
Abstract
Endometriosis is frequently related to infertility and little is known about the mechanisms underlying this association. Some studies point to an endometrial factor involved in this condition, which could compromise embryo implantation. Progesterone plays crucial role in endometrial receptivity by acting through progesterone receptor (PGR) isoforms PR-A and PR-B whose expression is epigenetically regulated by DNA methylation, in a specific promoter region for each isoform. Epigenetic changes in PGR-A and PGR-B may be related to progesterone resistance of endometriosis-related infertility. In order to better understand the mechanisms involved in endometrial receptivity, this case–control study aimed to compare the methylation pattern of PGR-A and PGR-B in eutopic endometrium from infertile women with and without endometriosis during the secretory phase. Endometrial biopsies from 19 patients (10 infertile women with endometriosis and 9 infertile controls) with regular cycles were performed during the secretory phase and were dated according to Noyes’ criteria. The percentage of DNA methylation at PGR-A and PGR-B was carried out by high-resolution melting assay. The PGR-A gene showed 0% of DNA methylation (unmethylated) in both control and endometriosis groups. However, PGR-B gene showed a partially methylated pattern in majority of the patients (n = 7), with methylation percentage corresponding to 50%, while in the control group the percentage of methylation was 20% (hypomethylated; P = .04). The increased percentage of methylation at PGR-B may be related to reduced gene expression, which could compromise the endometrial receptivity in patients with endometriosis.
Introduction
Endometriosis is a benign gynecological disease, characterized by the presence and growth of functional ectopic endometrial tissue, 1,2 which affects between 6% and 10% of women of reproductive age. 3 Studies suggest a compromised fertility in patients with the disease even in early stages, 4 –6 considering that 30% to 50% of women with this disorder are infertile. 7 However, the mechanisms involved in this condition are not yet fully understood. 8 In this regard, evidence indicates that functional endometrium defects may contribute to the decreased fecundity presented by patients with endometriosis. 9 –14
During the mid-secretory phase, the human endometrium undergoes molecular, histological, and structural changes that allow embryo implantation and the development of a pregnancy. 15,16 The coordinated alterations in this period are controlled by progesterone, whose action is mediated by progesterone-specific receptors. The progesterone receptor (PGR) gene encodes 2 proteins isoforms named PR-A and PR-B, each one with their specific promoter region and translation start sites. 17 The role of PGR-B is to be a dominant transcriptional activator of progesterone-sensitive promoters, whereas PGR-A acts as a dominant repressor of PGR-B and other steroid receptors. 18,19 Thus, the relative expression of PR-A:PR-B determines, in parts, the endometrial responsiveness to progesterone, 20 and consequently, the endometrial preparation for embryo implantation, once the interaction between progesterone and PGR-B triggers a gene cascade that regulates the expression of other genes essential for endometrial receptivity. 21
Progesterone resistance is commonly observed in women with endometriosis, 10,22,23 which could be due to problems related to ligand–receptor interaction, 24 ligand altered expression, and/or altered PGRs in these patients. 11,25,26 Studies evaluating the eutopic endometrium of women with endometriosis suggest alterations in many biomarkers directly or indirectly controlled by progesterone, such as αvβ3 integrin, 12,27,28 aromatase, 13,29 17-β-hydroxysteroid-dehydrogenase, 29,30 leukemia inhibitory factor, 31,32 HOXA10 and HOXA11, 14,32,33 osteopontin, 33,34 and mucin 1, 26 which are involved in the embryo implantation process.
The PGR-A and PGR-B are susceptible to epigenetic modulation of gene expression, such as DNA methylation, because of their promoter region rich in CpG dinucleotides. 35 Epimutations are related to aberrant gene expression in endometriosis, and the pattern of DNA methylation in the promoter region PGR isoforms could explain the progesterone resistance and the reported abnormal gene expression in infertile patients with endometriosis.
