
Abstract
Inflammation and oxidative stress are intrinsically linked to early poor placentation, typical of pregnancies complicated by preeclampsia associated with intrauterine growth restriction (PE-IUGR). Low mitochondrial DNA copy number (mtDNAcn) in peripheral blood constitutes a good peripheral surrogate marker of inflammation and oxidative stress. On these basis, we explored a possible correlation between mtDNAcn in peripheral blood in the first trimester of pregnancy and the PE-IUGR onset. To shed light on this issue, we setup a nested case–control study from a prospective cohort of pregnant women undergoing first-trimester aneuploidies screening. Two groups of patients affected by PE classified according to the clinical phenotype were identified: (1) patients who developed PE-IUGR and (2) patients who developed PE associated with appropriate for gestational age intrauterine fetal growth (PE-AGAf). Controls were women with a physiologic pregnancy matched to cases on the basis of age (±6 months, ratio 2:1). Mitochondrial DNA copy number was quantified using real-time polymerase chain reaction and normalized to nuclear DNA. The median (interquartile range) mtDNAcn in peripheral blood in patients with PE-IUGR (n = 12) and in patients with PE-AGAf (n = 16) was 70 (44-97) and 108 (95-145), respectively (P = .004). Both these values were significantly lower than that detected in the control group (161[133-183], P < .001). The area under the receiver–operator curve for PE-IUGR and PE-AGAf were 0.94 (95% confidence interval [CI]: 0.88-1.00, P < .001) and 0.81 (95%CI: 0.70-0.91, P < .001), respectively. In conclusion, MtDNAcn in peripheral blood resulted significantly lower both in patients affected by PE-IUGR and in those affected by PE-AGAf when compared to controls. The accuracy of this biomarker resulted particularly good in predicting PE-IUGR.
Introduction
Preeclampsia (PE) is a heterogeneous and multisystem disorder characterized by the new onset of hypertension associated with various organ damages and/or fetal growth restriction. 1 This syndrome is a major cause of maternal, fetal, and neonatal morbidity and mortality, especially in low- and middle-income countries. 2 -4
It is very likely that different maternal and placental causes give origin to this syndrome. According to the most accepted pathophysiological models, the final common pathway is determined by the oxidative stress of the syncytiotrophoblast and by the dramatic changes derived by this condition, including an abnormal balance between pro and antiangiogenic factors and relevant changes in the peripheral levels of micro RNA and microvescicles. 5,6 However, the same oxidative stress might origin from 2 different conditions: a shallow trophoblastic invasion occurring early in the first trimester or overcrowding of tertiary villa late in gestation. 7 The former condition is associated with fetal growth restriction, and the latter is associated with normal or large babies. 8 These 2 major clinical phenotypes of PE are very likely to be associated with different if not opposite maternal hemodynamic conditions. 9,10 Elevated oxidative stress associated with early shallow trophoblastic invasion is evident as early as 8 to 10 weeks’ gestation and manifests in both the placenta and the maternal circulation, with evidence of diminished antioxidant defenses, increased free radical formation, and isoprostanes, 11,12 as such to cause major hemodynamic abnormalities at the level of the uterine arteries as observed by Doppler velocimetry. 13 In contrast, early modifications may lack in the second form, that is, when initial development of the placenta occurs normally. This dualistic view of the pathogenesis of PE is important for both clinical and research reasons, but, not surprisingly, some risk factors or pathogenetic aspects can overlap. 14,15
Major challenges in modern obstetrics is the prediction of women at high risk of PE early in the first trimester. 14,15 Since the trophoblastic invasion and the consequent inflammatory reaction are among the earliest events in pregnancy, one could speculate that inflammation mediators might constitute adequate predictors. However, on the one hand, the selective dosage of a single cytokine lacks in specificity, and, on the other hand, the precise quantification of reactive oxygen species (ROS) is difficult. Surrogate markers reflecting inflammation and oxidative stress should thus be investigated. In this regard, mitochondrial DNA copy number (mtDNAcn) in peripheral blood might constitute a suitable candidate. In fact, recent findings showed an interplay between peripheral blood mtDNA content and inflammation biomarkers. 16 In particular, in a general population, lower peripheral blood mtDNA levels are to be associated with higher levels of classical inflammatory markers such as C-reactive protein, interleukin 6, white blood cell counts, and neutrophil-to-lymphocyte ratio. 17 -19
Both excessive oxidative stress and perturbed mitochondrial antioxidant capacity can disturb mtDNA replication and contribute to decline in mtDNA content in peripheral blood. 16 Furthermore, when compared to its nuclear counterpart, mtDNA accumulates damage more extensively when exposed to ROS. 19,20 Unfortunately, direct evidence showing an association between the amount of reactive ROS and the mtDNAcn in peripheral blood are lacking. However, several authors observed a reduced peripheral blood mtDNA content in patients with conditions traditionally characterized by an excessive oxidative stress such as metabolic syndrome and coronary heart disease. 21 -25
On these basis, we hypothesized a possible correlation between mtDNAcn in peripheral blood in the first trimester of pregnancy and the onset of PE associated with early placental damage and fetal growth restriction. The aim of this study was thus to explore whether mtDNAcn in maternal peripheral blood is reduced in pregnancies that develop PE associated with fetal growth restriction.
