
Abstract
Polycystic ovary syndrome (PCOS) is related to clinical and metabolic comorbidities that may limit the prescription of combined hormonal contraceptives, with consequent need to use progestogen-only contraceptives (POCs). Thus, the objective of the present study was to evaluate the clinical and metabolic effects of a POC, the levonorgestrel-releasing intrauterine system (LNG-IUS), in women with PCOS followed up over a period of 6 months compared to baseline and to women without PCOS. Thus, an observational, prospective, controlled study was conducted on 30 women with a diagnosis of PCOS who presented adverse effect secondary to the use of combined oral contraceptives (nausea, headache, mastalgia or vomiting; PCOS group) paired with 30 ovulatory women without PCOS (control group), both groups being free of comorbidities and having chosen the LNG-IUS as contraceptive. Clinical, laboratory, and ultrasonographic variables were evaluated immediately before LNG-IUS insertion and 6 months after the use of this method. Before LNG-IUS insertion, the PCOS group had higher total testosterone levels (P = .04), lower HDL levels (P = .04), and greater ovarian volume (P < .01) than the control group. Six months after LNG-IUS insertion, there was a 2.3% increase in abdominal circumference (P = .04) and a 3.4% increase in fasting glycemia (P = .02). On the other hand, mean ovarian volume was 10% smaller compared to the volume found before LNG-IUS insertion (P = .04), LDL levels were reduced by 5.2% (P = .03), and total cholesterol levels were reduced by 6.7% (P < .01) compared to baseline evaluation in the PCOS group. The remaining variables did not differ significantly during the 6 months of observation. The control group did not show significant changes compared to the period before LNG-IUS insertion. When the groups were compared after the 6-month follow-up, only glycemia showed a statistically significant variation between the groups, with glycemia levels increasing by 3.4% in the PCOS group and decreasing by 2.6% in the control group (P = .008). In conclusion, the use of the LNG-IUS for 6 months was not associated with relevant changes in clinical or metabolic variables of women with no comorbidities regardless of the presence of PCOS.
Keywords
Introduction
Polycystic ovary syndrome (PCOS) is a proinflammatoy 1 and atherogenic 2 disorder with a estimated prevalence of 4% to 13% among women of reproductive age. 3,4 This syndrome is the main cause of hyperandrogenism and oligo-anovulation and is normally associated with clinical and metabolic comorbidities. 5 –7
Women with PCOS may anticipate to the fourth decade of life the onset of the traditional risk factors for cardiovascular disease (CVD), 8 such as systemic arterial hypertension (SAH), obesity, dyslipidemia, metabolic syndrome, and type 2 diabetes mellitus (DM2). 5 –7 Since some of these comorbidities (dyslipidemia plus another risk factor for CVD or SAH) are considered to be category 3 (the risks of prescription exceed the potential benefits) for the prescription of combined hormonal contraceptives (CHC) according to the medical eligibility criteria for contraceptive use of the World Health Organization, 9 combined hormonal contraceptives should be prescribed with caution to women with PCOS in the presence of associated metabolic dysfunctions.
In these situations, the prescription of progestogen only contraceptives (POCs) may be safer, since they can be prescribed in almost all situations of risk for CVD. 9 However, no studies have evaluated the clinical and metabolic performance of these methods in women with PCOS. This lack of evaluation may be due to fear that POCs would not perform as well as combined contraceptives in hyperandrogenism control and may even aggravate this condition because of the androgenic effect of certain progestogens.
Thus, the objective of the present study was to evaluate the clinical and metabolic effects of a POC, the levonorgestrel-releasing intrauterine system (LNG-IUS), in women with PCOS followed up over a period of 6 months compared to baseline and to women without PCOS.
Patients and Methods
Study Design
An observational, prospective, controlled study was conducted on 30 women with a diagnosis of PCOS (PCOS group) paired for age and body mass index (BMI) with 30 women without the syndrome (control group).
Participants
Polycystic ovary syndrome was diagnosed according to the Rotterdam criteria. 3 Pairing was performed using age (± 2 years) and BMI (± 1 kg/m2). Each woman with PCOS who wished placement of the LNG-IUS was paired with a woman without PCOS who had chosen the LNG-IUS as a contraceptive. The LNG-IUS was not inserted on the same day of the invitation to participate in the study.