We question if an altered PGR epigenetic modulation may be an ethiopathogenic mechanism involved in endometriosis-related infertility. Thus, we sought to evaluate the methylation pattern of PGR-A and PGR-B promoter regions during the secretory phase in eutopic endometrial tissue of infertile patients with endometriosis.
Material and Methods
Setting and Duration
A prospective case–control study was conducted between December 2011 and November 2015 at the Human Reproduction Division, Department of Gynecology and Obstetrics, Ribeirão Preto School of Medicine, University of São Paulo (FMRP-USP). The research was approved by the Ethics Committee, and all patients signed the informed consent form.
Patients—Eligibility Criteria
Patients who presented regular cycles (every 24-38 days, 4.5 to 8 days of duration, and flow up to 80 mL per cycle) 36 for at least 3 months prior to the study, age between 18 and 45 years, body mass index (BMI) ≤30 kg/m2, absence of polycystic ovary syndrome and other etiologies of chronic anovulation, hydrosalpinx, and chronic diseases such as diabetes mellitus or other endocrinopathies, cardiovascular disease, dyslipidemia, systemic lupus erythematosus, and other rheumatologic diseases, HIV infection, any active infection, smoking habit, and use of hormonal medication, and anti-inflammatory drugs (such as nonsteroidal anti-inflammatory drugs and corticosteroids) during the 3 months preceding the beginning of the study were included. The endometriosis group consisted of patients with infertility exclusively associated with endometriosis diagnosed and classified by videolaparoscopy according to the American Society for Reproductive Medicine criteria. 37 The infertile control group consisted of patients with infertility attributable to male and/or tubal factors who underwent diagnostic videolaparoscopy for investigation of couple infertility and had ruled out endometriosis and other pelvic diseases.
The exclusion criteria for all groups were report of menstrual cycle alterations and use of hormonal medication during the monitoring before sample collection, and inability to attend at the scheduled date.
Sample Collection and Processing
Endometrial biopsy was performed during the early and mid-secretory phase on a scheduled date according to the individual cycle of each patient, by an experienced physician using Pipelle catheter under sterile conditions. For the standardization of data, ovulation day was considered as the 14th day of a 28-day menstrual cycle. To confirm that the collection was performed in the early and mid-secretory period, all samples were submitted to classical histological analysis with hematoxylin-eosin staining according to Noyes criteria, 38 performed by a pathologist with extensive experience. Immediately after collection, the endometrial samples were stored at −80°C immersed in phosphate-buffered saline.
High-Resolution Melting Assay
The genomic DNA was extracted using the QIAamp DNA Mini Kit (Qiagen, Hilden, Germany) and the bisulfite DNA modification was carried out with EpiTect Bisulfite Kit (Qiagen), according to the manufacturer’s specifications. The high-resolution melting (HRM) assay was performed using 2.5 μL of modified DNA from each sample, 1X of MeltDoctor HRM Master Mix (Applied Biosystems, Foster City, California), and 0.5 µM of each primer (PGR-A and PGR-B) in a final volume of 20 µL. The primers used were previously described by Wu et al, 35 specific for each isoform promoter region. A standard curve was performed with the PCR control kit DNA set (Qiagen) for each experiment with different percentages of methylated DNA (0%, 20%, 50%, 80%, and 100% methylated). Amplification was performed on the 7500 Fast Real-Time PCR System (Thermo Fisher Scientific, Carlsbad, CA, US).
Potential Sources of Bias
We avoided selection bias by inviting all patients who underwent diagnostic videolaparoscopy and fulfilled eligibility criteria to participate in the study. The between-group imbalances in covariates related to implantation and endometrial receptivity were avoided by adopting highly selective eligibility criteria for patient inclusion. We avoided detection bias by processing and analyzing all samples together and without group identification, since they were numbered consecutively in the order in which they were collected. The reporting bias was avoided by presenting and analyzing all results obtained.
Clinical Characteristics
Clinical characteristics such as age (years), height (meters), weight (kilograms), BMI, and cycle size (days) were collected from each patient.