Material and Methods
This is a nested case–control study drawn from a prospective cohort of pregnant women referred for routine first-trimester screening for aneuploidies (from 11+0 to 12+6 weeks of gestation) at the “Fondazione IRCCS Ca’ Granda Ospedale Maggiore Policlinico” between January 2012 and May 2013. All women referred were offered the opportunity to participate in the study. Those accepting provided a blood sample and were interviewed using a standardized questionnaire. Blood samples were collected in 3 mL EDTA-containing tube and immediately stored at −20°C. An active follow-up was performed 6 to 12 months later using hospital records or contacting by phone the patient if inconsistencies or incompleteness in the available documentation emerged. The study was accepted by the local institutional review board. All recruited patients provided a written informed consent to participate.
In this larger prospective cohort, we identified 2 groups of patients affected by PE classified according to the clinical phenotype: (1) patients who developed PE associated with intrauterine fetal growth restriction (PE-IUGR) and (2) patients who developed PE associated with appropriate for gestational age intrauterine fetal growth (PE-AGAf).
Preeclampsia was defined, according to the International Society for the Study of Hypertension in Pregnancy criteria, as de novo hypertension present after 20 weeks of gestation combined with proteinuria (>300 mg/d) andother maternal organ dysfunction, such as renal insufficiency, liver involvement, neurological or hematological complications, uteroplacental dysfunction, or fetal growth restriction. 4,26
Intrauterine growth restriction (IUGR) was defined as fetal abdominal circumference (AC) <5th centile for gestational age at recruitment in fetuses that were normally developed at the time of midgestation scan or had a decrease of AC in subsequent ultrasound measurements >40 centiles. 27 Patients were matched on the basis of age (±6 months) to the subsequently referred women with a physiologic pregnancy (controls) in a 1:2 ratio.
Inclusion criteria for both cases and controls were (1) first pregnancy, (2) singleton pregnancy, (3) natural conception (women conceiving with the use of controlled ovarian hyperstimulation with or without assisted reproductive techniques were excluded). Exclusion criteria were (1) chronic diseases or serious health problems in the past, (2) chronic therapies, (3) major fetal abnormalities identified at the time of scanning performed at 11 to 12+6 weeks of gestation, (4) fetal aneuploidies, and (5) gestational diabetes.
Blood samples were all thawed simultaneously. Total genomic DNA was isolated from whole-blood specimens by the Wizard Genomic DNA Purification Kit (Promega, Milan, Italy). ABI Prism 7900 fast sequence detection system (Applied Biosystems, Foster City, California) was used for real-time quantitative polymerase chain reaction (PCR) analysis, according to our previously published method, 28 using the RNase P gene as an endogenous control (Cat No. 4316844; Applied Biosystems) and AB Mitochondrial Gene 7 S, encoding D-loop, as target gene (Hs02596861_s1, Assays-on-Demand Gene Expression Products; Applied Biosystems). RNase P is a single-copy nuclear gene that encodes the RNA moiety for the RNase P enzyme. D-loop is a replication start site of the mtDNA. Real-time quantitative PCR was performed leading to reactions characterized by the point in time during cycling when amplification of a PCR product achieved a fixed level of fluorescence. Target and reference genes were amplified in separate wells in duplicate. Reaction conditions included 10 µL of 2X TaqMan fast universal PCR master mix, 1 µL of primers and probes mixture, 150 ng of template DNA, and nuclease-free water to a 96-well reaction plate. The total reaction volume was 20 µL. The cycling conditions were as follows: 20 seconds at 95°C and 40 cycles of 3 second at 95°C followed by 30 seconds at 60°C. Data were analyzed using the comparative Ct method, where Ct is the cycle number at which fluorescence first exceeds the threshold. The Δ cycle thresholds (ΔCt) values from each sample were obtained by subtracting the values for the reference gene from the sample Ct, thus normalizing to nuclear DNA. For each experimental sample, the 2−ΔCt was calculated, and data were graphically indicated as relative quantification. A standard curve for mtDNA quantification was not used. Data were indeed normalized to nuclear DNA and are reported as number of copies per nuclear DNA (mtDNA/nDNA).