All included women with PCOS had menstrual irregularity and clinical and/or laboratory hyperandrogenism with or without ultrasound (US) findings. The patients were 18 to 35 years old and wanted to use the LNG-IUS as a contraceptive due to secondary adverse effects of CHC use (nausea, headache, mastalgia, or vomiting). Control women had regular cycles (24-32 ± 3 days), which is sufficient to infer ovulatory cycles in daily clinical practice for women without infertility. 10 Also, they did not have hyperandrogenism or US findings of PCOS.
Exclusion criteria for both groups were: obesity (defined as BMI ≥ 30 kg/m2); current presence or a history of venous or arterial thrombosis; any known chronic disease; smoking, alcoholism and/or drug use; use of a hormonal contraceptive (injectable, implant, or intrauterine device) during a 6-month period before the beginning of the study; use of a hormonal contraceptive method (oral, vaginal, or transdermal) during a 3-month period before the beginning of the study; puerperium of 12 weeks or less; breast-feeding or interruption of breast-feeding during a 2-month period before the beginning of the study; chronic and/or acute inflammatory processes; use of medications that might interfere with CVD markers such as antiandrogenic drugs, glucose-lowering agents, anti-inflammatory agents, or statins; and clinical category 3 or 4 for LNG-IUS use according to the World Health Organization eligibility criteria. 9
Settings
Women with PCOS were recruited at the Gynecologic Endocrinology outpatient clinic of the University Hospital, Medical School of Ribeirao Preto, University of São Paulo (HC-FMRP-USP), Brazil, between November 2012 and October 2013. This is the sector responsible for the follow-up of most women with PCOS at public health units in Ribeirão Preto. Control women were recruited at the Contraception outpatient clinic of the same hospital and at basic health units under the administration of university. The study was approved by the institutional review board, and all women gave written informed consent to participate.
The patients were submitted to clinical and laboratory assessment at 2 time points: before and 6 months after LNG-IUS insertion at HC-FMRP-USP. The patients were adviced to not begin physical activity or diet during the study. The patients were evaluated in the laboratory of Gynecology of HC-FMRP-USP on single visit during the early follicular phase (third to fifth day) of the menstrual cycle, after a 12-hour fast. Women with amenorrhea were evaluated on a random basis as long as the absence of a corpus luteum or follicle >10 mm was documented by US.
Variables and Measurements
Clinical and metabolic variables
Age, weight (W), height (H), BMI defined as W(kg)/H(m)2, systolic arterial pressure (SAP) and diastolic arterial pressure, and abdominal circumference (AC) were determined. After a 15-minute rest, 20 mL of venous blood was collected. A 10-mL aliquot of this sample was centrifuged and stored at −70°C for determination of serum levels of insulin, total testosterone, C-reactive protein (CRP), and sex hormone-binding globulin (SHBG) at a single time point. The remaining 10 mL was used for biochemical analysis (glycemia and lipid profile) at a maximum of 2 hours after blood collection.
Fasting serum insulin, CRP, and SHBG levels were determined by chemiluminescence using DPC Immulite 2000 equipment (Diagnostic Products Corporation, Los Angeles, California). Total testosterone was determined by liquid chromatography/tandem mass spectrometry (Thermo Fisher Scientific, Franklin, Massachusetts, and Applied Biosystems-MDS Sciex, Foster City, California). Fasting glucose levels were determined by the oxidation method using Wiener Lab equipment (Rosario, Argentina). The intra-assay and interassay coefficients of variation were less than 5% for all laboratory variables. Total cholesterol (TC), high-density lipoprotein (HDL), and triglycerides (TG) were measured by the immunoenzymatic method using BT3000 Plus equipment (Wiener Lab). Serum low-density lipoprotein (LDL) levels were calculated using the Friedewald formula. 11
Ultrasonographic variables of cardiovascular risk
Ultrasound evaluation was performed 5 minutes after the arterial pressure measurements using the linear 6- to 12-MHz probe (SP6-12) of Voluson 730 Expert US equipment (GE Medical Systems, Zipf, Austria) with a coupled electrocardiogram. All echographic evaluations were performed by the same examiner.
Intima–media thickness (IMT) of the common carotid artery was measured on electrocardiographic images of the left common carotid, including the bulb as previously described. 12 The IMT of the distal wall of the common carotid artery was measured 4 times on this image, approximately 10 to 20 mm proximal to the carotid bulb and averaged.
