
Abstract
To reinforce Sampson’s theory of retrograde menstruation in the pathogenesis of endometriosis, proof should be provided that during menstruation endometrial cells are present in peritoneal fluid (PF). We hypothesize that the prevalence of PF samples containing endometrial cells is higher in patients with endometriosis than in controls without endometriosis during menstruation. We selected from our biobank PF samples of 17 reproductive-age women with (n = 9) or without (n = 8) endometriosis who had received a diagnostic laparoscopy for investigation of pain/infertility. Peritoneal fluid had been collected during laparoscopy in the menstrual phase of the cycle, centrifuged, and the resulting pellet was stored at −80°C. About 5-μm sections of frozen PF pellets were stained using the Dako Envision Flex system with primary antibodies against epithelial cell adhesion molecule (Ep-CAM; endometrial epithelial cells), CD10 (endometrial stromal cells), prekeratin (epithelial/mesothelial cells), vimentin (endometrial/mesothelial/immune cells), calretinin (mesothelial cells), and CD68 (macrophages). The PF cells positive for Ep-CAM were detected in 5 of 9 patients with endometriosis and 6 of 8 controls (P = .62). CD10 stained positively in 6 of the 9 patients with endometriosis and 3 of the 8 controls (P = .35). Calretinin and prekeratin staining showed the presence of mesothelial cells in all pellets. Vimentin stained approximately 100% of the PF cells. CD68+ macrophages represented >50% of cells in all pellets. The prevalence of PF samples containing endometrial epithelial and stromal cells was not higher in patients with endometriosis than in controls without endometriosis during menstruation. Our findings question the relevance of endometrial cells in PF for the pathogenesis of endometriosis and support the importance of other mechanisms such as immune dysfunction and/or endometrial stem cells.
Introduction
Endometriosis is a benign gynecological disorder characterized by the growth of endometrial-like tissue outside the uterus. 1 The most common hypothesis concerning its origin is Sampson’s theory of retrograde menstruation, which states that during menstruation endometrial cells and tissue fragments flow backward through the fallopian tubes into the peritoneal cavity where they attach and develop into endometriotic lesions. 2 This concept is supported by the observation of an increased prevalence of endometriosis in women with menstrual outflow obstruction 3 and by the capacity of menstrual endometrium to form endometriotic lesions in baboons when seeded in the peritoneal cavity. 4
Retrograde menstruation has been defined as the presence of red-stained peritoneal fluid (PF) at the time of menstruation and is regarded as a physiological phenomenon, occurring in up to 90% of reproductive-age women with patent tubes. 5 –7 In contrast, only 6% to 10% of the general female population develops endometriosis. 1 However, the definition of red-stained PF as proof of retrograde menstruation may be insufficient, since red-stained PF has been observed outside the menstrual period 5 and correlates only weakly with the presence of endometrial cells in PF. 8 In the context of endometriosis, the presence of endometrial cells in the peritoneal cavity is more relevant than the observation of bloody PF. 9 Furthermore, the presence of endometrial tissue fragments as opposed to single endometrial cells may be essential due to their higher adherence capacity and evasion of the immune system 10,11 and their higher ability to form endometriosis-like lesions. 12
The presence of endometrial cells in PF, based on morphology, has been shown to vary significantly between 0% and 59%, 8,13 –15 partially due to problems related to accurate identification of endometrial cells in PF. 9 In order to reliably identify endometrial cells, immunological panels for epithelial, stromal, and mesothelial markers have been applied, successfully identifying endometrial epithelial cells during menstruation in PF of both cases with endometriosis and controls (50%-92%). 16,17 However, in a recent study, our group demonstrated a low prevalence of endometrial cells in PF during menstruation, as detected by Prep-stain methodology, 9 challenging the concept that retrograde menstruation is associated with a high number of endometrial cells floating in PF. It is possible that the low prevalence of PF endometrial cells was related to limitations of the Prep-stain technology used in our previous study, 9 such as the type of fixation 18 and the limited amount of possible stainings. Therefore, in this study, we cryosectioned PF pellets, a method that is more representative to obtain the full cellular content of PF than Prep-stain monolayers, to test the hypothesis that the prevalence of PF samples containing endometrial single cells and endometrial fragments (strands of epithelial cells and clusters of stromal cells) is higher in women with endometriosis than in controls.
Materials and Methods
Patient Inclusion
Since 1999, a biobank has been developed based on the collection and storage of samples after signed informed consent from women undergoing laparoscopic surgery at the Leuven University Fertility Center (LUFC). For each patient, detailed clinical information is available in the electronic file of the patient, including age, cycle phase at surgery, medication use, and a detailed surgery report with scoring and staging according to the classification of the American Society for Reproductive Medicine. 19 For the current study, the electronic biobank database of the LUFC was searched (April 2013) in order to identify all PF pellet samples collected at laparoscopy performed during the menstrual phase of the cycle in patients who were not taking any hormonal medication at the time of laparoscopy. The search identified 18 reproductive-age women (range 25-41 years, demographic data in Table 1) who had received a diagnostic laparoscopy for investigation of pelvic pain and/or infertility at UZ Leuven between January 2005 and July 2009 (since March 2010, PF has no longer routinely been collected during laparoscopy in our center).
Demographic Characteristics of the Study Population.
Abbreviations: PF, peritoneal fluid; SD, standard deviation.
A total of 15 (83.33%) of the 18 selected patients had bilateral patent fallopian tubes, 2 (11.11%) of the 18 women had 1 patent tube, and 1 (5.56%) patient did not have patent tubes and was excluded from the study, resulting in a total of 17 patients. Endometriosis was visually observed during laparoscopy in 9 women, histologically confirmed in 7 of the 9 cases (77.78%), and classified 19 into minimal–mild (n = 5) and moderate–severe (n = 4) disease. Controls (n = 8) included women with a normal pelvis (n = 3) or with nonendometriotic pathology (n = 5: myoma, n = 4; nonendometriotic adhesions, n = 4; nonendometriotic ovarian cysts, n = 1; parasalpingeal cysts, n = 2; hydrosalpinx, n = 1).
Peritoneal Fluid Collection
Peritoneal fluid had been aspirated during laparoscopy from the pouch of Douglas using a 20-mL syringe before any surgical manipulation and had been centrifuged (centrifuge Eppendorf 5702R, 300 g, 10 minutes; VWR, Haasrode, Belgium). After washing with phosphate-buffered saline, the supernatant had been discarded and the resulting pellet had been stored at −80°C until analysis.
