
Abstract
It is well known that endometriosis is associated with an increase in the risk of deep dyspareunia, with potential negative effects on global female sexual functioning and couple relationship. The aims of this study were to review the literature on the impact of endometriosis on female sexual functioning and to suggest new avenues for future research and treatment strategies. An electronic database research was performed to identify all the studies on the relation between endometriosis and sexual functioning published in the period 2000 to 2016. This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. After the screening process, a total of 9 studies investigating the relation between endometriosis and female sexual functioning were considered. Overall, these studies indicated that around two thirds of women with endometriosis have some form of sexual dysfunction not limited to deep dyspareunia. These findings suggest that the global sexual impact of endometriosis requires further investigation, focusing not only on pain during intercourse but also on psychological and relational dimensions, including partner’s sexual functioning. Because sexual functioning is a complex, multidimensional phenomenon, the ideal treatment for endometriosis-related sexual dysfunctions should be conducted by a multidisciplinary team composed of gynecologists, sexologists, and psychologists/psychotherapists.
Introduction: “Sexual Health Matters”
Sexuality is a fundamental dimension of human life with important consequences on physical and psychological health and global quality of life. 1 This is particularly important if one considers that female sexual dysfunctions (including not only pain at intercourse but also desire, arousal, or orgasm problems) are relatively common. 2
Female sexuality can be negatively influenced by numerous factors, such as psychiatric and psychological dysfunctions, chronic diseases, endocrine disorders, drug use, 1 and operative vaginal delivery. 3 Moreover, women who are affected by chronic inflammatory gynecological diseases such as endometriosis may report sexual dysfunctions. Specifically, endometriosis is characterized by endometrial tissue located outside the uterine cavity (with ectopic implants on the ovaries, the tubes, the pelvic peritoneum, the bladder, the rectum) causing local inflammation. The most common symptom of endometriosis is pelvic pain, 4 which may lead to impaired mental health and quality of life. 5 Endometriosis is also associated with a 9-fold increased risk of deep dyspareunia. 4 -7 The presence of endometriotic lesions infiltrating the posterior vaginal fornix, the pouch of Douglas, the uterosacral ligaments, and the rectum (ie, deep infiltrating endometriosis [DIE]) causes pain at intercourse due to mechanical pressure on lesions occurring during coitus or due to traction of scarred and inelastic endometriotic tissue. 6
Because the disease afflicts about 5% to 10% of reproductive-age women, 8 it is reasonable to suppose that at least 2% to 4% of all sexually active women may experience painful intercourses due to endometriosis. As demonstrated by several studies, 9 -14 pain during intercourse is frequently associated with a wide range of different sexual dysfunctions, such as hypoactive sexual desire, lubrication, arousal, and orgasm disorders. Moreover, fear and anticipation of pain, resulting from repeated painful sexual experiences, represent powerful inhibitors of the sexual response cycle. 1,15,16
The negative sexual impact of endometriosis on women and their partners, as well as the effects of endometriosis on surgical and pharmacological treatments, was recently highlighted in 2 reviews. 17,18 A qualitative study by Denny and Mann 7 showed that endometriosis-related dyspareunia may negatively affect women’s lives to the point that some participants were completely avoiding sexual activity, with decreased self-esteem and quality of couple relationships (while some others were likely to tolerate pain only to please their partner).
Taken together, these findings indicate that women with endometriosis may experience remarkable sexual impairment, with potential negative consequences on their psychological and physical health and quality of life, especially if one considers the chronic nature of the disease and its association with infertility. In order to draw even more attention to the importance of sexual functioning in women with endometriosis, we conducted a systematic review to clarify the association between endometriosis and sexual dysfunction, which represents the specific focus of this article (ie, we did not explore the effects of endometriosis treatments, since they have been evaluated elsewhere 17,18 ). Moreover, secondary aims are to suggest new areas of research and future treatment strategies based on a critical analysis of the available evidence.
Materials and Methods
This systematic review was conducted according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines. 19 Since only published data were considered, the current research project was exempt from institutional review board approval.
An electronic database search (PubMed, MEDLINE) was conducted to identify all English language, peer-reviewed journal articles published between January 2000 and September 2016 on the impact of endometriosis on female sexual functioning, with a broad overview on several aspects of female sexuality and not just deep dyspareunia. Appropriate search terms were selected by reviewing titles, keywords, and abstracts of a sample of studies examining sexual functioning in women affected by endometriosis. Combinations of Medical Subject Headings terms “endometriosis,” “DIE,” “rectovaginal endometriosis,” “sexual functioning,” “sexual dysfunction,” “sexuality,” “dyspareunia,” and “sexual life” were used. Moreover, we further checked the reference lists of all the retrieved papers to identify additional articles. No effort was made to retrieve the results of unpublished studies.