In the flow-mediated dilation (FMD) evaluation, the right brachial artery was visualized approximately 5 to 10 cm proximal to the antecubital fossa on the longitudinal plane and measured as described previously. 12 To induce vasodilation, the pneumatic cuff of a standard sphygmomanometer was positioned on the forearm immediately below the medial epicondyle and inflated up to 50 mm Hg above SAP or to 200 mm Hg, whichever was higher. After 5 minutes, the cuff was rapidly deflated, and 60 seconds later, the brachial artery diameter (BDpost) was measured as described. The FMD was calculated using the following formula: FMD = ([Bdpost − BDbasal]/Bdbasal). 13 Measurements were performed 60 seconds after cuff deflation because several studies have shown that the maximum increase in diameter occurs during this period. 14,15 After the cardiovascular echographic evaluation, we performed a pelvic US examination to evaluate the ovarian characteristics and volume.
Bias
Standardized protocols for blood collection were used for the clinical and metabolic variables; this can reduce possible bias. The technicians responsible to evaluate the metabolic variables were blind regarding the groups. These variables were determined at a single time point in order to reduce interassay error. The intra- and interassay coefficients of variation were less than 5% for all laboratory variables. Liquid chromatography/mass spectrometry analysis was performed to avoid the interference of LNG in the determination of total testosterone. A single observer who was blind to the presence or absence of PCOS using triplicate or quadruplicate measurements carried out US procedures. Samples were paired in order to prevent imbalance between the PCOS and the control groups. Finally, statistical analysis was blind to the study group.
Sample Size
Considering that the main objective of the present study was to assess metabolic effects in women with PCOS, the sample was calculated using triglyceride levels, which is one of the metabolic variables most affected by combined hormonal contraceptives. In a previous study by our group, the use of a combined oral contraceptive increased 50% in the mean (±SD) of triglyceride levels in 12 months of follow-up. 12 Thus, 30 patients with PCOS would be necessary in order to observe this 50% difference after treatment with the LNG-IUS with 80% power and 5% alpha (STATA12 software; Texas). To determine whether there was a difference in the possible effects induced by the LNG-IUS between the PCOS and the control groups, we considered that a 20% difference between groups in the 6-month variation in triglyceride levels would be relevant. For this purpose, 18 patients per group would be necessary, with 80% power and 5% alpha with the use of the same software. On this basis, in the present study, we included 30 patients with PCOS and 30 control women.
Statistical Analysis
The Kolmogorov-Smirnov and Shapiro-Wilk tests were used to determine the normal distribution of the variables. Since some variables did not show normal distribution, we opted to use the nonparametric Wilcoxon test for paired intragroup comparison. Regarding intergroup evaluation, the Mann-Whitney U test was used for baseline comparison. For the intergroup comparison of the variation in each parameter within 6 months, analysis of variance with logarithmic transformation of the variables without normal distribution (LDL, SHBG, CRP and insulin) was used. The chi-square test or the Fisher exact test was used for the qualitative variables. All analyses were carried out using SAS 9.0 software (SAS Institute Inc, North Carolina University, North Carolina), with the level of significance set at 5%. The variation in each parameter (value at 6 months – baseline value) was determined for intergroup comparison. No sample loss occurred; therefore, no strategy was required for missing data imputation.
Results
A total of 146 patients with a diagnosis of PCOS without comorbidities were evaluated at the outpatient clinic of our institution between 2012 and 2013. Of these, 102 were not eligible for the present study because they were well adapted to the use of combined contraceptives. Thus, 44 women with PCOS met the inclusion criteria. However, 14 of these patients were excluded because 9 were obese, 3 wished to become pregnant, and 2 were smokers. The flowchart of the study is shown in Figure 1. The eligible women were paired with 30 control women who wished to use the LNG-IUS and who fulfilled the pairing and eligibility criteria.