Immunocytochemistry
All frozen PF pellets were embedded in KP Cryocompound (Klinipath, Olen, Belgium). 5-μm serial cryostat sections were prepared and mounted on Leica microsystems plus slides (Leica Biosystems, Diegem, Belgium). Sections were made vertically across the cell pellets to allow the detection of different cell layers possibly emerging after centrifugation. A total of 195 serial sections were prepared per pellet to ensure a representative image of its content (Figure 1). A total of 65 slides (3 sections per slide or total of 195 sections) were prepared to allow 9 independent immunocytochemical assessments of a Papanicolaou (Pap) staining and 6 different monoclonal antibodies (description below). Sections were fixed with Acetone GPR Rectapur (VWR) for 10 minutes before being air dried and stored at −20°C until staining. Immunocytochemical staining was performed using a standard protocol. Briefly, sections were rinsed in EnVision FLEX wash buffer (Dako Belgium NV, Heverlee, Belgium) before endogenous peroxidases were blocked with EnVision FLEX peroxidase-blocking reagent (Dako Belgium NV). After being washed, the slides were incubated for 30 minutes with ready-to-use primary mouse monoclonal (link) antibodies (Dako Belgium NV) against epithelial cell adhesion molecule (Ep-CAM, clone Ber-EP4), calretinin (clone DAK-Calret 1), prekeratin (PK, clone AE1/AE3), CD10 (clone 56C6), and CD68 (clone KP1), followed by another washing step and an incubation of 30 minutes with Dako EnVision FLEX/HRP detection reagent (antirabbit/antimouse HRP-linked secondary antibody; Dako Belgium NV). Incubation times for vimentin (clone V9) staining were 15 minutes for both primary and secondary antibodies. Then, the sections were washed again, and 3,3′-diaminobenzidine chromogen (EnVision FLEX DAB+ Chromogen diluted in EnVision FLEX Substrate Buffer; Dako Belgium NV) was added for 10 minutes to develop the immunostaining. After being rinsed in running tap water, sections were counterstained with hematoxylin and mounted using a standard automated protocol (AutoStainer XL-ST5010 Leica; Leica Biosystems).
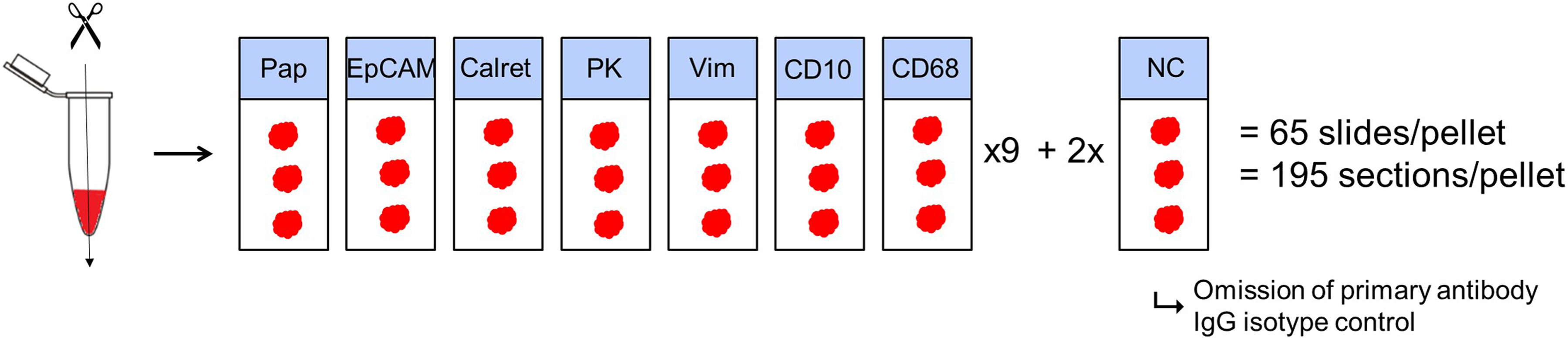
Overview of sectioning procedure. Sectioning was performed in vertical direction. The 7 different stainings (Papanicolaou, epithelial cell adhesion molecule [Ep-CAM], calretinin [Calret], prekeratin [PK], vimentin [Vim], CD10, and CD68) were successively performed 9 times per pellet. For the negative controls, the primary antibody was omitted. As an additional negative control, an immunoglobulin G (IgG)-matched isotype control was used. In total, 65 slides were made per pellet including 195 sections per pellet.
A Pap staining was performed using an automated protocol on a Coverstainer CS100-10037 (Dako Belgium NV) to affirm the presence of a sufficient amount of cells in the PF pellet.
Two types of negative controls were obtained for each pellet: omission of primary antibody and addition of an isotype control instead of primary antibody. A frozen endometrium biopsy and a frozen peritoneum biopsy were selected as positive controls for endometrial and mesothelial markers, respectively. Control biopsies were retrieved from our biobank (−80°C) and were refrozen in isopentane in liquid nitrogen to maintain tissue structure integrity during cryosectioning.
The selected markers (Table 2) are commonly used in effusion cytology and are relevant to identify endometrial epithelial or stromal cells, mesothelial cells, and macrophages in PF. According to the literature, Ber-Ep4 reacts with Ep-CAM and is specific for cells of epithelial 20 (and in rare cases mesothelial) origin. 9 Calretinin has been reported as a marker for mesothelial cells 20 and endometrial stromal cells. 21 Prekeratin is a marker for mesothelial and endometrial epithelial cells. 9 Vimentin stains endometrial stromal, mesothelial, and immune cells. 9 Vimentin is a mesenchymal marker but is also expressed in mesoderm-derived epithelia, such as the endometrial epithelium. 23 –26 CD10 is a marker specifically for endometrial stromal cells but also stains lymphocytes. 9,27,28 CD68 is specific for cells with monocyte/macrophage lineage. 9
Overview of Immunocytochemical Stainings of Different Markers According to Published Data and Comparison With the Current Study.