Study Selection and Data Extraction
An independent screening of all titles and abstracts was conducted by 2 authors (G.B. and F.F.) to exclude irrelevant or duplicate citations. Because our aim was to investigate all aspects of sexual functioning in women having endometriosis, we included in the present review only articles in which sexual outcomes were assessed with a comprehensive sexual questionnaire focusing not only on pain at intercourse but also on other aspects of female sexuality, such as desire, frequency of intercourses, arousal, pleasure with sex, and global sexual satisfaction. Exclusion criteria were qualitative research, commentaries, or review articles without original data; case reports; studies in which pain at intercourse was the sole sexual outcome considered; or studies in which sexual functioning was assessed as an outcome measure following surgical or pharmacological treatment for endometriosis.
A data extraction form was designed by 2 authors (G.B. and F.F.) and applied to each article to independently extract information on author, year of publication, country, main objective, study design, number of participants, type of endometriosis, sexual functioning questionnaire, and outcomes.
Results
During the electronic database research process, a total of 618 articles were identified as potentially relevant. Of these 618 articles, 63 had titles or abstracts reporting information on the association between endometriosis and sexual functioning and were thus retrieved for evaluation. A total of 54 articles were excluded for the following reasons: 22 because they were studies evaluating sexual functioning after surgical or pharmacological treatment for endometriosis 20 -41 ; 14 because no comprehensive sexual questionnaires were used and dyspareunia was the only sexual outcome evaluated or no specific information from the questionnaires used was reported 6,42 -54 ; 13 because they were review articles or commentaries 4,11,17,18,55 -63 ; 3 studies because the language was not English 64 -66 ; and 2 because they were qualitative studies. 7 -67
Complete author agreement (G.B. and F.F.) regarding included and excluded studies was obtained. The flow diagram of the literature search results is reported in Figure 1.
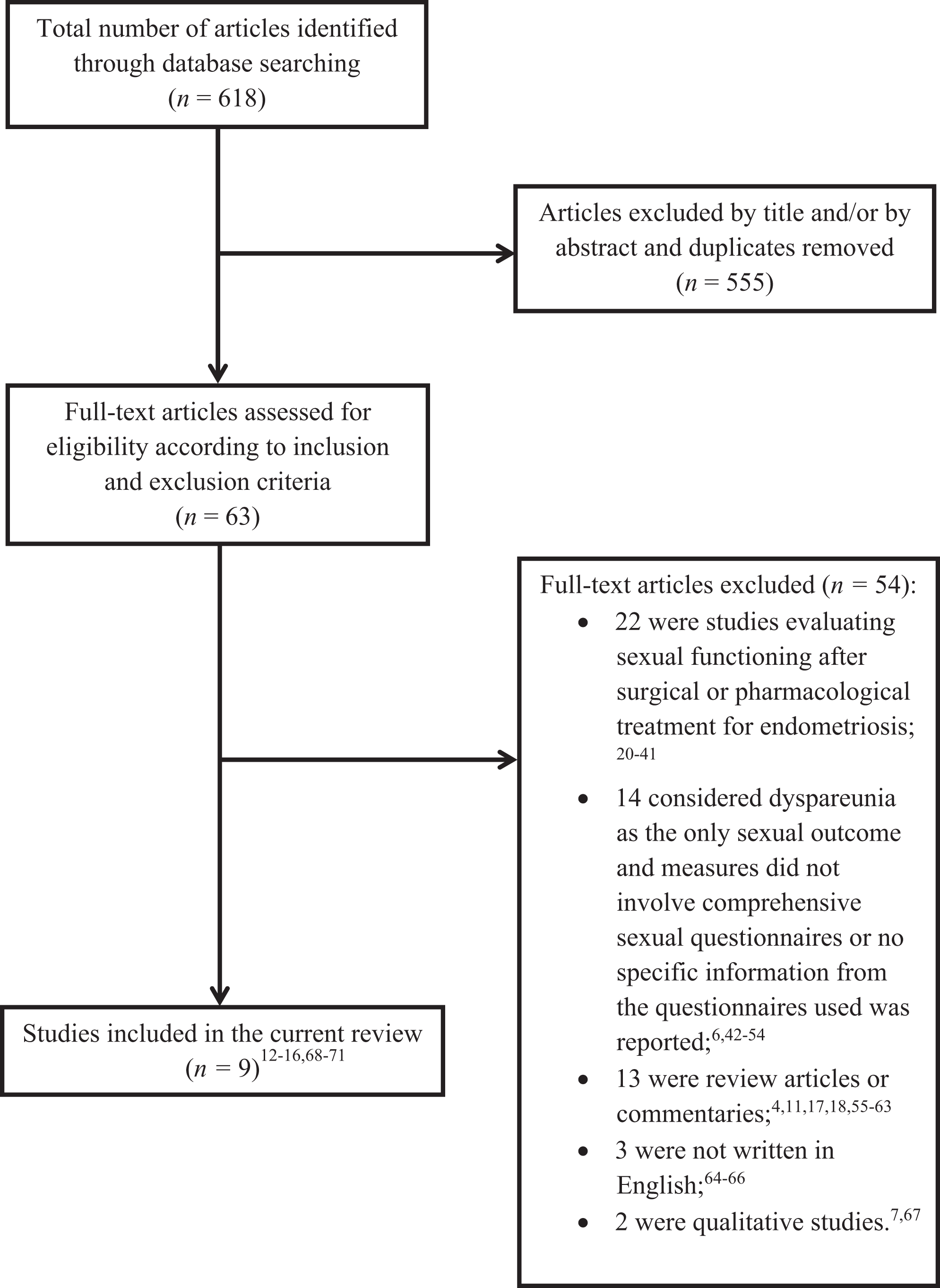
Study selection flowchart.