The primary end point of the study was the mtDNAcn assessment in peripheral blood of patients who developed PE-IUGR, PE-AGAf, and controls. A subanalysis was performed in order to test the accuracy of mtDNA copy number in peripheral blood in also predicting early- and late-onset PE. Pregnancy was defined as complicated by early-onset PE if delivery was required before 34 weeks of gestation.
Analysis of the data was carried out with the Statistical Package for Social Sciences 18.0 (SPSS Inc, Chicago, Illinois). Statistically significant differences were determined using Fisher exact test, χ2 test, Student t test, or the Mann-Whitney U test, as appropriate. The mtDNAcn in peripheral blood was presented as median (interquartile range [IQR]) and compared using the Mann-Whitney U test. Value of P below .05 were considered statistically significant.
To test the accuracy of mtDNAcn in peripheral blood in predicting PE, we performed a receiver–operator curve (ROC) analysis. The capacity of mtDNAcn in peripheral blood in predicting the onset of PE was considered excellent if the area under the curve (AUC) was >0.90, good if it was between 0.80 and 0.90, fair if it was between 0.70 and 0.80, and poor if it was between 0.60 and 0.70. The best threshold to discern between women who did and did not develop PE was identified using the Youden index (J) and used to calculate the odds ratio (OR) of developing PE. J is a measure for evaluating the biomarker effectiveness. Let Se (c) and Sp (c) be the sensitivity and specificity values associated to a particular cutoff point (c).
J is a function of Se (c) and Sp (c), such that:

Over all cutoff points c, cJ denotes the cutoff point corresponding to J. When the value of J is maximum, c J is the optimal cutoff point value. 29