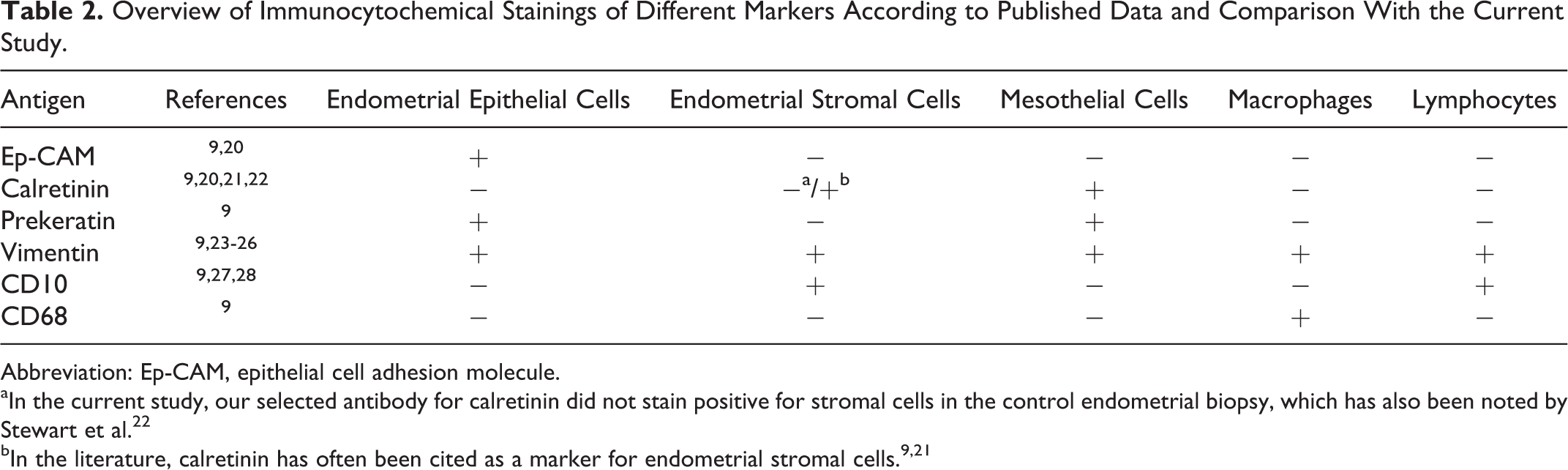
Abbreviation: Ep-CAM, epithelial cell adhesion molecule.
aIn the current study, our selected antibody for calretinin did not stain positive for stromal cells in the control endometrial biopsy, which has also been noted by Stewart et al. 22
Data Interpretation
For each PF pellet, all 195 sections were examined by the first author (D.O). Samples were considered positive if they exhibited any degree of cytoplasmic staining without nuclear aspecific reactivity and provided that the signal was observed in at least 2 subsequent sections. As the markers displayed a cytoplasmic/membrane staining pattern, any nuclear staining without cytoplasmic reactivity was considered negative. Each marker was reported as positive or negative. The PF pellets were defined to be positive for endometrial cells if they were positive for either Ep-CAM or CD10. Prevalence of samples containing a certain cell type was determined by dividing the amount of positive samples by the total amount of samples (either controls, endometriosis cases, or both). Fragments of endometrial cells were defined as (1) strands of Ep-CAM-positive epithelial cells or (2) cell clusters of CD10-positive stromal cell groups. Slides were evaluated by the first author (D.O), and representative slides were reviewed by an experienced and senior pathologist (T.R.) in a blinded fashion. All Ep-CAM and CD10-stained slides were assessed by the last author (A.F.), independently from the first author. If assessments between the first and last author did not correspond, the pathologist (T.R.) was consulted. This happened in 2 of the 17 pellets, once for Ep-CAM and once for CD10 staining. The pathologist’s decision was always decisive.
Statistical Analysis
Normality was tested with the D’Agostino and Pearson omnibus normality test to determine whether parametric or nonparametric tests were to be used in further analyses. Continuous variables were evaluated using the unpaired t test (age, PF volume) or Mann-Whitney U test (duration of infertility). A P value < .05 was considered statistically significant. To compare prevalence data, χ2 or Fisher exact test was used. All statistical analyses were done in GraphPad Prism version 6 (GraphPad Software, San Diego, California).
Ethical Approval
