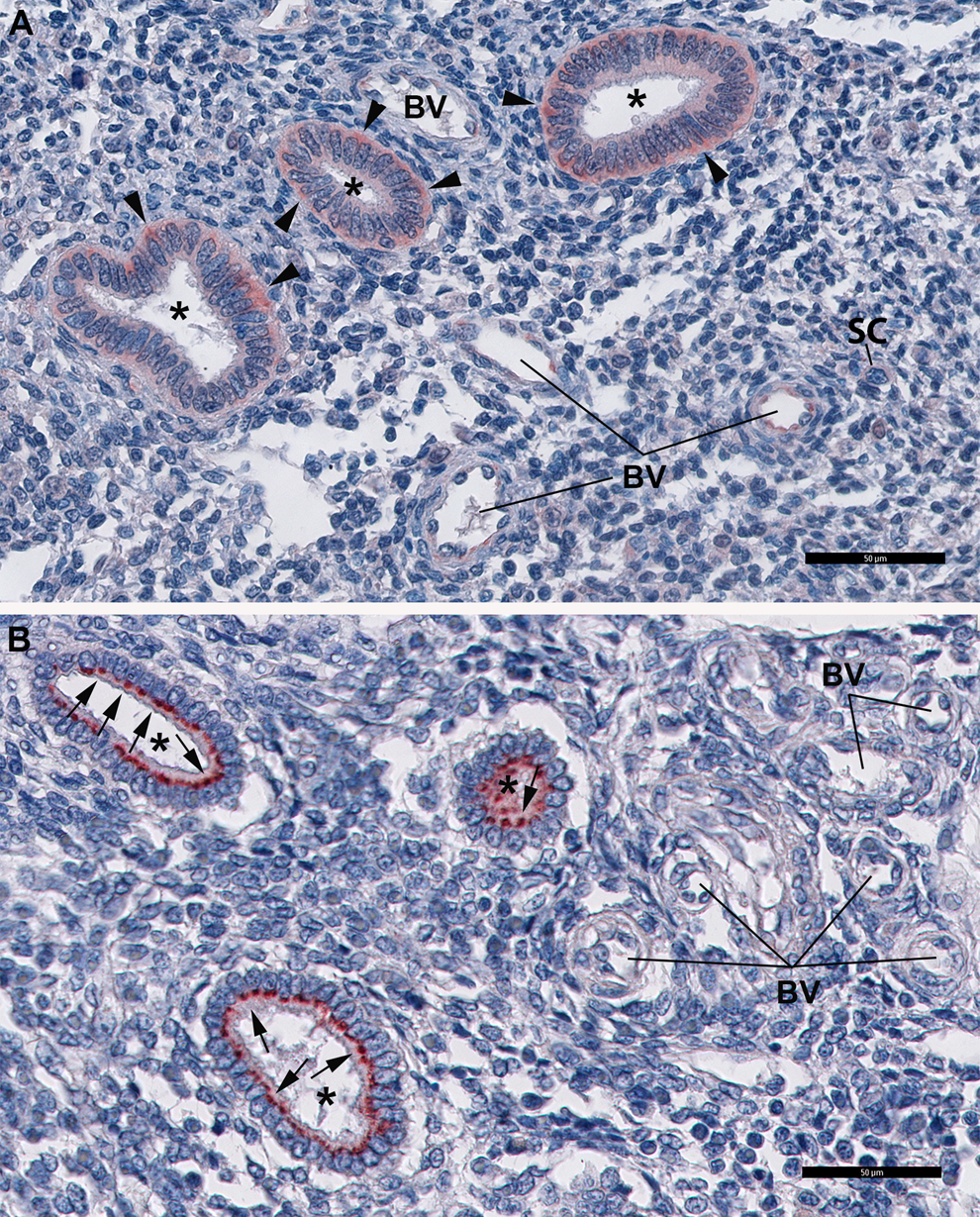
Expression of follicle-stimulating hormone receptor (FSHR) in endometriosis. The great majority of blood vessels (BV) express robustly FSHR (A, B, and C). A polarized distribution of FSHR, most frequently in the basolateral region of the cell (A, arrowheads) than on the apical domain (B, arrows) of endometriotic glandular epithelial cells (GEC) is detected. FSHR-positive-endometriotic stromal cells (SCs) are also present in endometriotic lesions (C; asterisks mark the lumen of the endometrial glands). Bars: 50 µm.