As a result of the article selection process, 9 studies were eventually included in the current systematic review, all of which investigated the impact of endometriosis on sexual functioning regardless of the effects of medical treatment. 12 -16,68 -71
The characteristics of the selected studies (author, year, country, study aims, study design, sample, type of endometriosis, sexual functioning measures) are reported in Table 1. Overall, there were 5 cross-sectional studies, 12,13,68,69,71 3 case–control studies, 14,15,70 and 1 multicenter cohort study. 16 Several sexual questionnaires were used in the studies considered (see Table 1): the revised Sabbatsberg Sexual Self-Rating (SRS) scale, 72 the Sexual Satisfaction Subscale of the Derogatis Sexual Functioning Inventory, 73 the Global Sexual Satisfaction Index, 73,74 the Sexual Health Outcomes in Women Questionnaire (SHOW-Q), 75 the Female Sexual Function Index (FSFI), 76 the Female Sexual Distress Scale, 77 the Golombok-Rust Inventory of Sexual Satisfaction (GRISS), 78 and the Sexual Self-Consciousness Scale. 79 The FSFI 76 was used in 4 of the 9 studies included as the main outcome measure. 13,16,69,71 Main results of studies included in the current systematic review are reported in Table 2.
Characteristics of Studies Included in Systematic Review of Evaluation of Sexual Functioning in Women With Endometriosis.
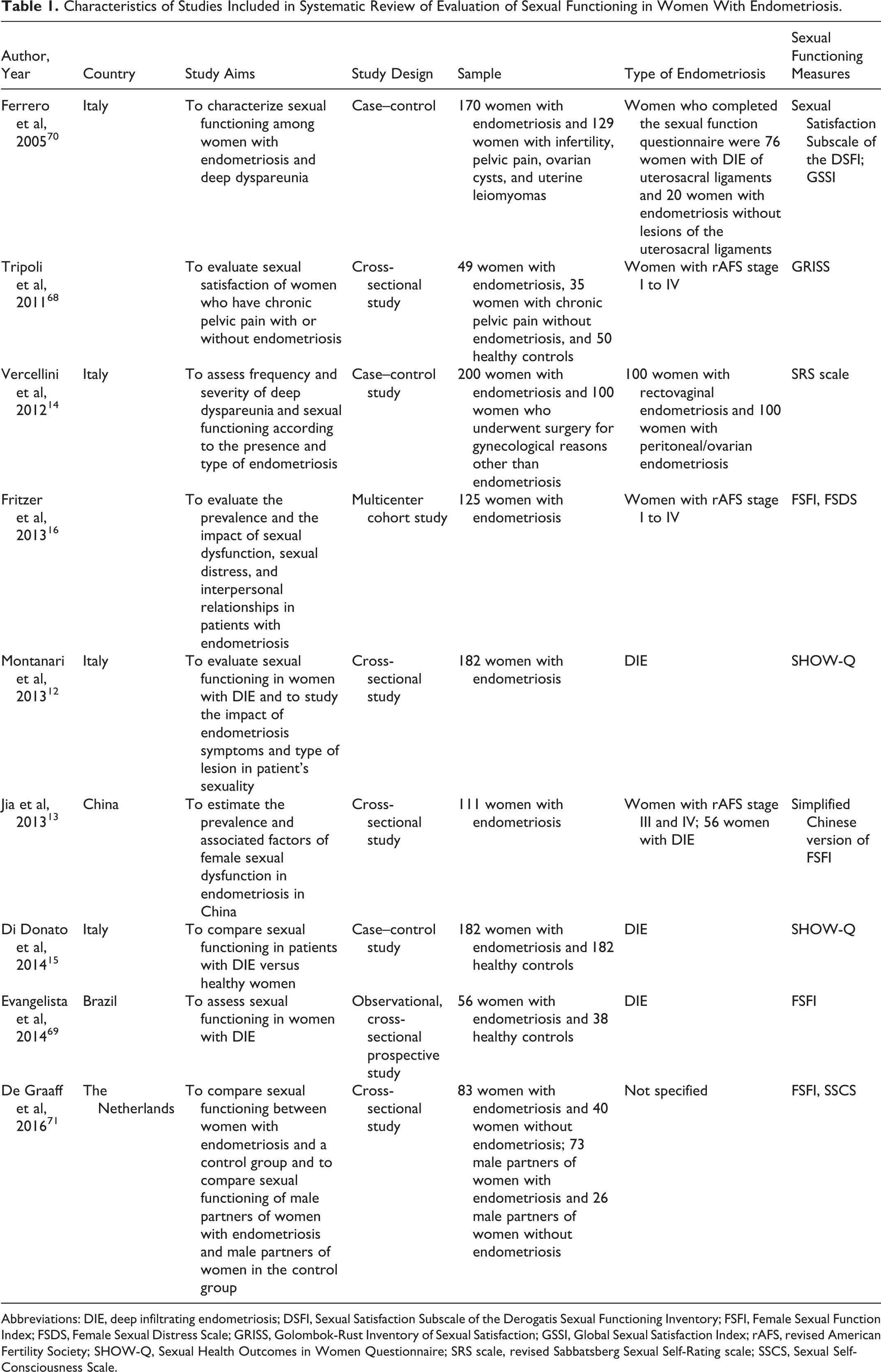
Abbreviations: DIE, deep infiltrating endometriosis; DSFI, Sexual Satisfaction Subscale of the Derogatis Sexual Functioning Inventory; FSFI, Female Sexual Function Index; FSDS, Female Sexual Distress Scale; GRISS, Golombok-Rust Inventory of Sexual Satisfaction; GSSI, Global Sexual Satisfaction Index; rAFS, revised American Fertility Society; SHOW-Q, Sexual Health Outcomes in Women Questionnaire; SRS scale, revised Sabbatsberg Sexual Self-Rating scale; SSCS, Sexual Self-Consciousness Scale.