The study protocol was approved by the Commission for Medical Ethics of the Leuven University Hospital Gasthuisberg (UZ Leuven, Belgium). All patients had signed an informed consent.
Results
Antibody Specificity for Endometrial and Mesothelial Cells in Positive Control Biopsies (Endometrium and Peritoneum)
In the endometrial positive control tissue, Ep-CAM and PK exclusively stained epithelial cells (Figure 2, Table 2). Vimentin stained both epithelial and stromal cells. CD10 was specific for endometrial stromal cells, even though staining was faint. Calretinin failed to stain any cells in the endometrial biopsy. Macrophages, dispersed in the endometrial stroma, showed immunoreactivity for CD68.
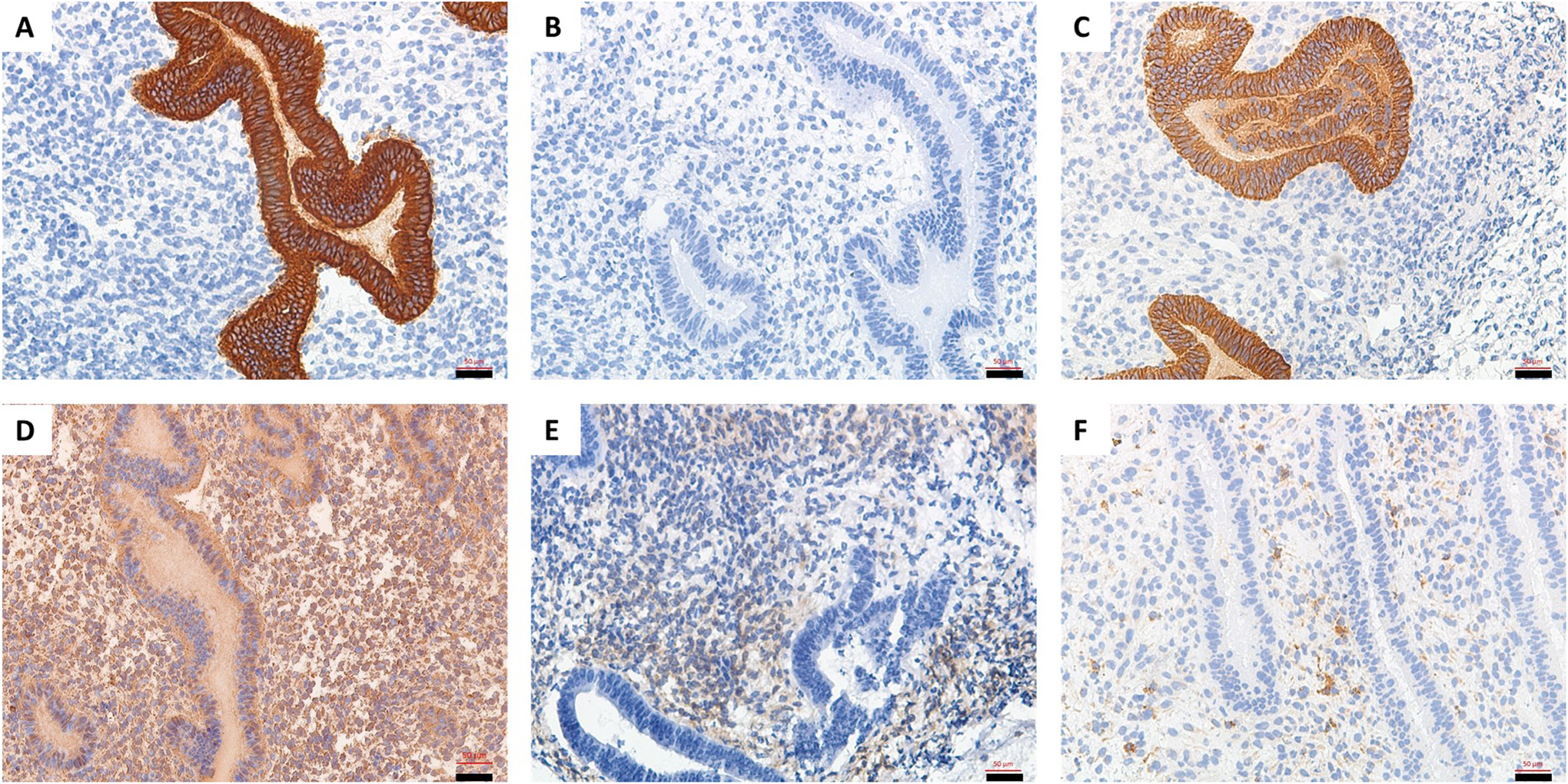
Endometrial biopsy as positive control for endometrial epithelial and stromal cell markers. The biopsy was stained with antibodies against (A) epithelial cell adhesion molecule (Ep-CAM; positive for endometrial epithelial cells), (B) calretinin (no positivity), (C) prekeratin (PK; positive for endometrial epithelial cells), (D) vimentin (positive for endometrial epithelial and stromal cells), (E) CD10 (positive for endometrial stromal cells), and (F) CD68 (positive for macrophages scattered in the endometrial stroma). Scale bars indicate 50 μm (20× magnification).
The normal peritoneum positive control tissue consisted of connective tissue covered by a mesothelial cell layer. The biopsy was oriented in order to visualize the mesothelial cell layer. Although mesothelial cells were negative for Ep-CAM, CD10, and CD68 (Figure 3, Table 2), they showed weak immunoreactivity for calretinin and strong immunoreactivity for PK. Vimentin was positive in mesothelial cells and the surrounding connective tissue.
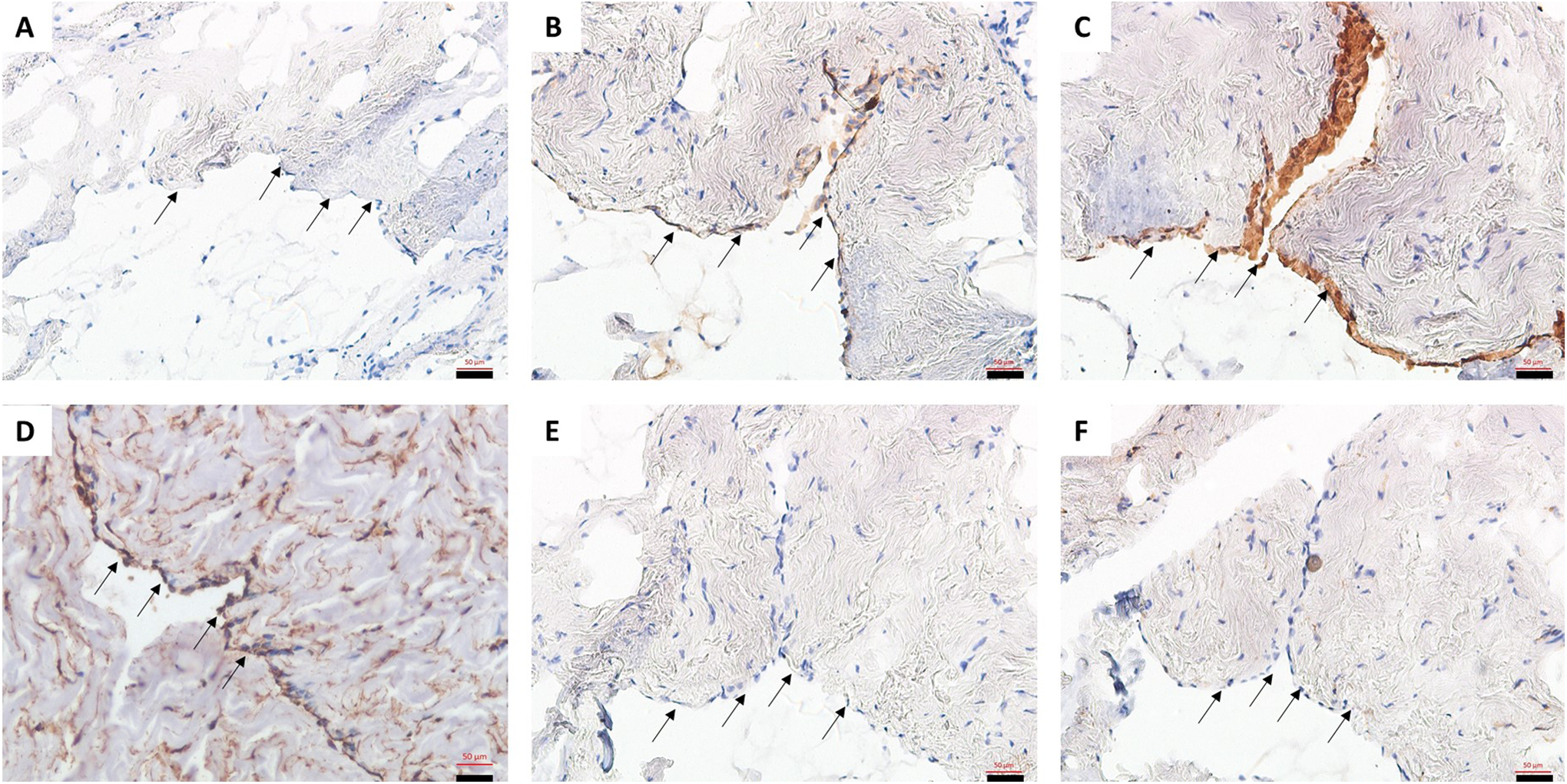
Peritoneal biopsy as positive control for mesothelial cell markers. The biopsy was oriented to visualize the mesothelial layer of the peritoneum (black arrows) and was stained with antibodies against (A) epithelial cell adhesion molecule (Ep-CAM; no positivity), (B) calretinin (positive in mesothelial cells), (C) prekeratin (PK; positive in mesothelial cells), (D) vimentin (positive in mesothelial cells and surrounding connective tissue), (E) CD10 (no positivity), and (F) CD68 (no positivity). Scale bars indicate 50 μm (20× magnification).