The sample size was calculated setting type I and II errors at the conventional 0.05 and 0.20 and considering clinically relevant a mtDNA copy number in peripheral blood 40% lower in women who developed PE-IUGR compared to controls. On these bases, the required sample size was at least 11 cases (women who developed PE-IUGR). Women with PE-AGAf were recruited from the whole cohort if they fulfilled the eligibility criteria.
Results
A total of 1200 women were initially eligible to participate. Of these, 1051 accepted and 149 refused for personal reasons. Preeclampsia was reported in 35 patients, of whom 28 fulfilled the eligibility criteria. Preeclampsia was associated with IUGR in 12 patients. Cases were matched with 56 controls.
Table 1 summarizes the maternal characteristics, laboratory results, and neonatal outcomes of the control, PE-IUGR, and PE-AGAf groups. Gestational age at delivery resulted significantly lower both in PE-IUGR and in PE-AGAf group when compared to controls and in PE-IUGR group when compared to PE-AGAf group. All preterm births in the PE-IUGR group were iatrogenic.
Maternal Characteristics, Laboratory Results, and Neonatal Outcomes of PE-AGAf Group, PE-IUGR Group, and of Control Group.a
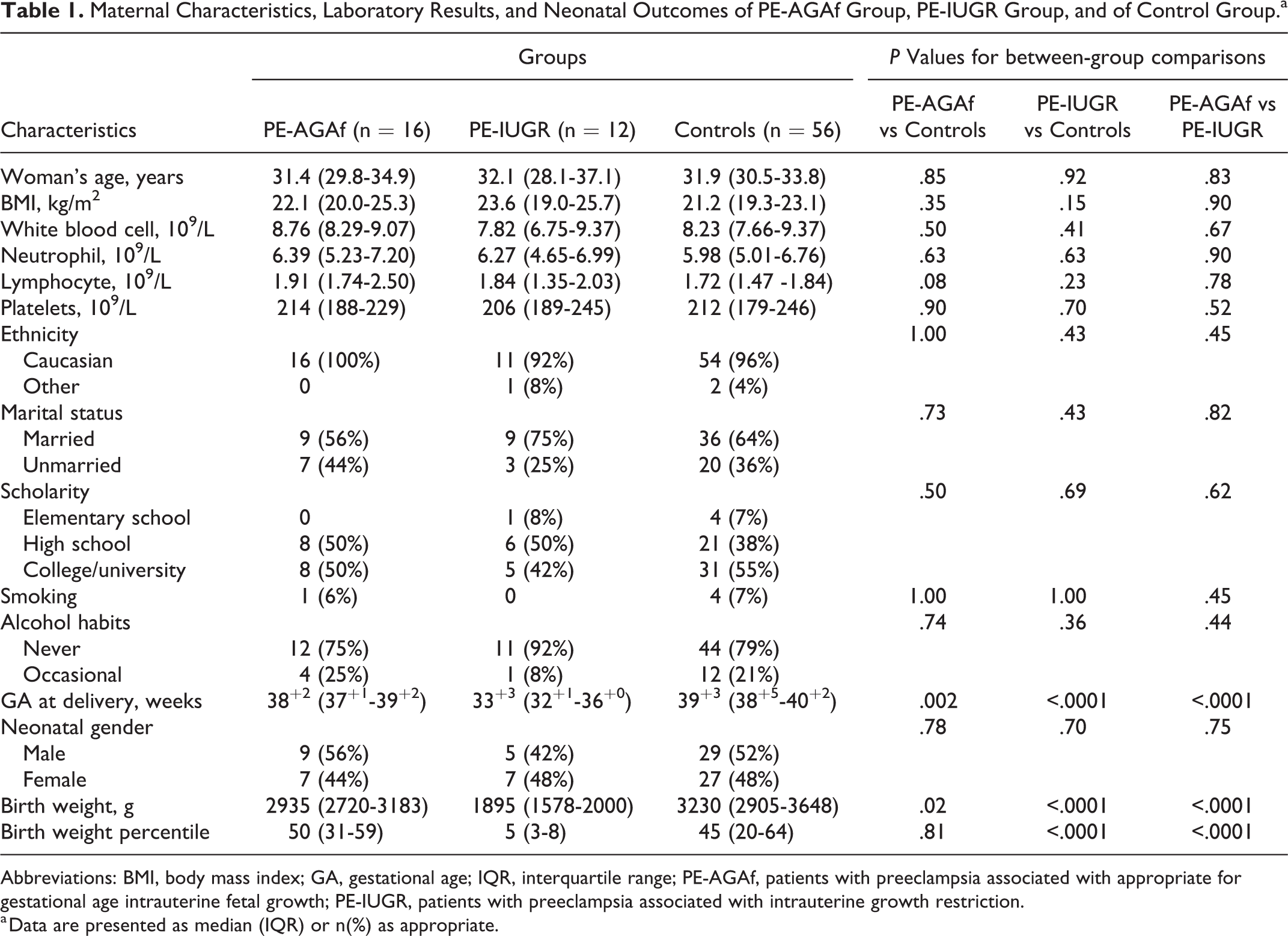
Abbreviations: BMI, body mass index; GA, gestational age; IQR, interquartile range; PE-AGAf, patients with preeclampsia associated with appropriate for gestational age intrauterine fetal growth; PE-IUGR, patients with preeclampsia associated with intrauterine growth restriction.
a Data are presented as median (IQR) or n(%) as appropriate.
The median (IQR) mtDNAcn in peripheral blood in PE-IUGR and in PE-AGAf was 70 (44-97) and 108 (95-145), respectively (P = .004). Both these values were significantly lower than that detected in the control group (161 [133-183], P < .001; Figure 1).