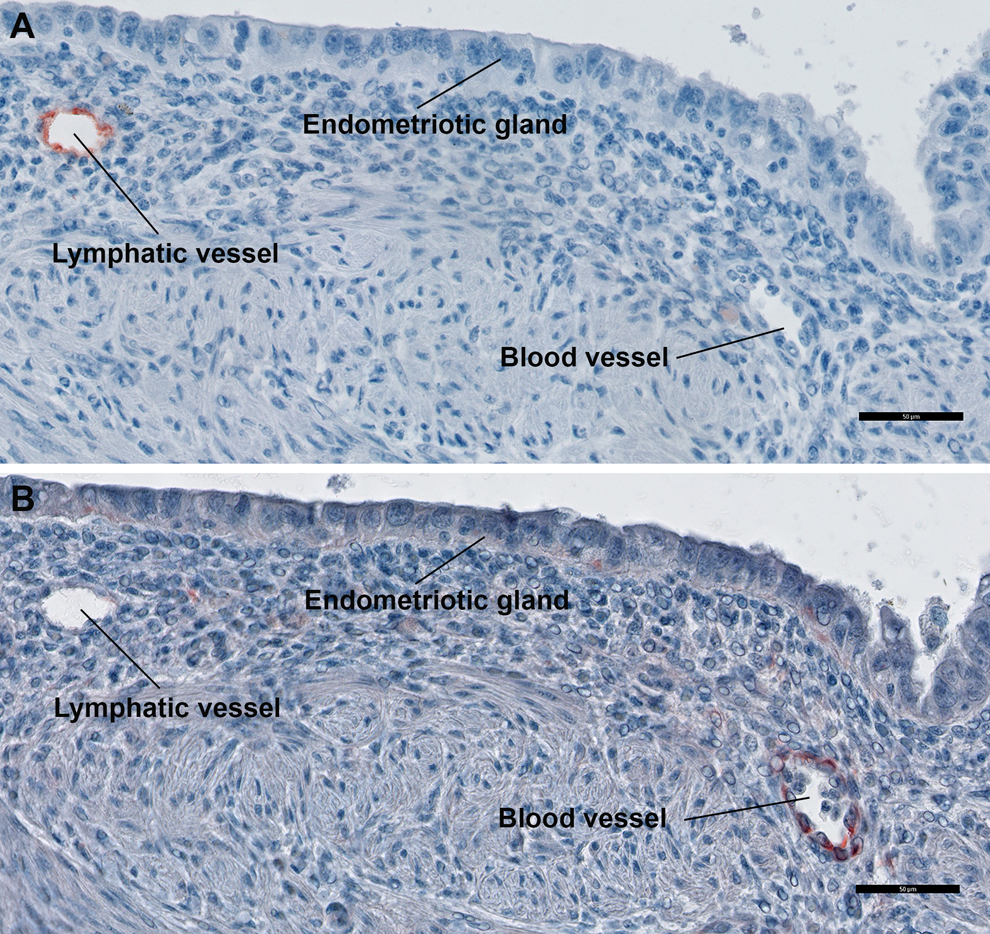
Endometriotic lymphatic vessels do not express follicle-stimulating hormone receptor (FSHR). Immunohistochemical analysis was performed on paraffin-embedded sections of endometriotic tissues with the use of the monoclonal antibody D2-40 (a marker of lymphatic endothelium; panel A) and the anti-FSH-receptor monoclonal antibody 323 (panel B), followed by a secondary peroxidase-coupled antibody visualized with the use of the red-brown peroxidase-reaction product of 3-amino-9-ethylcarbazole. Sections were also stained with hematoxylin. Bar: 50 µm. (The color version of this figure is available in the online version at http://rs.sagepub.com/.)