Peritoneal Fluid Pellet Cytology
Table 3 shows a summary of the immunocytochemical data. Figure 4 displays a representative image of each staining. In all pellets, the majority of the cells (50%-100%) were positive for vimentin. CD68 staining indicated the presence of macrophages in all PF pellets. Most pellets (14 of the 17) showed CD68 staining in >50% of the cells. Calretinin staining was seen in 12 of the 17 pellets, indicating the presence of mesothelial cells. The PK staining, representing the presence of endometrial epithelial cells or mesothelial cells, was overall more intense than calretinin staining and was detected in all pellets. In 3 pellets, calretinin was strongly present and overlapped with Ep-CAM staining for a proportion of the cells.
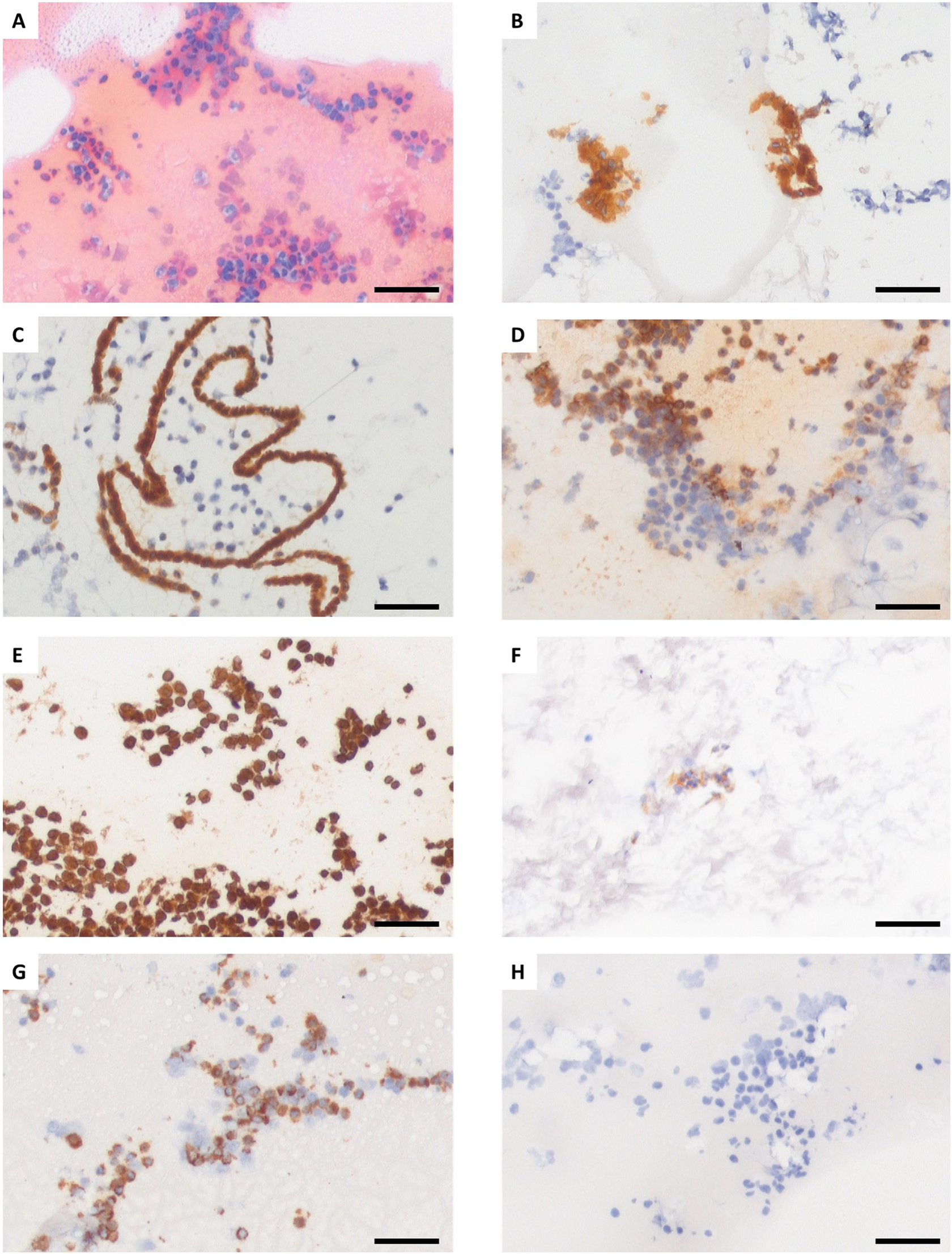
Representative images of prekeratin (PF) pellets for the selected markers. Illustration of (A) Papanicolaou (Pap), (B) epithelial cell adhesion molecule (Ep-CAM), (C) calretinin, (D) prekeratin (PK), (E) vimentin, (F) CD10, (G) CD68, and (H) negative control. Scale bars indicate 50 μm (20× magnification).
Immunocytochemical Reactivity Patterns for the 6 Different Markers in Peritoneal Fluid Pellets From Women With (n = 9) and Controls Without (n = 8) Endometriosis.