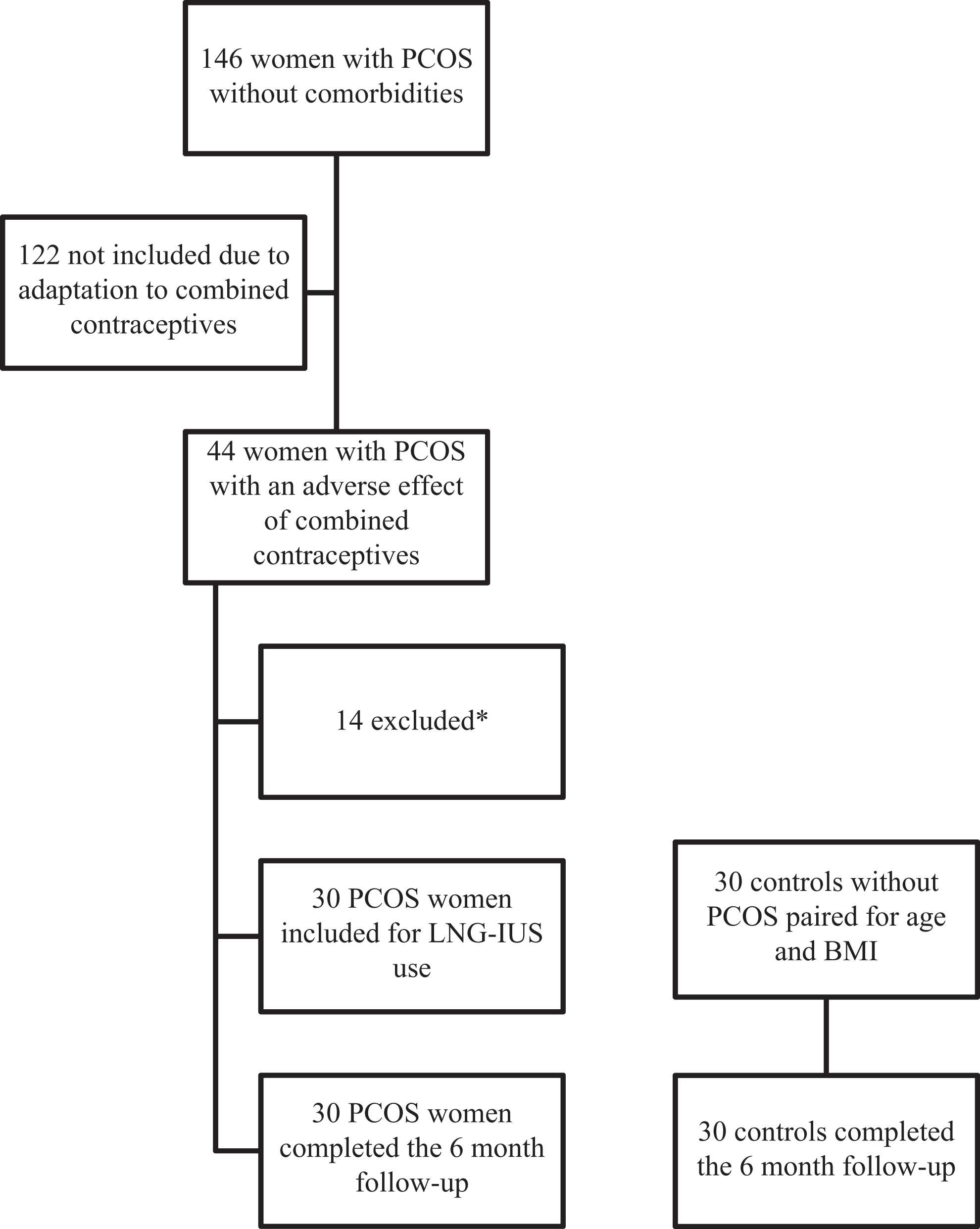
Flowchart of the study.