We quantified the endothelial FSHR-protein expression in paraffin sections from patients with rectovaginal endometriosis nodules (n = 49), ovarian endometriotic cysts (n = 5), and peritoneal endometriotic lesions (n = 3). The picture in Figure 4 is representative for the distribution of FSHR-positive blood vessels associated with endometriotic lesions we have analyzed. The density of FSHR-positive blood vessels (mean ± SD) in patients with rectovaginal endometriotic nodules was 46.0 ± 5.7 vessels/mm2. Similar values were obtained for ovarian endometriotic cysts and peritoneal endometriosis (55.2 ± 7.0 and 39.6 ± 5.8 vessels/mm2, respectively). Morphometric analysis performed on both endometriotic tissues and eutopic (normal) endometrium indicated that (i) the density of FSHR-positive blood vessels associated with the core of rectovaginal endometriotic nodules was 2-fold higher than that of the adjacent normal host tissue (64.2 ± 8.2 vs 27.2 ± 3.2 vessels/mm2, respectively) and (ii) endometriotic stromal microvessels (arterioles, capillaries, and venules) had a pattern of FSHR expression different from the eutopic (normal) endometrium (Table 2).
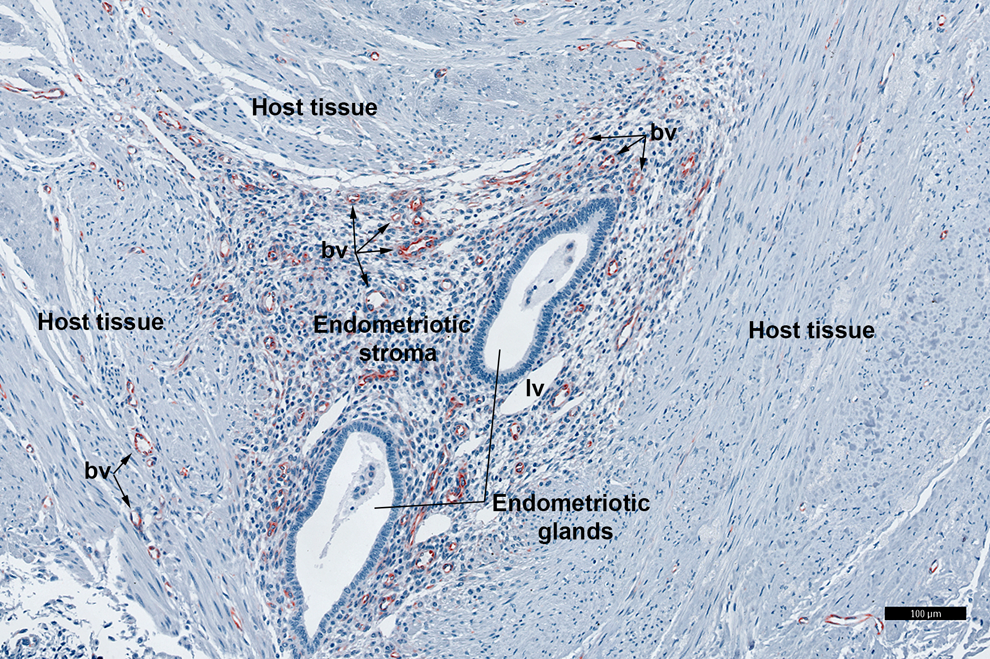
Follicle-stimulating hormone receptor (FSHR)-positive blood vessels are mainly associated with the endometriotic lesion core. Immunohistochemical analysis was performed as described in the legend of Figure 1. bv indicates blood vessels; lv, lymphatic vessels. Bar: 100 µm.
Endothelial FSHR Expression in Ectopic Versus Eutopic Endometrium.