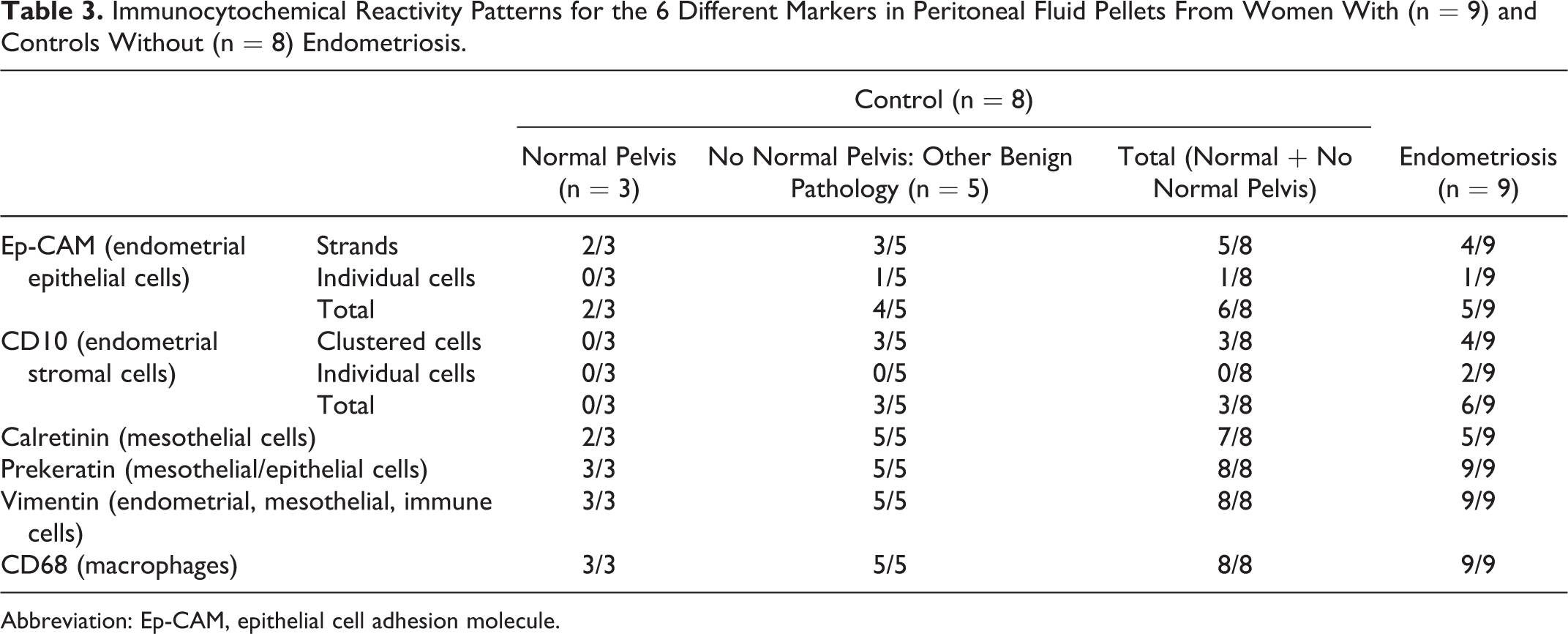
Abbreviation: Ep-CAM, epithelial cell adhesion molecule.
Tables 3 and 4 and Figure 5 show the results of immunocytochemical staining for endometrial epithelial (Ep-CAM) and stromal (CD10) cells. The Ep-CAM staining was seen in 11 of the 17 pellets (5 of the 9 endometriosis and 6 of the 8 controls). Of the 6 control women showing epithelial cells in the peritoneal cavity, 3 presented with myoma. Fragments of Ep-CAM-positive tissue in the form of strands were often seen, except in 1 case and 1 control where only individual positive cells were detected. CD10 staining was seen in 9 of the 17 pellets (endometriosis, n = 6; controls, n = 3). CD10 staining was found in clustered cell groups, except in 2 cases with endometriosis. Figure 5 illustrates the staining patterns of Ep-CAM and CD10 as individual cells or grouped in fragments in PF pellets. No significant difference in the prevalence of samples containing cells positive for Ep-CAM and CD10 was found when comparing cases with endometriosis and controls (P = .62 and P = .35, respectively) or when comparing cases with endometriosis and the subgroup of controls with a normal pelvis (P = 1 and P = .18, respectively). Comparing minimal–mild (stages I-II) and moderate–severe (stages III-IV) endometriosis did not reveal any significant difference in Ep-CAM (P = .21) or CD10 positivity (P = .52). Overall, the presence of fragments of endometrial cells (either Ep-CAM or CD10 positive) was not significantly different between cases with endometriosis and controls (P = .59).
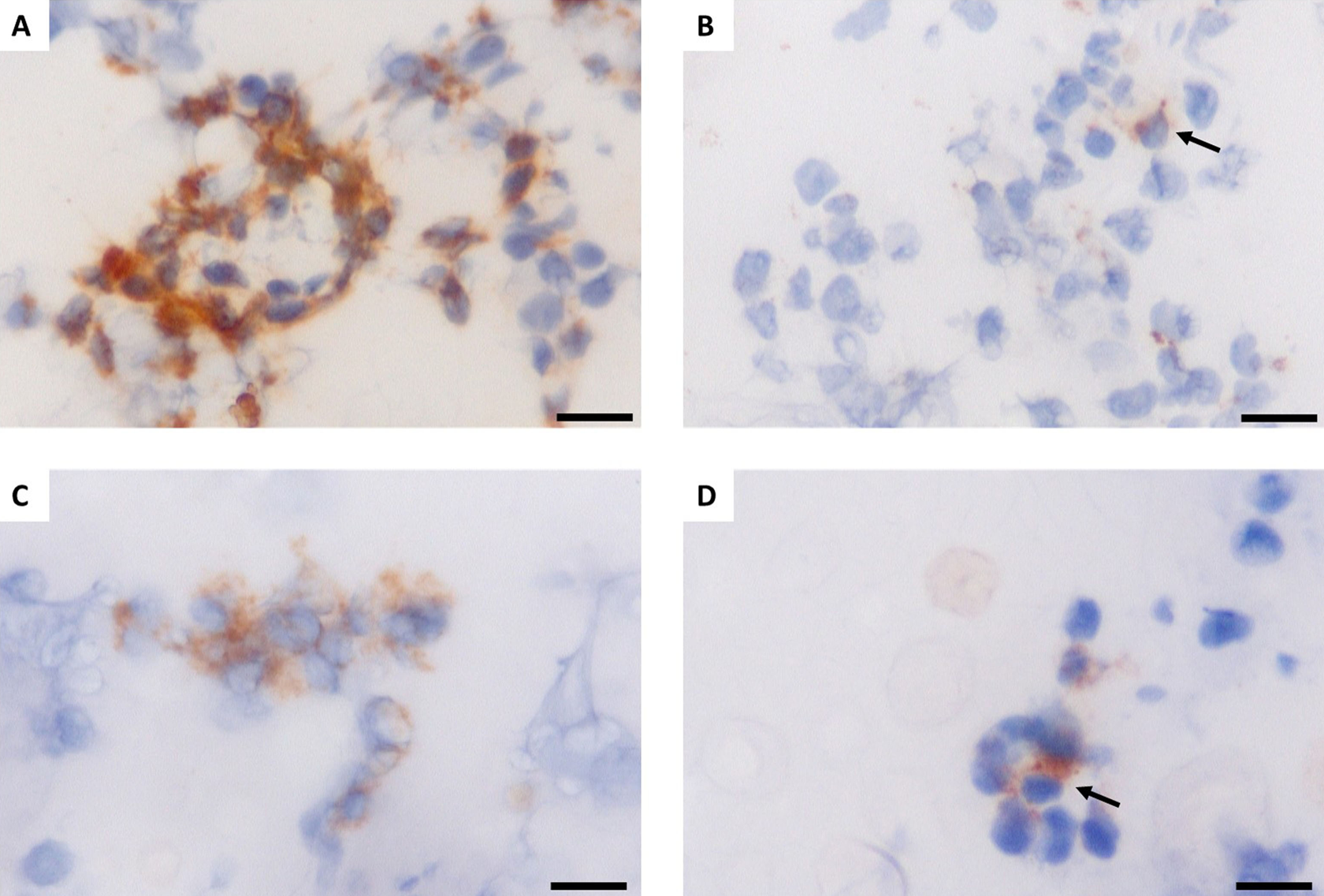
Epithelial cell adhesion molecule (Ep-CAM) and CD10 staining indicating the presence of endometrial epithelial and stromal cells. Illustration of (A) Ep-CAM positive cell strands, (B) an individual Ep-CAM positive cell, (C) a CD10-positive cell cluster, and (D) an individual CD10-positive cell. Scale bars indicate 20 μm (40× magnification). Arrows denote single positive cells.