Main Results of Studies Included in Systematic Review of Evaluation of Sexual Functioning in Women With Endometriosis.
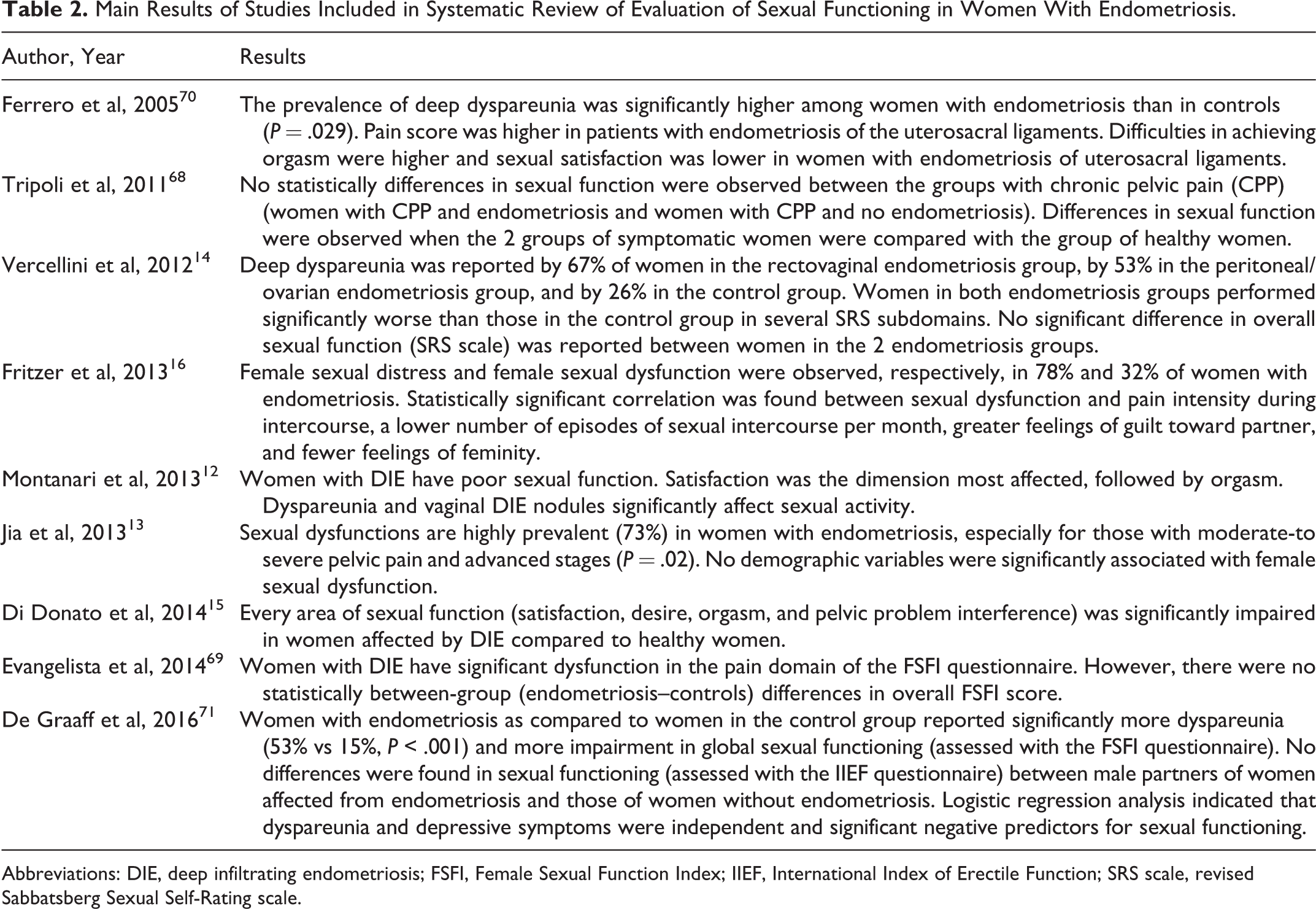
Abbreviations: DIE, deep infiltrating endometriosis; FSFI, Female Sexual Function Index; IIEF, International Index of Erectile Function; SRS scale, revised Sabbatsberg Sexual Self-Rating scale.
Six studies evaluated in this review focused on patients with a specific type of endometriosis, such as DIE. 12 -15,69,70 Overall, sexual functioning was investigated in 1158 women diagnosed with endometriosis and the sample size of the considered studies varied from 49 68 to 200 women. 14 As shown in Table 1, 6 studies involved a control/comparison group (healthy controls or women with gynecological conditions other than endometriosis). 14,15,68 -71
As regards the prevalence of sexual dysfunctions in women with endometriosis, in a multicenter cohort study on 125 women with endometriosis and dyspareunia lasting for at least 6 months, 16 sexual dysfunction and sexual distress were found in 32% and 78% of participants, respectively. Interestingly, 30% of patients referred that the primary motivation for sexual intercourse was just to try to conceive, whereas 46% of women reported that they were willing to tolerate pain at intercourse in order to satisfy their partner and avoid conflicts. There were significant correlations between female sexual dysfunctions and pain intensity during or after intercourse, sense of guilt toward the partner, and fewer feelings of femininity, whereas no significant associations were found with DIE.
The factors associated with the presence of sexual dysfunctions in women with endometriosis were specifically investigated by Jia et al. 13 In their study on 111 women with endometriosis, the prevalence of sexual dysfunction was 73%, and 3 potential predictors of dysfunctions were identified: pelvic pain intensity, presence of DIE, and advanced American Society for Reproductive Medicine classification stages. 