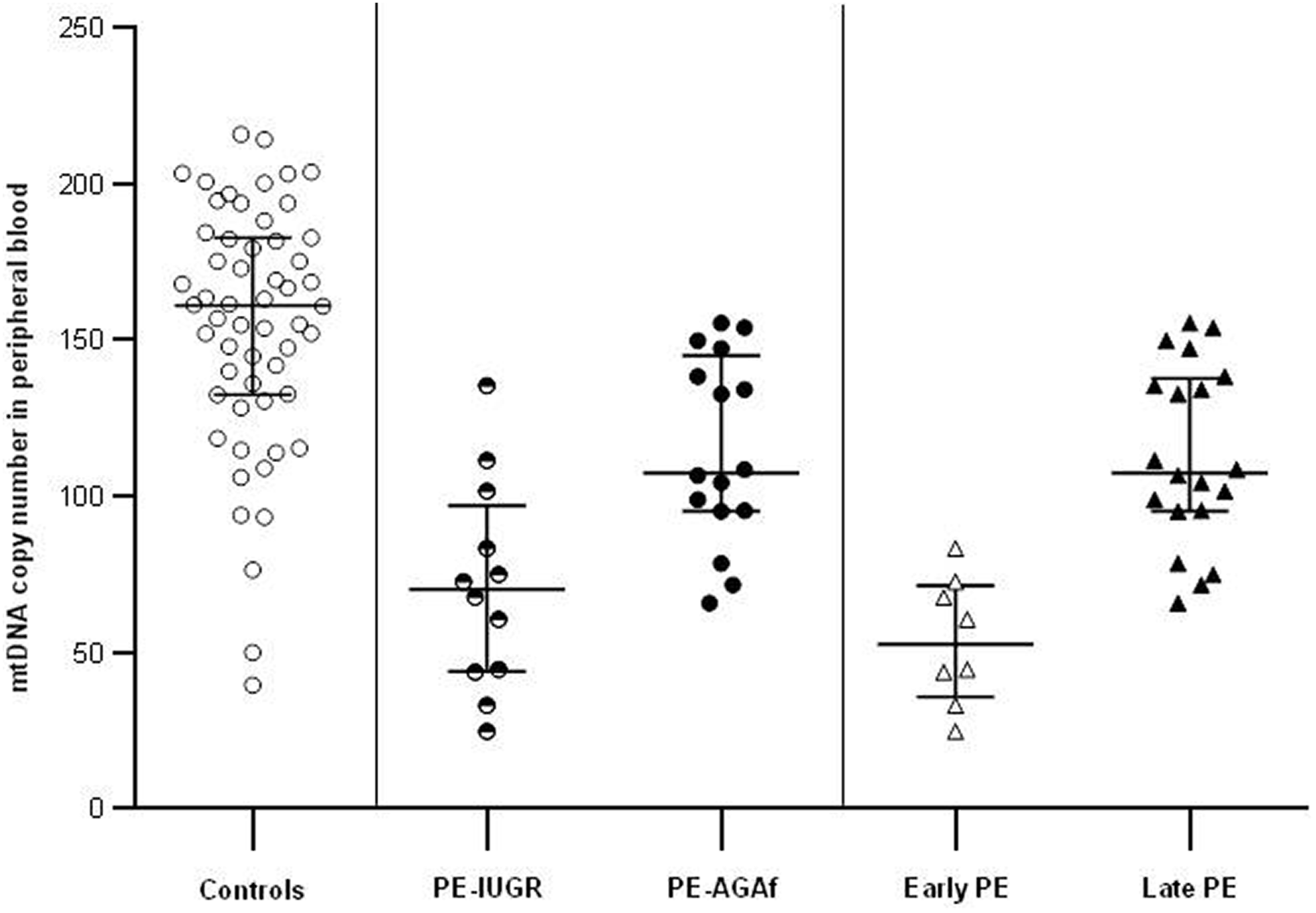
Mitochondrial DNA copy number (MtDNAcn) in peripheral blood in patients who developed PE defined on the basis of the 2 classifications (clinical phenotypes and temporal classification) and in controls. Bars represent median and interquartile range. Nonparametric Mann-Whitney U test was used to determine the difference in mtDNAcn between the groups. MtDNAcn resulted significantly lower in PE-IUGR group (half-filled circles) when compared to mtDNAcn in PE-AGAf group (filled circles; P = .004) and in control group (empty circles; P < .001). MtDNAcn resulted significantly lower in PE-AGAf group when compared to mtDNAcn in control group (P < .001). MtDNAcn resulted significantly lower in early-onset PE group (empty triangles) when compared to mtDNAcn in late-onset PE group (filled triangles; P < .001) and in control group (P < .001). MtDNAcn resulted significantly lower in late onset PE group when compared to mtDNAcn in control group (P < .001). PE indicates preeclampsia; PE-AGAf, preeclampsia associated with appropriate for gestational age intrauterine fetal growth; PE-IUGR, patients with preeclampsia associated with intrauterine growth restriction.
The median (IQR) mtDNAcn in peripheral blood in early PE and late PE was 53 (36-72) and 108 (95-138), respectively (P < .001). Both these values were significantly lower than that detected in the control group (P < .001; Figure 1).
The areas under the ROC curves based on the 2 PE classifications (clinical phenotype classification [PE-IUGR and PE-AGAf] and temporal classification [early and late onset PE]) are represented in Figure 2.