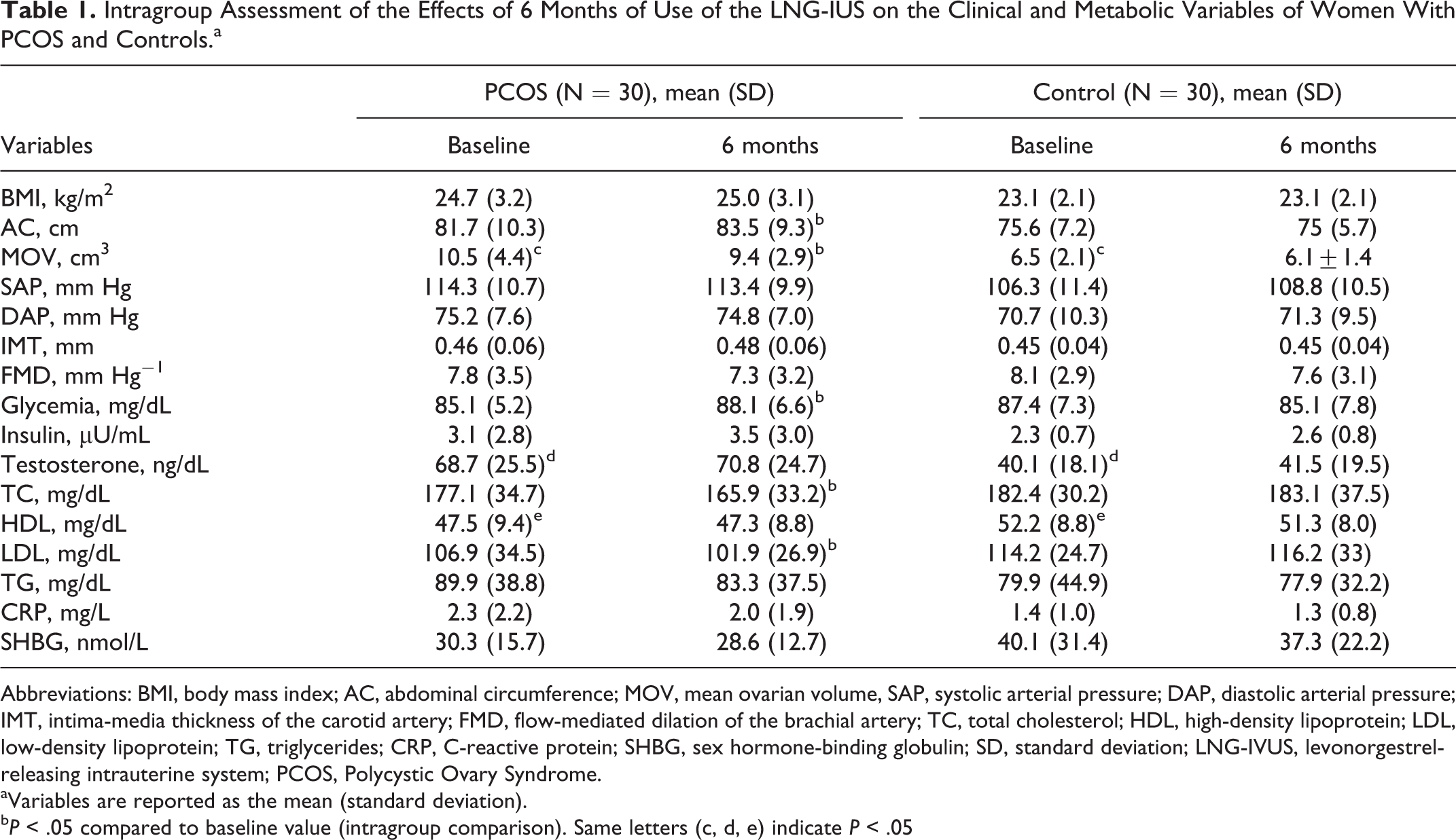
Mean age did not differ between the PCOS and the control groups (PCOS: 27.2 ± 4.1 years vs. Control: 28.1 ± 3.6 years, P = 0.35). Before LNG-IUS insertion, women with PCOS had higher levels of total testosterone (PCOS: 68.7 ± 25.5 ng/dL vs control: 40.1 ± 18.1 ng/dL, P = .04), lower HDL levels (PCOS: 47.5 ± 9.4 mg/dL vs control: 52.2±8.8 mg/dL, P = .04), and greater ovarian volume (PCOS: 10.5 ± 4.4 cm3 vs control: 6.5 ± 2.1 cm3, P < .01) than controls (Table 1).
Intragroup Assessment of the Effects of 6 Months of Use of the LNG-IUS on the Clinical and Metabolic Variables of Women With PCOS and Controls.a
Abbreviations: BMI, body mass index; AC, abdominal circumference; MOV, mean ovarian volume, SAP, systolic arterial pressure; DAP, diastolic arterial pressure; IMT, intima-media thickness of the carotid artery; FMD, flow-mediated dilation of the brachial artery; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides; CRP, C-reactive protein; SHBG, sex hormone-binding globulin; SD, standard deviation; LNG-IVUS, levonorgestrel-releasing intrauterine system; PCOS, Polycystic Ovary Syndrome.
aVariables are reported as the mean (standard deviation).