80 A recent cross-sectional study by Montanari et al, 12 investigating the specific sexual impact of different endometriosis symptoms and types of lesions in women with DIE, revealed that dyspareunia and vaginal nodules were significantly associated with poorer sexual functioning. Overall, women showed impaired sexual functioning, especially in relation to satisfaction and orgasm; 61.5% of patients with DIE indicated a low frequency of sexual intercourse, whereas 71.4% reported remarkable interference of their pelvic problems with sexual activity.
Six studies compared sexual outcomes in women with endometriosis versus healthy women or women without endometriosis, showing a significantly worse sexual functioning in the endometriosis population. 14,15,68 -71 Only 1 study 69 reported high prevalence of dyspareunia in 57 women with DIE (75%) versus 38 healthy controls (34%). Patients with DIE reported greater pain at intercourse (ie, the pain domain of the FSFI questionnaire), although with no effects on the overall sexual functioning (ie, the FSFI global score). The other 5 studies showed significantly decreased sexual functioning in women with endometriosis relative to the control/comparison group. 14,15,68,70,71 Ferrero et al 70 investigated the quality of sexual life in 309 women having deep dyspareunia by comparing 3 conditions: DIE of the uterosacral ligaments, endometriosis without deep infiltrating lesions of the uterosacral ligaments, and a control group composed of women without endometriosis. The prevalence of deep dyspareunia was significantly higher in the 2 endometriosis groups (60.6%) compared with controls (34.9%). Women with DIE of the uterosacral ligaments exhibited the most severely impaired sexual functioning, with greater pain and poorer orgasm, and felt less relaxed and satisfied after sex compared with the other 2 conditions. The presence of bilateral uterosacral ligament lesions did not affect symptom severity.