Study Size
Considering the lack of data in the literature to estimate the percentage of methylation in the promoter region of PGR gene by HRM in eutopic endometrium, we designed a pilot study powered to detect or discard expressive differences between the groups. 39 Thus, from December 2011 to December 2014, all eligible patients who agreed to participate and who donated appropriate samples were included in the study.
Statistical Analysis
An exploratory data analysis was carried out through measures of central position and dispersion. Clinical characteristics such as age, height, weight, BMI, and cycle size were compared between the endometriosis and infertile control groups by Student t test. To compare the percentage of methylation of the PGR-A and PGR-B isoforms between the endometriosis and infertile control groups, the Fisher exact test was performed. Missing data (samples with inappropriate material or methylation pattern not determined) were excluded from the analysis. All results were compared using SAS 9.0 software (SAS Institute Inc, Cary, North Carolina University, North Carolina), with a level of significance of 5% (P < .05).
Results
From December 2011 to December 2014, 629 patients who underwent diagnostic videolaparoscopy at the University Hospital (FMRP-USP) were evaluated according to the eligibility criteria. One hundred one patients were eligible, 74 of them were interviewed, and 27 were not localized. Twenty-three of the interviewed patients did not agree to participate in the study and 27 of the 51 who wanted to participate were excluded (5 for menstrual cycle alterations, 14 for use of hormonal medication, 6 for starting assisted reproduction treatment, and 2 patients were unable to attend the sample collection at the scheduled date). Thus, 24 patients provided written informed consent (11 infertile women with endometriosis and 13 infertile controls) and had endometrial sample collected. All samples were confirmed in the secretory phase by Noyes’ criteria. One sample had inappropriate material for the analysis and 4 samples had the methylation pattern not determined. Thus, 19 samples (10 infertile women with endometriosis and 9 infertile controls) had PGR-A and PGR-B promoter region methylation analyzed (Figure 1).
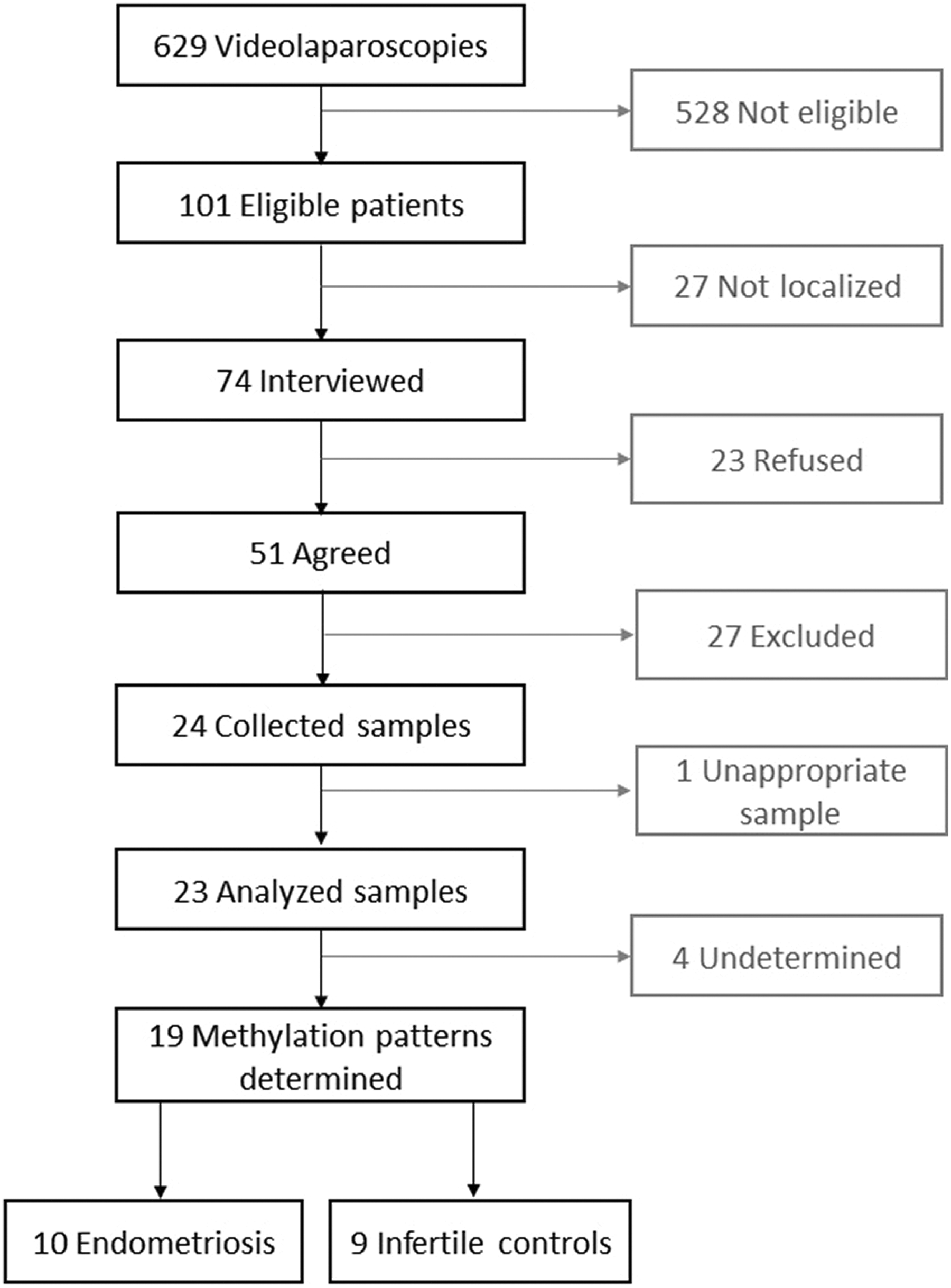
Study flowchart.
No differences were observed in any of the clinical characteristics evaluated between the endometriosis and infertile control groups (Table 1).
Clinical Characteristics of Infertile Patients With Endometriosis and Patients With Infertility Due to Tubal and/or Male Factor (Infertile Control).a
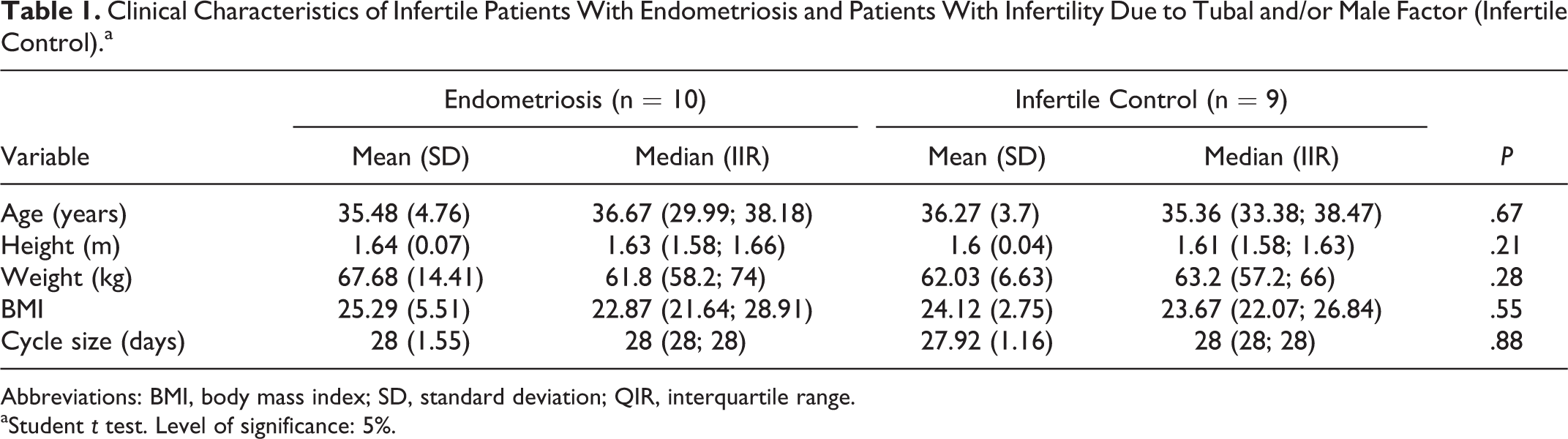
Abbreviations: BMI, body mass index; SD, standard deviation; QIR, interquartile range.