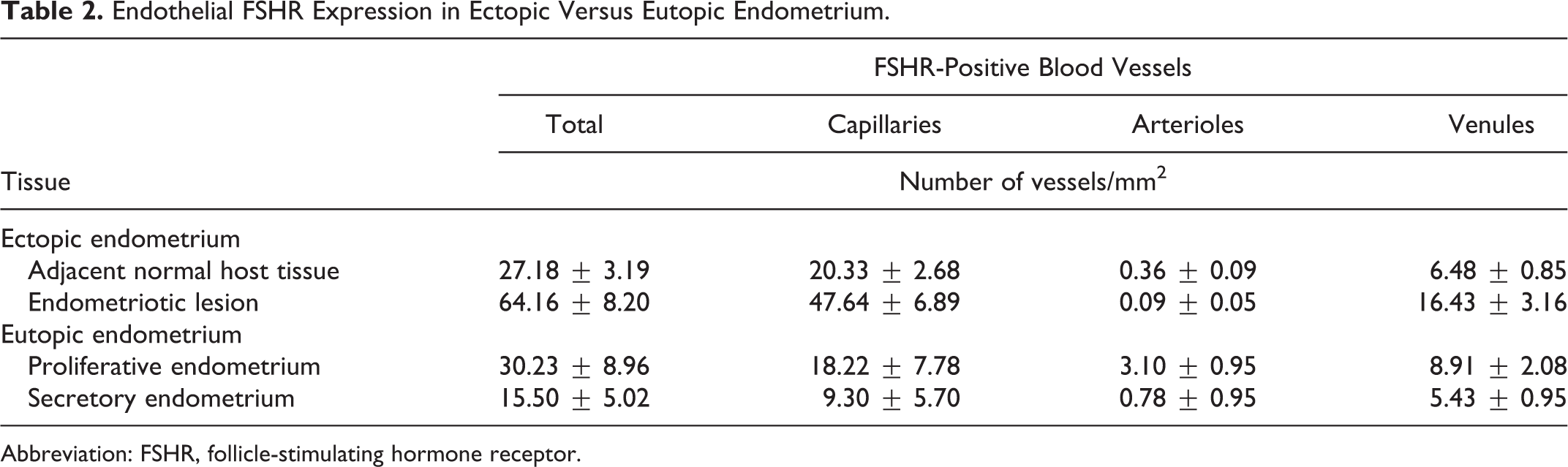
Abbreviation: FSHR, follicle-stimulating hormone receptor.
The expression of FSHR was also detected either in endometriosis GECs, SCs or in both cell types (Table 1). In patients with FSHR-positive GECs (n = 44), the receptor protein exhibited either a basolateral cellular distribution (Figure 2A; n = 30) or juxtanuclear localization (luminal aspect; n = 7) (Figure 2B). No receptor protein polarization was detected in 16% of patients (7/44) with FSHR-positive GECs. FSHR-positive SCs were detected in 24% of patients (48/194; Figure. 2C). In 32% of patients (61 of 194), GECs and SCs were FSHR negative. Follicle-stimulating hormone was not detected in surrounding healthy tissues located more than 5 mm from the lesions.
Altogether these results indicated suggested that normal endometrium and endometriosis lesions are qualitatively and quantitatively different from each other.
Correlation of FSHR Expression in Endometriosis With Clinicopathological Data
A positive correlation was found between the density of stromal FSHR-positive blood vessels and the density of peripheral FSHR-positive blood vessels (r = .9697; n = 44; P < .001). The density of FSHR-positive vessels surrounding endometriotic lesions correlated positively with the percentage of FSHR-positive glands (r = .3803; n = 49; P = .007) and the duration of infertility (r = .5944; n = 19; P = .007). The expression of FSHR in endometriosis glands correlated positively with the duration of infertility (r = .751115; n = 17; P = .0005) and with the rectovaginal nodule size (r = .4335; n = 48; P = .002). No correlations were noted between the level of FSHR expression and patient age or body mass index.