Tripoli et al 68 investigated sexual satisfaction in 84 women having chronic pelvic pain (CPP) with or without endometriosis versus 50 healthy controls. Sexual functioning was assessed using the GRISS questionnaire, 78 a psychometric instrument focused on frequency of relations, sexual communication, sexual satisfaction, sexual aversion, lack of expression of sensuality, vaginismus, and anorgasmia. Of the 84 participants with CPP, 40% were sexually unsatisfied and reported decreased frequency of sexual intercourses, reduced expression of sensuality, and higher rates of sexual aversion. No significant differences were found between the 2 CPP conditions (with and without endometriosis).
Vercellini et al 14 evaluated sexual functioning and deep dyspareunia in 100 women with rectovaginal endometriosis, 100 women affected by peritoneal and/or ovarian endometriosis, and 100 women without endometriosis. Items of the self-assessment questionnaire of sexual functioning (SRS) measured sexual interest, sexual activity, sexual satisfaction, experience of sexual pleasure, orgasm capacity, and sexual relevancy. Women with endometriosis (either rectovaginal or peritoneal/ovarian endometriosis) reported worse sexual functioning relative to women without endometriosis, although with marginal differences. The majority of participants with endometriosis (67% in the rectovaginal group and 53% in the peritoneal/ovarian group) had deep dyspareunia (vs 26% of women without endometriosis). Surprisingly, the severity of dyspareunia did not affect overall sexual functioning in women with endometriosis. A possible explanation of this unexpected finding was that because female sexuality is a multidimensional phenomenon and includes psychological processes, the effect of dyspareunia could have been diluted by other factors, such as degree of couple intimacy, coping capacity, personality traits, marital adjustment, and partner support.
Di Donato et al 15 used the SHOW-Q 75 to evaluate sexual functioning in 182 women with DIE versus 182 healthy women. Women with DIE exhibited greater sexual impairment in all sexual functioning domains (satisfaction, desire, orgasm, and pelvic problem interference with sex) relative to healthy controls; 58% of participants in the DIE group (vs only 1% in the control condition) reported that pelvic pain severely affected their sexual functioning. Sexual desire was absent or experienced less than 1 or 2 times per month in 45% of patients with DIE relative to 14% of healthy controls.
The only study evaluating sexual functioning in patients with endometriosis, in their partners, and in a control group was recently performed by De Graaf et al. 71 The authors found that women with endometriosis as compared with women in the control group reported significantly more dyspareunia (53% vs 15%) and CPP, as well as more impairment in global sexual functioning and in global quality of life. Interestingly, no differences were found in sexual functioning (assessed with the International Index of Erectile Function questionnaire 81 ) between male partners of women affected by endometriosis and those of women without endometriosis. Logistic regression analyses indicated that dyspareunia and depressive symptoms were negative predictors for sexual functioning. 71 Based on these findings, the authors suggest future investigations on the effect of depression-focused therapy on sexual functioning of women with endometriosis.
Overall, the clinical scenario described by these studies was that around two thirds of women with endometriosis have sexual dysfunctions (pain at intercourse, low satisfaction, lack of desire, low arousal, orgasm difficulties), with a negative impact on women’s psychological well-being and intimate relationships. 12 -14,16
Discussion and Conclusion
In the last 15 years, improving sexual functioning has become a major clinical challenge in treating women with endometriosis. Multiple forms of sexual dysfunction are reported by a remarkable percentage of women having endometriosis (about 60%-70%), with a significant negative impact on intimate relationships and quality of life in general. Moreover, research has shown that dyspareunia, although important, is not the exclusive sexual complaint in women affected by endometriosis, as hypoactive sexual desire and orgasm dysfunctions are relatively frequent.
The heterogeneity of the studies included in this review (in terms of research methods, types of endometriosis, and types of questionnaires used to assess sexual outcomes) did not allow us to perform a meta-analysis of the observed results, which we acknowledge as an important limitation of our study. However, this review may draw attention to the fact that endometriosis, especially DIE or those forms associated with severe deep dyspareunia, 12 -15,69,70 has a remarkable negative influence on several aspects of female sexual functioning, such as desire, orgasm, frequency of sexual intercourses, and global satisfaction with sex.