aStudent t test. Level of significance: 5%.
The PGR-A pattern of methylation was zero (0%) in both groups, endometriosis and control, corresponding to unmethylated pattern. Regarding the PGR-B isoform, a higher percentage of methylation was observed in the endometriosis group when compared to the infertile control group (P = .04). The partially methylated (50%) pattern was observed in 70% (n = 7) of endometriosis women and the hypermethylated (80%) pattern was presented in one participant. Two endometriosis women showed 0% to 20% of methylation at PGR-B (hypomethylated). In the infertile control group, the majority of patients (n = 7) had between 0% and 20% of methylation (hypomethylated) and only 2 (50%) participants showed a partially methylated PGR-B promoter region (P = .04). The hypermethylated pattern was not observed in the control group (Table 2; Figure 2).
Methylation Percentages of PGR-B Isoform in the Eutopic Endometrium of Infertile Patients With Endometriosis and Patients With Infertility Due to Tubal and/or Male Factor (Infertile Control).a
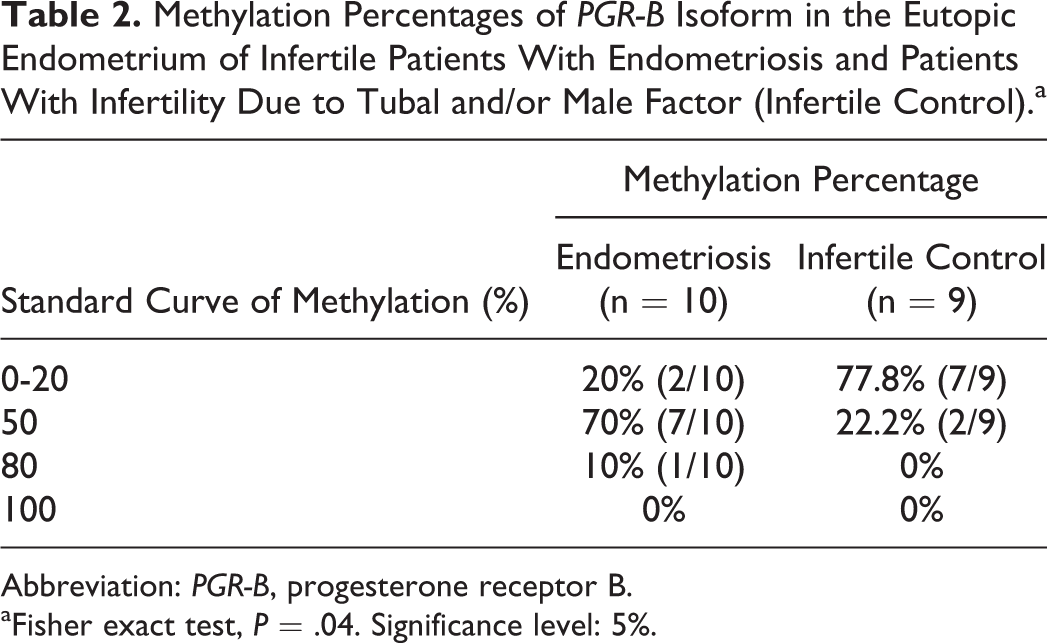
Abbreviation: PGR-B, progesterone receptor B.
aFisher exact test, P = .04. Significance level: 5%.