Discussion
Available evidence suggests that in healthy women, FSHR is present on endometrial SCs, endometrial glands of the proliferative and secretory endometrium, 17 –19 as well as on endothelia of its associated blood vessels. 19 However, comprehensive data on FSHR expression in endometriosis are missing. In the present study, we show that FSHR is expressed in all 194 tissue samples representing 3 endometriosis subtypes: ovarian endometriotic cysts, peritoneal endometriotic lesions, and rectovaginal endometriotic nodules. Our immunohistochemical results indicated that in the normal endometrium the FSHR localization is dependent on menstrual cycle phase (basolateral localization in proliferative phase versus juxtanuclear localization [luminal aspect] in secretory phase). This was not the case with that observed in endometriotic lesions where basolateral FSHR localization was frequently observed in the great majority (>85%) of endometriotic tissue samples. Therefore, our present results indicate the presence of proliferative endometriotic lesions in more than 85% of patients we have analyzed. These results are in agreement with a light microscopic study which showed that only 13% of endometriotic implants were synchronous with the corresponding eutopic endometria. 20 It is highly likely that FSHR signaling in GECs and/or SCs may exhibit a functional expression in proliferative endometriotic lesions, with a possible activation of aromatase that converts androgen to estrogen. The endothelial FSHR, robustly expressed in blood vessels associated with endometriotic lesions, should facilitate the transendothelial passage of pituitary FSH by a process of receptor-mediated transcytosis. 21 Further studies are needed to prove that the FSHR protein in proliferative endometriotic lesions is functional. The observation that the secretory phase effect of juxtanuclear FSHR in normal endometrium was lost in more than 85% of endometriotic lesions suggests that the normal balance achieved by sequential actions of estrogen (in proliferative phase) and progesterone (in secretory phase), essential to the normal cyclic functions of human endometrium, was disrupted. Disruption of this balance may explain the inability of endometriotic cells to respond to progesterone. The “progesterone resistance” and “estrogen dominance” are hallmarks of endometriosis and considered to play a significant role in the pathophysiology of this disease. 22 –24
Angiogenesis plays an important role in the implantation and development of endometriotic lesions. 22,23,25,26 Depriving an endometriotic lesion from its oxygen and nutrients by preventing the formation of new vessels may be a promising treatment modality in endometriosis. 24,27 Immunohistochemistry localized FSHR to ECs of blood microvessels in endometriotic tissue specimens from all 194 patients with endometriosis who were evaluated. The density of FSHR-positive capillaries and venules associated with the core of rectovaginal endometriosis nodules was 2-fold higher than that of the adjacent host tissue suggesting an important role of FSHR in the formation of new vessels that nourish these benign tissues with oxygen and nutriments. Therefore, compounds that interfere with FSHR signaling should impede the development of endometriosis. This interference may be achieved using deglycosylated FSH, 25,28 FSH neutralizing antibodies, 26,29 FSHR blocking antibodies, 14 nonsteroidal negative modulators of FSHR, 27,30 and GnRH analogues. 1,28,31,32 It should be remembered that agents that interfere with the FSHR signaling may cause detrimental effects on reproductive functions in patients with endometriosis. However, the concentration of vascular FSHR in ovary 14 and endometrium (present study) is much smaller than that corresponding to blood vessels associated with endometriotic lesions. Therefore, a therapeutic window can likely be identified, either as a concentration or schedule of repeated delivery.
Surgery for severe endometriosis is the standard treatment; however, postoperative symptomatic recurrences are frequent, and repeated surgery is performed in greater than 50% of all patients. 30,33 The results of these surgeries indicate that residual endometriotic lesions were missed in many cases. Therefore, the localization of endometriotic lesions and the determination of objective resection margins are required to improve the resection of endometriosis tissues. A salient finding of the present experiments was that the vascular FSHR expression was not dependent on the anatomic locations of endometriotic lesions (eg, ovarian endometriotic cysts, peritoneal endometriotic implants, and rectovaginal endometriotic nodules). Moreover, FSHR was robustly expressed in all endometriotic lesions but not in surrounding healthy tissues located more than 5 mm from the lesions. This observation provides support for the speculation that FSHR could be used as a biomarker in targeted intraoperative optical imaging of endometriotic lesions, especially nonovarian deep endometriotic lesions.
Conclusions
In conclusion, we found that the FSHR expression in endometriotic lesions is qualitatively and quantitatively different from that of normal endometrium.
Footnotes
Acknowledgements
We thank André Nicolas and Elise Martel for excellent technical assistance, Drs Donata Ponikwicka-Tyszko (Department of Biology and Pathology of Reproduction, IARFR, Polish Academy of Sciences, Olsztyn, Poland), Piotr Bernaczyk (Department of Pathomorphology, Medical University of Bialystok, Bialystok, Poland), Jakub Tomaszewski, and Slawomir Wolczynski (Department of Reproduction and Gynecological Endocrinology, Medical University of Bialystok, Bialystok, Poland
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Institut National de la Santé et de la Recherche Médicale, France.