bP < .05 compared to baseline value (intragroup comparison). Same letters (c, d, e) indicate P < .05
Six months after LNG-IUS insertion, the PCOS group showed a 2.3% increase in AC (basal: 81.7 ± 10.3 cm vs 6 months: 83.5 ± 9.3 cm, P = .04) and a 3.4% increase in fasting glycemia (basal: 85.1 ± 5.2 mg/dL vs 6 months: 88.1 ± 6.6 mg/dL, P = .02). On the other hand, their mean ovarian volume was 10% smaller compared to before LNG-IUS insertion (basal: 10.6 ± 4.4 cm3 vs 6 months: 9.5 ± 2.9 cm3, P = .04), their LDL levels were reduced by 5.2% (basal: 107 ± 34.6 mg/dL vs 6 months: 102 ± 27 mg/dL, P = .03), and their TC levels were reduced by 6.7% (basal: 177.1 ± 34.8 mg/dL vs 6 months: 165.9 ± 33.4 mg/dL, P < .01; Table 1). The remaining clinical and laboratory variables did not differ significantly during the 6 months of observation (Table 1). The control group did not show any statistically significant change during the 6-month period of evaluation.
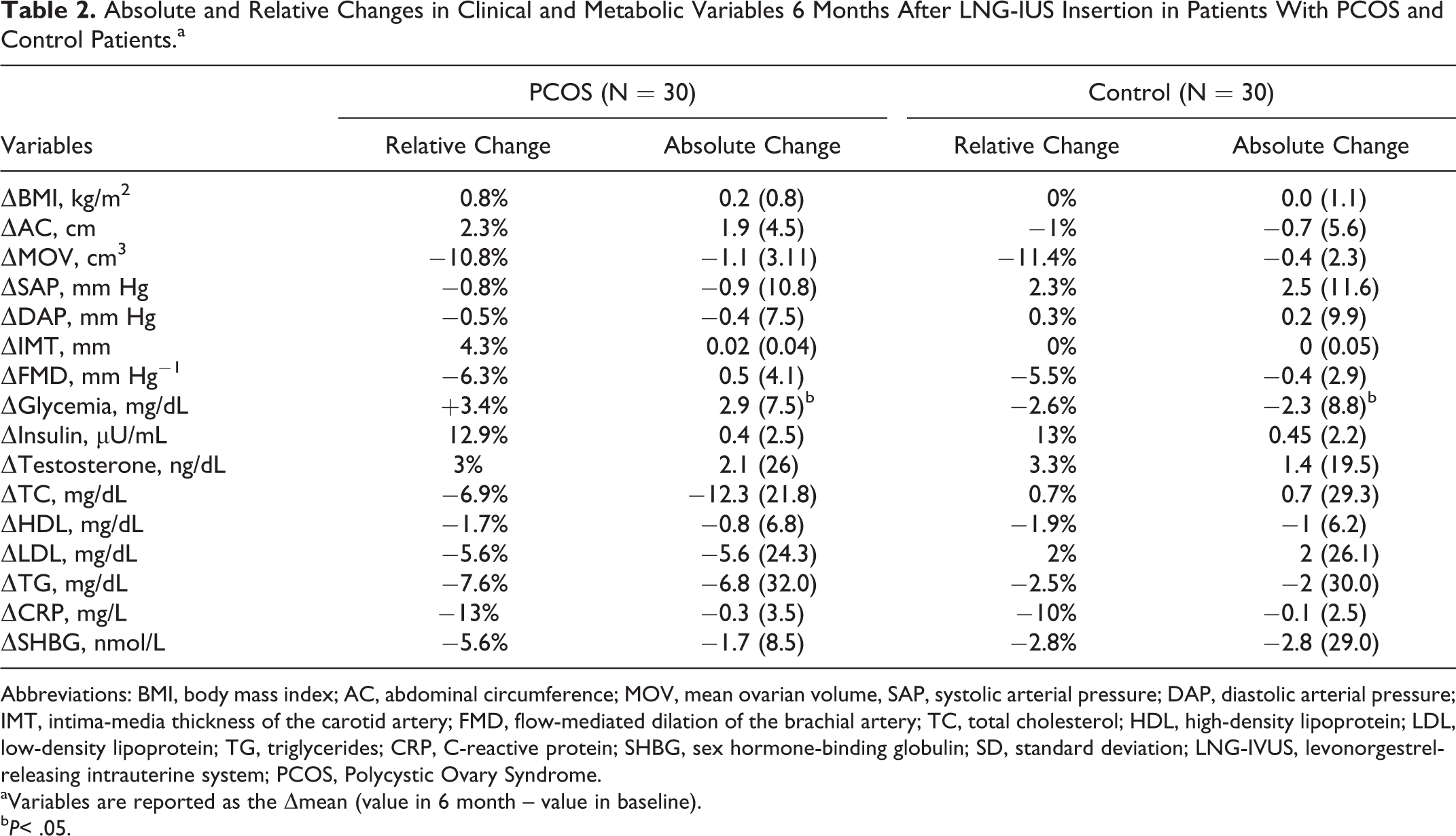
Only the variation in glycemia showed a significant difference between the groups, which increased 3.4% in the PCOS group and decreased 2.6% in the control group during the same period (P = .008). The remaining variables did not differ significantly between the groups (Table 2). Except for the ovarian volume of the women with PCOS, the remaining variables were within normal range.