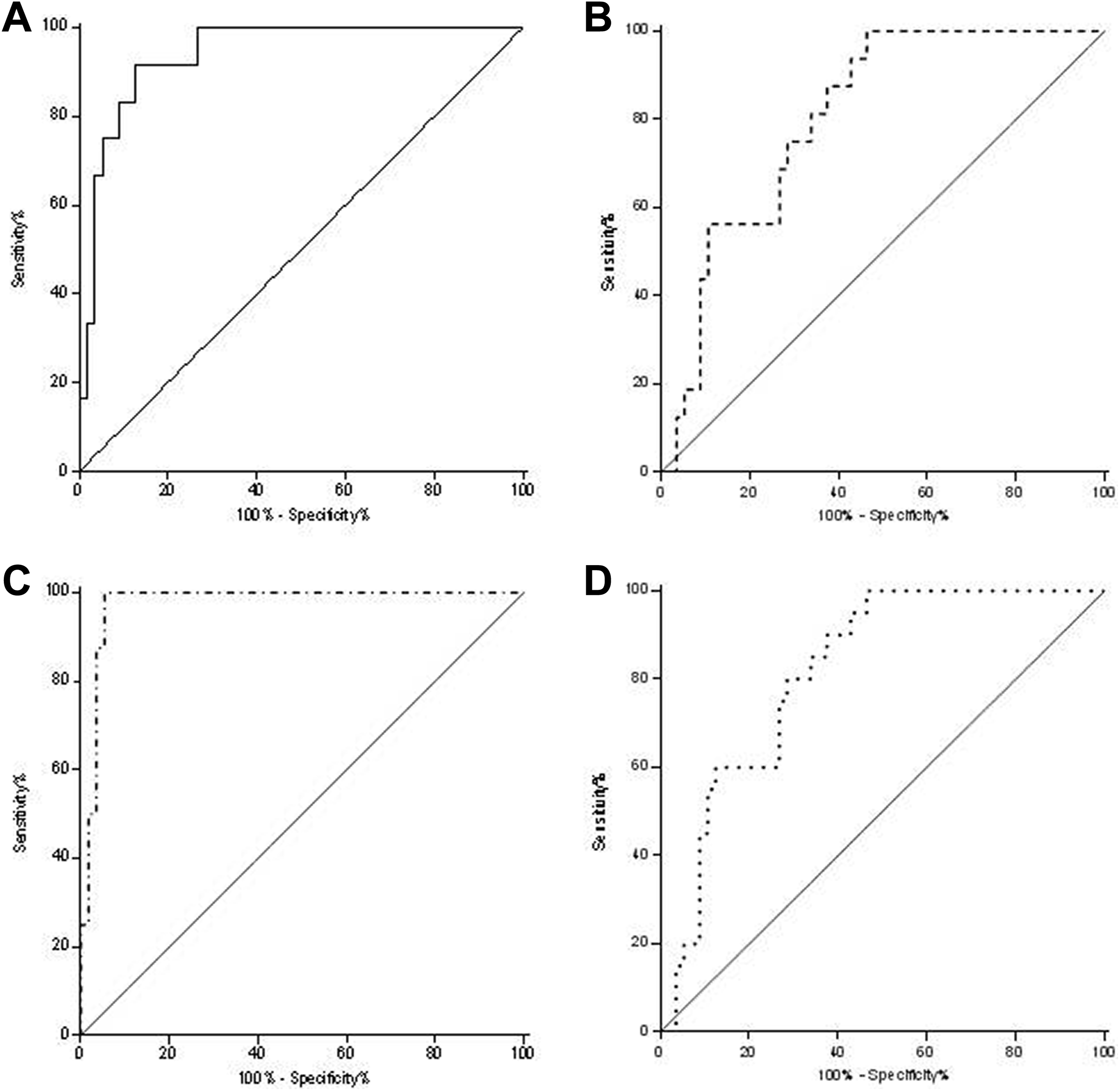
The figure represents the areas under the ROC curves based on the two PE classifications: clinical phenotypes (PE-IUGR and PE-AGAf) and temporal (early onset PE and late onset PE). Panel A: ROC curve for PE-IUGR (AUC 0.94 [95%CI: 0.88-1.00], P < .001). Panel B: ROC curve for PE-AGAf (AUC 0.81 [95%CI: 0.70-0.91], P < .001). Panel C: ROC curve for early onset PE (AUC 0.98 [95%CI: 0.00-1.00], P < .001). Panel D: ROC curve for late onset PE (0.82 [95%CI: 0.72-0.91], P < 0.001). AUC indicates area under the curve; CI, confidence interval; PE, preeclampsia; PE-AGAf, preeclampsia associated with appropriate for gestational age intrauterine fetal growth; PE-IUGR, patients with preeclampsia associated with intrauterine growth restriction; ROC, receiver operator curve.