Endometrial Markers Ep-CAM and CD10 Did Not Always Appear Concurrently in Peritoneal Fluid of Women With and Without Endometriosis.
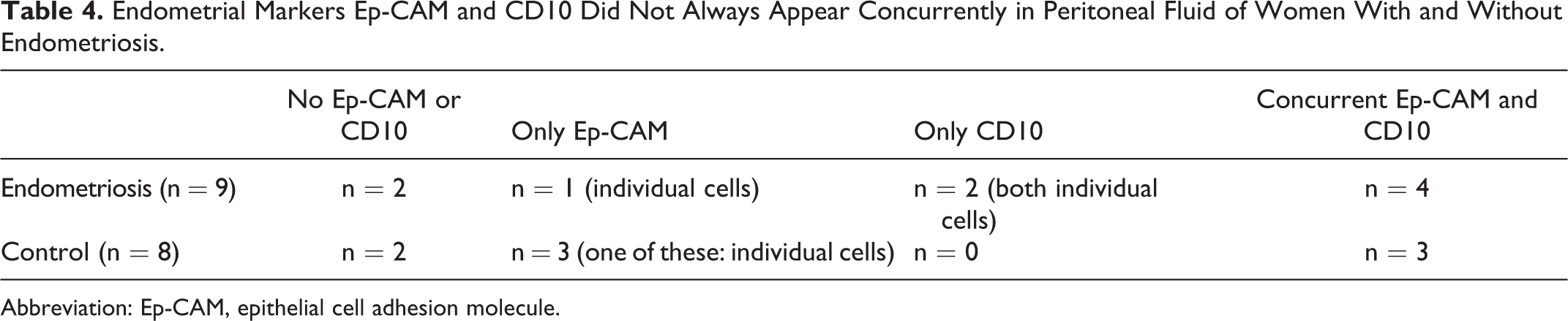
Abbreviation: Ep-CAM, epithelial cell adhesion molecule.
The Ep-CAM or CD10 staining was present in 13 of the 17 PF pellets (Table 4), but concurrent staining was only observed in 7 pellets, similarly in women with endometriosis and controls (P = 1).
Discussion
Our study investigated in detail the properties of the PF cell population using immunocytochemistry. Normal PF contains mainly macrophages and to a lesser extent mesothelial cells, lymphocytes, eosinophils, erythrocytes, and mast cells. 29 –31 In our study, CD68+ macrophages were the most abundant cell type in the PF, followed by mesothelial cells positive for PK and/or calretinin. We could not confirm our hypothesis that the prevalence of PF samples containing endometrial cells is higher in patients with endometriosis than in controls. We also did not find a difference in cell composition (tissue fragments vs individual cells) between cases with endometriosis and controls. Our data support the concept of retrograde menstruation as a common phenomenon but could not determine why some women develop endometriosis and others do not.
Diverging data have been reported on the prevalence of PF samples containing endometrial cells based on identification by (1) morphology (0%-59%) 8,13 –15,32 or (2) immunocytochemistry (0%-100%). 9,16,17,33 –36
In our current study, we report the presence of endometrial epithelial cells in PF collected during the menstrual cycle phase in 5 (55.56%) of the 9 cases with endometriosis and 6 (75%) of the 8 controls and the presence of endometrial stromal cells in 6 (66.67%) of the 9 cases with endometriosis and 3 (37.5%) of the 8 controls.
The strength of our study is the exclusive selection of PF pellets collected during menstruation, since we expected the most distinct difference in the presence of endometrial cells between cases and controls to occur at this time of the cycle. Four other studies using immunological methods reported results from patients in the menstrual phase of the cycle, 9,16,17,33 and none of these studies showed a difference in the presence of endometrial cells between cases with endometriosis and controls in this cycle phase (summarized in Table 5).
Summary of Literature Reporting Immunocytochemistry Techniques to Detect Endometrial Cells in PF of Patients With Endometriosis and Controls During the Menstrual Phase of the Cycle.