The estimated high prevalence of endometriosis-related sexual dysfunctions (about two thirds of women with endometriosis) is particularly alarming. This can be due to the fact that most of the studies were conducted in patients with DIE or in women having pain at intercourse caused by endometriosis; in this light, the observed high proportion of patients having sexual dysfunctions could be reasonably lower if one considers the entire population of women with endometriosis, including peritoneal and ovarian endometriosis and not only DIE. Moreover, it is a fact that sexual dysfunctions are estimated to be relatively common in the general adult population. 2 A large survey reported that about 40% of the women interviewed had some type of sexual problems, among which the most common was hypoactive sexual disorder, with an unadjusted prevalence of about 38%. 2 On one hand, such a surprising percentage of sexual dysfunctions in the general population raises clinical and sociological concerns with regard to contemporary society and disease mongering. On the other hand, this proportion may help understand the very high prevalence of sexual dysfunction in women with endometriosis and define its negative impact not only in terms of physical and psychological well-being but also in terms of endometriosis-related economic costs.
Overall, research on sexual functioning in women with endometriosis substantially investigated female sexual dysfunction using the classification reported in the different editions of the Diagnostic and Statistical Manual of Mental Disorders 82 (eg, orgasmic disorder, sexual interest/arousal disorder, and genito-pelvic pain/penetration disorder), as well as validated questionnaires such as the FSFI, which is important to increase methodological rigor and comparability of findings. However, conceptualizing sexual dysfunction only in terms of specific disorders, such as those mentioned above, does not allow comprehensive understanding of the extent to which endometriosis may negatively affect a woman’s sexual life.
We believe that sexual dysfunction in all women, and especially in those with a chronic gynecological disease such as endometriosis, depends on a variety of factors that may moderate the impact of the disease. Findings from qualitative research 7,67,83 suggest that either individual factors (such as self-esteem, mental health) or relational variables (such as the quality of intimate relationships) may shape the way in which each woman experiences endometriosis. A recent qualitative study 83 showed that nondistressed women were still enjoying their sexuality despite endometriosis (for instance, they had been able to find comfortable and painless sexual positions), while distressed women with clinically significant symptoms of anxiety and depression were totally avoiding any type of sexual activity due to not only pain but also overwhelming concerns about infertility and lack of support from partners. These findings suggest that there may be a mutual complex interaction between psychological distress, which is associated with pelvic pain (especially chronic, nonmenstrual pelvic pain 5 ), and sexual dysfunction. Thus, the high proportion of endometriosis-related sexual problems reported in this review may be not only due to coital pain caused by endometriosis-related anatomical distortion or pelvic inflammation (which has been the main focus of both endometriosis research and treatment) but also due to psychosocial factors, including emotional distress associated with the disease and quality of intimate relationships.
These ideas raise new important research questions. For example, why are some women with endometriosis more likely than others to tolerate pain at intercourse in order to satisfy their partner? Why do some women try to find personal solutions to relieve pain (for instance, by searching for the right position to avoid pressure or deep penetration), while others completely avoid any type of intercourse? As indicated by recent research on endometriosis, 84 individual factors such as personality traits (neuroticism, pessimism, harm avoidance) may play a role in the way women cope with the pain due to the disease. The association between personality and sexual behaviors in women with endometriosis may represent an interesting new area of research. Other individual factors such as sense of femininity, body image, and self-esteem should be investigated focusing on their association with sexual functioning. Moreover, relational dimensions may also be important. For instance, overall marital satisfaction and feelings toward the partner, as well as perceived partner responsiveness and support, intimacy, and closeness may significantly affect sexual functioning. Partner sexual functioning should also be investigated, since there is very poor research focused on endometriosis and intimate relationships. This is surprising, considering that according to the Endocost study, a large proportion of women have important relationship and marital problems (including divorce) due to endometriosis. 51
Such new research could lead to the implementation of more effective multidisciplinary treatment programs for the individual woman as well as for the couple (see Figure 2). This appears to be of particular importance in women dealing with a chronic disease affecting sexuality, such as endometriosis. In this regard, a holistic approach, rather than a mechanistic approach, is necessary to acknowledge the complex nature of human sexuality and the importance of individual differences.