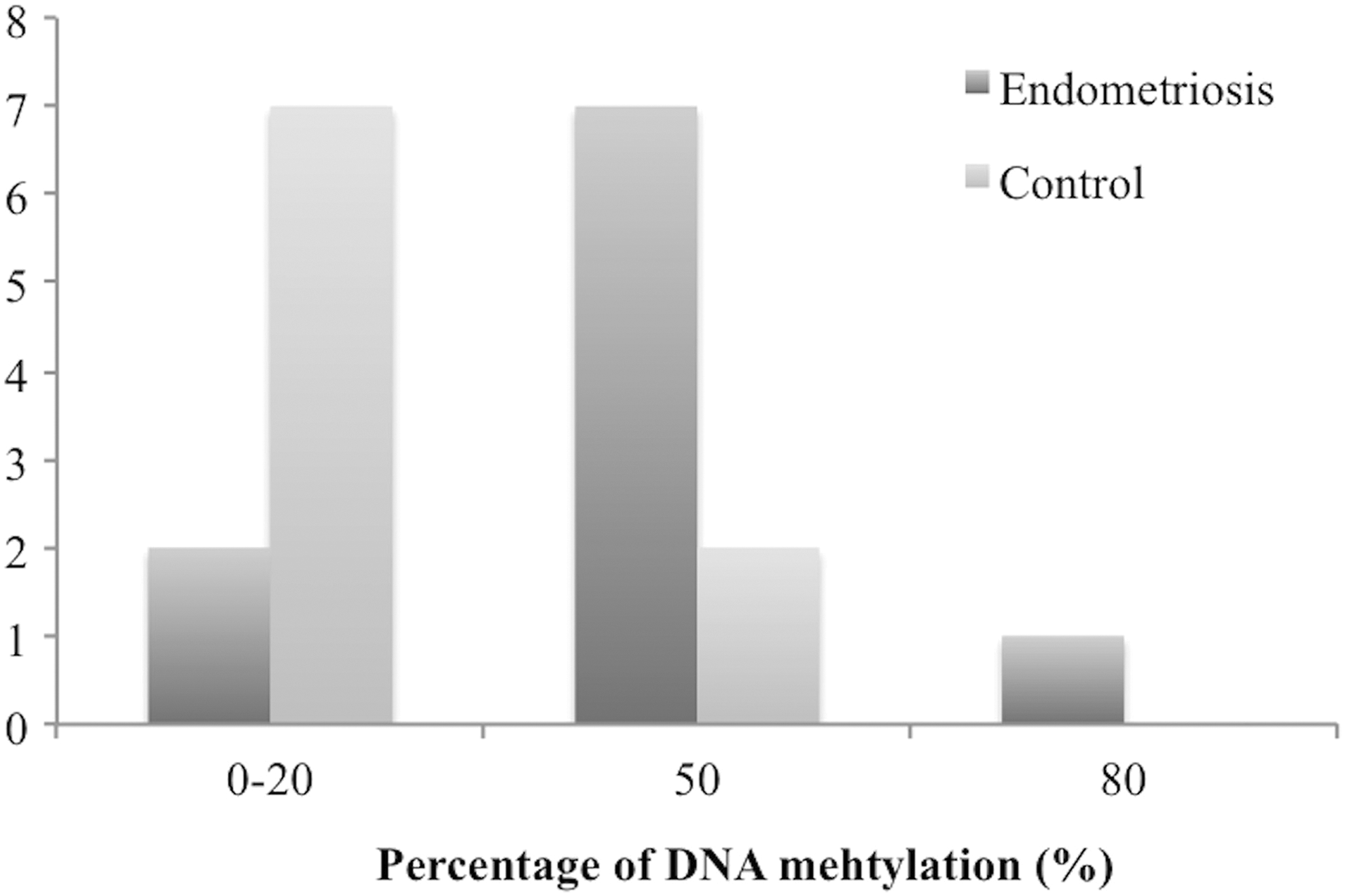
Percentage of DNA methylation at PGR isoform B (PGR-B) in the endometriosis and infertile control group (P = .04).