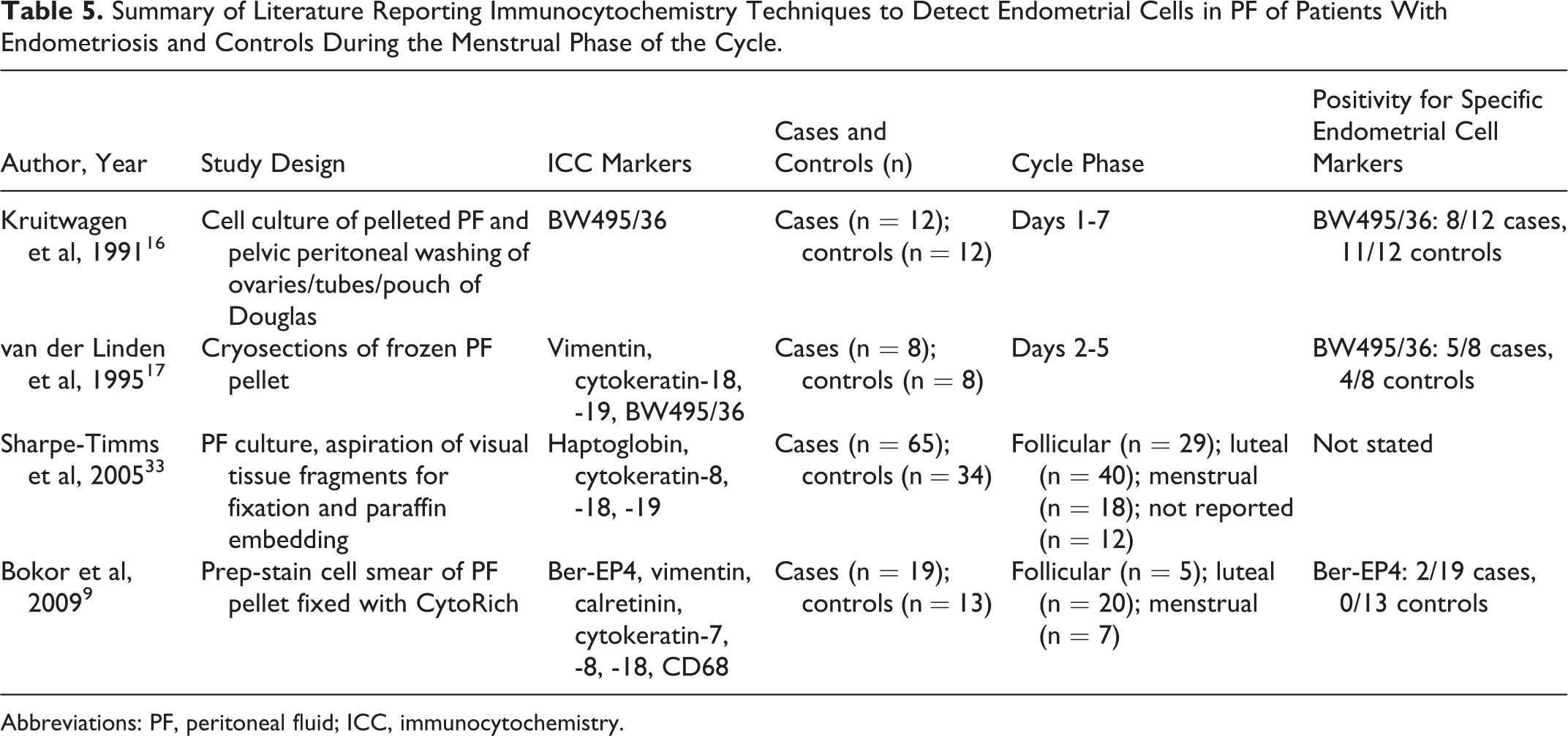
Abbreviations: PF, peritoneal fluid; ICC, immunocytochemistry.
A second strength of our study is the use of an extended antibody panel allowing us to distinguish endometrial, mesothelial, and immune cells (Table 2). Our study is the only one investigating both the epithelial (Ep-CAM) and stromal (CD10) component of the endometrial cells, whereas the other studies focused solely on the epithelial cell type. 9,16,17,33
Furthermore, our method of cryosectioning frozen PF pellets is preferred to cell culturing 16,33 or preparation of a cell monolayer 9 because it allows investigation of nonadherent, nonproliferative cells and avoids formalin-based fixation, which may cause loss of antigenicity. 18 Indeed, we found a higher prevalence of PF samples containing endometrial epithelial cells compared with the previous report by our group. 9 Cryosectioning was also used by van der Linden et al 17 whose results corresponded with ours, yet our study specified the serial staining of 195 consecutive sections, ensuring the reliable representation of the entire PF pellet content.
Our study was limited to a small sample size, especially for subgroup analysis of controls with a normal pelvis or patients with minimal–mild versus moderate–severe endometriosis. Overall, our sample size was comparable with the other studies investigating PF during the menstrual phase of the cycle (Table 5). Furthermore, semiquantitative assessment was impossible due to intra- and interpellet heterogeneity in antigen reactivity and cell density/number as also reported by Sharpe-Timms. 33 Heterogeneity is to some extent inherent to any cytological fluid.
The fact that we, and other groups, cannot (1) reliably associate endometriosis with the presence of endometrial cells in PF and (2) cannot document a difference between cases with endometriosis and controls, may have different origins. First, stem cells rather than the endometrial epithelial/stromal cells present in PF may be the major instigator of endometriosis. 37 Apart from endogenous endometrial cells, bone marrow stem cells may contribute to the regeneration of endometrium after menstruation. 38 These bone marrow stem cells may cause endometriosis by differentiating into endometrial cells in ectopic locations. 39 Second, acellular menstrual endometrial supernatant has been able to induce endometriosis in baboons, indicating the possibility that endometrial cells in the peritoneal cavity are not required for the development of endometriosis and that other substances in menstrual fluid may be involved. 40 Third, it may be difficult to document the presence of free-floating endometrial cells in the PF, because attachment of endometrial cells to peritoneum may take place within 1 hour according to in vitro data 41 or because endometrial cells may be cleared by the immune system. 42 Furthermore, clearance of endometrial cells by the immune system may be impaired in women with endometriosis. 42
In summary, we agree with other reports that endometrial cells are present in the PF of both cases and controls, without obvious difference between cases and controls of the prevalence of PF samples containing endometrial cells. In the future, studies should be performed with larger amounts of patients in the menstrual phase of the cycle, using adequate controls without tubal occlusion, implementing immunocytochemical methods and simultaneously investigating retrograde menstruation and the alternative theories for the development of endometriosis. To allow quantification of endometrial cells, fresh PF samples could be analyzed using flow cytometry. Further, it is important to note that the detection of endometrial cells in PF may be due to shedding from the lesions, 33 thereby representing a consequence rather than a cause of endometriosis. 11
Footnotes
Acknowledgments
The authors are grateful to Wilfried Versin and Carine Borgers for excellent technical assistance.
Authors’ Note
Thomas M. D’Hooghe and Amelie Fassbender are joint last authors.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Thomas D’Hooghe is vice president and head of Global Medical Affairs Infertility for the Multinational Pharmaceutical company Merck Serono (Darmstadt, Germany) and continues on a part-time basis his academic appointment as professor of Reproductive Medicine at the University of Leuven (KU Leuven) in Belgium.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Funding of this research was obtained from the Research Foundation-Flanders (FWO, application numbers 11X5515N and 33915) and the Clinical Research Foundation of Leuven University Hospitals.