The crude ORs for each PE subcategory development in women with mtDNAcn in peripheral blood below the corresponding Youden index are reported in Table 2.
Mitochondrial DNA Copy Number in Peripheral Blood and Risk of Preeclampsia Subcategories Development.
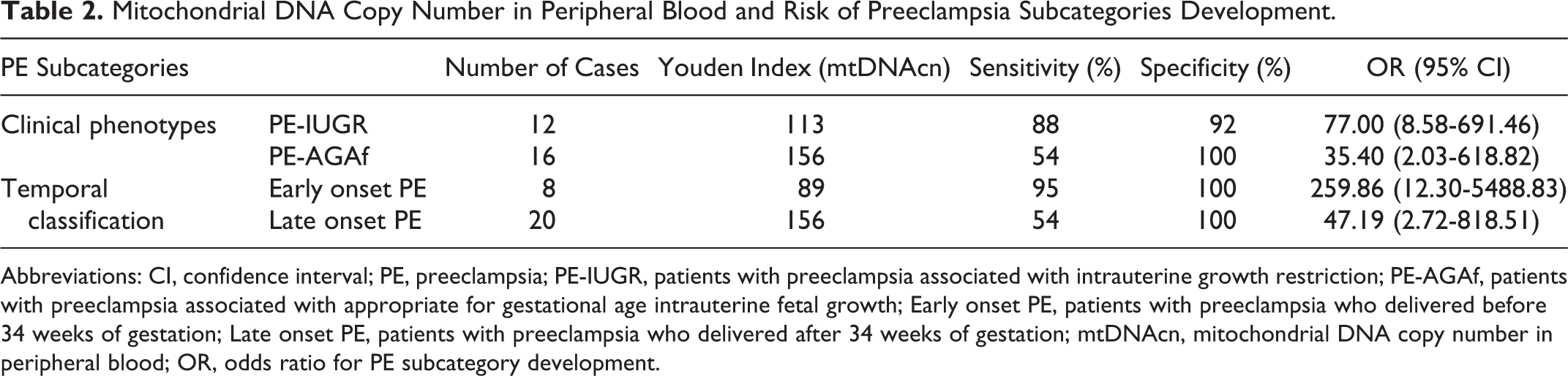
Abbreviations: CI, confidence interval; PE, preeclampsia; PE-IUGR, patients with preeclampsia associated with intrauterine growth restriction; PE-AGAf, patients with preeclampsia associated with appropriate for gestational age intrauterine fetal growth; Early onset PE, patients with preeclampsia who delivered before 34 weeks of gestation; Late onset PE, patients with preeclampsia who delivered after 34 weeks of gestation; mtDNAcn, mitochondrial DNA copy number in peripheral blood; OR, odds ratio for PE subcategory development.
In all patients who delivered before 34 weeks of gestation, PE was associated with IUGR. Their median (IQR) mtDNAcn in peripheral blood resulted significantly lower when compared to that of patients affected by PE-IUGR who delivered after 34 weeks of gestation (107 [82-130]; P = .004).
Discussion
In this study, mtDNAcn in peripheral blood resulted significantly lower in women who developed PE-IUGR compared to those who developed PE-AGAf and in both these clinical phenotypes compared to controls. The areas under the ROC curves show that mtDNAcn assessment in peripheral blood has an excellent accuracy in predicting the onset of PE-IUGR (AUC 0.94 [95% confidence interval, CI: 0.88-1.00], P < .001) and early-onset PE (AUC 0.98 [95%CI: 0.00-1.00], P< .001) and a good capacity in predicting the onset of PE-AGAf (AUC 0.81 [95%CI: 0.70-0.91], P < .001) and late-onset PE (0.82 [95%CI: 0.72-0.91], P < .001).
These findings seems to confirm our initial hypothesis. The extremely low mtDNA levels in peripheral blood assessed in patients who would have developed PE-IUGR may indeed be interpreted as a reflection of the particularly intense inflammatory process associated with the poor placentation that characterizes this PE phenotype already in the earliest stages of gestation and determines the release of placental factors. Interestingly, we also observed a significantly lower mtDNAcn in peripheral blood in early-onset PE-IUGR subgroup compared to late-onset PE-IUGR subgroup. Although the sample size is insufficient to draw reliable conclusions from this subanalysis, these findings seem to confirm an association between the extent of mtDNAcn depletion in peripheral blood and the severity of PE-IUGR.