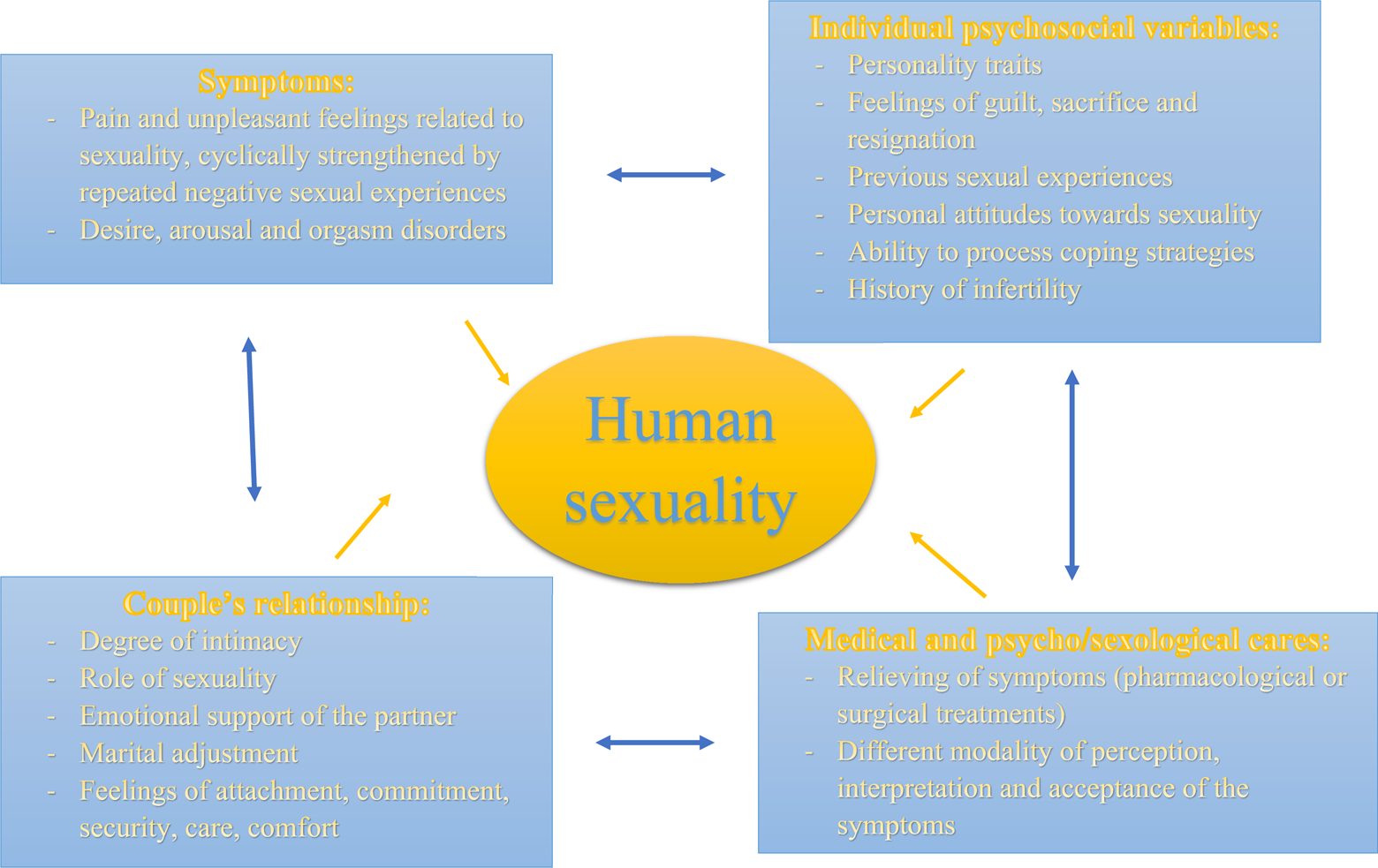
Multidimensional nature of human sexuality.
Both research and clinical practices with endometriosis require the cooperation between different professional figures, such as gynecologists, psychologists, and sexologists, which is consistent with the nature of endometriosis itself: a chronic disease that entails a life-long personalized management program. 85,86 In this specific long-term view of a patient-centered endometriosis care, aspects of quality of life and sexual health play a key role and should always be assessed with any patient. Specifically, during the first clinical assessment, gynecologists should offer a framing statement to show patients that a sort of “screening” on sexual health is routinely performed (and not because some type of sexual dysfunction is necessarily suspected), incorporating questions about sexual health into medical history. Moreover, it is of great importance to inform patient on the confidentiality of the discussion and to establish and maintain a trusty relationship. This could help women with endometriosis more easily disclose intimate aspects of their life.
As acknowledged by the World Health Organization, 87 sexual health matters. Consequently, medical school should provide elective courses on sexuality and sexual dysfunctions, as a lack of knowledge on sexuality among health-care professionals is perceived worldwide as a relevant problem, both in gynecological research and in clinical practice. 88 Building such a clinical and theoretical model may offer a framework for understanding the complex interaction of all the factors that influence sexual life and could therefore provide ideas and useful suggestions for prevention and intervention. This need for a comprehensive approach (ie, medical treatment of painful symptoms as well as attention to issues related to sexuality, couple adjustment problems, psychological aspects, and quality of life indicators) is particularly felt among women with endometriosis and should be encouraged and implemented in clinical practice.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.