Absolute and Relative Changes in Clinical and Metabolic Variables 6 Months After LNG-IUS Insertion in Patients With PCOS and Control Patients.a
Abbreviations: BMI, body mass index; AC, abdominal circumference; MOV, mean ovarian volume, SAP, systolic arterial pressure; DAP, diastolic arterial pressure; IMT, intima-media thickness of the carotid artery; FMD, flow-mediated dilation of the brachial artery; TC, total cholesterol; HDL, high-density lipoprotein; LDL, low-density lipoprotein; TG, triglycerides; CRP, C-reactive protein; SHBG, sex hormone-binding globulin; SD, standard deviation; LNG-IVUS, levonorgestrel-releasing intrauterine system; PCOS, Polycystic Ovary Syndrome.
aVariables are reported as the Δmean (value in 6 month – value in baseline).
bP< .05.
Discussion
The use of the LNG-IUS by women with PCOS was associated with some favorable modifications (a 6.7% reduction in TC levels, a 5.2% reduction in LDL levels, and a 10% reduction in ovarian volume) and some unfavorable changes (a 2.3% increase in AC and a 3.4% increase in fasting glycemia) during follow-up. However, these variations (except for ovarian volume) were less than 10% compared to the basal period, a fact that probably had no relevant clinical impact. Only the variation in glycemia differed between groups, with the PCOS group showing a 3.4% increase compared to a 2.6% reduction in the control group after 6 months of LNG-IUS use.
So far, the use of the LNG-IUS has been assessed only in women with PCOS who had endometrial hyperplasia, with no assessment of the metabolic or clinical effects of the use of this contraceptive by these women. 16,17 This information is interesting for the counseling of these patients, since there are women with PCOS for whom combined contraceptives are contraindicated, and there is no information about the impact of different POCs on women with PCOS. In addition, some women with PCOS could choose long-acting reversible contraceptives such as LNG-IUS due to their lower compliance with short-acting methods.
Among the variables of the lipid profile, combined contraceptives have a greater negative impact on triglyceride levels, causing increases of more than 40% among women without PCOS 18,19 and of up to 75% in women with PCOS, 12,20 regardless of the way of ethinyl estradiol administration. In women with PCOS, the increase in triglycerides is known to be associated with the antiandrogenic potential of progestogen. 21 The impact of the LNG-IUS on the lipid profile has been assessed only in women without PCOS and has been found to be associated with a reduction in TC and HDL compared to women who do not use hormonal contraceptives. 19 Healthy women with heavy menstrual bleeding using the LNG-IUS did not show significant changes in the variables of the lipid profile. 22,23 Another study showed that the use of the LNG-IUS as a contraceptive was associated with a reduction in HDL and triglycerides levels in women older than 40 years. 24 A reduction in the lipoproteins of the lipid profile has been observed in young patients with endometriosis after 6 months of LNG-IUS use. 25 In the present study, women with PCOS showed a modest reduction in LDL and TC without impairment of serum HDL or TG levels with the use of the LNG-IUS. This could be of interest, since the most prevalent changes in women with PCOS are elevated TG levels and reduced HDL levels, whereas increases in TC and LDL are less frequent. 26 In contrast, control women did not show any significant change in lipid profile. Since combined contraceptives may be associated with increased serum triglyceride levels, 27,28 the use of the LNG-IUS represents a potentially eligible method for women with PCOS with hypertriglyceridemia and other risk factors (such as obesity, for example) for whom the use of combined contraceptives is restricted. 9 Regarding HDL, POCs may reduce the serum levels of this lipoprotein, 19,23 although this effect was not observed in either group in the present study.