Preeclampsia associated with AGAf is traditionally less easy to predict than PE-IUGR and less distinguishable from pregnancies uncomplicated by PE. In fact, unlike early-onset PE-IUGR, there is no antecedent pathology (poor placentation). 7 Nonetheless, our results show a good performance of mtDNA quantification in peripheral blood also in predicting late-onset PE. This form of PE is more common and seems to be the manifestation of a mismatch between the metabolic demands of the growing fetus close to term and maternal supply. 30,31 Cardiovascular and metabolic risk factors for endothelial dysfunction are considered as determinant in its genesis. 30 -33 Given the robust evidence demonstrating an association between a low mtDNAcn in peripheral blood and cardiovascular and metabolic diseases, one could speculate that low levels of this biomarker reflect an unfavorable metabolic pattern predisposing to the development of this PE subtype. 21 -25 A possible alternative or complementary explanation is suggested by the chorionic villi immaturity that characterizes the placental histology of PE associated with AGAf. In this regard, the role of mitochondria in energy production is critically important during embryo development and for placental function. 34 Since the mtDNAcn in peripheral blood is believed to be able to reflect the mitochondrial function of the whole organism, it can be hypothesized that a placental lack of energy may contribute to the inadequate chorionic villi proliferation and, as a consequence, to the development of this PE phenotype.
These interpretations are intriguing. Nevertheless, claiming that the mtDNAcn in peripheral blood is a marker of inflammation, oxidative stress or altered metabolic profile is still speculative. In fact, direct evidence showing a correlation between mtDNA blood content and metabolic, inflammation, and oxidative stress peripheral biomarkers in the first trimester of pregnancy have not yet been provided.
To the best of our knowledge, this is the first study investigating the association between the mtDNAcn in peripheral blood in the first trimester of pregnancy and the risk of developing PE. However, the role of mitochondria in pathophysiology of PE has already been studied. Mutations in the mitochondrial genes coding for respiratory chain enzymes and anomalies in mitochondrial DNA content, activity, and ultrastructure have been extensively described in placentas of women affected by PE. 35 -41 Even if less exhaustively, also the potential association between peripheral blood mtDNA content and PE has been investigated. Qiu et al measured free mtDNA content in blood samples (ie, noncellular mitochondrial DNA) collected during labor and delivery. Interestingly, they reported a linear trend in higher odds of PE with increasing quartiles of mtDNAcn (P for trend = .03) after controlling for confounders. 42 These results are only apparently in contrast with ours. In fact, the high oxidative stress characterizing the entire gestation of women who develop PE progressively determines the damage and destruction of cellular structures including the lipid membranes of mitochondria. It has been hypothesized that the mtDNA release by damaged cells and the compensatory mitochondrial response to this remarkable cellular stress can lead to the accumulation of mtDNA in peripheral blood that reaches the highest levels at the end of gestation. 42 Interestingly, some authors also investigated a possible correlation between placental mtDNA and fetal growth both in animal and in human models. Their results seem to agree in demonstrating a reduction of mtDNAcn in IUGR placentas confirming the pivotal role of mitochondrial quantitative depletion in this pregnancy complication. 35,41,43
The main limitation of the present study concerns the mtDNA quantification method. This aspect is still debated and far to be fully clarified. 44 -48 Solving this issue is thus of utmost relevance before designing future studies aimed at assessing the potential clinical role of peripheral mtDNA in the prediction of PE. To note, our results are also exposed to a spectrum biases, since we intentionally selected healthy controls with unremarkable pregnancies. The accuracy of mtDNA may be lower in an unselected population.
In conclusion, our findings suggest a possible role of depleted mtDNAcn in peripheral blood in predicting both PE-IUGR and PE-AGAf development. These results deserve a biological deepening. First of all, it would be very useful to establish whether the mtDNAcn depletion in peripheral blood observed in these 2 PE clinical phenotypes is the epiphenomena of an underlying process (ie, the inflammatory process in the case of PE-IUGR and the metabolic alterations in the case of PE-AGAf) or reflects a lack of energy constituting a predisposing factor to their development. Defining these aspects would make it possible to clarify, on the one hand, the pathophysiology of the 2 PE clinical phenotypes and, on the other hand, the possible clinical application of this peripheral biomarker. Further independent prospective studies designed on a larger cohort of patients are thus warranted.
Footnotes
Authors’ Note
The authors consider that Andrea Busnelli and Debora Lattuada should be regarded as joint First Authors.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.