A methylation percentage greater than or equal to 50% was considered clinically significant. Based on the differences found (22% of the samples from the control group presented a methylation pattern of 50% or more versus 80% of the endometriosis group), our sample size allows a power of 80% considering the probability of type 1 or α error of 5%.
Discussion
The relationship between endometriosis and infertility is well established in the literature; however, the mechanisms involved in this condition remain uncertain. 8 Because endometriosis patients seem to present progesterone resistance, 10,22,23 we question if an altered PGR epigenetic modulation may be an ethiopathogenic mechanism involved in endometriosis-related infertility. Thus, we performed the first study evaluating PGR-A and PGR-B methylation pattern in eutopic endometrium from infertile women with endometriosis during the secretory phase.
According to our data, the PGR-A promoter region presented 0% of methylation in both groups, corresponding to an unmethylated pattern and an active gene expression. It is known that this isoform acts as a modulator of transcription, and its expression is related to transcriptional repression of PGR-B isoform and other steroid receptors. 18,19 This finding is in accordance with Koukoura et al, 40 which observed different pattern of methylation between the isoforms PGR-A and PGR-B. This finding also corroborates the study by Wu et al 35 in which the PGR-A isoform was also found unmethylated (0%). Taken together, these data suggest that there is no modification in the PGR-A promoter DNA methylation in endometriosis eutopic endometrium.
On the other hand, the PGR-B promoter region was found with higher level of DNA methylation in the endometriosis group, in which the majority of patients showed around 50% of methylation. Differently, in infertile patients without endometriosis, a lower percentage of methylation was observed in the analyzed region of PGR-B, which suggests that the infertility may be related to the expression of this isoform through epigenetic modulation. The PGR-B is a strong transcriptional activator of progesterone-sensitive promoters. 18 It is known that progesterone is the predominant steroid of the secretory phase and controls molecular events that promote the establishment of endometrial receptivity and the interaction between the endometrium and the embryo during implantation. 21 Its action occurs through specific ligand–receptor bonds, which trigger a gene cascade whose transcripts act autocrine, paracrine, or endocrinously, with consequent histological, molecular, and functional changes. 21 It is already known that promoter methylation leads to decreased gene expression or even total silencing. 41 Based on the present findings, we suggest that this higher percentage of DNA methylation observed in PGR-B promoter region may contribute to reduced expression of the receptor and trigger a cascade of molecular changes previously observed in the eutopic endometrium of women with endometriosis, consequently affecting the embryo implantation and the fertility of these patients. Moreover, since responsiveness to progesterone is inversely related to the PR-A:PR-B ratio, 17 and considering that PGR-A can be a potent and dominant ligand-dependent repressor of PGR-B transcriptional activity, 19 the increased DNA methylation at PGR-B and absence (0%) at PGR-A genes suggests an altered isoform ratio that may lead to lower progesterone response in the eutopic endometrium of these patients, and impact on embryo implantation.
Wu et al 35 evaluated the methylation of PGR-B in epithelial cells from eutopic endometrium and endometriotic foci of patients with the disease, using another methodology (methylation-specific PCR [MSP] and sequencing). In contrast to our data, these authors evidenced no alterations in the methylation pattern of PGR-B in eutopic tissue, while in endometriosis lesions a partially methylated pattern was observed. However, their focus was to evaluate the role of PGR methylation in the pathogenesis of endometriosis but not in the infertility associated with this condition, since they included patients with the disease regardless of infertility and obtained samples during different phases of the cycle, mostly in the proliferative phase.