Glucose metabolism is not altered in users of LNG-IUS without PCOS. 19 Studies with a longer follow-up period (20 months) also demonstrated that neither the LNG-IUS nor the copper intrauterine device interferes with the daily need for insulin, levels of glycosylated hemoglobin, and glycemia in women with type 1 diabetes. 29 In the present study, a 3.4% increase in glycemia levels was observed in the PCOS group after 6 months of LNG-IUS use. This result may be secondary to the fact that the assay for glycemia determination showed a 5% coefficient of variability. Although there were no statistically significant changes in insulin levels, both groups showed a 13% increase in this hormone. Both groups had normal insulin levels not compatible with hyperinsulinemia. 30 However, studies with a longer follow-up, especially in women with PCOS, should be conducted to determine whether this finding has any long-term clinical relevance.
The markers of arterial function and structure such as FMD and IMT are preclinical markers of atherosclerosis. 13,31 Women with PCOS have an increased risk of various comorbidities, 5 –7 and these risk factors and metabolic disturbances may be associated with functional and structural impairments of the vascular system resulting in acceleration of atherosclerosis as these women age. The assessment of the impact of the use of combined contraceptives on the arterial function and structure of women with PCOS has contradictory results for combined methods involving antiandrogen progestogens (cyproterone, drospirenone, and chlormadinone), with data ranging from beneficial changes 12,28 to worsening of some markers. 32 The effect of the LNG-IUS on subclinical markers of atherosclerosis has been assessed only in women without PCOS, showing absence of negative effects within 12 months of observation. 33 In the present study, the use of the LNG-IUS did not change the arterial function or structure of women with and without PCOS during 6 months of observation. Since women with PCOS are more likely to have changes in these markers, 34,35 the use of a contraceptive that does not interfere with these markers in a negative manner contributes to the safety profile of the LNG-IUS in these women.
In the present study, women with PCOS showed a 2.2% increase in AC after 6 months of LNG-IUS use. However, since AC is a risk factor for the development of metabolic syndrome and of cardiovascular events, studies with longer follow-up periods are necessary to infer the impact of the LNG-IUS on the factors causing metabolic syndrome. Within this context, blood pressure did not alter with the use of the LNG-IUS, which is reassuring because women with PCOS are at higher risk of SAH during the fourth decade of life. 5
Total testosterone was first analyzed by radioimmunoassay which showed an increase of about 50% in serum total testosterone levels along follow-up in women with and without PCOS (data not shown). However, since the women had no complaints of increased clinical hyperandrogenism, we suspected that the levonorgestrel released by the LNG-IUS might have interfered with this result. To minimize this possible limitation, a new androgen determination was performed by liquid chromatography/mass spectrometry, the gold standard technique for this analysis, 36 showing that the use of the LNG-IUS for 6 months was not associated with changes in serum levels of total testosterone or SHBG. Thus, caution should be taken in choosing the method for the determination of total testosterone in women using contraceptives containing levonorgestrel in order to avoid inappropriate conclusions.
Combined oral contraceptives increase the hepatic synthesis of SHBG, with a consequent reduction in free testosterone and a contribution to the improvement in hyperandrogenism. 37 Progestogen-only contraceptives may not alter SHBG level. 38,39 In the present study, SHBG and free androgen levels did not change over the 6-month period of the study.
Both PCOS and control women had a reduction of about 10% in mean ovarian volume during follow-up, a characteristic that was not associated with the reduction in serum testosterone levels. This reduction may have been due to the effect of transitory suppression of ovulation which is more frequent during the first year of LNG-IUS use, 38 since this device does not have sufficient LNG concentrations to guarantee anovulation in most women. When using combined contraceptive methods, women with PCOS show a reduction in ovarian volume close to 30%, 12 since ovarian suppression is more pronounced in the presence of a higher dose of progestogens.
As a limitation of the study, the short follow-up period could be responsible for the lack of difference of most of the variables evaluated in PCOS women from the baseline period and from women without PCOS. Another limitation is as we evaluated multiple variables, we could not have enough power to detect differences in some comparisons. However, the relative changes in most of the variables were lesser than 10%, what could reflect a real lack of clinical effect of LNG-IUS in these variables even with a large sample size.
In conclusion, the use of the LNG-IUS for 6 months was not associated with relevant changes in clinical or metabolic markers in women without comorbidities, regardless of the presence of PCOS. Longer follow-up studies of women with PCOS using a LNG-IUS are needed to confirm whether or not there are long-term negative effects of this contraceptive in this group of women. In addition, LNG-IUS should be evaluated in women with PCOS and comorbidities. This information is important to produce evidence to the contraceptive counseling for women with PCOS who elect LNG-IUS, avoiding extrapolation of data from women without the syndrome.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the