Our data are in accordance with some of the previous studies on PGR’s expression in eutopic endometrium from women with endometriosis, which found alterations in endometrial PRB protein level or mRNA expression. 11,26,42 In this sense, Shen et al 26 evidenced lower protein levels of PRB in infertile patients with endometriosis as compared with the infertile control group. On the same way, Igarashi et al 11 found lower PR-B:PR-A ratio in eutopic endometrium from infertile women with the disease by immunoblotting. In addition, a lower expression of PGR-B was previously found during the mid to late secretory phase in eutopic endometrium of women with endometriosis. 42
Nevertheless, we are not able to affirm if the alteration found is a cause, a consequence or a parallel feature of the disease. However, based on studies that evidenced an estrogen receptor (ER) aberrant expression during the secretory phase of baboons 43 and women with the disease, 44,45 we hypothesize that the higher methylation of PGR-B in these patients could be related to an inappropriate ER downregulation during this period of the cycle, which could affect the uterine receptivity. 46 This hypothesis should be evaluated by appropriate methodologies.
The main limitation of this study was the small sample evaluated due to the restrictive eligibility criteria adopted, limiting the study’s generalizability. However, in order to increase the internal validity, strict eligibility criteria are necessary to eliminate other factors that are potentially related to compromised endometrial receptivity and implantation. In addition, it was not possible to stratify the endometriosis group into the stages of the disease due to the small sample size.
Despite the limitation of the sample size, we observed increased DNA methylation level in the PGR-B promoter region in eutopic endometrium of infertile patients with endometriosis that was partially methylated and hypermethylated in some patients. These alterations could directly affect its expression and consequently influence the response of the endometrial cells to progesterone, impacting embryo implantation and fertility of these women. The present findings suggest an epigenetic deregulation involved in compromised fertility and may be a key mechanism involved in the endometriosis ethyopathogeny. Further studies, with greater casuistry, are necessary to confirm these data.
Supplemental Material
Supplemental Material, STROBE_checklist - Progesterone Receptor B (PGR-B) Is Partially Methylated in Eutopic Endometrium From Infertile Women With Endometriosis
Supplemental Material, STROBE_checklist for Progesterone Receptor B (PGR-B) Is Partially Methylated in Eutopic Endometrium From Infertile Women With Endometriosis by Carlos Valério Rocha-Junior, Michele Gomes Da Broi, Cristiana Libardi Miranda-Furtado, Paula Andrea Navarro, Rui Alberto Ferriani and Juliana Meola in Reproductive Sciences
Footnotes
Acknowledgments
The authors thank the staff of the Human Reproduction Division, University Hospital, Department of Gynecology and Obstetrics, Faculty of Medicine of Ribeirão Preto, University of São Paulo (FMRP-USP) specially Dr Filomena Marino Carvalho, Dr Júlio César Rosa e Silva, Dr Stael Porto Leite, Dr Anderson Melo, Dr Valeria Leitão, Dr Ludimila Seko, Dr Lilian A. Nunes, Dr Danielle M. Teixeira, Dr Clarissa V. Dias, Dr Marcela Alencar, Dr Maria Lucia Lima, Dr José Vitor Zanardi, Cristiana Padovan, Maria Auxiliadora Rosa, Ocelia Vasconcelos, Lourdes Adriana Andrade and Marisa Blanco and the staff of SERPAT—Pathology Service of the Department of Pathology, FMRP-USP, specially Dr Alfredo Ribeiro and Dr Francesca Maia Faria for their valuable assistance.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study received financial support from the National Institute of Science and Technology—Hormones and Woman’s Health (Instituto Nacional de Ciência e Tecnologia—Hormõnios e Saúde da Mulher), the São Paulo Research Foundation (FAPESP—Fundação de Amparo à Pesquisa do Estado de São Paulo; fellowships 2011/17614-6, MGB and 2012/11069-9, CLMF) and from the National Council for Scientific and Technological Development (CNPq—Conselho Nacional de Desenvolvimento Científico e Tecnológico; grant number 471943/2012-6, PAN; fellowship 140137/2015-7, MGB).
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.